
Abstract
This study examined the relationship between childhood abuse experiences and health anxiety in adulthood and investigated the role of attachment in this relationship. In total, 181 university students (aged 18–29 years) completed a battery of measures that assessed childhood abuse, health anxiety, and attachment orientation. Health anxiety was associated with all categories of childhood abuse and overall childhood abuse severity. Anxious attachment partially mediated the relationship between overall childhood abuse and health anxiety in adulthood. The results further our understanding of the relationship between childhood abuse and health anxiety in adulthood and provide support for the interpersonal model of health anxiety.
Health anxiety (HA) refers to health-related worries and preoccupation with having, or acquiring, a serious medical condition (American Psychiatric Association (APA), 2013). It is generally believed that experiences during childhood may predispose a person to the development of HA later in life (Barsky et al., 1994; Thorgaard et al., 2017, 2018). For example, personal illness or illness of a family member during childhood have been identified as possible risk factors for severe HA in adulthood (Alberts and Hadjistavropoulos, 2014; Alberts et al., 2016; Barsky et al., 1994; Noyes et al., 2002; Thorgaard et al., 2018).
Previous research has also identified a link between childhood abuse experiences and HA (Anuk and Bahadir, 2018; Bailer et al., 2014; Barsky et al., 1994; Brown et al., 2005; Fiddler et al., 2004; Haugaard, 2004; Reiser et al., 2014; Salmon and Calderbank, 1996; Taycan et al., 2014; Weck et al., 2014). Specifically, relationships have been found between childhood sexual and physical abuse and two components of HA (i.e. disease concern and disease conviction) in a sample of undergraduate students (Salmon and Calderbank, 1996). Furthermore, cumulative adverse childhood experiences (ACEs) have been associated with HA in adulthood (Bailer et al., 2014). Inconsistent with the aforementioned findings, Noyes et al. (2002) found that reports of childhood physical and sexual abuse did not significantly differ between patients with and without hypochondriasis. In addition, sexual abuse in childhood was found to be a risk factor for a lifetime diagnosis of multiple psychiatric disorders, but not somatoform disorders in general (Chen et al., 2010). Due to the contradictory findings within the literature, additional research is warranted to clarify the relationship between childhood abuse and HA and to further examine multiple types of childhood abuse experiences to provide a more comprehensive understanding of the association between specific abuse experiences and HA in adulthood.
One factor that might be influenced by early abuse experiences and play a role in HA is attachment orientation. Attachment theory (Bowlby, 1969, 1973) emphasizes the influence of early intimate relationships, usually with parents, on one’s subsequent interpersonal interactions and relationships (Maunder and Hunter, 2012). The quality of these emotional connections leads to the development of attachment styles, which are thought to remain relatively stable from childhood through adulthood (Bowlby, 1979; Waters et al., 2000; Widom et al., 2018). An empirically supported, dimensional model of attachment proposes two converging dimensions of attachment insecurity: attachment anxiety and attachment avoidance (Brennan et al., 1998; Fraley and Shaver, 2000). Attachment anxiety includes fear of interpersonal rejection, the need for approval, and concern about the availability of others. Attachment avoidance includes fear of interpersonal closeness, reluctance to self-disclose, and the need for self-reliance.
Rooted in attachment theory, the interpersonal model of health anxiety (IMHA; Noyes et al., 2003; Stuart and Noyes, 1999) proposes that illness behaviors displayed by individuals with elevated HA can be best understood as a form of social behavior that is motivated by maladaptive attachment styles. The model suggests that insecure attachment can foster patterns of reassurance seeking and persistent complaints of illness to elicit care from others. Previous research has found an association between elevated HA and insecure attachment (Alberts and Hadjistavropoulos, 2014; Bizzi et al., 2015; Jordan et al., 2015; Noyes et al., 2003; Schmidt et al., 2002; Sherry et al., 2014; Thorgaard et al., 2017; Wearden et al., 2006) and provides support for the IMHA (MacSwain et al., 2009). Elevated HA and increased somatization have been linked to general insecure attachment (Noyes et al., 2003) and anxious attachment, in particular (Alberts and Hadjistavropoulos, 2014; Birnie et al., 2013; Maunder et al., 2017; Schroeter et al., 2015; Sherry et al., 2014). Moreover, several studies have also shown significant association between insecure attachment and frequent attendance in the healthcare system, a trait often observed in individuals who experience HA (Ciechanowski et al., 2002; Taylor et al., 2012).
The IMHA also proposes that childhood abuse can significantly affect the development of attachment styles and influence illness behavior into adulthood (Hollifield and Finlay, 2014; Stuart and Noyes, 1999). More specifically, maltreated children may receive attention when expressing somatic concerns and illness-related behavior; subsequently, symptoms of HA may develop as a way to receive comfort and care (Stuart and Noyes, 1999). Research supports the relationship between childhood maltreatment and insecure attachment (Muller et al., 2000; Styron and Janoff-Bulman, 1997). There is also evidence that insecure attachment may mediate the relationship between childhood adversity and psychopathology (Bifulco et al., 2006; Sitko et al., 2014; Tasca et al., 2013). Preliminary findings have supported the potential role of attachment security as a mediator between childhood adversity and HA (Maunder et al., 2017). Taken together, further research is necessary to provide additional evidence to support the notion that attachment plays a mediating role in the association between childhood abuse and HA in adulthood.
The purpose of this study was to examine the relationship between childhood abuse experiences and HA in adulthood within a nonclinical population and to investigate the role of attachment in this relationship. We hypothesized that (1) there would be significant, positive associations between HA, categories of childhood abuse, childhood abuse severity, and anxious attachment and (2) anxious attachment would mediate the relationship between childhood abuse and HA.
Methods
Participants
Males and females (18 years of age and older) were recruited for the study. Pre-Screen Questionnaires were distributed in undergraduate classrooms to approximately 605 students. Students who endorsed at least one abuse category, or those who reported no childhood abuse history and were randomly selected, were invited to participate in the online study. Overall, the study comprised 181 participants, of which 104 endorsed a history of childhood abuse. Participants in the online survey were compensated with either a 1% course credit or were entered into a draw for a gift certificate. Participants completed the study between September 2012 and December 2012. Ethical approval to conduct this research was obtained from the Institutional Research Ethics Board and informed consent was obtained from all participants.
Measures
Pre-Screen Questionnaire
Students were pre-screened for a history of childhood abuse using a self-report questionnaire comprised of items from the ACEs study (Felitti et al., 1998). The ACEs study is a retrospective measure consisting of yes/no questions pertaining to adverse childhood experiences (up to the age of 18 years), including items concerning different forms of childhood maltreatment. For this study, 10 questions from the ACEs study were utilized, which assessed physical abuse, emotional abuse, sexual abuse, emotional neglect, and physical neglect (i.e. two questions from each category). Participants were defined as being exposed to a specific category of abuse if they responded yes to either or both of the category items. Participants were defined as being exposed to childhood abuse if they responded yes to one or more of any of the pre-screen questions.
Demographic variables
Basic demographic information (e.g. age, sex, relationship status, ethnicity) and self-reported information regarding history of medical and mental health conditions were obtained via a brief demographics form.
Childhood Trauma Questionnaire
The Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994) is a retrospective, self-report measure that assesses childhood traumatic experiences and the severity of these experiences, which was used as the overall measure of childhood abuse experiences. The measure consists of 28 items, most of which are rated on a 5-point Likert-type-style scale ranging from 1 (never) to 5 (very often). Examples of items on the CTQ include “I didn’t have enough to eat,” “I knew that there was someone to take care of me and protect me,” and “People in my family said hurtful or insulting things to me.” The CTQ produces a total score, ranging from 25 to 125, and scores for the following five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. Mean CTQ total score in a sample of undergraduate students was 35.21 (Wright et al., 2001). The CTQ has demonstrated high internal consistency and good test–retest (2–6 months) reliability (Bernstein et al., 1994). This measure has been found to be a valid measure of abuse and neglect in undergraduate student samples (Paivio and Cramer, 2004).
Experiences in Close Relationships–Revised
The Experiences in Close Relationships–Revised (ECR-R; Fraley et al., 2000) is a self-report questionnaire that measures adult attachment orientation. The measure consists of two subscales, attachment anxiety (ECR-R-AN) and attachment avoidance (ECR-R-AV), which each contain 18 items. The ECR-R-AN measures fear of interpersonal rejection, the need for approval from others, and the extent to which a person is concerned about the availability of others. Examples of items on the ECR-R-AN subscale include “I often worry that others don’t really love me,” “I worry that others won’t care about me as much as I care about them,” and “I’m afraid that I will lose others’ love.” The ECR-R-AV measures fear of interpersonal closeness, reluctance to self-disclose, and the need for self-reliance. Examples of items on the ECR-R-AV subscale include “I prefer not to show others how I feel deep down,” “I find it difficult to allow myself to depend on others,” and “I get uncomfortable when others want to be very close.” All responses are rated on a 7-point Likert-type-style scale ranging from 1 (strongly disagree) to 7 (strongly agree), and each subscale yields a score ranging from 18 to 126. ECR-R mean scores in a sample of undergraduate students were 64.95 for ECR-R-AN and 51.24 for ECR-R-AV (Wei et al., 2007). The ECR-R has demonstrated good psychometric properties (Sibley and Liu, 2004; Sibley et al., 2005) and is among the most commonly used attachment scales in psychosomatic research (Ravitz et al., 2010).
Short Health Anxiety Inventory
The Short Health Anxiety Inventory (SHAI; Salkovskis et al., 2002) is a self-report questionnaire that measures nonclinical and clinical levels of HA in adults. The measure consists of 18 items, each containing four statements from which the respondents select the statement that best describes their experience within the past 6 months. The SHAI was administered as a 14-item measure, which excludes the four-item negative consequences subscale (Alberts et al., 2011). The items are scored on a scale from 0 (no symptoms; for example, “I do not worry about my health” and “I do not have any difficulty taking my mind off thoughts about my health”) to 3 (severe symptoms; for example, “I spend most of my time worrying about my health” and “Nothing can take my mind off thoughts about my health”). The sum of items produces a total score ranging from 0 to 42. The mean SHAI total score in a sample of undergraduate students was 10.79 (Abramowitz et al., 2007). Another study found means of 9.4 in a sample of healthy adults and 9.6 in a sample of students (Salkovskis et al., 2002). The 14-item version has demonstrated good reliability and validity (Salkovskis et al., 2002).
Statistical analyses
Statistical analyses were conducted using Software Package for the Social Sciences (SPSS: version 22.0). Descriptive statistics were computed for the demographic variables and to summarize the scores for each measure. Two primary sets of analyses were completed. First, bivariate correlations were computed to examine the relationships between HA, categories of childhood abuse, childhood abuse severity, and attachment orientation. Second, mediation analyses utilizing the Preacher and Hayes (2004) procedure was employed to explore whether attachment orientation mediates the relationship between childhood abuse and HA. Skewness and kurtosis were examined for each measure and the SHAI and the CTQ displayed a non-normal distribution. Consequently, the values for these measures were transformed using square root and logarithmic transformations, as these are recommended approaches for reducing positive skew (Field, 2009). All analyses were conducted twice, with the non-transformed data set and again with the data set that included the transformed variables. There were no significant differences in the results between the two sets of data, with one exception—with the non-transformed data, physical abuse did not demonstrate a significant association with HA, r(179) = .111, p = .136; however, with the transformed variables, physical abuse and HA demonstrated a positive, statistically significant relationship, r(179) = .158, p = .033. As the difference between the data sets was minimal, the non-transformed data were utilized and will be presented to simplify data interpretation.
Results
Descriptive information and preliminary analyses
There were 38 male (21.0%) and 143 (79.0%) female participants, who ranged from 18 to 29 years of age (M = 20.29 years; SD = 2.31). The majority of participants identified as Caucasian (n = 140; 77.3%), while other ethnicities included Asian (n = 14; 7.7%), multiple ethnicities (n = 8; 4.4%), Metis (n = 6; 3.3%), Hispanic (n = 3; 1.7%), Middle Eastern (n = 3; 1.7%, other ethnic origins (n = 3; 1.7%), African/black (n = 2; 1.1%), and Aboriginal/First Nations (n = 2; 1.1%). Participants reported either being in a relationship (n = 99; 54.7%) or being single (n = 82; 45.3%). Several participants reported currently having a diagnosed medical condition (n = 32; 17.7%) or a diagnosed medical condition or serious injury in childhood (n = 49; 27.1%). A number of participants reported a current (n = 27; 14.9%) or past (n = 30; 16.6%) mental health condition. Current mental health conditions reported included attention deficit hyperactivity disorder (ADHD; n = 4; 2.2%), anxiety (n = 10; 5.5%), depression (n = 8; 4.4%), and anxiety and depression (n = 5; 2.8%). Past mental health conditions reported included ADHD (n = 1; 0.6%), anxiety (n = 4; 2.2%), depression (n = 18; 9.9%), anxiety and depression (n = 4; 2.2%), and bipolar disorder (n = 1; 0.6%). Mean scores, standard deviations, ranges, and reliability coefficients (Cronbach’s alpha) for each measure are presented in Table 1.
Descriptive statistics for study measures (N = 181).

SD: standard deviation; SHAI: Short Health Anxiety Inventory; CTQ: Childhood Trauma Questionnaire; ECR-R: Experiences in Close Relationships–Revised; AN: attachment anxiety; AV: attachment avoidance.
The participants reiteratively completed the Pre-Screen Questionnaire during the full survey, and of the 181 participants, 104 of them endorsed at least one category of childhood abuse. A summary of the reported childhood abuse categories by sex and for the overall sample is presented in Table 2. Several participants endorsed only one type of childhood abuse experience (36.5%), while others endorsed two (24.0%), three (28.8%), four (7.7%), or all five types (2.9%).
Prevalence of childhood abuse categories for full study sample.

n = 38.
n = 143.
N = 181.
Between-group differences in levels of HA were examined for demographic variables. As sample sizes in other reported ethnicities were not large enough to compare between each other, we grouped together other self-reported ethnicities and compared differences between this group and the largest reported ethnicity group (i.e. Caucasians). Independent sample t-tests were conducted to compare levels of HA between males and females, Caucasians and non-Caucasians, those with and without a current medical condition, and those with or without a childhood medical condition/serious injury. There was a significant difference between males (M = 10.08, SD = 6.02) and females (M = 12.86, SD = 6.04; t(179) = 2.52, p = .012) and those with (M = 14.50, SD = 5.67) and without (M = 11.80, SD = 6.13) a current medical condition (t(179) = 2.29, p = .023). Significant differences were not found between Caucasians and non-Caucasians (t(179) = .501, p = .617) or between those with or without a childhood medical condition/serious injury (t(179) = .913, p = .362). The relationship between age and HA was not significant (r(179) = .034, p = .647).
Relationships between childhood abuse, HA, and attachment
Bivariate correlations were computed to examine the associations between childhood abuse, HA, and attachment orientation. Statistically significant relationships were observed between HA and the measures of interest, with the exceptions of the physical abuse subscale (using the non-transformed data) and avoidant attachment. All correlations among measures are presented in Table 3.
Summary of correlations among measures (N = 181).
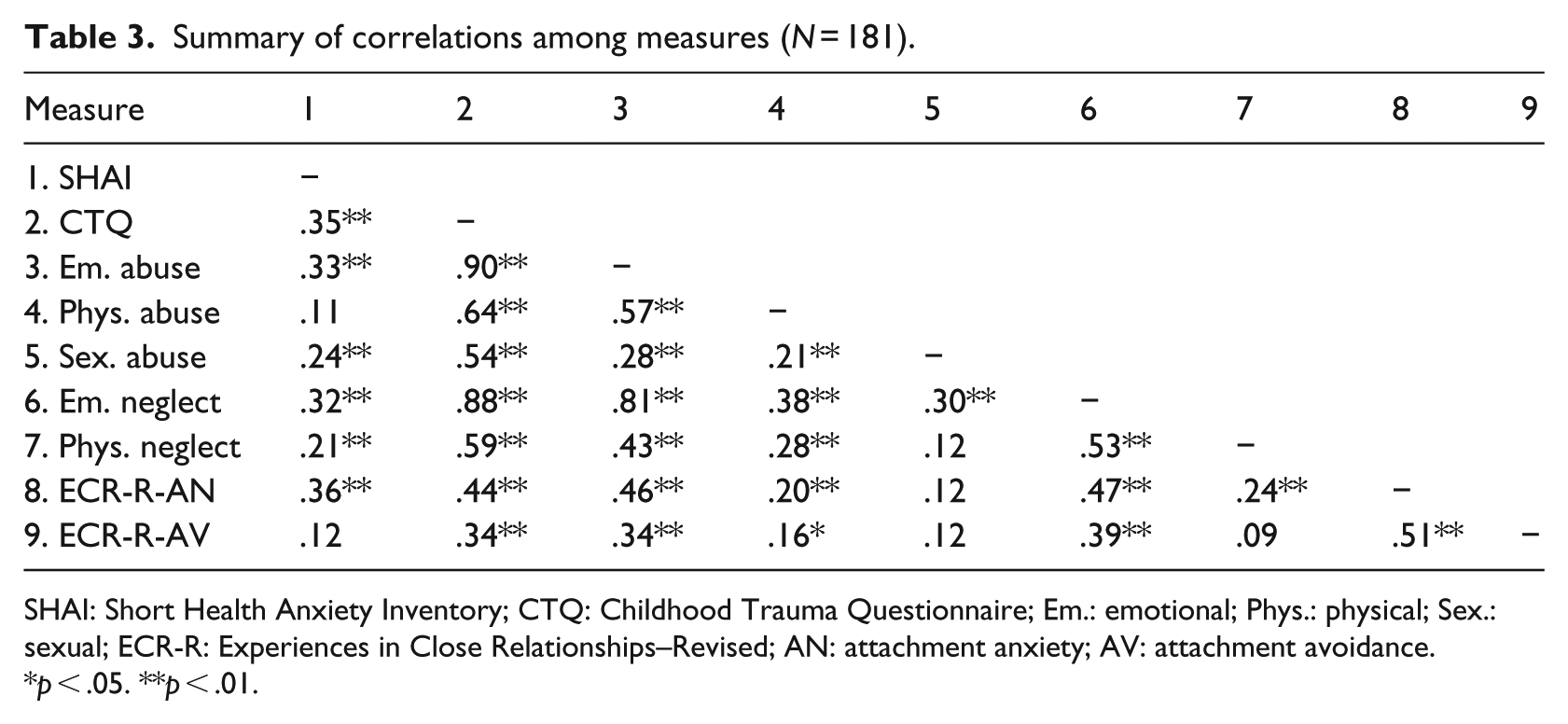
SHAI: Short Health Anxiety Inventory; CTQ: Childhood Trauma Questionnaire; Em.: emotional; Phys.: physical; Sex.: sexual; ECR-R: Experiences in Close Relationships–Revised; AN: attachment anxiety; AV: attachment avoidance.
p < .05. **p < .01.
Testing models of childhood abuse, attachment, and HA
To test the mediating role of anxious attachment, a mediation analysis was conducted employing the procedure outlined by Preacher and Hayes (2004). The total effect of childhood abuse (β = .15) on HA was statistically significant (p < .001). The effect of childhood abuse (β = .68) on anxious attachment was also statistically significant (p < .001), indicating severity of childhood abuse was greater among those with relatively higher levels of anxious attachment. The effect of anxious attachment (β = .07) on HA, when controlling for childhood abuse, was also statistically significant (p < .01), suggesting that participants with relatively high anxious attachment were more likely to have elevated HA while controlling for childhood abuse. Finally, the direct effect of childhood abuse (β = .10) on HA, when controlling for anxious attachment, was statistically significant (p < .01), demonstrating that when controlling for anxious attachment there is still a statistically significant relationship between childhood abuse and HA, indicating that anxious attachment did not fully mediate the effect of childhood abuse on HA.
However, results of the Sobel test (Sobel, 1982) demonstrated that the mediated effect had dropped significantly (z = 2.92, p = .004) and that anxious attachment partially mediated the relationship between childhood abuse and HA. Finally, the bootstrapped estimate of the true indirect effect was estimated to lie between .0197 and .0810 with 95% confidence intervals, indicating that the indirect effect is different from 0 at p < .05 (two-tailed). Overall, these analyses indicate that anxious attachment was a partial mediator in the relationship between childhood abuse and adult HA.
A second mediation analysis was conducted to examine the mediating role of avoidant attachment. The results reiterated that the total effect of childhood abuse (β = .15) on HA was statistically significant (p < .001). The effect of childhood abuse (β = .52) on avoidant attachment was also statistically significant (p < .001), indicating severity of childhood abuse was greater among those with relatively higher levels of avoidant attachment. The effect of avoidant attachment (β = –.001) on HA, when controlling for childhood abuse, was not statistically significant (p = .96), suggesting that participants high in avoidant attachment were not more likely to have elevated HA when controlling for childhood abuse. Avoidant attachment did not predict HA in this model and therefore this model was a failure for mediation. Finally, the direct effect of childhood abuse (β = .15) on HA, when controlling for avoidant attachment, was statistically significant (p < .001), demonstrating that when controlling for avoidant attachment, the relationship between childhood abuse and HA does not change. These results indicate that avoidant attachment does not mediate the effect of childhood abuse on HA.
The results of the Sobel test (Sobel, 1982) were not statistically significant and confirmed that avoidant attachment does not play a mediating role in the relationship between childhood abuse and HA (z = –.05, p = .96). Finally, the bootstrapped estimate of the true indirect effect was estimated to lie between –.0220 and .0208 with 95% confidence intervals. Because 0 is in the 95% confidence interval, it can be concluded that the indirect effect does not differ from zero at p < .05 (two-tailed) and, therefore, also does not support the mediating role of avoidant attachment. Overall, these analyses indicated that avoidant attachment was not a mediator in the relationship between childhood abuse and adult HA.
Discussion
It has been proposed that experiences in childhood, including childhood abuse, may contribute to the development of HA later in life (Barsky et al., 1994). The purpose of this study was to expand upon existing research by examining the relationships between childhood abuse experiences and HA in adulthood, in a nonclinical population, and to investigate the role of attachment in this relationship. We found a significant, positive association between childhood abuse severity and HA in adulthood. In addition, HA demonstrated significant, positive associations with all categories of abuse. These findings are consistent with previous research (Reiser et al., 2014; Salmon and Calderbank, 1996). While some research has not found a relationship between childhood abuse and HA in adulthood (Bailer et al., 2014; Noyes et al., 2002), the current findings support a relationship between these experiences in a nonclinical population. It is possible that this discrepancy is due to the severity of symptoms within clinical samples, which may impact research outcomes.
HA research has typically focused on the impact of physical and sexual forms of abuse and often excludes emotional abuse and neglect. The current results emphasize the importance of considering childhood emotional abuse and neglect, as these experiences demonstrated a relationship with HA in adulthood. These findings are consistent with research that suggests that these forms of maltreatment, independently, can have a significant impact on functioning in adulthood (Spertus et al., 2003).
Our findings demonstrated severity of childhood abuse was greater among those with relatively higher levels of anxious attachment and avoidant attachment, which is consistent with previous research (Muller et al., 2000; Styron and Janoff-Bulman, 1997). The results that demonstrate a relationship between childhood abuse history and attachment should be interpreted with caution, as this was a cross-sectional study that utilized self-report measures. It may be necessary to further confirm these findings in a longitudinal study. A significant relationship between HA and anxious attachment was observed, indicating that as anxious attachment increased, levels of HA also increased. HA and avoidant attachment were not significantly associated, which is also consistent with previous findings (Alberts and Hadjistavropoulos, 2014; Sherry et al., 2014).
The examination of the potential mediating role of anxious and avoidant attachment in the relationship between childhood abuse severity and HA contributes to our understanding of the mechanism by which childhood adversity and HA are associated. Our results demonstrated that avoidant attachment was not a mediator in this relationship. In contrast, anxious attachment was associated with both childhood abuse and HA and was a partial mediator in this relationship. This novel finding provides insight into anxious attachment as a possible risk factor for the development of HA in individuals who have experienced childhood abuse. These findings lend support to the IMHA (Noyes et al., 2003; Stuart and Noyes, 1999) and suggest that anxious attachment is the dimension of attachment that is most significantly related to HA. The current results, and subsequent research, can assist the development of prevention, assessment, and intervention strategies related to HA. For example, the understanding that anxious attachment may be an etiological factor contributing to the development of HA in individuals with a history of childhood abuse may inform tailored interventions. Interpersonal psychotherapy (IPT), which is based on attachment theory, may be an appropriate treatment option for those presenting with significant HA and attachment issues (Stuart et al., 2008). IPT for HA focuses on developing positive social supports and effective communication of one’s needs to prevent maladaptive care-seeking and illness behavior (Stuart et al., 2008). Our results also warrant further investigation of other possible mediating factors in the relationship between childhood abuse and HA, as a significant portion of the effect of childhood abuse on HA remains unexplained.
There are several study limitations to consider. First, our sample consisted of undergraduate students and the majority of the participants were female and Caucasian. These factors may limit the generalizability of the results. Second, this study utilized retrospective reports of childhood abuse, which may be subject to recall bias. Third, it is possible that potential confounding variables (e.g. comorbid disorders) may play a role in these relationships. Fourth, the cross-sectional nature of the data prevents an assessment of the temporal relationship between childhood abuse and HA. Longitudinal research is needed to examine the development of HA over time. Future research should employ more diverse samples and explore additional variables (e.g. personality factors, medical issues, relationship to the abuser) that may play a role in the path from childhood abuse to elevated HA to provide a more comprehensive understanding of this relationship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported by Canadian Institutes of Health Research (CIHR) Canada Graduate Scholarship 115987 (Ms Sarah Reiser).