
Abstract
The objective of the present study was to test if outcome expectancy mediated the relationship between fitness and self-efficacy, perceived stress, and depressive symptoms.Adolescents with obesity (n = 228) completed measures of perceived stress and depressive symptoms at baseline, self-efficacy and outcome expectancy at baseline and 3 months, and fitness at baseline and 6 months. Structural equation modeling was used to analyze the data. Results showed that self-efficacy was positively associated with fitness via outcome expectancies. For females, fewer depressive symptoms were linked to fitness via self-efficacy and outcome expectancies. Exercise interventions that enhance exercise self-efficacy, outcome expectancy, and reduce depressive symptoms may increase fitness.
Introduction
The proportion of North American adolescents who have obesity has increased by threefold over the last three decades to 11.6 percent in Canada (Statistics Canada, 2016) and 20.6 percent in the United States (Ogden et al., 2016). Despite media interventions aimed at increasing exercise, the majority of the North American children and adolescents do not meet physical activity guidelines (The Canadian Society for Exercise Physiology, 2012). This trend is worrisome, as obesity rates in adolescents typically translate into increased obesity rates in adults. Promoting exercise and fitness among adolescents promotes better current and future health (Penedo and Dahn, 2005), offers protection against cardiovascular disease risk factors (Eisenmann et al., 2007; Lee et al., 2012), and improves psychological health (Goldfield et al., 2011). Despite this, research on the psychological and motivational factors associated with exercise and fitness in this population is currently lacking.
One of the most prominent frameworks for understanding exercise behavior is social cognitive theory (SCT), which posits that behaviors are determined by the reciprocal interaction of psychological, environmental, and social factors (Bandura, 1977, 1986, 1997). This framework has been used extensively to model and predict health behaviors, especially in the context of encouraging positive health behavior change (Bandura, 2004; McAlister et al., 2008; Riekert et al., 2014).
While SCT posits several potential determinants of behavior, the most important one appears to be self-efficacy (Bandura, 1977, 1986, 1997). Self-efficacy refers to an individual’s belief that he or she is capable of successfully achieving a given outcome. The application of this construct to exercise (i.e. the belief that one is capable of exercising regularly) has consistently been shown to be a strong, positive predictor of exercise behaviors in children and adolescents (Fisher et al., 2011; Sallis et al., 1992; Van Der Horst et al., 2007). For example, higher levels of exercise self-efficacy have been shown to correlate with higher activity levels in children (Reynolds et al., 1990; Strauss et al., 2001), and this remains true even when controlling for parental support (Fisher et al., 2011), baseline activity levels, and body mass index (BMI; Reynolds et al., 1990).
Another integral component of SCT, outcome expectancy, refers to whether one expects a positive outcome from a given behavior (Bandura, 1998). For exercise, outcome expectancy can take varied forms, including whether people believe exercise will improve their health, their appearance, or their self-esteem. One cross-sectional study reported that lower perceived benefits of exercise was a key determinant in reduced levels of exercise, especially in young females (Garcia et al., 1995). Another longitudinal study based on self-reported activity found that more positive outcome expectancies predicted greater levels of exercise in children, but only for males (Trost et al., 1997). A systematic review of the exercise literature for adolescents found that the perceived benefits of exercise and actual participation were positively correlated for both sexes; however, the authors noted that most of the studies included in the review were cross-sectional in nature and relied on self-reported measures of exercise behavior (Park and Kim, 2008). As others have suggested (Ten Hoor et al., 2015), more longitudinal research is needed regarding the relationship between motivational constructs, exercise behaviors, and health-related outcomes. Such research should look at adolescents in general, take into account sex comparisons, and specifically examine adolescents with obesity that are at higher risk of comorbidities.
Bandura (1997) argued that greater self-efficacy for a given task shapes an individual’s outcome expectancy by making it more likely that he or she will expect positive results. As such, outcome expectancy may serve as a mediator between self-efficacy and behavior by increasing the likelihood that an individual engages in the behavior. For exercise, some support of this has been found in older adults (Resnick, 2001; Resnick and D’Adamo, 1997; Resnick et al., 2000). This mediation relationship has not yet been evaluated in adolescents, with or without obesity, though one might expect similar results as to what has been observed in older adults.
Self-efficacy and outcome expectancy are beliefs that depend on a variety of psychological factors (Bandura, 1986; Clark and Becker, 1998), including perceived stress and depressive symptoms (Bandura, 1989, 2001; Bussey and Bandura, 1999). Bandura (1989) argued that those with lower levels of self-efficacy are more likely to believe that they cannot exert control over their environment and tend to experience more stress. To date, however, results on the relationship between exercise, perceived stress, and exercise self-efficacy have been mixed. One study found that decreased stress was associated with greater levels of exercise for female adolescents, but not for males (Reynolds et al., 1990). Another observed no relationship between exercise and perceived stress in adolescents (Sallis et al., 2000). More recently, a large review of the literature including mainly cross-sectional studies found that stress and exercise were negatively correlated in the majority (about 73%) of studies; however, positive correlations were also reported for both adults and children (Stults-Kolehmainen and Sinha, 2014). More research using longitudinal designs is needed to clarify the relationship between perceived stress and exercise, including identifying the psychological mechanisms by which these variables interact.
While the nature of how perceived stress affects exercise behaviors requires further study, an inverse relationship between depressed mood and exercise behaviors has consistently been shown (Ammouri et al., 2007; Park and Kim, 2008; Wiles et al., 2012). It is likely that the negative self-perception, and lack of motivation that typically accompanies depressive symptoms, leads to decreased self-efficacy (Bussey and Bandura, 1999). Although few studies have looked at this among adolescents, one showed that depressive symptoms had a negative indirect effect on exercise behaviors that was mediated by outcome expectancy (Ammouri et al., 2007). More research is needed on how depressed mood indirectly affects exercise levels, including further studies evaluating whether intermediary SCT variables play a role.
No studies have examined the meditational relationship between exercise self-efficacy, outcome expectancy, and fitness in adolescents. The two main objectives of this study were to assess: (1) whether greater outcome expectancy would mediate the relationship between greater exercise self-efficacy and greater aerobic fitness, as defined by improvements in cardiorespiratory capacity (i.e. VO2 peak), in adolescents with obesity who were participating in the Healthy Eating, Aerobic and Resistance Training in Youth (HEARTY) randomized controlled exercise trial (Sigal et al., 2014); and (2) whether the effects of perceived stress and depressive symptoms on aerobic fitness would be mediated by exercise self-efficacy and/or outcome expectancy. We predicted that greater self-efficacy, lower perceived stress, and fewer depressive symptoms would indirectly lead to greater aerobic fitness via more positive outcome expectancies.
Methods
Participants
Participants were enrolled in the HEARTY trial, a randomized controlled trial designed to evaluate exercise interventions in adolescents with obesity (Alberga et al., 2012; Sigal et al., 2014). Participants were inactive, postpubertal (Tanner stage IV or V) adolescents aged 14–18 years with BMI at or above the 95th percentile for age and sex or above the 85th percentile with an additional diabetes or cardiovascular risk factor (see Sigal et al., 2014). Exclusion criteria were habitual exercise twice weekly for more than 20 minutes per session (other than routine physical education classes), diabetes mellitus (either type), any illness for which exercise would be inadvisable or unfeasible (e.g. uncontrolled hypertension, unstable pulmonary disease, and eating disorders), body weight above 159 kg and/or BMI > 45 kg/m2, cognitive deficits, pregnancy or intention to become pregnant in the next year, inability to communicate in English or French, and the consumption of any performance-enhancing medications. For individuals taking medications that might affect body composition, lipids, or glucose metabolism (e.g. birth control and metformin), participants were required to be taking the same dose as they had for 2 months prior to the trial and to not change dosage throughout. Participants were recruited by posters and print advertisements (e.g. signage on city buses) or via the obesity/endocrinology clinic at the Children’s Hospital of Eastern Ontario. All participants provided written informed consent, and parents co-signed for adolescents who were under the age of 16 years. The ethics boards of the Ottawa Hospital and the Children’s Hospital of Eastern Ontario approved this study.
Measures
Demographic and clinical information
At baseline, participants reported their age, sex, and ethnicity; study staff measured participants’ weight, height, waist and hip circumferences, and Tanner stage.
Exercise self-efficacy
Exercise self-efficacy was assessed at baseline and 3 months using the Exercise Confidence Survey (ECS; Sallis et al., 1988). The ECS has 12 items designed to assess two factors of exercise self-efficacy: resisting relapse (six items, for example, “Continue to exercise with others even if they seem too fast or too slow for you”) and making time for exercise (six items, for example, “Get up earlier to exercise, even on weekends”). Responses are provided on a 5-point Likert-type scale (0 = I know I cannot; 5 = I know I can) and the summed total of all items represents overall exercise self-confidence. Higher values on the ECS indicate greater self-efficacy for engaging in exercise. The ECS has been shown to be reliable and to have high internal consistency, as well as high criterion validity by correlating with reported exercise behaviors (Sallis et al., 1988); Cronbach’s alpha was also high in our sample (α = .85).
Outcome expectancy
Participants’ outcome expectancy was measured at baseline and 3 months with an adapted version of the Outcome Expectancy Attitude Scale (Dishman et al., 2005, 2002). Example items included “It would be fun,” “It would make me more attractive,” and “It would make me better in sports, dance, or other activities.” Responses were indicated on a 5-point Likert-type scale (1 = Disagree a lot; 5 = Agree a lot) and the summed total of all eight items represents overall outcome expectancy. Higher scores indicated greater expected outcomes of exercise. The reliability and validity of this measure has been previously established (Dishman et al., 2005) and was acceptable among the current sample (α = .74).
Depressive symptoms
Depressive symptoms were measured at baseline using the Children’s Depression Inventory, Second Edition (CDI-2; Kovacs, 1985, 2011). The CDI-2 has 27 items designed to assess global depression (total summed score). On each item, participants select 1 of 3 statements, choosing that which is the most appropriate for them (e.g. “All bad things are my fault,” “Many bad things are my fault,” or “Bad things are usually not my fault”). Higher total scores on the CDI-2 indicate greater levels of depressive symptoms; scores about 20 are considered elevated and may warrant follow-up. The CDI-2 has been demonstrated to be reliable and valid in previous studies (Kovacs, 2011) and our sample (α = .90).
Perceived stress
Perceived stress was measured at baseline using the 10-item Perceived Stress Scale (PSS; Cohen et al., 1983). The PSS provides a global measure of perceived stress (total summed score). Example items include “In the last month, how often have you felt nervous or stressed” and “In the last month, how often have you felt that you were on top of things.” Responses are provided on a 5-point Likert-type scale (0 = Never; 5 = Very often). Higher values on the PSS indicate greater perceived stress. The PSS has been found to be reliable and valid (Roberti et al., 2006); Cronbach’s alpha was also high for our sample (α = .85).
Aerobic fitness
Aerobic fitness, defined by changes in cardiorespiratory function, was measured at baseline and 6 months (VO2 peak, in milliliters of oxygen per kilogram of body weight per minute) by indirect calorimetry using a metabolic cart (MOXUS Modular Metabolic System, AEI Technologies, Naperville, IL, USA) during a Balke–Ware treadmill test (Balke and Ware, 1959). The treadmill test was stopped when the participant felt exhausted and indicated that they could no longer continue (i.e. volitional fatigue).
Procedures
Full details of the procedures for the HEARTY trial have been published previously (Alberga et al., 2012). Briefly, after completing a minimum of 13 of 16 sessions during the 4-week supervised exercise run-in period, participants were eligible for randomization into groups: (1) aerobic exercise (using cycle ergometer, elliptical, or treadmill), (2) resistance exercise (using weight machines, free weights, or body weight resistance), (3) combined aerobic and resistance exercise, or (4) diet-only control. All participants received dietary counseling with a dietitian at baseline, 3 months, and 6 months and were prescribed a maximum daily energy deficit of 250 kcal. For those participants in the exercise conditions, an exercise program was prescribed based on their baseline fitness assessments, and exercise sessions were progressively increased in intensity and duration (to a maximum of 45 minutes per session) as the trial went on; the combined group performed both exercise regimens and the duration extended to a maximum of 90 minutes per session. All participants in the exercise groups attended four exercise sessions per week. A personal trainer met with each participant twice per week during run-in, once per week from randomization to 3 months, and once every other week from 3 to 6 months; trainers were not trained to provide behavioral change or motivational enhancement interventions. The main results of the HEARTY trial were that aerobic, resistance, and combined exercise training reduced total body fat and waist circumference, and those assigned to the combined condition had greater decreases than the other conditions (Sigal et al., 2014).
Data analyses
Using IBM SPSS v24, data were cleaned following procedures outlined in Tabachnick and Fidell (2007); we verified normality of all variables, eliminated univariate outliers, and checked for patterns of missing data. Missing data were imputed using multiple imputation (i.e. with five repeated imputations), a validated method of estimating missing values when data are missing at random (Rubin, 1996). We checked for group and sex differences in all dependent variables of interest using multivariate analysis of variance (MANOVA). Structural equation modeling (SEM) was performed using IBM AMOS v24, and multiple-group path analysis was used to compare males and females. First, we evaluated the fit for the unconstrained model and removed paths that were non-significant for both sexes. Next, we compared the constrained and unconstrained models to determine whether sex differences existed for the trimmed model (using chi-square difference tests). Finally, we constrained each factor separately in order to assess whether each specific path differed by sex (also using chi-square difference tests). For all SEM analyses, we used the following parameters to determine excellent model fit: non-significant χ2, comparative fit index (CFI) ≥ .95, and root mean square error of approximation (RMSEA) ≤ .05 (see Kline, 2015). Values ranging from 2 to 5 for the CMIN/df model fit parameter were considered to reflect reasonable fit (Marsh and Hocevar, 1985). For all standardized indirect coefficients, we used the bias-corrected percentile method of generating two-tailed significance values. Indirect effects were calculated using 2000 bootstrap samples.
Results
Preliminary analyses
A total of 304 adolescents were randomized in the HEARTY trial (Alberga et al., 2012). As this study was interested in constructs related to beliefs about exercise, participants who were randomized to the non-exercising control group were excluded (n = 76). All statistical analyses were performed on the remaining 228 participants. Demographic characteristics of the sample are shown in Table 1.
Demographic characteristics of sample.
SD: standard deviation.
Preliminary analyses indicated that all variables were normally distributed and that missing values were missing at random, Little’s Missing Completely at Random (MCAR) (93) = 110.50, p = .104. We evaluated potential exercise group differences across study variables using MANOVA. The overall MANOVA was not significant, F(20, 432) = 0.70, Wilks’ λ = .94, p = .830. There were no exercise group differences in terms of age, BMI, baseline and 6-month aerobic fitness, exercise self-efficacy and outcome expectancy at baseline and 3 months, and baseline perceived stress and depressive symptoms (all ps < .05). In addition, the proportion of girls was equal across the randomized exercise groups, χ2(2) = .01, p = .99; given this, we combined data across the exercise groups prior to performing SEM analyses. See Table 2 for all Pearson’s r correlation coefficients between variables.
Mean values, standard deviations, and correlations for all study variables.

M: mean values; SD: standard deviation; ESE: exercise self-efficacy; m: months; OE: outcome expectancy.
Mean values, standard deviations, and correlations were computed after multiple imputation procedure. Correlations represent overall sample. VO2 peak = change in cardiorespiratory function (in milliliters of oxygen per kilogram of body weight per minute) as measured by indirect calorimetry using a metabolic cart during a Balke–Ware treadmill test (treadmill test was stopped when participants reported exhaustion and could no longer continue). Depression (CDI-2) scores ranged from 0 to 32; scores above 20 indicate that follow-up may be warranted.
Indicates statistically significant sex difference.
p < .05; **p < .01.
We evaluated potential sex differences across study variables using MANOVA. The overall MANOVA was significant, F(10, 217) = 10.09, Wilks’ λ = .68, p < .001. Significant sex differences were observed for perceived stress (p < .001), depressive symptoms (p = .001), aerobic fitness at baseline (p < .001), and aerobic fitness at the end of the trial (p < .001); males reported lower stress and depressive symptoms and had better aerobic fitness scores at baseline and end of trial (see Table 2). No sex differences were observed for exercise self-efficacy, outcome expectancy, age, or BMI (all ps > .05).
Main analyses
Overall, the analysis of the direct and indirect effects on aerobic fitness determined that the model fit was good, χ2(66) = 125.15, p < .001, RMSEA = .04 (CI90% = .03–.06), CFI = .95, CMIN/df = 1.90. As illustrated in Figure 1, the model predicted over half the variance in aerobic fitness values at 6 months (R2 = .56). There was a marginally significant trend that greater outcome expectancy at 3 months was associated with greater end-of-trial aerobic fitness (p = .053). While controlling for baseline aerobic fitness, exercise group, and BMI, there were significant indirect effects on end-of-trial aerobic fitness, with greater baseline outcome expectancy and greater exercise self-efficacy at 3 months associated with greater end-of-trial aerobic fitness (see Table 3); both significant indirect effects were mediated by outcome expectancy at 3 months (see Figure 1).

Model predicting aerobic fitness (VO2 peak) at 6 months.
Standardized indirect effects for path analysis model predicting outcome expectancy and exercise self-efficacy at 3 months.
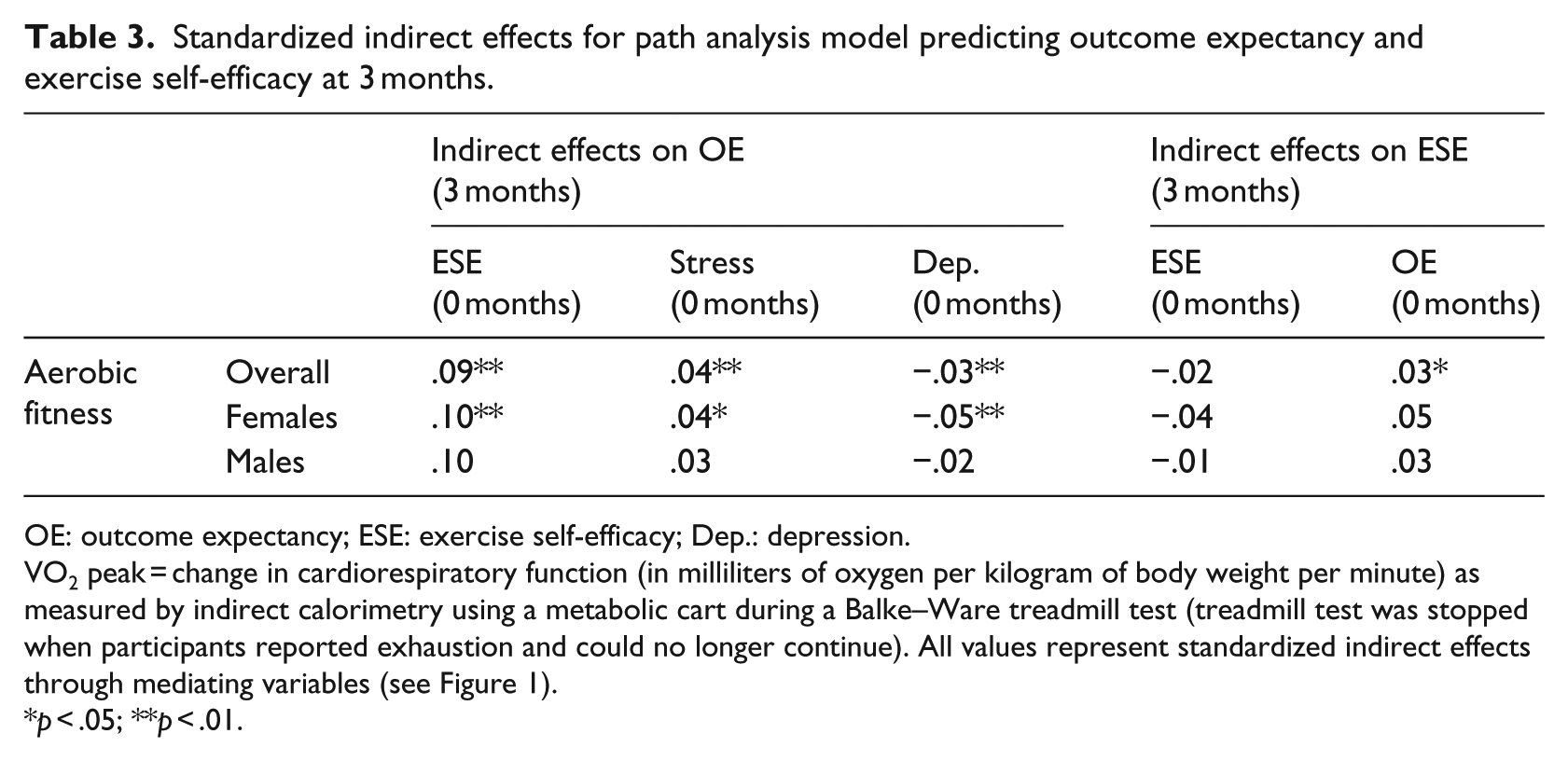
OE: outcome expectancy; ESE: exercise self-efficacy; Dep.: depression.
VO2 peak = change in cardiorespiratory function (in milliliters of oxygen per kilogram of body weight per minute) as measured by indirect calorimetry using a metabolic cart during a Balke–Ware treadmill test (treadmill test was stopped when participants reported exhaustion and could no longer continue). All values represent standardized indirect effects through mediating variables (see Figure 1).
p < .05; **p < .01.
A multiple-group path analysis was then conducted to see if paths differed for males and females. We compared the constrained and unconstrained models using a chi-square difference test and the result was not significant, indicating that the models did not differ significantly by sex overall, ∆χ2(16) = 21.17, p = .172. We then ran the model constraining each factor separately and found several sex differences; see Figure 1 for specific paths. The pattern of indirect effects was approximately the same for females as it was for the overall model, save for the fact that lower baseline depressive symptoms indirectly predicted better aerobic fitness as trial end among females only (see Table 4).
Standardized indirect effects for path analysis model predicting aerobic fitness (VO2 peak) at 6 months.

ESE: exercise self-efficacy; OE: outcome expectancy; Dep.: depressive symptoms.
VO2 peak = change in cardiorespiratory function (in milliliters of oxygen per kilogram of body weight per minute) as measured by indirect calorimetry using a metabolic cart during a Balke–Ware treadmill test (treadmill test was stopped when participants reported exhaustion and could no longer continue). All values represent standardized indirect effects on aerobic fitness through mediating variables (see Figure 1).
p < .05; **p < .01.
Discussion
This is the first study to examine the meditational relationship between exercise self-efficacy, outcome expectancy, and fitness among adolescents. Our objective was to test whether exercise self-efficacy and outcome expectancy would predict aerobic fitness, as defined by cardiorespiratory capacity, in adolescents with obesity who were participating in the HEARTY randomized controlled exercise trial (Sigal et al., 2014). Our hypotheses that greater exercise self-efficacy and lower depressive symptoms would indirectly lead to greater aerobic fitness via more positive outcome expectancy was supported. Using a longitudinal design rather than cross-sectional design, this study addresses a gap in the literature regarding motivational variables and fitness and allows for additional insight into the impact of depressive symptoms and perceived stress on SCT variables and fitness. As such, our data support the use of more tailored exercise interventions that enhance outcomes for youth with obesity.
Bandura (1997) argued that greater self-efficacy makes people more likely to expect positive results from a task (i.e. greater outcome expectancy), and the allure of such positive results is a powerful motivating force. Indeed, in this study, participants who had higher exercise self-efficacy tended to have better aerobic fitness at the end of the trial via improved outcome expectancies at 3 months. Of note, this was true even after accounting for baseline aerobic fitness, lending more weight to the role of SCT variables in predicting fitness. Our study is the first to observe this relationship in adolescents with obesity and is in accordance with previous observations in older adults (Resnick, 2001; Resnick and D’Adamo, 1997; Resnick et al., 2000); however, previous research with adolescent girls in the general population did not observe such a relationship (Dishman et al., 2005).
Compared to previous studies examining SCT models of exercise behaviors, we went a step further by modeling actual aerobic fitness in adolescents with obesity. Our data provide evidence that adolescents with higher exercise self-efficacy had better end-of-trial fitness levels via better outcome expectancies about exercising, suggesting that they derived more value (in terms of improving their fitness) from their exercise sessions than those with lower exercise-self efficacy. This has important ramifications: improving exercise self-efficacy and outcome expectancies may be a method of increasing the effectiveness of exercise programs (i.e. improving overall fitness levels) that goes beyond simply increasing exercise behaviors or the number or length of program sessions. For example, providing assessment feedback regarding one’s progress as they exercise may assist with improving one’s expectancy that their behavior is producing improved outcomes.
Another key finding of this study was that baseline depressive symptoms indirectly predicted end-of-trial aerobic fitness for females. While previous studies that have shown negative correlations between depressive symptoms and exercise behaviors (Ammouri et al., 2007; Park and Kim, 2008; Wiles et al., 2012), this was the first research to show a negative relationship between depressive symptoms and objectively measured aerobic fitness via its effects on SCT constructs. Specifically, depressive symptoms at baseline were associated with decreased exercise self-efficacy and outcome expectancies at 3 months, and this led to decreased aerobic fitness at the end of the trial for female participants. This finding supports the previous argument that depression-related motivational deficits may lead to decreased self-efficacy (Bussey and Bandura, 1999). This finding implies that interventions designed to increase aerobic fitness among female adolescents would benefit by targeting intervention efforts on reducing depressive symptoms in addition to addressing exercise self-efficacy and outcome expectancy. For example, suggesting concomitant psychological intervention for depression while engaged in an exercise training program may improve fitness at the end of the intervention. Exercise also improves mood (Goldfield et al., 2011); increasing exercise behaviors may help alleviate depressive symptoms as well, producing an interactive effect that serves to further increase motivation to exercise.
The nature of the relationship between perceived stress and exercise continues to be complicated and our data add further to the complexity. We observed a positive association between perceived stress and exercise self-efficacy, but not aerobic fitness. This is contrary to the negative correlation between perceived stress and exercise behaviors observed by the majority of the studies in this area (Stults-Kolehmainen and Sinha, 2014). Perhaps, the difference between the latter and our results (i.e. insignificant indirect effect) was due to the fact that we directly measured aerobic fitness, rather than self-reported exercise behaviors. Another possibility is that participants’ exercise performance increased as a function of perceived stress according to the optimal level of arousal theory (i.e. that performance increases with stress levels until a certain point, at which it drops off). Participants may have improved their fitness when experiencing “optimal” (i.e. only somewhat elevated) levels of perceived stress (Zuckerman, 2014). This is supported by the fact that the observed mean for the PSS in this study (see Table 2) was similar to those seen in previous samples of the general population (Roberti et al., 2006), suggesting that those in this study had normative levels of perceived stress; one might expect a significant negative correlation at high levels of perceived stress. Although more research is clearly needed on the role of perceived stress in exercise and fitness, our findings provide the foundation for a working model of how perceived stress interacts with SCT constructs to lead to higher aerobic fitness.
We observed sex differences in this study, but these were complicated by the uneven sex distribution in our sample. The majority of the participants in this study were female (about 70%), and the main findings we observed (i.e. that depressive symptoms and exercise self-efficacy have indirect effects on aerobic fitness levels via outcome expectancy) were not significant for males alone. One possibility for this result is that the analysis may have been underpowered for males (n = 67). Alternatively, the relationship between perceived stress, depressive symptoms, exercise self-efficacy, and outcome expectancy may be less important for predicting aerobic fitness in males. The present data are not in agreement with the findings of Fisher et al. (2011), who found that exercise self-efficacy was significantly correlated with objectively measured exercise in male, but not in female children aged 7 to 9 years. No comparable studies exist in adolescents; clearly, future studies will have to explore this relationship further.
This study is not without limitations. First, as noted previously, the unequal number of males and females may influence the results; it is unclear if the results would be different if a larger sample of males was included. Future studies should continue to examine the impact of sex on similar SCT models. The results may not be generalizable to all adolescents with obesity as those participating in this study were enrolled in a structured exercise trial, which may not be attractive or feasible to the overall population. In addition, our sample was primarily Caucasian and had parents that were well educated (74% of mothers and 68% of fathers had obtained college or university education); the results reported herein may not be applicable to other race-ethnicity groups or those from lower socioeconomic backgrounds. Replication of these findings in the general population would be beneficial. The use of qualitative criteria (i.e. participants’ indication of exhaustion and feeling they cannot continue) to determine the timing of termination of the maximal stress test may be another limitation; the addition of quantitative indicators of volitional fatigue (e.g. rate of perceived exertion, ± 10 beats of age-predicted maximum heart rate, plateau in VO2 despite an increase in the workload) may have lead to more accurate recordings of fitness and produced different results. Future intervention studies might also aim to use a randomized, between-subjects design to assess whether experimentally manipulating exercise self-efficacy, outcome expectancy, depressive symptoms, or perceived stress can produce changes in aerobic fitness levels in this population.
Conclusion
We observed that fewer depressive symptoms and greater exercise self-efficacy led to greater aerobic fitness levels via increased outcome expectancy. To our knowledge, this is the first study to employ an expanded SCT model that includes perceived stress and depressive symptoms in the context of predicting objectively measured aerobic fitness levels. The results highlight the possibility of tailoring interventions that target depressive symptoms, exercise self-efficacy, and outcome expectancies about exercise to enhance fitness in adolescents with obesity, a population at high risk of health complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HEARTY trial was supported by a grant (MCT-71979) from the Canadian Institutes of Health Research.