
Abstract
Apathy—a reduction in goal-directed behaviour, cognition, and emotional responsiveness—is a highly prevalent, debilitating symptom in people with amyotrophic lateral sclerosis (pwALS). This study investigated the association between apathy in 69 pwALS and their 54 informal caregivers and constructs from social cognitive theory and self-determination theory. Participants also provided subjective accounts of apathy in semi-structured interviews. Multiple regression analysis demonstrated that constructs from both motivational theories were significant predictors of overall apathy scores and its sub-domains (executive, emotional, initiation), accounting for 32%–64% of the variance. Specifically, frustration of the basic psychological need for competence was a consistent and prominent predictor of greater apathy. Qualitative findings revealed that pwALS lack a clear awareness of apathy, often experiencing it as a manifestation of activities requiring increased physical and temporal effort. Future research should use psychosocial theories to understand apathy and develop interventions.
Keywords
Introduction
Amyotrophic Lateral Sclerosis (ALS) is a progressive neurodegenerative disorder leading to muscle weakness, impaired movement, and ultimately, respiratory failure (Hobson and McDermott, 2024). The distress and burden of the disease affect people with ALS (pwALS) and their family members or informal caregivers, and the progression of disability causes social, emotional, and financial strain (Hobson and McDermott, 2016). ALS typically leads to death within 2–4 years (Verber et al., 2019); however, the disease is heterogeneous and the needs of each individual with ALS and their family are unique. ALS prevalence is estimated at two per 100,000 globally, with incidence rates varying across populations (Marin et al., 2017; Pliner et al., 2014).
While ALS is primarily characterised by motor impairments, cognitive and behavioural symptoms are increasingly recognised as significant components of the disease. Apathy is defined as a reduction in goal-directed behaviour, cognition, and emotional responsiveness (Robert et al., 2018) and is present in 30%–70% of pwALS (Radakovic et al., 2015, 2025). There are three domains to apathy (Radakovic et al., 2016). Executive apathy describes the inability to engage several cognitive processing functions such as attention or organisation, which restrict pwALS from developing more detailed plans to take part in activities. Emotional apathy refers to a decrease in the ability to link an affect to an emotional signal; whereby, pwALS may experience reduced willingness to engage in activities or lack the ability to consider the consequences of actions. Initiation apathy is the difficulty or inability to engage in the self-generation of behaviours or thoughts (Levy and Dubois, 2006).
Apathy is associated with diminished quality of life and increased informal caregiver burden (Chiò et al., 2010; Radakovic et al., 2025) and may also reduce treatment adherence. Therefore, although interventions such as Riluzole, multidisciplinary care and non-invasive ventilation are linked to prolonged survival, if apathy prevents pwALS from engaging with these interventions (or the decision-making process for these), their full life-extending effects may not be realised (Aridegbe et al., 2013; Hobson and McDermott, 2024).
Despite its prevalence, apathy in ALS remains under-researched, particularly in terms of its predictors and potential interventions (Francis et al., 2023; Radakovic et al., 2025). To date, many studies exploring apathy have focussed on utilising neuroimaging to link neural structures and neuro-modularly systems to specific aspects of motivated behaviour (Husain and Roiser, 2018; Le Heron et al., 2018). With previous research focussing on the physiological elements of apathy, exploration into the involvement of psychosocial elements has been overlooked, limiting our current understanding of apathy and preventing the development of theory-informed treatments.
Motivational theories have been used to explain and predict motivation and behaviours in multiple conditions (Michie et al., 2007; Painter et al., 2008) and therefore may provide insight into apathy in ALS. This mixed-methods study will explore the association between apathy in pwALS and two widely applied motivational theories; social cognitive theory—which focuses on the quantity of motivation—and self-determination theory—which focuses on the quality of motivation.
Social cognitive theory (Figure 1) emphasises the role of self-efficacy in goal-directed behaviour, with higher self-efficacy correlating with better health outcomes and an increased likelihood a behaviour will occur (Bandura, 1986). Social cognitive theory-based interventions have guided and been implemented in the development of health promotion strategies, as well as disease prevention and treatment across a range of long-term health conditions (Dougherty et al., 2022; Manjarres-Posada et al., 2020).
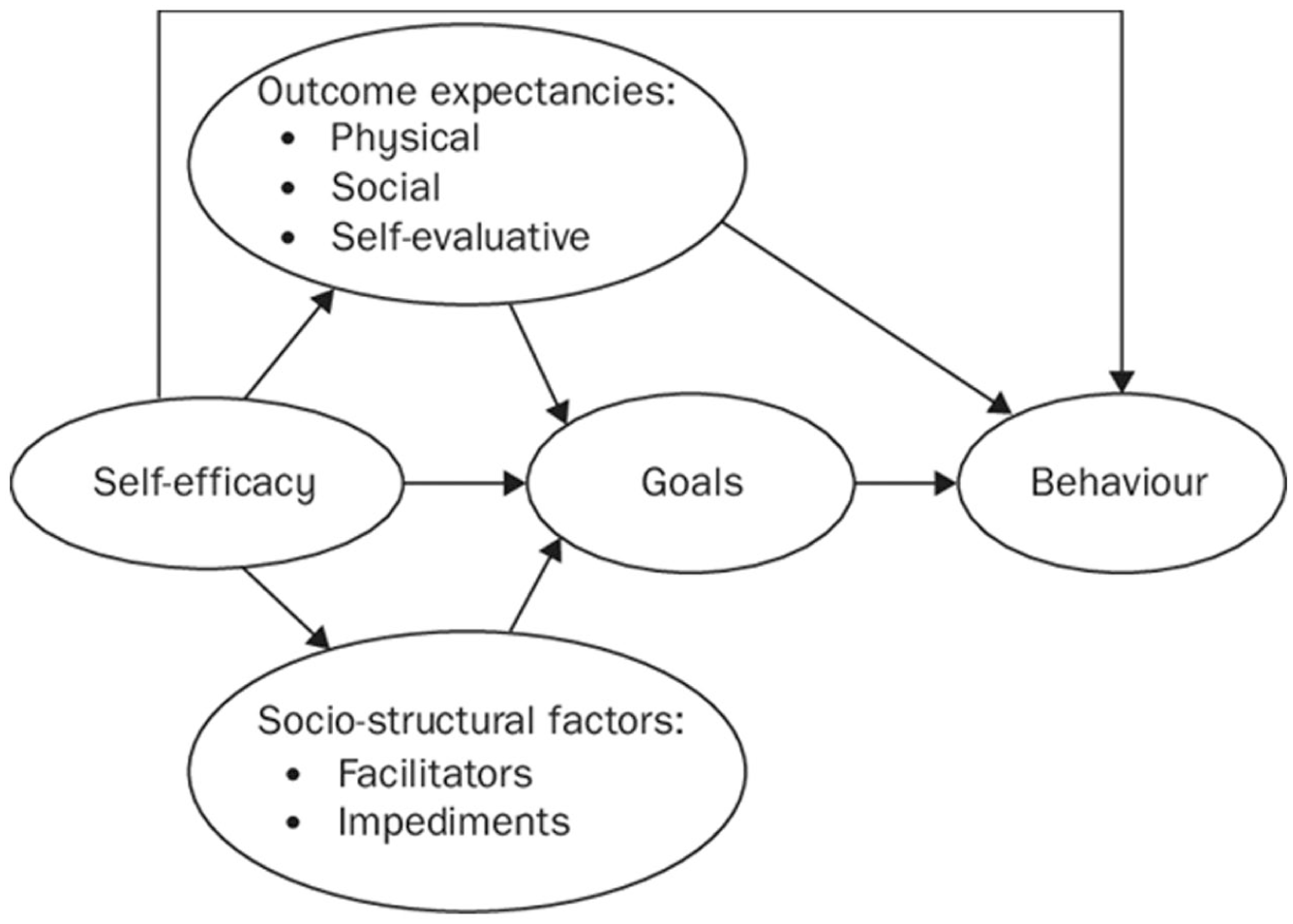
Social cognitive theory (Bandura, 2023).
Self-determination theory (Figure 2) focuses on types of motivation from amotivation (no motivation to conduct a behaviour) to intrinsic motivation (conducting a behaviour for the sheer joy). The different types of motivation are influenced by how much a behaviour satisfies three basic psychological needs; autonomy, competence, and relatedness (Ryan and Deci, 2017). Autonomy is the ability to be a causal agent, competence refers to the need to feel environmental effectiveness, and relatedness is the need to feel connected to other individuals (Ryan and Deci, 2017). These needs can also be frustrated, which is the active hindrance of need satisfaction and could lead to a behaviour being less likely to be conducted (Knox et al., 2021b). Self-determination theory-based interventions have demonstrated efficacy in promoting self-management, smoking cessation, and physical activity (Knox et al., 2025a; Williams et al., 2006; Wilson et al., 2006).
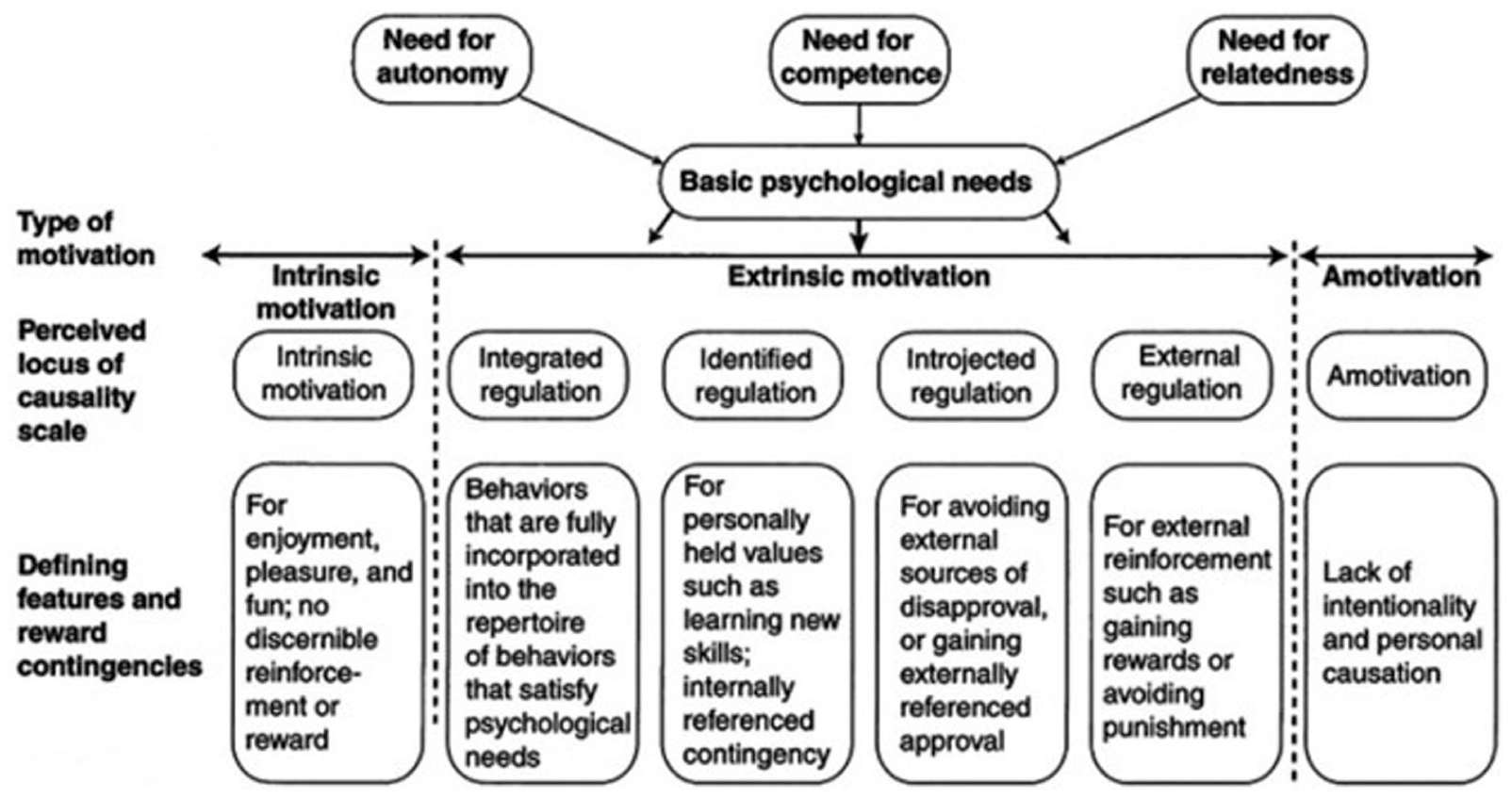
Self-determination theory, figure adapted from Hagger and Chatzisarantis (2007) and Knox et al. (2021b).
Methods
Design
This study used a mixed-methods design with cross-sectional, quantitative questionnaires and qualitative semi-structured interviews. The aims of the study were to explore the association between apathy in ALS, social cognitive theory, and self-determination theory, and the experiences of people with ALS with apathy.
Data were collected between April 2023 and April 2025. The study was approved by an NHS Research Ethics Committee (23/YH/0038).
Participants
PwALS were either recruited from a list of those attending the Sheffield MND Care and Research Centre by a postal invitation, or through an online research platform called Join MND Research. If the individual with ALS participated, a family member/informal caregiver was also invited. PwALS also had the option to take part in a semi-structured interview. PwALS had to have ALS, be at least 18 years old, understand verbal and written English, and have capacity to give written informed consent to be eligible. Family members/informal caregivers additionally had to be providing informal care for someone with MND or be a family member to be eligible. There were no exclusion criteria.
Sixty nine pwALS and 54 family members/informal caregivers completed the questionnaires. Their demographics are presented in Table 1.
Participant demographics.
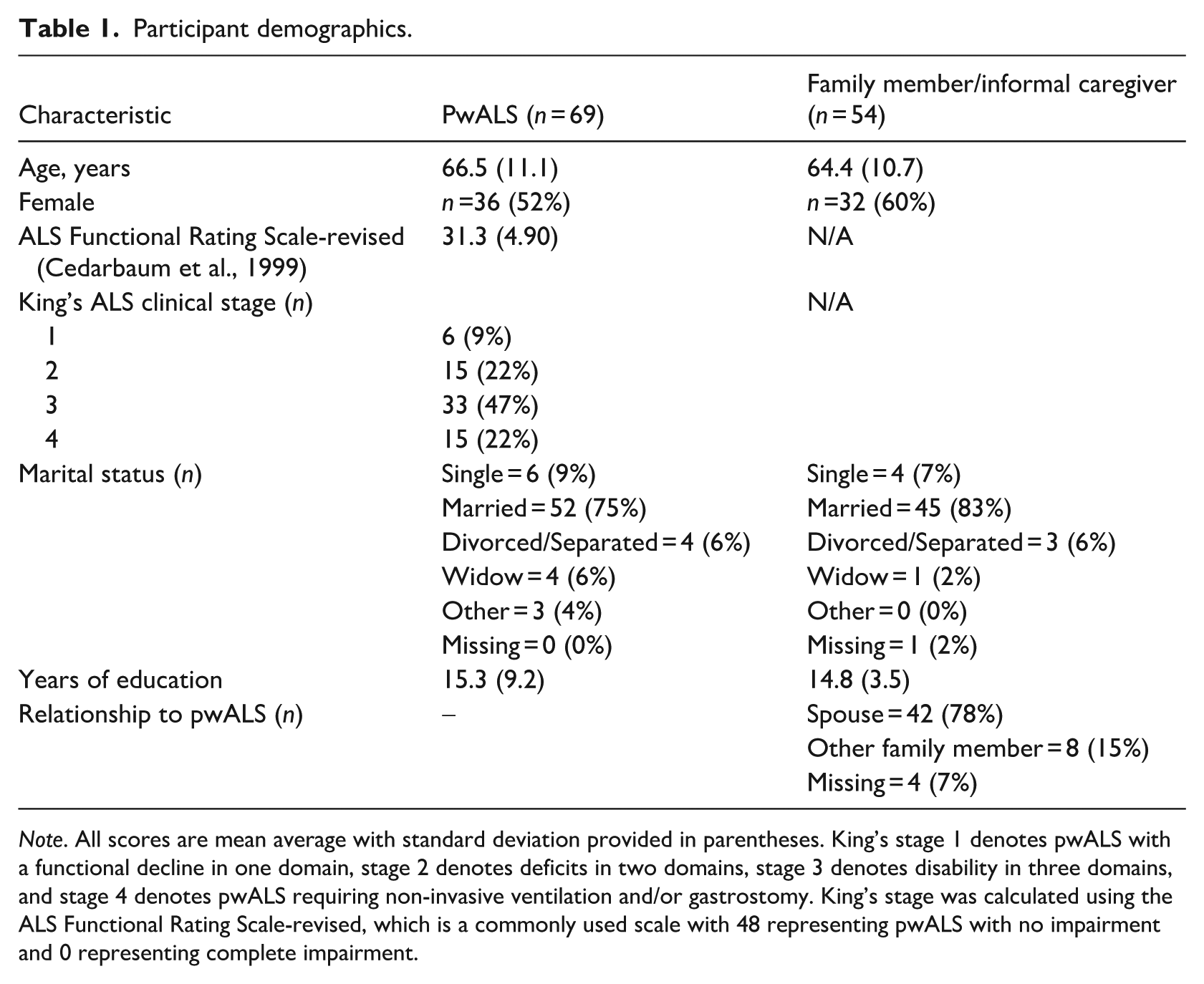
Note. All scores are mean average with standard deviation provided in parentheses. King’s stage 1 denotes pwALS with a functional decline in one domain, stage 2 denotes deficits in two domains, stage 3 denotes disability in three domains, and stage 4 denotes pwALS requiring non-invasive ventilation and/or gastrostomy. King’s stage was calculated using the ALS Functional Rating Scale-revised, which is a commonly used scale with 48 representing pwALS with no impairment and 0 representing complete impairment.
Eight pwALS took part in an interview. Their average age was 67.1 (SD = 9.2), five were men, and three were female.
Data collection
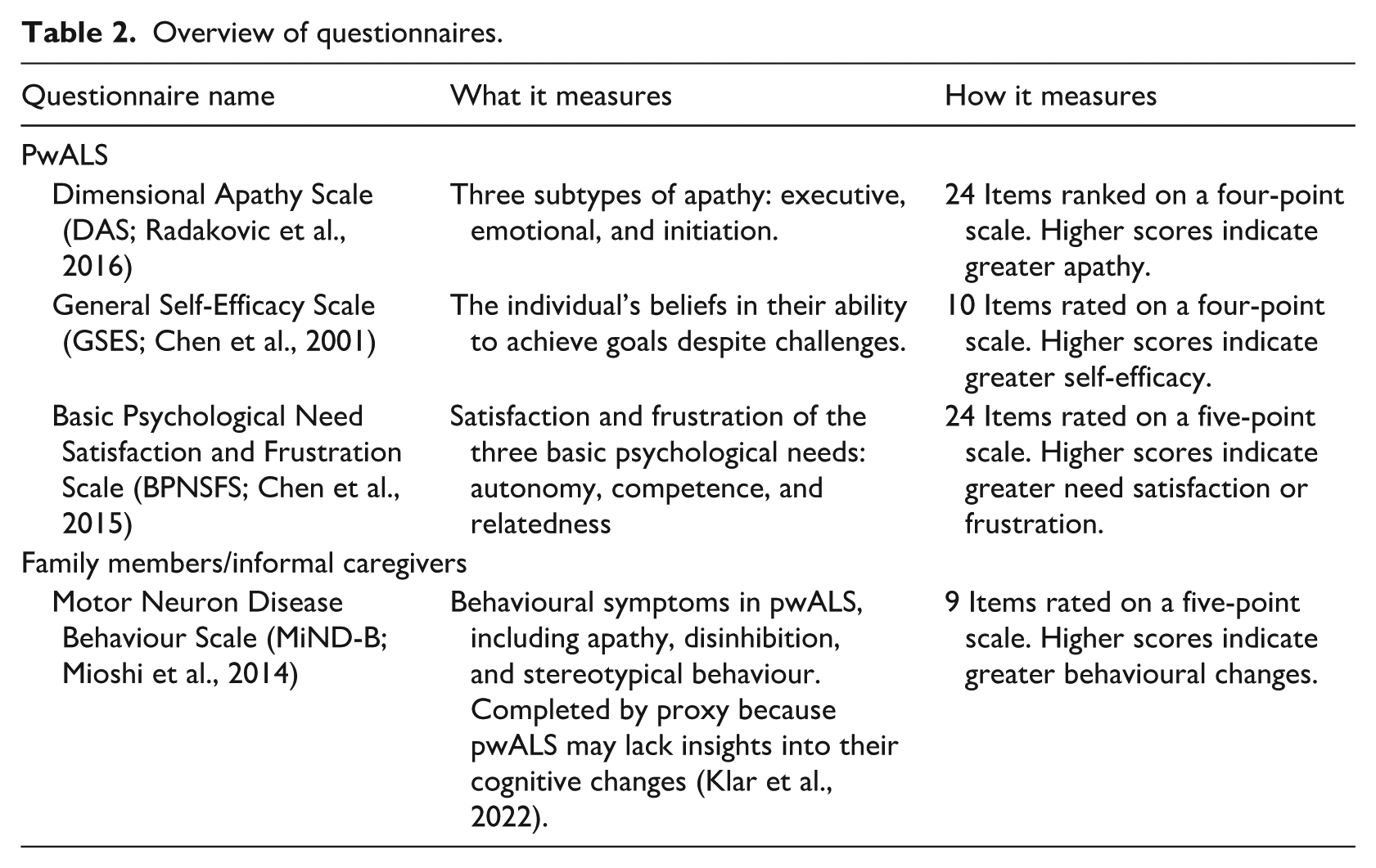
Three questionnaires were completed by pwALS at one timepoint and one questionnaire by family members/informal caregivers (see Table 2). If the pwALS could not physically complete the questionnaires (e.g. due to hand or arm weakness), a family member/informal caregiver could support them. Questionnaires were either completed on paper, or online (if recruited by Join MND Research).
Overview of questionnaires.
Online semi-structures interviews were conducted by LK and MWE using Google Meets. Questions focussed on understanding and experiences of apathy. The interview schedule (Appendix 1) was not based on social cognitive theory or self-determination theory but enabled participants to discuss apathy and motivation-related topics. Interviews lasted between 30 and 60 minutes and were audio-recorded and transcribed verbatim.
Data analysis
Multiple regression analyses were performed to explore whether apathy (measured by DAS or MiND-B) is associated with social cognitive theory (measured by GSES) and self-determination theory (measured by BPNSFS). Separate regression analyses were performed using the DAS overall score as the dependent variable, followed by the three DAS subtypes (executive, emotional, and initiation), and lastly the MiND-B overall score (a proxy measure of apathy). GSES and the six BPNSFS subtypes (autonomy, competence, and relatedness satisfaction/frustration) were the only dependent variables used, entered using a backwards elimination approach (see Figure 3). There was no missing data from the questionnaires.
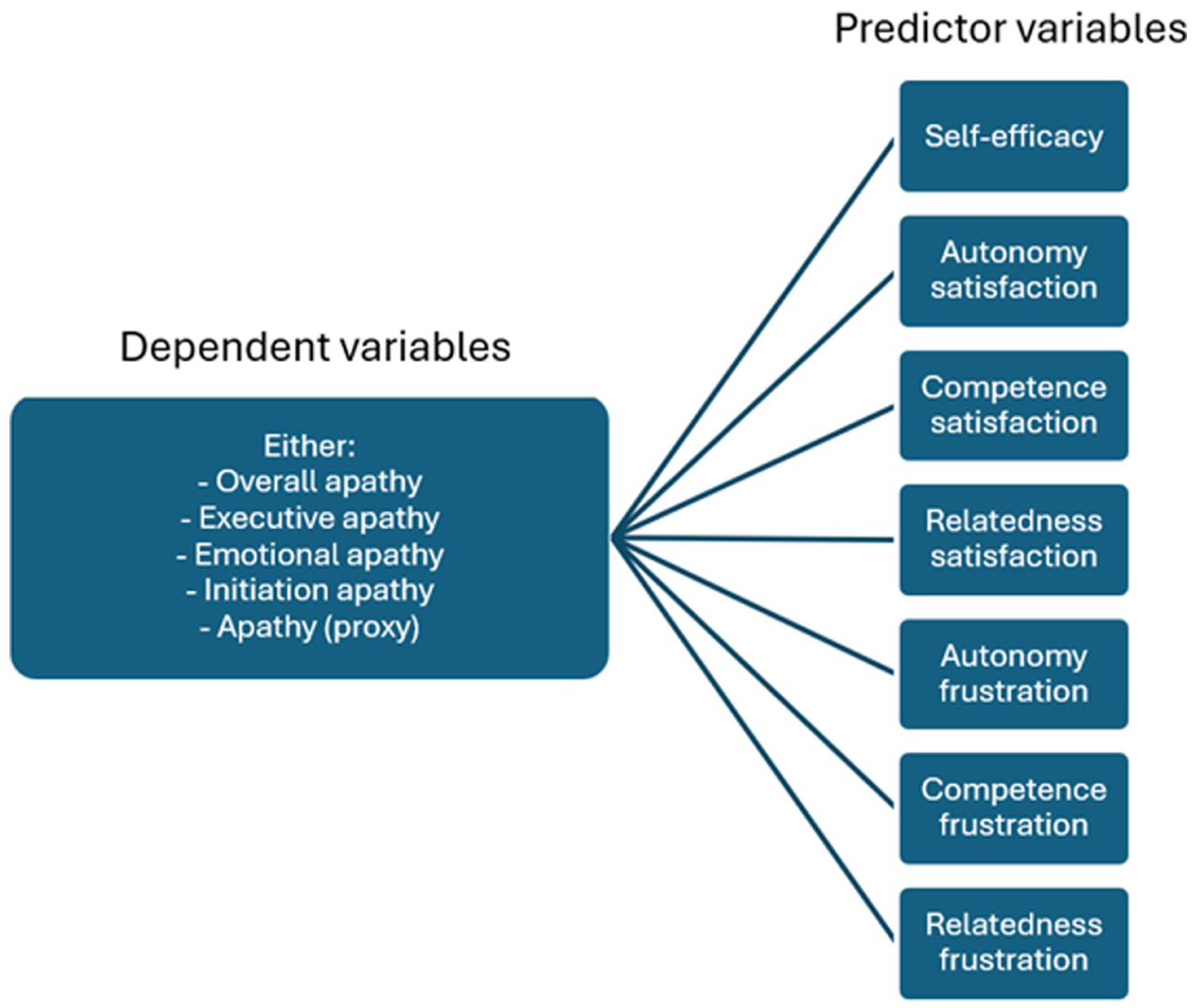
Overview of regression analyses.
An a priori sample size calculated using a medium effect size, alpha of 0.05 and beta of 0.80 recommended 103 participants would be required.
Pearson’s correlation assessed relationships between DAS (both overall and subtype scores) and MiND-B scores to explore if levels of apathy reported by pwALS were related to levels reported by family members/informal caregivers.
Reflexive thematic analysis (Braun and Clarke, 2019) was used to develop themes from transcripts created from the audio recordings of the semi-structured interviews by two researchers (LK and MWE). The researchers were collaboratively involved in the whole, iterative qualitative analytical process from familiarisation to theme naming (see Braun et al., 2014 for a detailed overview of reflexive thematic analysis) and focussed on latent meanings within the data. Although the quantitative element of this study adopted a deductive approach, the qualitative element maintained an inductive approach to explore how participants described apathy in general—not solely in relation to social cognitive theory and self-determination theory.
Results and discussion
Quantitative results and discussion
Descriptive statistics for each of the questionnaires are displayed in Table 3.
Descriptive statistics for questionnaire responses.
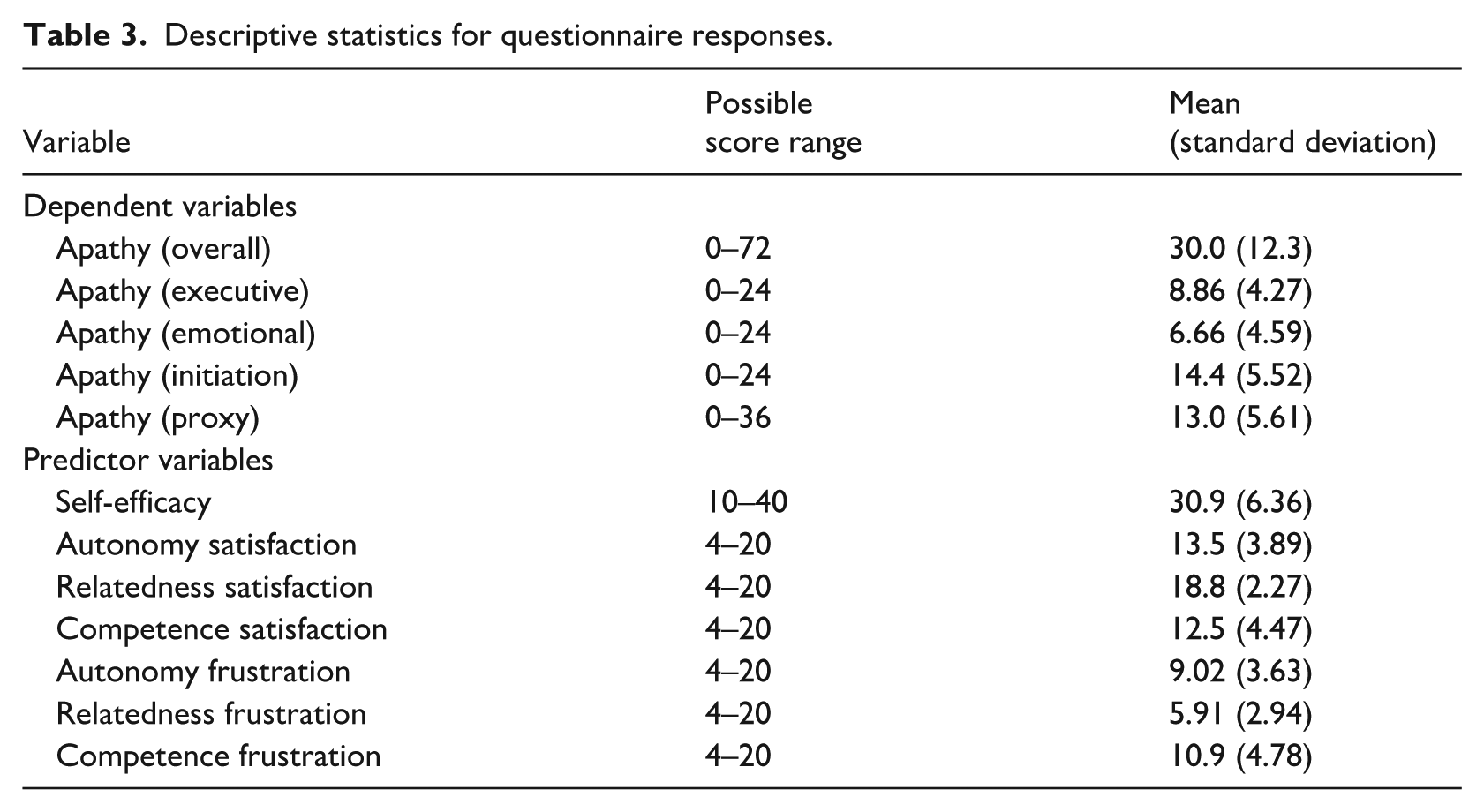
Table 4 shows the results from the five regression analyses alongside the standardised beta coefficients of the predictor variables that remained after the elimination of non-contributory variables. All five were statistically significant, indicating that self-efficacy and the satisfaction and frustration of the basic psychological needs were strongly associated with reported apathy. The observed power for all regression analyses was at least 98%.
Multiple regression equations for the five analyses.
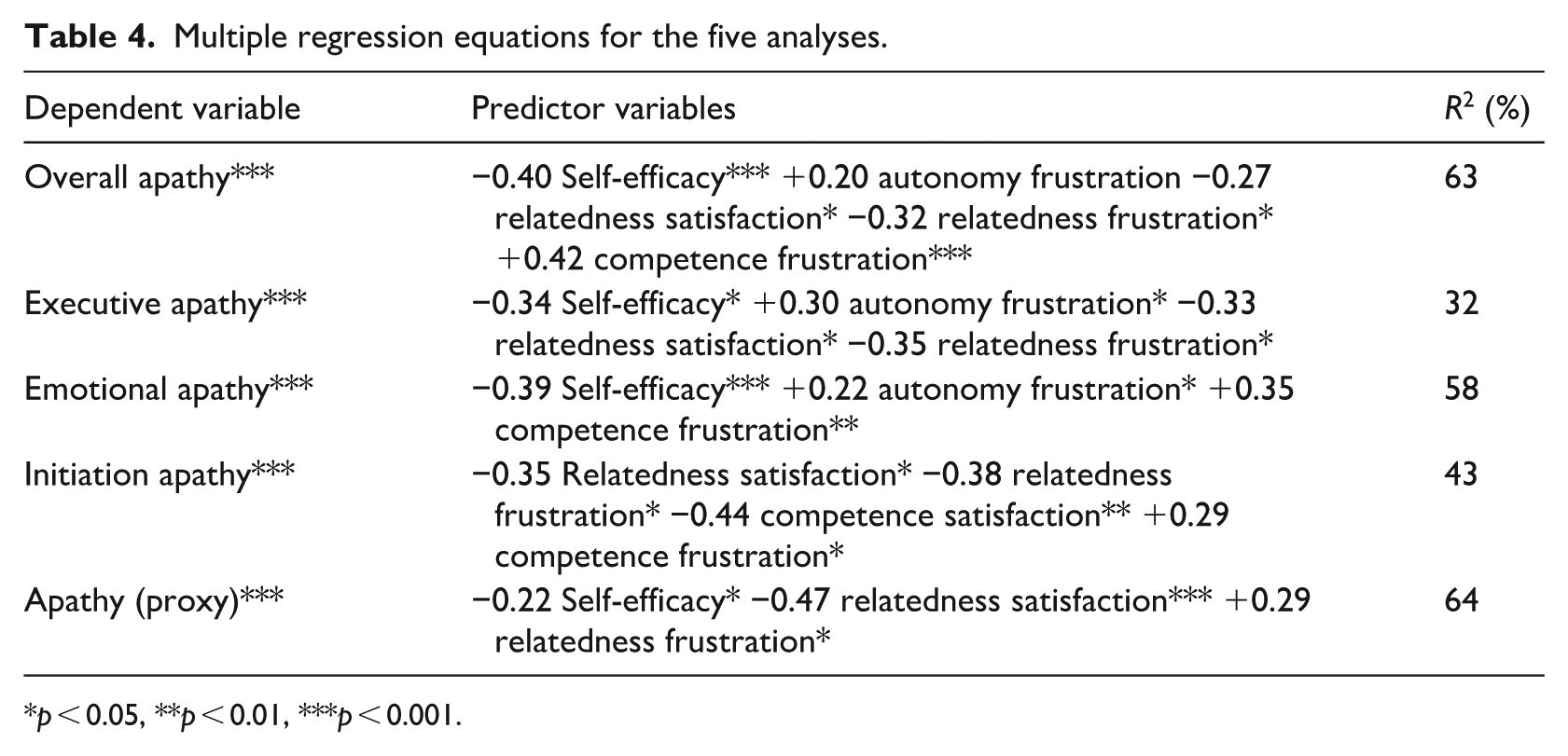
p < 0.05, **p < 0.01, ***p < 0.001.
Despite relatively low levels of need frustration reported (see Table 3), these variables were significant predictors of apathy (Table 4). Thus, similar to previous research in other conditions, even low levels can have a negative impact on behaviour (Knox et al., 2021b) and interventions aiming to decrease frustration could have beneficial results.
Aligning with previous studies, compared to other sub-types, initiation apathy was greatest (Radakovic et al., 2025) and predicted by both the satisfaction and frustration of the needs for competence and relatedness. Competence was the most frustrated basic psychological need in this study, where this finding is strengthened by the qualitative interviews (see the ‘effortful activities and adaptations’ theme). However, the role of relatedness frustration is less clear, as most of the regression analyses found a negative association between this variable and apathy. This suggests that as relatedness frustration increases, apathy decreases, which does not conform to self-determination theory (Ryan and Deci, 2017). The interviews do not elucidate this finding, as they describe examples of how participants were reluctant to go out in public for fear of being treated differently (see ‘seeing and being seen by other peoples’), which was interpreted as relatedness frustration associated with an avoidance of behaviour. Previous studies with similar findings have found this to increase relatedness frustration and thereby decrease a behaviour being conducted (Knox et al., 2021b), rather than the reverse. Relatedness is considered the key basic psychological need in behavioural initiation (Ryan and Deci, 2017); therefore, future research should aim to increase our understanding of how the frustration of this need interacts with apathy in pwALS. Although this future research should consider that approximately 33% of pwALS live alone (Gamble et al., 2025).
A Pearson correlation analysis demonstrated a significant positive relationship between overall apathy scores and proxy apathy (i.e. MiND-B) scores (r = 0.62, p < 0.001), with a similar finding between proxy apathy scores and executive apathy (r = 0.51, p < 0.001), emotional apathy (r = 0.65, p < 0.001), and initiation apathy (r = 0.44, p < 0.001). This demonstrates that apathy measured by the individual with ALS and family members/informal caregivers were similar.
Qualitative results and discussion
Two overarching themes were developed from the transcripts: ‘understanding and experiencing apathy’ and ‘relationships and control in ALS’.
Understanding and experiencing apathy
Within this theme, participants described their perspectives on apathy and how they experienced this symptom. There were two sub-themes.
‘A lack of apathy awareness’ describes how almost every participant had a different view on what apathy was, which also extended to whether the participants themselves felt they experienced apathy. ‘Effortful activities and adaptations’ explores how participants felt everyday activities had become harder and how adaptations could be used to overcome symptoms.
A lack of apathy awareness
Participants described apathy in multiple ways, with little agreement between their accounts, or between how easy it would be to overcome this symptom.
I suppose it's just laziness. Just everything is too much effort. So, I mean it's not something I have a problem with as such. Participant 1.
Terms such as ‘laziness’ or ‘unwillingness’ were often used by participants throughout the interviews, which were interpreted by the researchers as attributing an element of shame or ability of participants to choose to become ‘willing’ again. Despite some participants stating they themselves did not have apathy, in several interviews they then described how they had feelings of ‘a lack of motivation’ or stated that others thought they may have this symptom.
Lack of motivation. Apathy is not really wanting to do something and probably getting less willing to do things. I don't think I suffer from apathy, but other people might think [I do] because I am doing less now than I was. Participant 2.
The quantitative analysis demonstrated that pwALS and family members/informal caregivers reported similar apathy scores. Therefore, when asked closed questions (via questionnaires) responders may be able to provide accurate information; however, when asked open questions (via interviews) participants may not process the knowledge or language to describe their feelings or symptoms. This theory is strengthened by many participants not knowing how common feelings of apathy were.
It's not something I've ever discussed with anybody. So, whether they do feel apathetic, I have no idea. Participant 5.
The lack of a common language to describe apathy and its effects may be hindering the ability of clinical care or research exploring this symptom. Future research should aim to develop this shared understanding to support the development of clinical care interventions.
Effortful activities and adaptations
Participants described how the progression of ALS made activities more difficult. Therefore, although they were still capable of certain activities, they did not see them as worth the time and effort.
Now it is really a lot of effort. So, for example to go down to the coffee shop that is half a mile down the road. It will involve the best part of half an hour to get ready and dressed and out in van, down the road, out of the van, into the coffee shop. So, there's an awful lot of things there. Participant 8.
This quote was interpreted as a description of how the need for competence can be frustrated. As described above, competence was the most frustrated need, and as discussion around this need largely revolved around the physical capability of participants, it is likely that this would increase for pwALS as muscle impairment increases.
Many of the participants described that although they had lost the ability to fully engage in activities which they used to enjoy, they could still engage in alternative ways. Participants used a variety of methods, where forward planning and habit formation were key strategies and helped overcome any feelings of apathy.
I'm quite disciplined in making things a habit. . . I've got an assisted exercise bike. So, I do 15 minutes on that every morning. I've got quite a schedule to my day because carers come in usually at lunchtime. So, I have my routines that I have to stick to really. So that kind provides some structure Participant 1.
Previous research describes how people with initiation apathy have relatively uninhibited abilities if they can overcome the initial lack of motivation (Levy and Dubois, 2006). Within the two presented accounts in this sub-theme, Participants 8 and 1 both demonstrate their planning abilities (interpreted as a lack of Executive apathy), but where Participant 8 appeared daunted by the cognitive load of the activity, Participant 1’s use of routine may provide an initial prompt to overcome initiation apathy. Relatedness is the key basic psychological need in beginning a behaviour or routine (Ryan and Deci, 2017); therefore, this strengthens the above recommendation for future research to increase our understanding of this concept.
Relationships and control in ALS
This theme focussed on how participants approached a range of relationships and tried to maintain control over ALS. There were two sub-themes.
‘Seeing and being seen by other people’ explores how participants had varied relationships with other pwALS, support groups or the public. ‘Maintaining control’ was a small but very salient theme and describes the tension between independence and asking for help.
Seeing and being seen by other people
Multiple participants described an unwillingness to attend ALS support groups as they did not want to see other pwALS with a more advanced disease. Although some participants had people they could talk to instead, others actively hid their feelings from friends and family.
I talk to my wife [about apathy] just no one else really knows. I don't want to start, not to my friends. Although eventually [I will]. But at the moment, I can hide it, if you want to put it that way. Participant 6.
Although there may be several reasons why pwALS do not want to attend support groups or discuss symptoms with friends, an unwillingness to discuss apathy could be related to the lack of a common language to discuss apathy as discussed above.
Participants also described how ALS and apathy had resulted in a loss of identity and were hesitant to go out in public due to how they felt others perceived them.
What I don't want is a situation where I walk into a room [and people] treat me differently. I want to be treated as I normally would, which is important I think. Participant 4.
The quantitative results found relatedness satisfaction to be relatively high and relatedness frustration to be low (see Table 4). However, as exemplified by the two participant quotes, this theme was interpreted by the researchers to demonstrate how ALS inhibits the need of relatedness. In fact, the descriptions of how ALS restricts relatedness closely aligns with descriptions in other diseases reported previously (Knox et al., 2021a, 2025b).
Maintaining control
Participants described the importance of maintaining independence and, through this, control over ALS, which has similarly been highlighted in previous research (Hogden, 2014). This could create worry that the loss of independence would result in the loss of being able to cope with the condition.
‘If I ever lose the ability to have my own transport, I'm not quite sure yet how I would cope with that mindset. At the minute, I have my own autonomy with what I do, where I go, who I see, and that type of stuff. If that changed, I might have a different mindset to it all’. Participant 4. Therefore, participants described how they maintained independence through practical adaptations to tasks which are common in ALS. However, they also described an avoidance of adaptations as this could represent a loss of independence.
“I wouldn't use the stair lift; I would only use it if I absolutely had to”
“Is that because you want to keep your independence before you start”
“Absolutely. that's the main thing”
Thus, this theme describes a delicate balance between adaptations that may support autonomy and those that represent the abilities they have lost. Previous literature has also described how pwALS avoid adaptations (Glennie et al., 2023), which could make it difficult to implement adaptations to support people to overcome apathy.
Overall discussion
The aim of this study was to understand the association between apathy, social cognitive theory and self-determination theory and explore the experiences of pwALS with apathy. The quantitative analyses highlight how significant levels of apathy are related to both motivational theories. This remained constant when apathy was considered as a whole, by three sub-domains, or measured by proxy. The qualitative interviews begin to explore how pwALS understand and experience apathy in terms of activities taking greater effort; however, there is limited consensus in how this symptom is understood.
From a theory perspective, the quantitative and qualitative findings highlight the importance of autonomy and self-efficacy. Additionally, even small levels of need frustration can have significant effects, which underline the importance of considering the ‘dark side’ of motivation whilst conducting motivation research (Knox et al., 2021b, 2025b). However, this study also provides conflicting accounts regarding the role of relatedness, which future research should aim to elucidate.
From a clinical care perspective, the ability of both social cognitive theory and self-determination theory to significantly contribute within this study supports their use in future research and the development of interventions to support pwALS with apathy. As attempts to integrate social cognitive theory and self-determination theory into one unified theory have had mixed results (Sweet et al., 2012, 2014), using constructs from either or both theories rather than an amalgamation appears warranted.
The findings of this study suggest that interventions supporting self-efficacy or decreasing need frustrating stimuli may be effective to mitigate apathy in pwALS. Acceptance and Commitment Therapy uses a combination of elements including motivation and behaviour change techniques to support pwALS to re-engage with life-enriching activities and is associated with improved quality of life (Gould et al., 2024). It is possible that this therapy works through social cognitive theory and self-determination theory concepts and could be effective at supporting pwALS with apathy and future research should explore these possibilities. Additionally, Acceptance and Commitment Therapy could be beneficial to use alongside other interventions to overcome some of the difficult emotions described within the qualitative interviews, such as the acceptance of apathy as a symptom and conflicting perceptions of support for independence.
An alternative could be to aim interventions at informal caregivers. However, although clinical guidelines frequently mention informal caregivers as important to supporting pwALS (National Institute for Health and Care Excellence, 2019), there are few interventions that actively involve training informal caregivers in elements of treatment. A notable exception is the MiND Toolkit, which is aimed to provide informal caregivers training and increases awareness of behavioural changes in ALS (Mioshi et al., 2024). Future research is needed to explore how to support pwALS to maintain control, without the need for interventions becoming evidence of a loss of control.
From a research perspective, although participants’ perceptions of their own symptoms are best, the similarity in findings when using participant-derived scores (from the DAS) compared to proxy scores (from the MiND-B), alongside the high correlation between measures, does demonstrate the value of proxy-derived apathy scores. This finding is similar to previous findings (Radakovic et al., 2025) and proxy-measures may be beneficial if there are worries that pwALS lack insight into cognitive changes (Klar et al., 2022).
A limitation of this study is the cross-sectional design disabling the ability for causation to be drawn from the findings, alongside the relatively small qualitative component. Although these limitations do restrict the application of the findings, this study represents a proof-of-concept for the use of motivational theory to understand the psychosocial determinants of apathy in ALS. Despite fewer participants being recruited as recommended by the a-priori sample size calculation (i.e. 69 pwALS out of the target of 103), the observed power for all regression analyses was at least 98%. This high observed power was due to very large effect sizes, as demonstrated by the large R2 values in Table 4.
Future research should build upon this study and overcome the limitations by measuring apathy longitudinally and including a larger qualitative element. The inclusion of family members/informal caregivers and healthcare professionals would also provide a beneficial perspective to understand how to support pwALS with apathy.
Footnotes
Appendix 1
Acknowledgements
We would like to thank the Join MND Research team and its users for supporting this study to recruit participants.
Ethical considerations
This study was approved by the Yorkshire and The Humber-Bradford Leeds Research Ethics Committee (approval no. 23/YH/0038) on 01/02/2023.
Consent to participate
Respondents gave written informed consent before starting the questionnaires and/or interviews.
Consent for publication
Respondents gave written informed consent for their data to be published, including anonymised quotes.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to not having the ethical approval to make the data publicly available, but are available from the corresponding author on reasonable request.