
Abstract
This study investigated associations between stress, resilience factors, and symptoms of depression and anxiety in a cross-sectional sample of 1183 adolescents 13–18 years old. The results showed a positive significant association between stress and symptoms of depression and anxiety. Personal competence was significantly negatively associated with depression and anxiety, whereas social support was significantly negatively associated with anxiety. Significant interaction effects were found between gender by personal competence and gender by structured style in relation to anxiety, with stronger associations for girls. A compensatory role of resilience was found on the relation between stress and emotional symptoms.
Introduction
The transition into adolescence seems to be the starting point for an increase in psychological symptomatology of clinical significance (Hankin, 2009; Thapar et al., 2012). The probability of symptoms (especially depressive symptoms) affecting adolescents’ daily living rises from around 5 percent in early adolescence to as high as 15 percent by the end of adolescence, with a strong female preponderance (about 2:1) (Thapar et al., 2012). The gender differences seem to increase in middle to late adolescence (Hankin, 2009; Thapar et al., 2012). Anxiety symptoms are estimated to appear in about 13 percent in a population of 13- to 18-year-old Norwegian adolescents (Skrove et al., 2013) with gender differences appearing by middle childhood and remaining throughout adolescence (Hankin, 2009).
Most emotional symptoms are caused by multiple factors and processes rather than singular causes (Hjemdal, 2007). Exposure to multiple independent and cumulative stressors plays a substantial role in the development of symptoms of depression and anxiety (Byrne et al., 2007; Charbonneau et al., 2009). Girls report higher stress levels (Moksnes et al., 2014) and seem to be more vulnerable to the negative emotional health effects of stress than boys (Charbonneau et al., 2009; Moksnes et al., 2014). However, the stress process and the impact from stress vary individually and lead to different health outcomes; this depends on individual vulnerabilities and resources, as well as the individual’s ability to cope (Compas and Reeslund, 2009; Hjemdal, 2007).
Resilience has received considerable attention as a relevant protective factor modifying the impact of stressors. Resilience is defined as “… the protective factors and processes that, despite experiences with situations shown to carry significant risks for developing psychopathology, contribute to good outcome” (Hjemdal et al., 2006b: 195). Being resilient is a dynamic personal resource that develops throughout life, reflecting an ability to cope with different life condition using protective resources within the individual or the individual’s environment (Davydor et al., 2010; Zolkoski and Bullock, 2012). Empirical evidence indicates a consensus on three overarching resilience characteristics in a persons’ life, serving as a guiding principle for the construct of resilience: (1) personal characteristics and resources of the individual; (2) a stable and supportive family environment marked by coherence; and (3) social resources outside the family (Hjemdal, 2007; Luthar, 2006). Although findings are not consistent, females seem to report higher scores on social and interpersonal resources, whereas males rate themselves higher on personal dispositions (Hjemdal et al., 2006a, 2006b, 2011). Furthermore, higher levels of resilience characteristics are related to lower levels of depressive symptoms (Hjemdal et al., 2006a, 2007, 2011; Skrove et al., 2013), anxiety (Hjemdal et al., 2011; Skrove et al., 2013; Von Soest et al., 2010), stress, and obsessive–compulsive symptoms (Hjemdal et al., 2011; Von Soest et al., 2010).
Researchers have also investigated whether resilience has a compensatory or protective role on the relation between stress and emotional functioning. A compensatory model argues that the protective resources operate irrespective of stress levels (compensation), while a protective model claims that resources are activated in the face of adversity (buffer effect). Previous studies have found support for the protective model among adults (Hjemdal et al., 2006b), whereas the compensatory model has been supported in studies with adolescents (Hjemdal et al., 2007), indicating varying findings across samples.
To improve prediction of good outcomes and healthy development despite experience of stressful situations, further studies are necessary to investigate which resilience characteristics are most relevant in the context of stress and emotional functioning and whether resilience has a protective or compensatory role (Grant et al., 2006). It is also important to further investigate potential gender differences on the associations between stress, resilience, and emotional health. Gaining more knowledge in this area is necessary for successful intervention work aimed at the adolescent population in general, as well as particular groups recognized as being at potential risk of emotional problems.
The aim of this study is to
Investigate the association between stress, resilience factors, and emotional symptoms (depression and anxiety);
Investigate the potential moderating role of gender on the association between stress (gender × stress), resilience (gender × resilience factors), and emotional symptoms;
Investigate the potential moderating role of the resilience factors (stress × resilience factors) on the relationship between stress and emotional symptoms.
On the basis of previous findings, it was expected that a compensatory role of resilience would be found.
Method
Participants
This study’s cross-sectional sample included public elementary and secondary schools in two counties in Mid-Norway. Of the 25 randomly selected schools, six (24%) (three urban and three rural) agreed to participate. A total of 1229 questionnaires were distributed (593 in elementary schools and 636 in secondary schools), and N = 1209 completed questionnaires were returned (51%, n = 617, from girls and 48.5%, n = 586, from boys; in 0.5% cases, n = 6, gender was not identified), giving an overall response rate of 98.4 percent. The age range of the sample included for analyses was 13 to 18 years and the data analyses were therefore undertaken for n = 1183, excluding 26 respondents who were older or younger than the defined age group.
Procedure
The data collection was approved by the Regional Committee for Medical Research Ethics (REK) and the Norwegian Social Science Data Services (NSD). The headmaster from each of the schools approved the content of the questionnaire prior to agreeing to participate in the survey. The adolescents and their parents received a letter that briefly explained the purpose of the study, emphasizing that participation was voluntary and anonymous, that participants were free to withdraw from the study at any time, and that the information collected was confidential. Passive consent from the participants was found to be sufficient because no sensitive personally identifying data were collected, implying that consent was given by answering the questionnaire. Questionnaire administration was completed in one session, in whole class groups, during one regular school period of 45 minutes.
Measures
Resilience
The Resilience Scale for Adolescents (READ) (Hjemdal et al., 2006a) is a 28-item self-report scale where adolescents are asked to evaluate how they have experienced their personal and social resilience resources during the last month. Items are rated on a 5-point Likert scale, ranging from (1) totally agree to (5) totally disagree, where higher scores indicate stronger resilience (Supplemental Table 1). The instrument comprises five factors: (1) personal competence, for example, “I reach my goals if I work hard”; (2) structured style, for example, “I always make a plan before I start something new”; (3) social competence, for example, “I easily make others feel comfortable around me”; (4) family cohesion, for example, “In my family we support each other”; and (5) social resources, for example, “My friends always stick together.” The READ has shown satisfying internal consistency with Cronbach’s alphas ranging from α = .69 (structured style) to α = .89 (family cohesion) (Hjemdal et al., 2006a, 2007; Von Soest et al., 2010). Cronbach’s alphas for the five resilience factors and all the scales used in the study are presented in Supplemental Table 2.
Stress was assessed using the Norwegian version of the Adolescent Stress Questionnaire (ASQ-N) (Moksnes et al., 2010a). The ASQ-N is a 56-item inventory designed to measure normative stressors that adolescents may experience in their daily lives (Byrne et al., 2007) during the last year. Items are rated on a 5-point Likert scale from (1) not at all stressful or is irrelevant to me to (5) very stressful; higher scores indicates higher level of perceived stress. Examples of items are “Disagreements between you and your parents,” “Keeping up with the school work,” and “Being hassled for not fitting in.” The ASQ-N has been appropriately tested with reference to internal consistency and construct validity (Moksnes and Espnes, 2011; Moksnes et al., 2010a).
Depressive symptoms
The depression scale was constructed by Byrne et al. (2007). The scale consists of 15 items assessing the respondent’s current level of non-clinical depressive mood in the past week, where items are rated on a 5-point Likert scale ranging from (0) never to (4) always, with higher scores indicating more symptoms of depression (Supplemental Table 1). Item choice was informed by reference to commonly experienced depressive features outlined in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association (APA), 2000) and the Zung (1965) Self-Rating Depression Scale. Some item examples are as follows: “I have felt sad or unhappy,” “I feel like crying,” and “I have felt like I have failed.” The internal consistency of the scale has been found to be high, showing Cronbach’s α between .91 and .96 (Byrne et al., 2007; Moksnes et al., 2010b).
State anxiety
The Spielberger (1983) State-Trait Anxiety Inventory (STAI) is a questionnaire measuring respondents’ level of anxiety. The state subscale was included to assess current emotional affect (like the depression scale) that represents a significant impairment of the individual’s psychological well-being. The scale consists of 20 items, rated on a 4-point Likert scale, ranging from (1) not at all to (4) very much so, where a higher score indicates more symptoms of anxiety (Supplemental Table 1). Example items are as follows: “I feel secure,” “I feel satisfied,” and “I am tense.” The STAI has been used extensively in adolescent populations (Byrne et al., 2007; Moksnes et al., 2010a, 2010b). The internal consistency of the scale has been found to be high, showing Cronbach’s α = .98 (Moksnes et al., 2010a) and α = .91 (Moksnes et al., 2010b).
Statistics
All statistical analyses were carried out using SPSS, version 21.0. Means and standard deviations were calculated for the continuous variables, using independent sample t-tests to investigate gender mean differences. To evaluate the strength of the gender differences on the continuous variables, effect sizes were interpreted following Cohen’s (1988) guidelines: small (.20), medium (.50), and large (.80+) effect size. Pearson product moment correlation was used to test bivariate associations between the variables separately for gender.
Multiple hierarchical linear regression analyses tested the associations between the independent variables of stress, resilience factors, and the dependent variables of depression and anxiety, controlling for gender and age. The interaction effects of gender by resilience factors and stress by resilience factors were examined by constructing interaction terms. The independent variables were included in five steps: (1) gender, (2) age, (3) stress, (4) resilience factors, and (5) interaction terms. Gender and age were entered in the first two steps in order to investigate their role as covariates. Stress and resilience were included in steps 3 and 4, respectively, in order to investigate the unique main effect of each variable. The interaction effects were entered in the last step in order to evaluate the potential protective or compensatory role of the resilience factors in relation to stress and the potential moderating role of gender in relation to stress and resilience factors. The p values ⩽.05 were considered statistically significant.
Results
Gender differences on stress, resilience factors, anxiety, and depression and correlations between variables in the study
The results from the independent sample t-tests showed that girls scored significantly higher on depression, anxiety, and stress levels (Supplemental Table 1). Boys scored significantly higher on three resilience factors: personal competence, structured style, and family cohesion. No significant differences were found on social competence and social resources. Generally, the gender differences presented small to medium effect sizes, but strong gender differences were found on depressive symptoms (Cohen’s d .57).
Results of the correlation analyses are presented separately for gender in Supplemental Table 2. Significant positive correlations were found between stress, depression, and anxiety. All resilience factors were significantly inter-correlated and showed significant and moderate negative associations with depression, anxiety, and stress. In girls, age showed significant positive weak correlations with depression, stress, social competence, and social resources. In boys, age showed significant negative correlations with two of the resilience factors: structured style and family cohesion.
Regression analysis for variables explaining depression and anxiety
The results from the hierarchical multiple regression analyses are presented in Table 1. When examining the regression model with depression, gender showed a significant association with depression (β = .28) in the first step of the model, where girls scored higher than boys. A positive weak, significant association (β = .08) was found between age and depressive symptoms in the second step. In the third step, a strong, significant positive association was found between stress and depressive symptoms (β = .57) controlled for gender and age, where stress explained 31 percent of the variance in depressive symptoms. When looking at the resilience factors in step 4, personal competence was significantly negatively related to depressive symptoms (β = −.24) controlled for gender, age, and stress; the other resilience factors were non-significant. In the last step, summing up the whole model, stress showed a strong positive association with depressive symptoms (β = .49), whereas personal competence showed a negative association with depressive symptoms (β = −.17); all other associations were non-significant, the interaction effects included. In total, the model explained 46 percent of the variance in depressive symptoms.
Summary of the hierarchical regression analysis for variables associated with symptoms of depression and anxiety.

SE: standard error.
p < .05; **p < .01; ***p < .001.
In the regression model with anxiety, gender was significantly associated with anxiety in the first step of the model, where girls scored higher than boys (β = .17). Age was not significantly associated with anxiety in step 2. Stress showed a significant and positive association with anxiety (β = .42) in step 3, explaining 17 percent of the variance. When entering the resilience factors in the fourth step, personal competence (β = −.29) and structured style (β = −.08) showed significant negative associations with anxiety, controlled for gender, age, stress, and resilience factors. When looking at the last step of the model, gender (β = .12), age (β = −.05), stress (β = .29), personal competence (β = −.16), and social support (β = −.13) were significantly associated with symptoms of anxiety. The majority of the interaction effects were non-significant, except gender x personal competence (β = −.16) and gender x structure style (β = −.12), where the associations were stronger for girls than for boys (see Figure 1). Totally, the model explained 31 percent of the variance in anxiety.
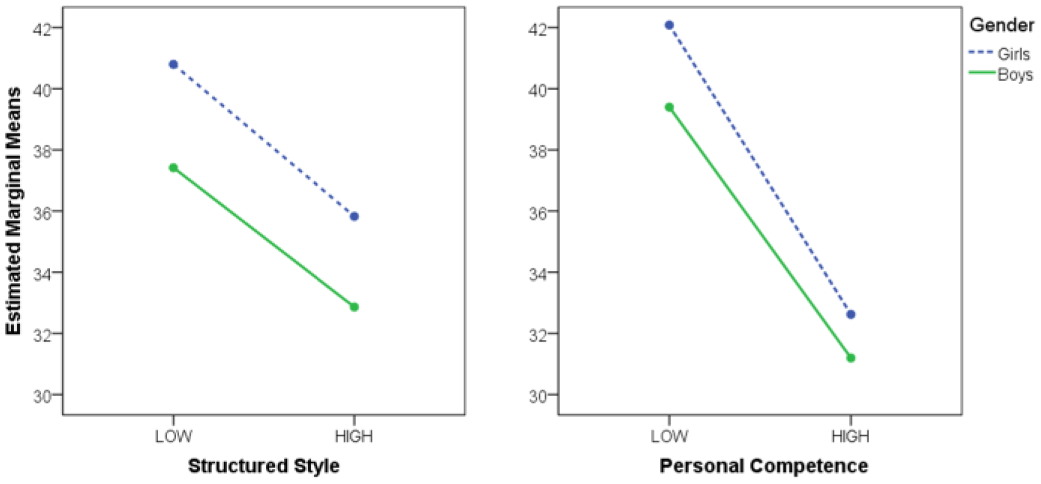
Interaction effects of gender by structured style and gender by personal competence in relation to symptoms of anxiety.
Discussion
The results of this study illustrate how the different dimensions of resilience may contribute to understanding the relation between stress and emotional symptoms in a sample of adolescents from 13 to 18 years old. The initial analyses showed that girls scored higher than boys on stress and symptoms of depression and anxiety. Boys scored higher on the resilience factors including personal competence, structured style, and family cohesion, whereas no significant differences were found on social competence and social resources. The gender differences found on resilience are in accordance with previous findings using the same resilience measure, showing that boys seem to rate themselves higher than girls, especially on personal competence (Hjemdal et al., 2006a, 2011; Von Soest et al., 2010). The gender differences on the other resilience dimensions seem to vary, indicating that adolescents’ self-perception of resilience is a dynamic and variable characteristic during adolescence (Hjemdal et al., 2006a, 2011; Skrove et al., 2013; Von Soest et al., 2010).
The female preponderance of depressive symptoms (especially) and anxiety during adolescence is among the most robust findings in the field of psychology (Hankin, 2009; Thapar et al., 2012). Explanation for this difference is complex and includes the combination of affective (emotional reactivity, sensitivity), biological (genetic vulnerability, pubertal timing, and development), and cognitive (cognitive style, rumination) factors, in interaction with gender role intensification and stress exposure during adolescence (Essau et al., 2010; Hyde et al., 2008).
The present findings of gender differences on stress correspond with previous studies showing that girls seem to report higher stress level than boys (Byrne et al., 2007; Moksnes et al., 2010a). Furthermore, the present results showed that adolescents who reported higher levels of stress also reported more symptoms of depression and anxiety, where stress explained more of the variance in symptoms of depression than of anxiety. Meanwhile, no significant interaction effects of gender by stress were found on any of the outcome variables. The findings thus contradict previous studies showing that girls appear to be more vulnerable to the negative psychological health effects of stress than boys (Charbonneau et al., 2009; McLaughlin and Hatzenbuehler, 2009; Moksnes et al., 2014). However, the results clearly correspond with studies showing that the experience of cumulative and simultaneous stressors is related to symptoms of depression (especially) and anxiety during adolescence (Charbonneau et al., 2009; McLaughlin and Hatzenbuehler, 2009; Moksnes et al., 2010b). The personal evaluations of the individual and environmental resources one possesses, as well as the perceived importance of the stressor, are fundamental for the individual impact of the stressor and for the response, which has profound impact on the health outcomes of stress. However, one should be aware of the possibility of reciprocal associations. Just as stress experience may lead to higher levels of anxiety and depression, it is equally possible that anxiety and depressive symptoms can lead to increased stress, leading to spiraling negative effects.
The results from this study showed that higher personal competence is significantly related to lower levels of depression and anxiety, whereas higher social support is significantly related to lower levels of anxiety, controlled for the other variables. Although boys scored higher on personal competence and structured style, the significant interaction effects found of gender by personal competence and gender by structured style shows that personal resilience characteristics may affect boys’ and girls’ emotional health differently, where stronger associations were found for girls than for boys. Personal competence reflects having confidence in own abilities and judgments, and having realistic expectations, whereas structured style refers to being organized and having clear goals and plans before undertaking activities. These personal characteristics may strengthen girls’ perception of predictability, coherence, and self-confidence, which seem to be an important protective factor in relation to anxiety symptoms. The significant findings can also relate to differences in gender role expectations and confidence regarding how girls and boys perceive and judge their personal resources and abilities. In total, the resilience factors only explained 6 percent of variance in depressive symptoms and 10 percent of the variance in anxiety, which are in line with a study of Hjemdal et al. (2011), where resilience explained between 9 and 16 percent of the variance in symptoms of depression and anxiety in adolescents. This study tested the role of each individual resilience factor while controlling for the influence of the other factors, which may contribute in explaining the weak variance of each resilience factor in this study. Overall, most of the variance accounted for by resilience could be attributed to the direct relationship between resilience (especially personal competence and social support) and emotional symptoms controlled for stress levels (Hjemdal et al., 2007, 2011; Skrove et al., 2013).
The results supported the hypothesis of a compensatory role of resilience where the protective resources of resilience operate irrespective of stress levels (compensation). The results are in line with previous findings showing that of the five resilience factors, personal competence and social support seem to explain most of the variance in relation to depression and anxiety (Hjemdal et al., 2007, 2011). The protective element of personal resilience characteristics has been associated with displaying more confidence in own abilities and judgments, having self-efficacy and realistic expectations (personal competence). Furthermore, this resilience characteristic is recognized by preferences of having and following routines, being organized, and crafting clear goals and plans before undertaking activities (structured style). The protective element of social support addresses the availability of support from family and peers, and furthermore, whether one can turn to someone outside the family for help (Hjemdal et al., 2007; Von Soest et al., 2010). Individuals with higher levels of resilience effectively manage to use skills available to them to cope with challenging situations, which is an important protective resource in relation to emotional functioning.
The findings contribute to the research field by providing insight into the significant role of stress experience for emotional symptoms in adolescents. The results also show the unique role of five different resilience factors in association with stress and emotional symptoms and how the strength of the associations differs between gender across a broad age span of adolescents. Moreover, based on the findings from this study, it seems logical to presume that facilitation of resilience factors in adolescents, especially personal competence and social support, is important in the promotion of positive psychological functioning despite being exposed to significant stressors. The results also indicate that personal resilience characteristics recognized by personal competence and structured style are especially relevant for girls’ experience of anxiety symptoms, suggesting gender-specific strategies could be relevant. It is a reason to believe that an important strategy for promoting resilience resources is to integrate them into developmental contexts in adolescents’ daily life, such as in the school context, which represents a natural setting where adolescents interact with peers and adults and where one can work on universal and targeted strategies. Based on the present and earlier findings, there is a reason to believe that this would contribute in facilitating positive coping in times of stress and promote positive emotional functioning among adolescents.
Strengths and limitations
A strength of this study is the large sample size and high response rate. The study also builds on a strong theoretical foundation and uses well-validated instruments. However, the cross-sectional nature of this study is an obvious limitation and precludes causal interpretation of both main and interaction effects. The study combines both state constructs for the assessment of emotional symptoms and scales that asks about adolescents’ experiences of resilience during the last month and stressor experience during the last year, which may potentially affect how adolescents perceive and answer the different scales. Also, the results do not allow for firm conclusions with regard to clinical levels of stress, emotional affect, or disorder. Nevertheless, we believe that the results are relevant for levels of emotional affect that represent a significant impairment of the individual’s psychological well-being. All data were derived from self-report measures that require that adolescents are at a level of cognitive development where they are able to reflect and understand concepts of health and illness and are thus able to give valid and reliable evaluations. There are no corroborative data from others (parents, teachers, peers) with which to compare the present results. It should be acknowledged, however, that all such data might be more prone to bias due to the possible influence of social desirability factors. The study did not include a category of lesbian, gay, bisexual, transgender, and queer (LGBTQ) for participants to report instead of identifying with their biological sex. This would potentially have strengthened the study as it is established that adolescents who identify as LGBTQ experience higher levels of stress, anxiety, and depression (Collier et al., 2013; Kelleher, 2009). The large sample size and high response rate in this study can be an important protector against the influences of potential random errors related to self-reporting.
Conclusion
This study showed that girls scored higher on stress and emotional symptoms than boys and boys scored higher on the resilience factors personal competence, structured style, and family cohesion. Stress was significantly positively associated with both symptoms of depression (especially) and anxiety controlled for gender, age, and resilience factors. Of the five resilience factors, personal competence was significantly and negatively associated with both depression and anxiety, whereas social support showed a significant negative association with symptoms of anxiety. Significant interaction effects were found between gender by personal competence and gender by structured style, where the associations were strongest in girls. The interaction effects of stress by resilience factors were not significant, supporting a compensatory role of resilience in relation to stress and emotional symptoms. The findings may contribute as a basis for further investigation of the role of resilience in longitudinal studies, intervention studies and in the development of resources-strengthening and potentially gender-specific intervention programs for adolescents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.