
Abstract
For type 1 diabetes management, the role of attentional bias remains unclear. This secondary analysis examined type 1 diabetes attentional bias and adolescent type 1 diabetes management prior to and during a cognitive and behavioral intervention. Youth with type 1 diabetes and above target glycemic control were assigned to intervention or usual care control. Participants completed baseline and follow-up type 1 diabetes Stroop tasks, HbA1c tests, and blood glucose meter downloads. Intervention was associated with greater reductions in type 1 diabetes attentional bias than control, and these reductions partially mediated the effect of treatment on diabetes management behaviors. Type 1 diabetes attentional bias is a potential target to improve type 1 diabetes management.
Introduction
Adolescents with type 1 diabetes (T1D) must engage in several health behaviors multiple times each day (e.g. blood glucose checks, carbohydrate counting, and precise insulin dosage) to achieve target glycemic control and prevent negative short- and long-term health outcomes (Atkinson et al., 2014). A myriad of individual (e.g. self-efficacy, coping, and emotional processing) and interpersonal (e.g. parental monitoring and family conflict) factors influence the degree to which adolescents engage in these diabetes management behaviors (Lansing and Berg, 2014). Given the cognitive and attentional demands of T1D management, it is perhaps unsurprising that cognitive processes have been shown to play a key role in diabetes management (Duke and Harris, 2014). However, research to date has largely focused on voluntary executive function capacities that benefit diabetes management and glycemic control (Bagner et al., 2007; McNally et al., 2010; Murphy et al., 1997) rather than implicit or automatic biases in cognitive processing that may also affect diabetes management in adolescence.
An implicit cognitive process that may influence T1D management is attentional bias, that is, when a person gives preferential attention to a particular type of information (MacLeod and Mathews, 2012). When an individual has attentional bias, cues related to what he or she desires or avoids are given special attention, which in turn influences his or her perceptions, emotions, cognitions, and behavior (Field and Cox, 2008). For example, for individuals craving alcohol or highly palatable foods, attentional bias to stimuli that signify access to alcohol or foods amplifies the salience of perceived rewards and drives approach behavior (e.g. using alcohol or eating highly palatable food; Calitri et al., 2010; Field and Cox, 2008; Sharma et al., 2001). In contrast, attentional biases to aversive stimuli can also guide behavior, including avoidance behaviors. For example, individuals with anxiety demonstrate increased attentional bias to threatening information (Bar-Haim et al., 2007; Cisler and Koster, 2010; Mogg et al., 1992), which in turn may increase avoidance behaviors.
Research on attentional bias has also been extended to the context of chronic illness management. In individuals with asthma, attentional bias to asthma cues has been associated with poorer adherence to asthma management plans (Jessop et al., 2004). These results can be explained by the hypervigilance-avoidance hypothesis, which postulates that attention is initially heightened toward threatening cues, followed by attentional and behavioral avoidance of the threatening stimulus (Bar-Haim et al., 2007; Mogg et al., 1997). For example, attentional biases to asthma cues may be amplified by negative representations of the chronic illness, which is followed by decreased engagement in illness-related behaviors (Jessop et al., 2004). In adolescents with T1D, aversive experiences occur often with diabetes management (e.g. pain from using lancets or syringes and social stigma associated with diabetes), and negative illness representations (e.g. the lack of a cure, economic cost, long-term complications, and diabetes-related negative effect) have been linked with both decreased diabetes management behaviors and worse glycemic control (Fortenberry et al., 2009; Hughes et al., 2012; Lansing et al., 2016; Law et al., 2002; Mc Sharry et al., 2011). Thus, adolescents with T1D may have attentional bias to diabetes cues due to aversive aspects of the disease management process, which potentiates cognitive and behavioral avoidance of diabetes management.
Moreover, research has supported that cognitive and cognitive-behavioral interventions might modify attentional biases, which in turn decrease the problematic avoidance behaviors. Much of the research in this domain has focused on attentional bias modification (ABM), a cognitive intervention that targets specific biases in attention to threat via computer-based attentional training (Bar-Haim, 2010; Bar-Haim et al., 2011; Beard et al., 2011; Eldar et al., 2012). However, other cognitive and behavioral intervention approaches have also shown efficacy in reducing attentional bias toward threat, including working memory training and cognitive-behavioral therapy (CBT; Reinecke et al., 2013; Roughan and Hadwin, 2011; Tobon et al., 2011; Waters et al., 2012). First, working memory training is theorized to improve overall attentional control, which facilitates the modification of attentional bias (Roughan and Hadwin, 2011). Second, CBT is theorized to modify attentional bias through cognitive restructuring and repeated exposure. Cognitive restructuring and exposure to negative stimuli dismantle stimulus-driven response cycles and modify preconscious belief systems, which in turn reduce attentional bias (Cowart and Ollendick, 2010; Ochsner et al., 2002). It is through improvements in processing of negative stimuli and normalization of threat bias in response to both working memory training and CBT that behavioral avoidance may be lessened (Reinecke et al., 2013).
Consistent with this theory, Hadwin and Richards (2016) found that 10 sessions of CBT (including cognitive reframing, problem solving, and development of coping mechanisms) and 25 sessions of a working memory training program (CogMed), delivered across 5 weeks, each reduced attentional bias to threat and reduced anxiety symptoms among adolescents with anxiety. Thus, it was hypothesized that CBT and working memory training interventions may benefit diabetes management in adolescents with T1D in part by decreasing attentional biases to diabetes cues that in turn reduces avoidance of aversive daily disease management tasks such as self-monitoring of blood glucose (SMBG) levels.
This study tests this hypothesis through a secondary analysis of a published randomized controlled trial testing a web-delivered multi-component intervention (involving CBT and working memory training) that aimed to improve diabetes management among youth with T1D and above target glycemic control (see section “Method” for more details; Stanger et al., 2018). The initial design of this intervention was to target self-regulation of SMBG levels. The primary study analyses found that adolescents assigned to the intervention had lower glycated hemoglobin percentages (HbA1c, an indicator of metabolic control) at post-treatment compared to the control group and that increased SMBG was the key mechanism that explained improvements in HbA1c (Stanger et al., 2018). A Stroop task was included to measure if working memory training impacted impulse control. The inclusion of the diabetes Stroop task allowed us to measure attentional bias, which was not an originally proposed mechanism of treatment. As such, primary analyses did not consider attentional bias to diabetes cue as a possible mediator of treatment effects on the behavioral mechanism of change, SMBG.
This study hypothesized that the multi-component intervention would reduce attentional bias to diabetes cues and that these effects would mediate increases in SMBG, suggesting reduced avoidance of this behavior. Mediational analyses were used to test these hypotheses.
Method
Participants
As reported previously (Stanger et al., 2018), participants for this study included 61 adolescents with T1D and above target glycemic control (43% female, 98% White, 66% using an insulin pump, Mage = 15.08 years, SD = 1.43, average length of diagnosis = 6.20 years, SD = 3.54, average Hollingshead nine-step socioeconomic status (SES) = 5.44, SD = 2.48) recruited from two clinical sites affiliated with a children’s hospital in New Hampshire, which serves the northern New England region of the United States with a predominantly White population. Inclusion criteria were aged 13–17, T1D diagnosis more than 18 months prior, HbA1c percentage ⩾8 percent for the past 6 months and most recent ⩾8 percent, and broadband Internet and computer at home (to allow participation in web-delivered treatment). Exclusion criteria included pregnancy and severe medical or psychiatric illness. For complete details on study methodology, see Stanger et al. (2018). This study was conducted in compliance with the Committee for the Protection of Human Subjects at Dartmouth College (Study ID: 23559).
Procedures
This study is a secondary analysis of a published randomized controlled trial testing a web-delivered multi-component intervention targeting diabetes management among youth with T1D and above target glycemic control (Stanger et al., 2018). The 25-week treatment consisted of (a) incentives for SMBG to increase adolescent exposure and modify the contingencies around an aversive behavioral task that is key for managing T1D; (b) motivation enhancement therapy (MET) and CBT to address deficits in motivation for change, problem-solving skills, and coping skills, and to target negative cognitions; (c) working memory training to address deficits in neurocognitive functioning that impact self-regulation of health behaviors; and (d) parent training about behavioral contracting and parent incentives for engaging in behavioral contracting around SMBG. The control group received usual, standard care for T1D across the same 25-week period.
Intake and follow-up (25 weeks post-intake) assessments were conducted in the pediatric endocrinology department or a study office centrally located in the region. The study was explained to parents and adolescents, and parental/guardian written consent and adolescent written assent were obtained from all participants prior to participation. At intake and follow-up, a series of cognitive tasks and questionnaires, including a modified diabetes Stroop task, was completed by the adolescent, while the parent completed questionnaires including parent reports of youths’ diabetes management. Also, a venous glycosylated hemoglobin blood sample was collected from the adolescent and data were collected from his or her blood glucose meter. Randomization—to a 6-month intervention targeting glycemic control (n = 30) or usual care (n = 31)—was conducted using computerized minimum likelihood allocation after completion of baseline measures by research assistants. Participants were paid $50 each for the baseline and follow-up assessment.
Intervention
A Health Insurance Portability and Accountability Act (HIPPA)-compliant video conference software (WebEx) was used to record web-delivered intervention sessions. The intervention was delivered by master-level therapists and working memory training coaching sessions were delivered by bachelor’s level working memory coaches (research assistants).
MET/CBT
Brief (30 minute), manualized MET/CBT sessions were web-delivered for the first 12 weeks of treatment. Sessions in weeks 1–5 focused on MET treatment components, including building awareness around SMBG and goal setting. Subsequently, in weeks 6–12, therapists introduced CBT intervention components, including a functional analysis that elucidated antecedents and consequences to missing or skipping diabetes management behaviors, problem solving, and management of mood, anger, and stress. Participants completed related homework assignments outside of session, which were reviewed at the following session. In weeks 13, 16, 20, and 25, session content focused on additional CBT-based problem solving.
Incentives
Incentives for diabetes management were earned by participants for uploading glucometer data to an online portal (Carelink Personal) and for meeting SMBG goals (e.g. ⩾5 times daily with checks at least 2 hours apart), on 1 day more than the prior week, up to 5 days per week. SMBG incentives began at $10 per week and increased $5 weekly until reaching $30 per week, with the potential of a $5 bonus if participants exceeded their goal for that week. The minimum weekly goal became 5 days per week for weeks 8–25. Participants were paid weekly in weeks 1–11, but a fading strategy was utilized in following weeks, such that every payment was delayed by an additional week, and participants were paid in weeks 13, 16, 20, and 25.
Working memory training
In week 3 of treatment, working memory training was introduced. Adolescents were instructed to complete 5 working memory training sessions (CogMed-RM v.2 program) weekly across 5 weeks, amounting to 25 sessions of working memory training in total. Participants could earn up to $10 per working memory session: $5 for completing all the session’s tasks in 1 day and $5 for maintaining or improving performance in three out of eight of the session’s tasks, totaling to a possible $245 earned for working memory training. Participants had weekly video conference calls with a bachelor-level coach who helped participants interpret their weekly progress, provided information on incentives, and delivered motivational support.
Parent contingency contracting
Parents completed their own 20 minute sessions, in which they were trained in developing and implementing a contingency contract for SMBG. Parents earned incentives for creating a daily report of teens’ SMBG frequency on 5 days per week, earning $10 in weeks 1 and 2, which escalated to $30 in following weeks, and incentives were delivered on a delayed schedule after week 11. In addition, beginning in week 11, therapists asked parents to engage in a weekly family meeting in which they reviewed teens’ SMBG data and collaboratively problem-solved barriers to adherence. Both adolescents and parents earned an extra $5 weekly for this weekly family review in weeks 12–25.
Measures
Combined Stroop task
Participants completed a computerized Stroop task to assess attentional bias to diabetes cues. The Stroop task required subjects to select the color in which a word appeared on the computer screen. The Stroop task for this study included four conditions: (1) traditional neutral word control, (2) additional block X’s control, (3) classic Stroop, and (4) diabetes Stroop. The control condition presented neutral words and the additional control presented “XXX” instead of words. In the classic Stroop condition, color words were presented in a conflicting color (e.g. “BLUE” printed in red letters), whereas in the diabetes Stroop condition, diabetes-related words were presented. After a practice session with prompts from all four conditions to familiarize participants with the task, participants completed the four different blocks (one for each condition) of the Stroop task with the order of each block randomized across participants. In each block, 20 word prompts relevant to the specific condition were presented on a computer screen and participants pressed computer keys labeled with red, yellow, blue, and green stickers to indicate the color of the word on the screen. Words were presented in a random color (red, yellow, blue, or green). Participants were instructed to press the key of the same color in which the word appeared on the screen. All stimuli were in capital letters, presented at the center of a light gray dialogue box on a white background, and were approximately 1 cm high. Each key press advanced the screen to the next prompt, or if no key was pressed, the screen would automatically advance to the next prompt after 3 seconds. There was a break of 30 seconds between each block. Computerized Stroop tasks have been validated with other samples of adolescents and adults (Klingberg et al., 2002; Mintzer and Stitzer, 2002; Olesen et al., 2004).
The diabetes Stroop portion of this task included the following 20 words: basal, bolus, carbohydrate, diabetes, eat, glucose, HbA1c, health, hyperglycemia, hypoglycemia, injection, insulin, lancet, Lantus, meter, needle, pump, shaky, sugar, and tired. Diabetes interference time was calculated as the difference in the average number of milliseconds (ms) a participant took to respond on each trial in the neutral condition compared to the diabetes condition, with longer response times indicating higher interference times. Greater diabetes interference time was examined as an indicator of greater attentional bias to diabetes cues.
Self-care inventory
The self-care inventory (SCI; La Greca, 2004) was used as a measure of diabetes management at baseline. This parent report scale contained 14 items assessing teens’ diabetes management such as SMBG and administering the right amount of insulin. Higher scores on each item are indicative of better diabetes management. Mean scores on the SCI were calculated by averaging scores across all 14 items. The validity of the SCI as an empirically supported measure of diabetes management in adolescents with T1D has been independently supported (Greco et al., 1990; Lewin et al., 2009). Reliability of this measure was also good in the current sample (alpha = .73).
SMBG
Self-monitoring of blood glucose (SMBG) was measured using teens’ blood glucose meters. The number of times teens self-monitored their blood glucose over the past 14 days was used to calculate an average to determine daily frequency of SMBG at baseline and follow-up.
Glycemic control
Glycated hemoglobin percentage (HbA1c) from a blood draw at study intake was used as a measure of glycemic control. Although participants were recruited from two clinic locations, all blood samples were analyzed in the same laboratory. HbA1c serves as an indicator of glycemic control over the past 3 months by measuring the level of glycated hemoglobin in a sample.
Analyses
The study was powered to detect intervention compared to control group differences in HbA1c and was not powered for the secondary analyses conducted in this study. Analyses were conducted using SPSS v.25 and Mplus v.8.1.5. First, Pearson correlation analyses were conducted to assess the bivariate associations between key study variables at baseline: diabetes Stroop interference time, the SCI, SMBG, and HbA1c. Next, the hypothesized model was tested through structural equation (SE) modeling, examining if improvements in attentional bias to diabetes cues mediated improvements in SMBG frequency post-intervention in the treatment versus the usual care group. Chi-square, comparative fit index (CFI), and root mean square error of approximation (RMSEA) were used as fit indices for all models. The following indices indicated good model fit: Chi-square p > .05, CFI > .9, and RMSEA < .05. We did not model correlated error terms for any variables. The hypothesized model was tested using bias-corrected bootstrapping with 95 percent confidence intervals (CIs). Unstandardized coefficients, standard errors, and confidence intervals also have been provided. We used residualized (baseline score as covariate) change scores for attentional bias to diabetes cues and SMBG, as this intervention primarily targeted increase in frequency of SMBG. The continuous covariates, baseline diabetes attentional bias and baseline SMBG, were grand mean centered. The only additional covariate was baseline pump use, a dichotomous variable. The hypothesized predictor of change in SMBG was treatment (0 = usual care and 1 = treatment).
Results
Bivariate associations of baseline diabetes Stroop task interference time with diabetes management and HbA1c were examined across all (N = 61) participants (see Table 1). A significant bivariate association was found between greater diabetes interference and poorer parent-reported diabetes management (r = –.31, p = .02), but not between diabetes interference and SMBG (r = .16, p = .21) or HbA1c (r = –.17, p = .20).
Descriptive statistics and correlations for baseline study variables.

SCI: self-care inventory; SMBG: self-monitoring of blood glucose; HbA1c: glycated hemoglobin percentage.
p < .05, **p < .01.
The hypothesis that changes in diabetes attentional bias would mediate improvements in SMBG frequency post-intervention for the treatment condition (N = 31) as compared to the control condition (N = 30) was tested using a SE model, which had good fit (see Figure 1 for more detail). The full model explained 38 percent of the variability in changes in diabetes attentional bias from baseline to post-treatment. Both the treatment condition (as compared to the control) and greater baseline attentional bias predicted reductions in diabetes attentional bias (treatment: b = –1.40, SEb = 0.47, p = .003, 95% CI [–2.25, –0.40]; baseline attentional bias: b = –0.92, SEb = 0.08, p < .001, 95% CI [–1.08, –0.74]). Change in attentional bias among those in the treatment condition (△M = –1.31 ms, SD = 2.51) as compared to those in the usual care condition (△M = –0.09 ms, SD = 2.60) corresponded to a 1.22 ms difference, with those in the treatment showing larger decreases in diabetes attentional bias. See Table 2 for statistics related to all direct and indirect effects.
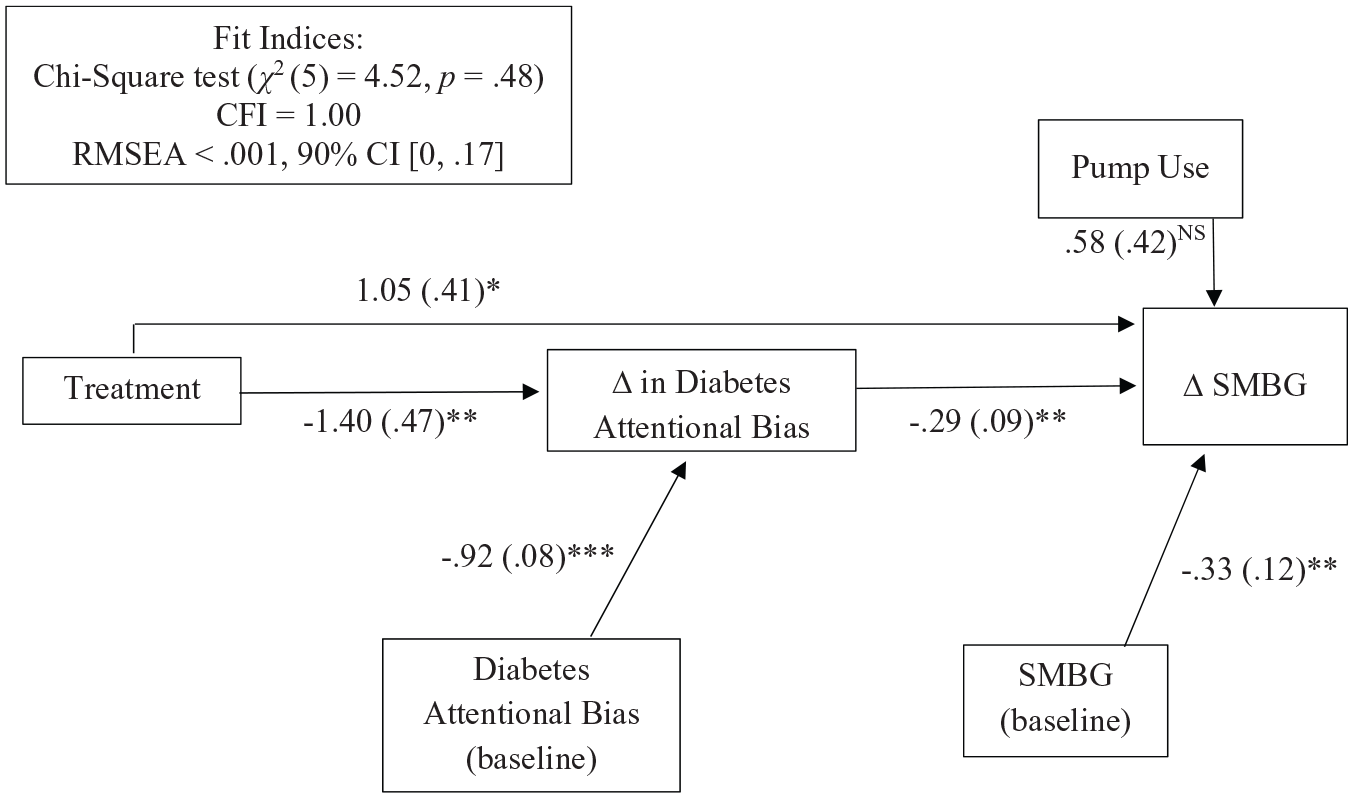
The multi-component treatment was associated with reductions in diabetes attentional bias and in turn increased SMBG at 6-month follow-up.
Direct and indirect effects of structural equation model examining if improvements in attentional bias to diabetes cues mediated improvements in SMBG frequency at post-treatment.

SMBG: self-monitoring of blood glucose; SE: standard error.
p < .05, **p < .01, ***p < .001.
The full model also explained 19 percent of the variance in change in SMBG from baseline to post-treatment. Treatment condition (as compared to the control condition), change in diabetes attentional bias, and SMBG at baseline all predicted change in SMBG from baseline to follow-up. Treatment was associated with a 1.05 unit increase in daily SMBG from baseline to follow-up (b = 1.05, SEb = 0.41, p = .01, 95% CI [.24, 1.88]). In addition, for every one unit decrease in diabetes attentional bias from baseline to follow-up, there was an expected 0.29 unit increase in daily SMBG (b = –0.29, SEb = 0.09, p = .001, 95% CI [–0.46, –0.12]). Also, for every additional unit of baseline SMBG, there was a 0.33 unit decrease in daily SMBG from baseline to follow-up (b = –0.33, SEb = 0.12, p = .005, 95% CI [–0.56, –0.12]). Pump status was not a significant predictor of change in diabetes attentional bias (b = 0.31, SEb = 0.46, p = .50, 95% CI [–0.56, 1.23]) or change in SMBG (b = 0.58, SEb = 0.42, p = .16, 95% CI [–0.15, 1.48]).
There was a significant total effect of treatment condition on changes in SMBG (total = 1.46, SEb = 0.37, p < .001, 95% CI [0.71, 2.14]). The total effect comprised a significant indirect effect of treatment on changes in SMBG through change in diabetes attentional bias (indirect effect = 0.40, SEb = 0.18, p = .03, 95% CI [0.13, 0.80]) and a significant direct effect of treatment (direct effect = 1.05, SEb = 0.41, p = .01, 95% CI [0.24, 1.88]). These findings indicate that a participant with average diabetes attentional bias who received the treatment experienced a 1.31 ms decrease in attentional bias and that reduction in diabetes-specific attentional bias explained improvements in SMBG at post-treatment.
Discussion
In this study, we examined if a multi-component intervention targeting diabetes management reduced attentional bias to diabetes cues and if so, if these reductions mediated improved diabetes management. Results showed that diabetes attentional bias decreased in response to the multi-component treatment, which included web-delivered MET/CBT, working memory training (CogMed), incentives, and parental contracting. Further, changes in attentional bias to diabetes cues in the treatment condition were associated with changes in SMBG, that is, attentional bias partially mediated treatment effects on diabetes management. Thus, these findings suggest that attentional bias to diabetes cues is malleable and that reducing attentional bias to diabetes cues in treatment may help to reduce avoidance of aversive health behaviors such as SMBG and improve diabetes management outcomes. In addition, although extant research has shown voluntary executive function capacities benefit diabetes management (Bagner et al., 2007; Duke and Harris, 2014; McNally et al., 2010), this study’s results are significant in that they suggest implicit or automatic biases in cognitive processing might also affect diabetes management.
These findings are consistent with results showing that working memory and CBT interventions targeting attentional bias can reduce attentional bias and related avoidance behaviors. For example, research has found that CBT can reduce attentional bias and avoidance of related behavior in clinical populations with anxiety (Hadwin and Richards, 2016; Reinecke et al., 2013; Waters et al., 2012), and one study, in particular, found that CBT and working memory training were effective in reducing attentional bias to threat and related anxiety symptoms among adolescents with anxiety (Hadwin and Richards, 2016). This study provides support for a similar effect in a different clinical population, adolescents with T1D, by showing that a CBT/working memory-based treatment reduced attentional bias to diabetes cues and related disease management challenges.
The intervention may have reduced attentional bias to diabetes cues through multiple pathways. There are data to support that CBT, through cognitive restructuring and exposure with incentives, may have changed the relation between stimulus (e.g. blood glucose checking) and response (e.g. feeling annoyed). These improvements in processing of negative stimuli or normalization of threat bias in response to CBT may in turn have lessened behavioral avoidance related to T1D management (e.g. avoidance of SMBG; Cowart and Ollendick, 2010; Ochsner et al., 2002; Reinecke et al., 2013). Although past research on CBT and working memory training supported the role of working memory training for attentional bias modification, a recent meta-analysis found that working memory training effects do not generalize to other overt, explicit cognitive skills (Melby-Lervåg et al., 2016), for example, attentional control. This suggests that the role of working memory training in modifying attention biases needs more careful consideration, for example, it may be that the working memory training potentiates the impact of CBT on implicit cognitive processes, for example, attentional bias, before warranting greater utilization. Finally, although there is less evidence to support this pathway, it remains possible that parental contracting influenced attentional bias to diabetes cues. Evidence suggests family cohesion and parental response can influence children’s attentional bias to threat (Hughes-Scalise and Connell, 2014; Luecken et al., 2006). However, more research is needed to understand if this family functioning influences attentional bias to illness- or disease-related cues, in particular. Future research investigating these pathways with an a priori hypothesis is needed to understand which of these intervention components (CBT, working memory training, and parental contracting) are mostly related to reduced attentional bias to diabetes cues.
The results finding that decreased attentional bias was associated with improved engagement in (or reduced avoidance of) diabetes management behaviors may also provide support for the hypervigilance-avoidance hypothesis. This hypothesis would posit that attentional bias to diabetes cues (e.g. lancet), which represent threat, would be initially and automatically heightened among adolescents with T1D and above target glycemic control; then following that initial hypervigilant response, adolescents would try to avoid the stimuli to reduce the anxious state, leading to attentional and behavioral avoidance of diabetes management activities (e.g. not engage in SMBG; Bar-Haim et al., 2007; Mogg et al., 1997). By extension, the treatment’s reduction of attentional bias to diabetes cues may also have decreased the subsequent attentional and behavioral avoidance of diabetes management behaviors, leading to improved engagement in behaviors like SMBG.
These findings should be interpreted in the context of the study’s limitations. This sample comprised mostly White adolescents, and it is possible that these findings may not generalize to adolescents who identify with different racial or ethnic minority backgrounds. Also, this sample included adolescents with HbA1c greater than or equal to 8 percent, limiting generalizability to the small proportion of adolescents with T1D (21%) experiencing in-range glycemic control (Wood et al., 2013). In addition, this study was not designed to identify which component of the intervention (e.g. MET/CBT, working memory training, and parent contracting) was most important in driving reductions of attentional bias to diabetes cues. Future research with a priori hypotheses is needed to parse out which components are responsible for change and replicate the finding that changes in attentional bias to diabetes cues is associated with improvements in diabetes management. Finally, the sample size was powered to detect differences in HbA1c in the context of the primary intervention aims and not for this study specifically, meaning this study may have been underpowered.
Importantly, the modified diabetes Stroop task used in this study requires further development, as control words were not matched for semantic properties including world length, syllables, and frequency in language (Field and Cox, 2008). More research will be needed to further develop and validate a Stroop task to measure attentional bias to diabetes cues that meets all of the standards identified by Field and Cox (2008) and that is tested in a larger, more diverse sample, as well as over a wider range of HbA1c. Finally, it may be that the relation between attentional bias and diabetes management is not linear. The Jessop et al.’s (2004) asthma study measured management of asthma as a categorical variable and found that high attentional bias significantly discriminated low adherence, but there was also an association trending toward significant for discriminating high adherence. This observation points to the possibility that attentional bias serves to reduce or promote adherence behaviors depending on the illness representation, such that positive illness representations with high attentional bias may serve to improve disease management. Future studies should explore this pattern of associations in a larger sample that includes adolescents with the full range of both adherence and glycemic control.
Finally, this study offers evidence to further investigate diabetes-specific attentional bias and additional implicit cognitive processes that may influence diabetes management and glycemic control in adolescents with T1D. This study also supports that attentional bias to diabetes cues is malleable, can be reduced through intervention, and may confer improvements in diabetes management. These findings point to the potential value of a novel intervention (e.g. diabetes-focused ABM) aimed at attentional retraining among adolescents with T1D who evidence biases in processing of diabetes-related cues and are struggling to maintain optimal disease management. Moreover, it is likely that those with elevated attentional bias to diabetes cues would benefit the most from this treatment approach, as this study found that those with greater attentional bias to diabetes cues experienced the greatest reductions in attentional bias, which in turn predicted changes in SMBG. However, given individuals with higher attentional bias more generally have shown greater anxiety (Dudeney et al., 2015), these treatments may need to be tailored to meet the needs (e.g. higher psychopathology) of this particular population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute of Child Health and Human Development (Grant No. DP3 HD076602) and the National Institute on Drug Abuse (Grant No. P30 DA029926).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Trial registration
The primary intervention was registered with the ClinicalTrials.gov registry (No. NCT01722643).