
Abstract
An understanding of what variables are involved in a better adjustment to chronic disease makes it possible to implement more suitable community healthcare interventions. It also allows the design of educational programmes aimed at increasing the independence of these patients, thereby enabling them to achieve a better health status. Both the personality and the resilience of the patient have been shown to play an important role in the process of adjusting to the new living conditions that result from having a chronic disease. Yet, to date, little research has been conducted in this area. This study uses structural equation modelling to explore the relationships among the personality factors, resilience and the variables of adjustment to disease (i.e. quality of life and level of self-care). The sample consists of 125 patients with a drainage enterostomy. Results show that the relationship model with the best fit is the one that considers resilience as a mediating variable in the relation between personality and disease adjustment variables. The implications of the findings and the limitations of the study are also discussed.
Introduction
Understanding the mechanisms underlying adaptation and adjustment to highly stressful situations, as is the case of suffering from a chronic disease, is becoming increasingly important in the scientific world, as a result of the change in tendency towards a higher incidence of chronic diseases (Bähler et al., 2015; García-Conde, 2014).
This changing tendency is also a result of earlier diagnoses, improved surgical techniques and adjunct therapies, which have allowed acute diseases that were formerly considered fatal to now become chronic illnesses with a longer life expectancy (Sociedad Española de Oncología, 2014). This is the case of inflammatory bowel diseases or colon cancer, where one of the main consequences of their surgical treatment is a drainage enterostomy. Hence, the number of patients around the world with a drainage enterostomy is very high and is rising from year to year. In fact, in the year 2005, the prevalence of persons with an ostomy in Spain was estimated to be 1.5 per thousand inhabitants, that is to say, around 60,000 people (Cobos et al., 2013). But in 2014, the number of new cases of patients with a drainage enterostomy was estimated to stand at about 13,329 per year (Cancio López et al., 2014). Following this same line are the data from the studies conducted by the United Ostomy Associations of America, which in 2012 estimated that there were over 700,000 people with a drainage ostomy in America (Grant et al., 2013).
The magnitude of the problem, the increased prevalence and the incidence of persons who end up with a drainage enterostomy justify the growing interest of researchers in understanding everything related with these patients’ process of adjusting to the disease so as to be able to achieve better disease management and improve their quality of life (QOL; Araujo and Decesario, 2014).
Adjustment to disease in patients with an enterostomy
Becoming someone with a drainage enterostomy has a strong impact on a patient’s daily life since after coping with major surgery, they then have to carry a device that collects their faeces. In consequence, the patient has to develop new self-care skills in order to regain their autonomy and competence (Araujo and Decesario, 2014; Liao and Qin, 2014). The fact they have a drainage ostomy turns them into chronic patients and produces a strong physical, psychological and social impact, thus making it necessary to implement certain adaptation mechanisms that have a decisive effect on how they cope with their new situation (Bonill et al., 2014; Kenderian et al., 2014).
To measure adjustment to disease, healthcare professionals use a series of health indicators. The QOL of patients with a drainage stoma and the level of self-care of the stoma appear to be the most important health indicators when it comes to predicting the level of adjustment to their new condition (Cheng et al., 2014).
Personality and adjustment to disease
In the comprehension of what factors affect people’s adjustment to stressful situations, personality psychology offers empirical evidence of the existence of a close relationship between personality and health measures, as well as an influence of the personality traits on efficiency in disease management (Weston and Jackson, 2014). In particular, it has been shown that the clinical variables do not have as much influence on the perceived level of QOL and autonomy in self-care as some other psychological variables, especially personality. Some studies reveal that personality accounts for over 60 per cent of the variance in the perception of the QOL of chronic patients (Glavi et al., 2014; Rassart et al., 2013). Personality is considered a determining factor in coping; since it predisposes the person to choose to use certain coping strategies rather than others, it has an influence on how people think, feel and act and, consequently, affects their perception of health outcomes, such as the perception of QOL and the level of self-care (García-Conde, 2014).
In particular, from the theoretical framework of the Big Five personality traits, previous studies have shown that there is a personality profile that theorists call distress (high scores in Neuroticism and low scores in Extraversion, Agreeableness, Conscientiousness and Openness), which, in persons with chronic diseases, is associated to poor responses in disease self-management programmes. Moreover, there is a correlation between personality and the level of adjustment to the chronic condition that goes beyond the effects of socio-demographic (e.g. sex, age) and clinical variables (e.g. complexity of the disease) (Rassart et al., 2013).
Resilience and adjustment to disease
A construct that is being incorporated included on an increasingly more frequent basis in the research conducted in this area in order to understand why some people adapt to severe chronic stress better than others is that of resilience. Within the domain of chronic diseases, resilience stands at a meeting point between health psychology and positive psychology, since it considers the health–illness processes from a perspective of positive promotion and intervention. It is also located within the emerging paradigms that attempt to provide an answer to the shortcomings of the biopsychosocial model when it comes to understanding the health and sickness process in a linear manner. We are referring to complex thinking and to chaos and fractal theories, which conceive disease as a non-linear, complex, multicausal phenomenon resulting from the auto-eco-organisation processes emerging from the interrelation among systems. From this perspective, resilience is understood as a dynamic process, which is not only the result of adding up the different risk or protective factors but is also a consequence of certain interactions among factors that yield other emerging factors which, in turn, continue to interact and give rise to others. Within a constructionist vision, resilience is defined as the result from a process of negotiation undertaken between a person and their environment for the resources needed to define themselves as healthy. According to these definitions, resilience is considered to be the result of a mechanism that empowers the individual in the face of adversity (García and Dominguez, 2013).
More specifically, one of the pioneering researchers in the study of resilience and its relationship with adjustment to chronic disease was Bonanno (2004), who defined resilience as the capacity of adults who have been exposed to traumatic events to maintain relatively healthy and stable levels of psychological and physical functioning, as well as the capacity for generative experiences and positive emotions. In his research on people with severe diseases, Bonanno identified four prototypical long-term patterns or responses that most people present as a response to the stress of suffering a serious disease. These patterns were resilience, chronic dysfunction, recovery and delayed reaction. In this way, he highlighted the difference between recovery and resilience, since recovery from traumatic events is associated with an increase in psychological problems over a period of time, and the resilience pattern is characterised by the search for social support, carrying on with life and accepting the circumstances with hope (Garcia-Dia et al., 2013; Ho et al., 2010).
Many studies have also been conducted on the relationship between resilience and different health indicators in patients with chronic diseases. Thus, for example, this correlation has been studied in women diagnosed with rheumatoid arthritis and osteoarthritis (Sturgeon et al., 2014) and with populations with type 2 diabetes and spinal cord injuries (Rudow et al., 2014). All these studies conclude that resilience is related with factors such as self-care, treatment compliance, health-related QOL, as well as perception of the disease (Bowen et al., 2003; Costanzo et al., 2009; Haase et al., 2014; Harris et al., 2010; Lee et al., 2007; Liu et al., 2012; Molina et al., 2014; Ong et al., 2009; Wu et al., 2017).
Likewise studies conducted with cancer patients show that resilience is positively correlated with mental health indicators, such as emotional health and well-being, satisfaction with life, self-esteem, social adaptation and social support. Conversely, negative correlations have been found with negative emotions, depression and anxiety, vulnerability to stress and distress (Min et al., 2013; Yu et al., 2015). This has led to a sharp growth in the number of resilience intervention programmes for chronic patients over the last 15 years (Fombuena et al., 2015; Molina et al., 2014; Perna et al., 2015; Shamaskin-Garroway et al., 2015)
Personality and resilience in the understanding of adjustment to disease
The understanding of individual differences in adaptation to disease has been addressed from personality psychology for decades. Nevertheless, today the resilience perspective is becoming increasingly more important both in clinical practice and in the development of community health importance. This is due to the results from studies about adaptation to stressing phenomena, which have shown that most people tend to overcome exposure to traumatic events without later developing any mental disorders. Thus, the personality and resilience approaches have coexisted for years as a means to account for the differences in adaptation to stressful situations, but few studies have explored the relationship existing between these constructs and how this relation influences the process of adaptation. In the studies in which this relationship has been analysed, the conclusion is that resilience is negatively correlated with neuroticism and positively correlated with extraversion. Moderately positive correlations have also been found between resilience and the other dimensions of the Big Five model, such as agreeableness, openness and conscientiousness (Hjemdal et al., 2012; Lü et al., 2014; Rudow et al., 2014; Sarubin et al., 2015).
If we focus specifically on the studies which attempt to provide an understanding of the relationship between these two constructs and adjustment to stressful situations, some researchers have tried to study which model best predicts adjustment, although the findings are inconclusive. Some support the notion that resilience adds little to account for the variance of the adaptive behaviours explained by personality (Waaktaar and Torgersen, 2010). Others, however, have found that resilience explains this adjustment in a clearer way than personality (Hjemdal et al., 2012).
In the study of what factors or variables best predict adjustment to a stressor, in addition to these two tendencies, that is, that which defends personality factors and that which defends resilience, there is also a third which considers resilience as a mediator between the antecedents and the consequences of adaptation to disease (Terrill et al., 2014). This suggests that the antecedent variable precedes the mediating variable and that both of them precede the appearance of the outcomes. This mediating role has been confirmed in several studies with a normal population. In particular, in a study on emotional exhaustion related with burnout, the authors analysed the relations between personality under the theoretical model of the Big Five and resilience, according to Richardson’s model, and the emotional exhaustion dimension. They found evidence for the mediating effect of resilience but it only occurred with the conscientiousness dimension. Using the same theoretical model of resilience and personality, Campbell (2006) found the mediating function of resilience between anxiety and four of the five personality factors, namely, agreeableness, openness, conscientiousness and neuroticism (Ai and Hu, 2016; Bernabé and Botia, 2016; Shi et al., 2015). In another study conducted with a population of university students, a mediating effect of resilience was also found between positive affect and two of the five dimensions: neuroticism and extraversion (Lü et al., 2014). Resilience has also been seen to mediate between the perception of pain and depressive symptoms, between depressive symptoms and suicidal thoughts, as well as between stressful life events and mental health (Lü et al., 2014; Shi et al., 2015).
Current study
In the light of these studies, on one hand, we can see the theoretical framework that relates personality and adjustment to chronic disease (Waaktaar and Torgersen, 2010) and, on the other hand, the theoretical framework that relates the process of resilience to adjustment (Hjemdal et al., 2012). There is also scientific evidence of the relationship between personality and resilience (Lü et al., 2014; Peng et al., 2012; Rudow et al., 2014; Sarubin et al., 2015; Yu and Zhang, 2007). All this is linked with the theoretical perspective that orients us towards the study of the variables that mediate in adjustment to disease, and the need to measure this latter by means of the two health indicators (Cohen et al., 2014). These indicators, which are becoming increasingly more significant in the scientific literature, are QOL and the level of self-care. This led us to posit the following research question, given the scarcity of previous studies on this issue: what is the role played by resilience in the relationship between personality and adjustment to disease in patients with a drainage enterostomy? Our initial hypothesis is that resilience plays a mediating role in the relationship between the personality variables and the disease adjustment variables, such as the perception of QOL (general and specific) and the level of self-care.
Method
Participants and procedure
We obtained approval from the Spanish Agency for Medicines and Healthcare Products of the Spanish Ministry of Health, and also from two research ethics committees (RECs) as well as authorisation to access the sample from the management of four hospitals in the health department in which the study was conducted. Inclusion criteria were that patients had to be over 18 years of age, and to have been colostomised/ileostomised in one of the hospitals with a digestive surgery service and stomal therapy nursing unit in the province of Castellón. A further criterion was that, when the study was conducted, they should have already completed a period of post-surgery adaptation to their enterostomy of at least 3 months. This criterion was added following the recommendations of previous studies on the adjustment of patients with an enterostomy (De Frutos et al., 2011).
Exclusion criteria were that patients were in the terminal phase of their disease, and that they did not understand Spanish. Cognitive impairment was also taken into account as another exclusion criterion. Hence, patients who obtained scores below 24 on the Mini-mental Status Exam test (Folstein et al., 1975) were excluded from the study. The last exclusion criterion was that, in addition to a drainage enterostomy, patients also had to have a urostomy.
Initially our sample consisted of 185 patients who had had a drainage enterostomy for more the three months. After applying the eligibility and exclusion criteria, we were left with 125 patients, who were first interviewed and then went on to complete the measurement instruments (n = 80 males and n = 45 females).
Their ages ranged from 36 years to 87 years with a mean age of 66.72 years (standard deviation (SD) = 11.85). Moreover, 80 per cent of the sample was over 60 years of age, because this kind of pathology is more frequent in older people. Of the total, 85.6 per cent were patients diagnosed with colon cancer, 7.2 per cent of them had been diagnosed with an inflammatory intestinal disease (i.e. Crohn’s Disease or Ulcerative Colitis), 3 per cent had a diagnosis of Diverticulitis and the remaining 4.2 per cent underwent surgery due to other causes (i.e. endoscopic perforations, traumatic injuries resulting from a road accident and intestinal infarction). With regard to the type of enterostomy, the majority of them had a colostomy (81.6%), while 18.4 per cent had an ileostomy. Most of the patients (80%) claimed they were autonomous as regards caring for their stoma and only 16.8 per cent performed irrigations on a regular basis. 83.2 per cent of the patients with an enterostomy did not report having had any kind of complication.
Instruments and measurements
Demographic and basic medical information
A number of socio-demographic variables were collected (e.g. sex, age, reference hospital, marital status, education), together with the clinical variables (e.g. medical diagnosis, type of stoma, time frame, level of the stoma, irrigations, self-care or complications).
Personality
This was measured using the reduced Spanish version of the NEO Five-Factor Inventory (NEO-FFI; Costa and McCrae, 1999). This instrument has a total of 60 items, 12 for each of the Big Five factors (Neuroticism, Extraversion, Openness, Agreeableness and Conscientiousness) by means of a Likert-type scale ranging from 0 (Not at all) to 4 (Totally).
Resilience
This was measured by means of the Spanish version of the Connor–Davidson Resilience Scale (CD-RISC) translated from the original English by Bobes et al. 2001. The scale consists of 25 items measured by means of a Likert-type scale ranging from 0 (Not at all) to 4 (Nearly always). The exploratory factorial analysis performed by Connor and Davidson (2003) identified five factors that they called (1) personal competence, high standards and tenacity; (2) trust in one’s instincts, tolerance of negative affect and strengthening effects of stress; (3) positive acceptance of change and secure relationships; (4) control; and (5) spiritual influences. The authors, however, considered it a unidimensional scale. The scale ranged between 0 and 100. It has no set cut-off point, and thus, the higher the score, the higher the person’s level of resilience is.
General QOL
This was measured by means of the Multidimensional QOL Questionnaire (Quality-of-Life Index (QLI)), which consists of 10 items each corresponding to a general QOL indicator and which are measured on a Likert-type response scale that ranged from 1 (Bad) to 10 (Excellent). These indicators refer to physical well-being, psychological and emotional well-being, self-care and independent functioning, occupational functioning, interpersonal functioning, social and emotional support, communitarian and services support, personal realisation, spiritual satisfaction and global perception of QOL (Mezzich et al., 2011).
Specific QOL for enterostomy patients
This was measured by means of the Stoma-QOL (QOL Questionnaire for patients with colostomy or ileostomy) (Prieto et al., 2005). It measures four areas of the life of patients with a drainage enterostomy, namely, sleep, sexual activity, relationships with the family and close friends and social relationships with persons other than relatives and close friends.
Self-care
This was measured by means of the Specific Self-Care for Ostomised Patients Questionnaire (CAESPO) (Collado, 2015), created to measure self-care among enterostomy patients in the Spanish population. The questionnaire has been validated in the same sample used in this study. In this validation, and in consonance with the theoretical construct of the general theory of self-care, all the self-care dimensions appeared in three clearly distinct factors: General, Developmental and Specific self-care, as well as some second-order factors within these, concerning knowledge, practice and interest.
Data analysis
To adapt the measurement instruments referring to personality, resilience and QOL to this sample of patients, we followed the indications of George and Mallery (2003) as regards the classification of the values of the Cronbach’s Alpha Coefficient (Excellent: >.9; Good: .8–.89; Acceptable: .7–.79; Questionable: .6–.69; Poor: .5–.59; and Unacceptable: <.5). A confirmatory factorial analysis (CFA) was performed and the model fit was evaluated by means of structural equation modelling (SEM) using EQS 6.1 and following the robust indices. Although SEM is certainly a large-sample technique (Kline, 2011), it can be applied to samples below 200 when the population from which a sample is hypothesised is restricted in size, as might be the case in medical research (Barrett, 2007), such as patients with a drainage enterostomy. Moreover, due to the specific characteristics of this population (i.e. their health problems were irreversible in some cases), it was very difficult to obtain a larger number of participants in the study. Thus, a model is said to fit when the Satorra–Bentler χ2 is not significant (p ⩾ .05), and the Bentler–Bonett Normed Fit Index (BB-NFI), Bentler–Bonett Nonnormed Fit Index (BB-NNFI), Comparative Fit Index (CFI) and Incremental Fit Index (IFI) have to be higher than .9 (if the NFI is not higher, then the NNFI must be). Additionally, the root mean-square error of approximation (RMSEA) must be below .08 (Herrero et al., 2011).
The descriptive analyses of all the variables included in the study (i.e. resilience and personality variables and general and specific health QOL variables) were performed using the software package SPSS v21.
In order to determine whether the theoretical models fit or not, SEM was employed, using EQS 6.1 and following the robust fit indices. Personality, resilience, QOL and self-care variables were included. The factorial scores were used for all the variables obtained through the fit of the instruments.
Several theoretical models were evaluated following the literature. The first model (M1) is the one that relates neuroticism negatively and extraversion positively with self-care with three indicators (General, Developmental and Specific Self-care) and QOL with three other health indicators (Stoma-QOL personal dimension, Stoma-QOL social dimension and QOL) (Samartzis et al., 2014). The second model (M2) holds that there is a personality profile, in accordance with the Big-Five personality model, which correlates with poorer adjustment to a chronic disease. This profile, called distress, includes persons with high Neuroticism and a low score on Extroversion, Agreeableness, Conscientiousness and Openness (Jerant et al., 2010). In the third model (M3), resilience is positively related with variables such as self-care and QOL (Wu et al., 2015). The fourth model (M4) represents the mediating effect of resilience among the personality dimensions of Neuroticism, Extraversion and adjustment to disease (Lü et al., 2014; Shi et al., 2015). And, the fifth model (M5) postulates that resilience mediates between the personality profile that includes the Big Five and the adjustment to disease variables (Shi et al., 2015).
To determine which of the structural models best explains the relation among the variables, the next step was to determine the difference among the chi-square (χ2) of the models that fit and the difference in the degrees of freedom of those models. After obtaining the differences, a χ2 table was used to evaluate whether the difference was significant or not and thus to determine which was the one with the best fit.
Results
Adaptation of the measuring instruments (confirmatory factor analysis)
Adaptation of the NEO-FFI (Costa and McCrae, 1999). This questionnaire was adapted with the sample in this study. Hence, for the fit of the CFA of the inventory, the starting point was taken as the structure of the test whose original theoretical model had five factors and SEM was performed. For the best fit of the instrument, it was necessary to remove certain items from the different factors.
Adaptation of the CD-RISC by Connor and Davidson (2003) and translated into Spanish (Bobes et al., 2001). The CD-RISC was adapted to our study sample by means of CFA and then SEM.
Adaptation of the Multidimensional QOL Questionnaire (QLI) (Mezzich et al., 2011). This instrument was also adapted to the study sample by means of CFA and then its SEM.
Adaptation of the Stoma-QOL (QOL Questionnaire for patients with colostomy or ileostomy) (Prieto et al., 2005). This resulted in a questionnaire made up of 18 items with one principal factor and a secondary bifactorial structure that was different from the original one.
Descriptive analyses
Table 1 shows the descriptive statistics of the NEO-FFI instrument. The direct scores on the different factors were converted into typical scores (t) or transformed with the aim of being able to compare them with the normal Spanish population, following the criteria from the NEO-FFI handbook (Costa and McCrae, 1999). Thus, in both females and males in our sample, the greatest distancing, towards scores lower than the central point, was obtained on the factors Extroversion, Openness and Conscientiousness. And, in both cases, the scores on Neuroticism tended towards higher scores.
Mean and standard deviations on typical scores (t) according to the criteria for NEO-FFI sex, on scores out of 100 points on the CD-RISC, QLI and Stoma-QOL (N = 125).
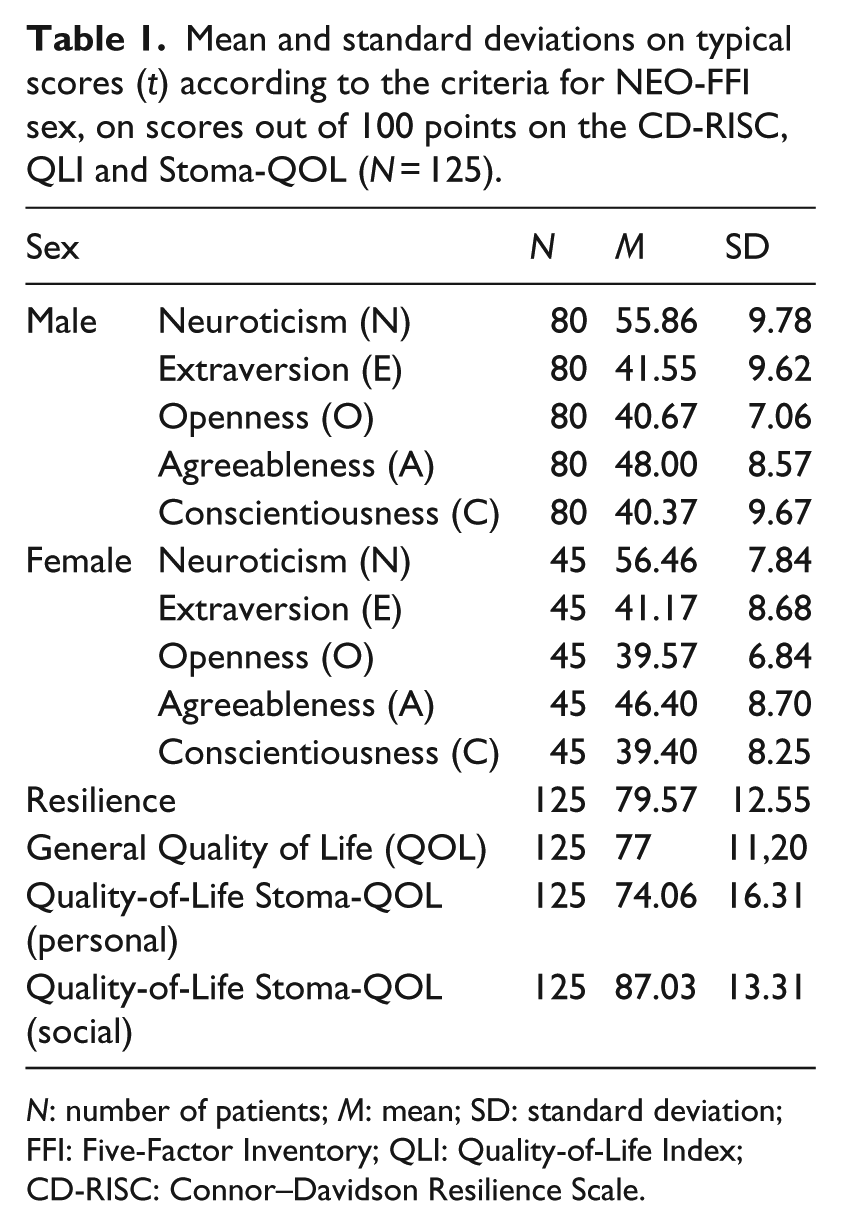
N: number of patients; M: mean; SD: standard deviation; FFI: Five-Factor Inventory; QLI: Quality-of-Life Index; CD-RISC: Connor–Davidson Resilience Scale.
Table 1 also shows the descriptive statistics of Resilience (CD-RISC), of the QLI, and of the Stoma-QOL, after converting the scores of the data into scores out of 100. With regard to resilience, we can see that the mean of our sample is considerably lower than that of the general US population (80.7), but somewhat higher than the clinical population (71.8) or than that with post-traumatic stress disorder (52.8) (Connor and Davidson, 2003).
The authors of the QLI instrument do not propose any cut-off point, but we can see that the mean of our sample presents a perception of a high QOL. With respect to Stoma-QOL, according to the authors’ criteria, the level of QOL perceived by the patients who participated in the study was Good (result 70%–100%) (Juul and Prieto, 2008).
Table 2 shows the values of the Pearson correlation among the factors on the NEO-FFI, CD-RISC, QLI, Stoma-QOL and CAESPO scales. As expected, the results of the Pearson correlation show that there is a significant negative correlation between Neuroticism and Resilience, as well as with the social dimension of the Stoma-QOL and developmental self-care. Extraversion was positively and significantly correlated with Resilience and with the specific self-care and the social dimension Stoma-QOL, but negatively with the personal dimension of the Stoma-QOL.
Intercorrelation Pearson correlation among the factors of the NEO-FFI, CD-RISC, QLI, STOMA_QOL and CAESPO scales (N = 125).

QOL: quality of life; QLI: Quality-of-Life Index; FFI: Five-Factor Inventory; CD-RISC: Connor–Davidson Resilience Scale.
p < .10, **p < .05,
Also as expected, there is a significant positive correlation between Resilience and nearly all the variables of adjustment to disease, that is to say, QOL and level of self-care.
Testing the research model: the mediating role of resilience
In this section, we present the results for the different SEM that were performed in order to analyse the hypothesised relationships; accordingly, Table 3 shows the fit indices of the models.
Fit of the research models (N = 125).
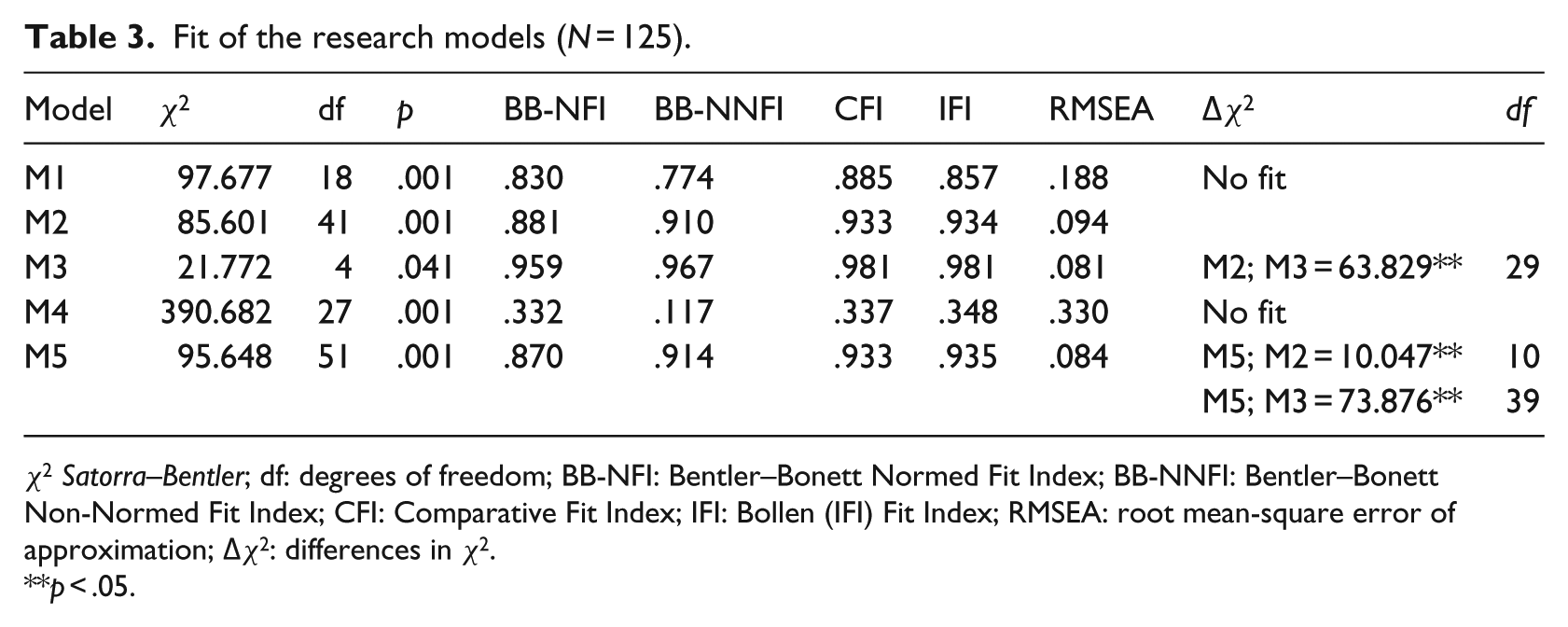
χ2 Satorra–Bentler; df: degrees of freedom; BB-NFI: Bentler–Bonett Normed Fit Index; BB-NNFI: Bentler–Bonett Non-Normed Fit Index; CFI: Comparative Fit Index; IFI: Bollen (IFI) Fit Index; RMSEA: root mean-square error of approximation; Δχ2: differences in χ2.
p < .05.
The first model (M1) was the one that corresponded to the theoretical framework which related the personality dimensions of Neuroticism and Extraversion to adjustment to chronic diseases. On testing the Model and its goodness-of-fit, we saw that this model did not fit because the BB-NNFI was .774 and ought to have been above .90; likewise, the RMSEA ought to have been below .08 and was .188. Hence, this model could not be compared to the others.
On testing M2, the latent variable was taken as personality with five indicators or observed variables (Neuroticism, Extraversion, Openness, Agreeableness and Conscientiousness), self-care with three indicators (General, Developmental and Specific Self-care) and QOL with another three indicators (Stoma-QOL personal dimension, Stoma-QOL social dimension and QOL). On examining their goodness-of-fit, we saw that for this model, all the indices fitted well. Hence, the model of the relationship between personality as a profile and the variables of adjustment to disease (QOL and self-care) fitted adequately.
On evaluating M3, in which resilience was used as the observed variable, and self-care with three indicators or observed variables and QOL with three other indicators were taken as the latent variables, we saw that their goodness-of-fit indicated that all the indices fitted. The model of the relationship between resilience and the adjustment to disease variables (QOL and self-care) therefore fitted adequately.
On evaluating M4, where we used three observed variables, Neuroticism, Extraversion and Resilience, and self-care with three indicators or observed variables and QOL with another three indicators as the latent variables, we saw that this model did not fit, since the BB-NFI, BB-NNFI, CFI, and IFI indices were all below .9 and the RMSEA ought to have been below .08 and it was .330. Hence, this model could not be compared to the others.
On testing M5 (see Figure 1) and checking its goodness-of-fit, we saw that in this model, all the indices fitted. In the structural equation models (SEM), in order to achieve a better fit of the final model, first it was necessary to remove the developmental self-care indicator from the latent variable self-care and the social dimension of the Stoma-QOL indicator from the latent variable QOL. As a result, the model of the mediation of resilience between personality as a profile of the Big Five and the variables of adjustment to disease (the general and specific indicators of QOL) fitted and was compared to other models to see which one best represented the relationship between the variables.

Structural model of the mediation of resilience between personality (Big Five) and disease adjustment variables (Quality of Life and Level of Self-care).
In order to compare the structural models, we found the difference between the chi-squares of the models to be compared and the difference in the degrees of freedom of those models. After obtaining the differences, they were evaluated on a
Then, on comparing the chi-square of the mediation model M5 with that of M2, we found that the chi-square differential (Δχ2 = 10.047) was greater than the chi-square from the table (χ2 = 18.3070), which allowed us to state that there are differences between the models. Therefore, given these differences, the model that best explained the data was M5, which had more degrees of freedom (df = 51).
Finally, on comparing the chi-square of M5 against that of M3, the value we obtained (Δχ2 = 73.876) was higher than the chi-square from the table (χ2 = 54.5722), which allows us to state that there are differences between the models. The Mediation Model M5 is the one that best explains the relationship among the variables since it has more degrees of freedom (df = 51).
We can thus say that the theoretical model that best explains the relationship among the variables under study is M5, or the mediation model, and it fully satisfies the hypothesis. Resilience mediated in the relationship between personality made up of five indicators or observable variables and the latent variables related to adjustment to disease. These latent variables were the QOL represented by the personal dimension of the indicator health-related QOL and the general QOL, as well as by the latent variable self-care represented by the indicators or observable variables general and specific self-care.
Discussion
The aim of this study was to analyse the mediating role of resilience in the relationship between personality and the adjustment to disease variables, namely, level of perceived QOL and level of self-care in patients with a drainage enterostomy. In previous studies with another type of clinical sample, resilience has been found to play a mediating role between the perception of pain and depressive symptoms. It has also been found to mediate between depressive symptoms and suicidal thoughts, as well as between stressful life events and mental health (Lü et al., 2014; Shi et al., 2015). With regard to personality within the theoretical framework of the Big Five, a mediating effect was found among the personality dimensions of Neuroticism, Extraversion and positive affect (Shi et al., 2015). The results of our study are in line with those obtained in previous work, since, as expected, resilience acts as a mediator between the latent variable personality, made up of the Big Five Factors, and adjustment to disease, consisting of, according to the model, general and specific self-care, in addition to the personal part of specific QOL for stoma patients and general QOL. Hence, the results seem to indicate that a personality profile with low scores on Neuroticism and high scores on the other four factors, that is, Extraversion, Agreeableness, Openness and Conscientiousness, has an indirect effect, that is, mediated by Resilience, upon variables that indicate adjustment to the chronic health situation of having a drainage enterostomy.
One explanation for this result could be that resilience is a mechanism for maintaining both physical and psychological health, as it offsets some of the negative consequences of the difficult times in the disease process (Connor and Davidson, 2003), through the people’s psychological improvement (Lü et al., 2014). The results of this study and from previous research show that resilience can be a key factor in adjusting to stressful situations and thus to chronic diseases (Shi et al., 2015).
The model also shows that the adjustment indicators are the QOL, which is made up of a specific QOL, related to living with a stoma, while in its personal part it refers to the most private, as opposed to the social, domain of the fact of having a stoma and the general QOL. QOL is closely related to the other indicator of adjustment to disease, namely, the level of self-care, consisting of general self-care. Surprisingly, the model indicates that the influence of personality mediated by resilience is negative in the specific self-care component. Perhaps the explanation of this result can also be found in the results of previous studies on the relationship between level of self-care and QOL, whose results reflect a negative correlation in certain aspects of self-care. The explanation given by these authors is that in patients with chronic pathologies, having more knowledge on the matter or even having an excessive amount of information, that is, of intellectual preparation, means an increase in stress for the patient. This has negative repercussions on the QOL (Collado, 2015).
Practical implications
Finally, as a general conclusion to our study, it can be said that Resilience plays a mediating role in the relationship between the five personality factors and the disease adjustment factors, that is, perception of QOL and the level of self-care. This model of the relationship between personality and adjustment to disease, in which resilience plays a mediating role, provides scientific evidence of the need to include interventions and actions aimed at fostering the process of resilience within educational programmes aimed at promoting better management of a drainage enterostomy. This would make it possible to achieve better adjustment to the disease, and therefore, a better prognosis at all levels and in all areas of life, in persons who have to live with a drainage enterostomy despite the initial dispositional conditions.
Limitations and future studies
First of all, one very important limitation is that this study is of a cross-sectional rather than a longitudinal nature. A longitudinal study that focused on examining the relationship among the variables involved in the study prior to performing the operation that left the patient with a drainage enterostomy would shed more light on the matter. Second, and as a limitation related with the methodological aspect and with the sample, selection was performed by intentional or convenience (non-representative) sampling, which was conditioned by the difficulties involved in gaining access to the study population. The recommended sample size for this type of study is more than 200. This study, however, was based on a valid theoretical model and on instruments with strong psychometric properties. Taking this into account, a smaller sample size was acceptable, although more comprehensive studies are needed to confirm these preliminary findings.
Hence, the results of this study point us towards future research in which we will continue with our aim of evaluating and understanding the process of resilience in patients with chronic diseases. We also consider the need to include strategies that arouse and drive the process of resilience with integrated intervention programmes for chronic patients, since we have found that it is a protection factor against other variables or factors that can affect good adjustment to disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.