
Abstract
Depression in people with amyotrophic lateral sclerosis, a fatal and progressive neurodegenerative disorder, is a serious issue with important clinical consequences. However, physical impairment may confound the diagnosis when using generic questionnaires. We conducted a comprehensive review of literature. Mean scores from depression questionnaires were meta-regressed on study-level mean time since onset of symptoms. Data from 103 studies (3190 subjects) indicate that the Beck Depression Inventory and, to a lesser degree, the Hospital Anxiety and Depression Scale are influenced by the time since symptom onset, strongly related to physical impairment. Our results suggest that widely used depression scales overestimate depression due to confounding with physical symptoms.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disorder characterized by progressive loss of upper and lower motor neurons, leading to increasing weakness, spasticity, paralysis, and death, usually by respiratory insufficiency. Even with the current best medications, patients experience a median survival of 2–3 years (Kiernan et al., 2011). The incidence of ALS is reported to be between 1.5 and 2.7 per 100,000 population/year (average 1.89 per 100,000/year) in Europe and North America (Worms, 2001).
The diagnosis of ALS has a significant impact on the quality of life of both patients and their families (Gibbons et al., 2013; Pagnini, 2013). The disorder can invoke a wide range of psychological reactions including anxiety, stress, and hopelessness (Averill et al., 2007; McLeod and Clarke, 2007). Moreover, the burden experienced by ALS caregivers is often severe and they are at risk of developing depressive and anxiety reactions (Pagnini et al., 2010).
Given the severe and the irreversible nature of the disease, high levels of depression may be expected in people living with ALS (Rabkin et al., 2000). However, there is still uncertainty about the prevalence of depressive disorders (Wicks et al., 2007). Rates of reported depression in patients with ALS, based on assessment using questionnaire screening instruments such as the Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, 1983) or the Beck Depression Inventory (BDI; Beck et al., 1988), vary greatly, with some prospective studies reporting as many as 45 percent of patients depressed and some as low as 8 percent. Estimates of depression using structured clinical interviews for depression or disease-validated questionnaire measures tend to vary less, generally indicating case-level depression in 7–11 percent of patients with ALS. Despite the daunting clinical picture of the disease, rates of depression appear to be paradoxically low. Some commentators refer to the phenomenon of good psychological health in the face of incurable terminal illness as the well-being paradox (Grehl et al., 2011). A number of studies have shown that quality of life in the disease is statistically unrelated to functional ability, which will necessarily decrease as the condition progresses (Gibbons et al., 2013; Goldstein et al., 2002; Robbins et al., 2001; Simmons et al., 2000).
The diagnosis of depressive disorder in people with ALS is difficult because the Diagnostic and Statistical Manual of Mental Disorders (4th edn; DSM-IV; American Psychiatric Association (APA), 1994) classification of depressive symptoms includes both psychological and somatic aspects (Kurt et al., 2007), including fatigue or loss of energy, loss of appetite, psychomotor retardation, insomnia, or hypersomnia. All of these symptoms can occur as a direct consequence of motor neuron disease, independent of depression (Pagnini, 2013). Labeling the person with ALS as depressed, by making a diagnosis, has a potentially severe impact on his or her quality of life, with differences in the clinical care (Gibbons and Young, 2012; Kurt et al., 2007). Moreover, there are findings that suggest a strong relationship between role of psychological factors and outcome in ALS (McDonald et al., 1994).
There is some evidence suggesting that the wide variation in reported estimates of depression is due to measurement error caused by confounding with physical symptoms of illness that may be unrelated to depression (Gibbons et al., 2011). Patient-reported depression questionnaires that rely heavily on measuring the physical components of depression may overestimate psychological suffering. The BDI (Beck et al., 1996), in all its versions, is one of the most widely used instrument for the assessment of depression and contains different questions about physical issues that contribute to the depression scores, whereas the HADS (Zigmond and Snaith, 1983) has been developed for the assessment of hospitalized patients and ostensibly avoids evaluation of somatic symptomology related to anxiety and depression.
Many papers have previously analyzed depressive issues in ALS, but no meta-analytic synthesis has ever been conducted. Meta-analysis allows measurement error and small-sample bias to be minimized by collecting data from a wide range of international studies.
We aim to compare different depression screening instruments, with a particular emphasis on the BDI and the HADS, and their course during the illness progression using meta-regression. With the analysis of these two instruments, we aim to investigate the hypothesis that depression will increase as disease course carries on. We hypothesize that the HADS-Depression (HADS-D) measure is less influenced by prevalence of physical impairment than the BDI, which includes more somatic symptoms of depression. This study represents the first attempt to test these hypotheses using meta-analysis on a large international sample of patients with ALS.
Methods
The scientific literature was screened, to search for papers that included an assessment of depressive features in people with ALS. In order for the paper to be included in the analysis, the assessment of depressive features should have been conducted with a standardized questionnaire instrument or with a diagnostic interview. Many papers do not report indicators of physical functions, such as the ALS Functional Rating Scale (ALSFRS), or present a certain heterogeneity of measures (e.g. ALSFRS or ALSFRS-R). However, many papers do report time since diagnosis, which is strongly related to functional status, with strong correlation with the ALSFRS (Kollewe et al., 2008). Given the strong relationship between functional ability and time since diagnosis, and the increased quality and availability of the latter, time since diagnosis was selected for use in the study as a proxy measure for physical impairment.
The following databases were considered, without time limits: PubMed (MEDLINE), PsycINFO, the Cochrane Central Register of Controlled Trials, CINAHL, Scopus, and ISI Web of Science. The searches included the following terms: (“Amyotrophic Lateral Sclerosis” AND/OR “Motor Neuron Disease”) AND (“Depress*” AND/OR “Quality of Life” AND/OR “Mood” AND/OR “Psych*”). These words were searched as key words, title, abstract, and Medical Subject Heading (MeSH) subject heading terms. Additionally, citation maps were examined and the “cited by” search tools were used. These findings were cross-referenced with additional references from reviews. Unpublished works were not considered.
Two reviewers screened the abstracts of all publications obtained by the search strategy. Whenever papers were not included in the available academic databank or whenever data were not reported or missing, authors were approached to provide missing data. For all selected papers, the full articles were obtained and inspected to assess their relevance. Data were independently extracted by the two reviewers (F.P. and G.M.M.) using a pre-designed data collection form: number of subjects, geographic origin of the study, mean age and sex information (percentage female), months since symptoms onset, assessment measure used, mean scores, and standard deviations (SDs). Any disagreements were discussed with a third reviewer (C.J.G.).
Statistical analysis
Three random-effects models, one for each considered instrument (BDI, Beck Depression Inventory-II (BDI-II), and HADS), were used to estimate the overall (mean) depression scores. The three between-studies variances that are used to assign weight under the random-effects model were estimated by the Unrestricted Maximum Likelihood approach, which does not make any assumptions about the distribution of the true depression means (Borenstein et al., 2011). All analyses were performed using the Comprehensive Meta-Analysis software version 2 (version 2.2.064 released on 27 July 2011) (Borenstein et al., 2005).
The first random-effects analysis involved an unconditional (intercept-only) model. Homogeneity was tested with the Q-statistic and indexed as a percentage of variance with the I-squared statistic (Borenstein et al., 2011). Q follows a central chi-squared distribution with k − 1 degrees of freedom, where k is the number of studies aggregated, so a p value (considered threshold: p < .05) for any observed value of Q can be calculated. A Q value with a corresponding p value that is less than the critical alpha results in the rejection of the null hypothesis of homogeneity. I-squared is a percentage index of heterogeneity and reflects the proportion of between-studies variability that is due to true differences among the studies.
A conditional meta-regression model was then examined in order to assess the relationship between the study-level predictor variable, that is, time since onset of symptoms, and mean depression scores. Statistical significance of the slope was assessed with the Z-test, while goodness of fit was tested with the Q-statistic on residuals and indexed as a ratio with a random-effects analogous R2 (Borenstein et al., 2011).
Results
The search strategy generated 680 citations, of which 110 papers reported depression scores from psychometric questionnaires. Among these, data from 103 studies were included. Studies and their results are reported in Table 1. The overall number of subjects with ALS included in the studies is 3190, with a mean age of 59 years and an average length of the illness of 24 months.
List of analyzed papers (in alphabetic order referred to the first author).

HADS: Hospital Anxiety and Depression Scale; QIDS-SR-16: Quick Inventory of Depressive Symptomatology (16 items) (Self-Report); HDRS: Hamilton Depression Rating Scale; ZDS: Zung Depression Scale; BDI: Beck Depression Inventory; ADI: ALS Depression Inventory; MADRS: Montgomery–Asberg Depression Rating Scale; BSI: Brief Symptom Inventory; DIS: Diagnostic Interview Schedule; D-S: Depressivitats-Skala; EQ-5D: EuroQoL 5 Dimensions; GDS: Geriatric Depression Scale; DASS: Depression, Anxiety, and Stress Scale; CES-D: Center for Epidemiological Studies Depression Scale; MDI: Major Depression Inventory; PHQ: Patient Health Questionnaire; POMS: Profile of Mood States; BHS: Beck Hopelessness Scale; PEG: percutaneous endoscopic gastrostomy.
The most widely used instruments to assess depression were the HADS (42 studies) and the two versions of the BDI (BDI-I, 35 studies; BDI-II, 9 studies). The ALS Depression Inventory, an ALS-specific questionnaire for depression, has been used in five works. Many other instruments have been reported by a small number of papers (see Table 2).
Assessment instruments used.
ALS: amyotrophic lateral sclerosis.
Some studies have used more than one instrument.
The weighted mean value obtained with the HADS-D was 4.59, with a SD of 3.16. The BDI-I has an average score of 11.37, with an SD of 7.39, while the weighted mean score of the BDI-II was 12.97, with an SD of 7.15.
Unconditional models
The overall (mean) scores that resulted from the unconditional random model analyses were 11.926 for BDI (k = 27, 95% confidence interval (CI) = 10.272, 13.581), 13.054 for BDI-II (k = 8, 95% CI = 10.849, 15.26), and 4.152 for the HADS-D score (k = 37, 95% CI = 3.521, 4.783). Homogeneity of mean scores was firmly rejected for each measure (Q = 843.231, p < .0001, I-squared = 96.917%; Q = 46.999, p < .0001, I-squared = 85.106%; Q = 536.569, p < .0001, I-squared = 93.291% for BDI, BDI-II, and HADS, respectively), indicating substantial true variations in mean depression scores across studies within the three subgroups. Meta-regression random models were then fit in an attempt to explain some of the variability.
Conditional models
Study-level mean BDI and HADS scores were separately meta-regressed on study-level mean times since onset of ALS symptoms in order to test the significance of the slopes and assess the goodness of fit of the two conditional random models. Study-level mean BDI-II scores were not regressed due to the small number of studies (n = 9) that used that measure.
Z-test on slopes showed that the predictor, that is, study-level mean time since onset of ALS symptoms, was statistically significant within studies that used the BDI (k = 20, β = .132, p = .0098, 95% CI = 0.032, 0.232), but not within studies that used the HADS (k = 27, β = .026, p = .455, 95% CI = −0.043, 0.096). Unsurprisingly, residual variances of both models were not significantly different from zero (Q-residual(19) = 19.51, p = .42 and Q-residual(26) = 31.61, p = .2 for BDI and HADS, respectively). Given that the Q-statistic and its p values are sensitive both to the number of studies and to the within-study variance, non-significant results should not be taken as evidence of no between-study variation when studies are few and the within-study variances are large (Borenstein et al., 2011). Analogous R2 was thus calculated to quantify the amount of explained variabilities and showed a different picture. Study-level time since onset of ALS symptoms was able to explain 58 percent of the variance across studies that used the BDI (Figure 1), while 19 percent of between-study variance was explained for studies that used the HADS (Figure 2).
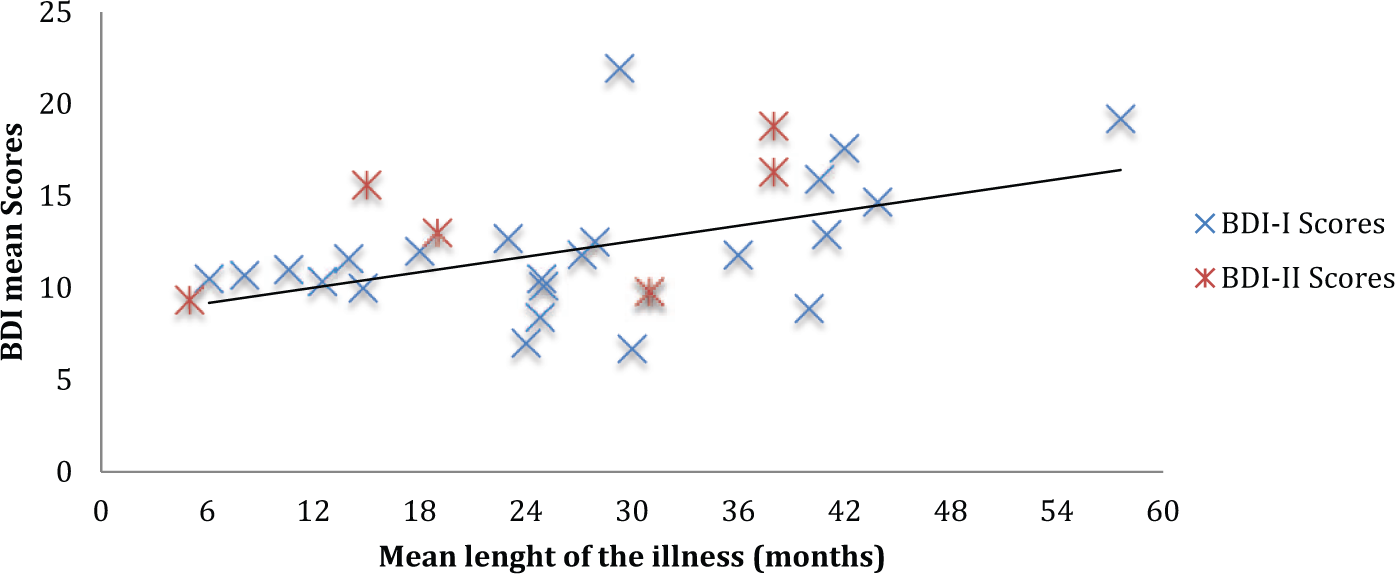
BDI mean scores and length of the illness.
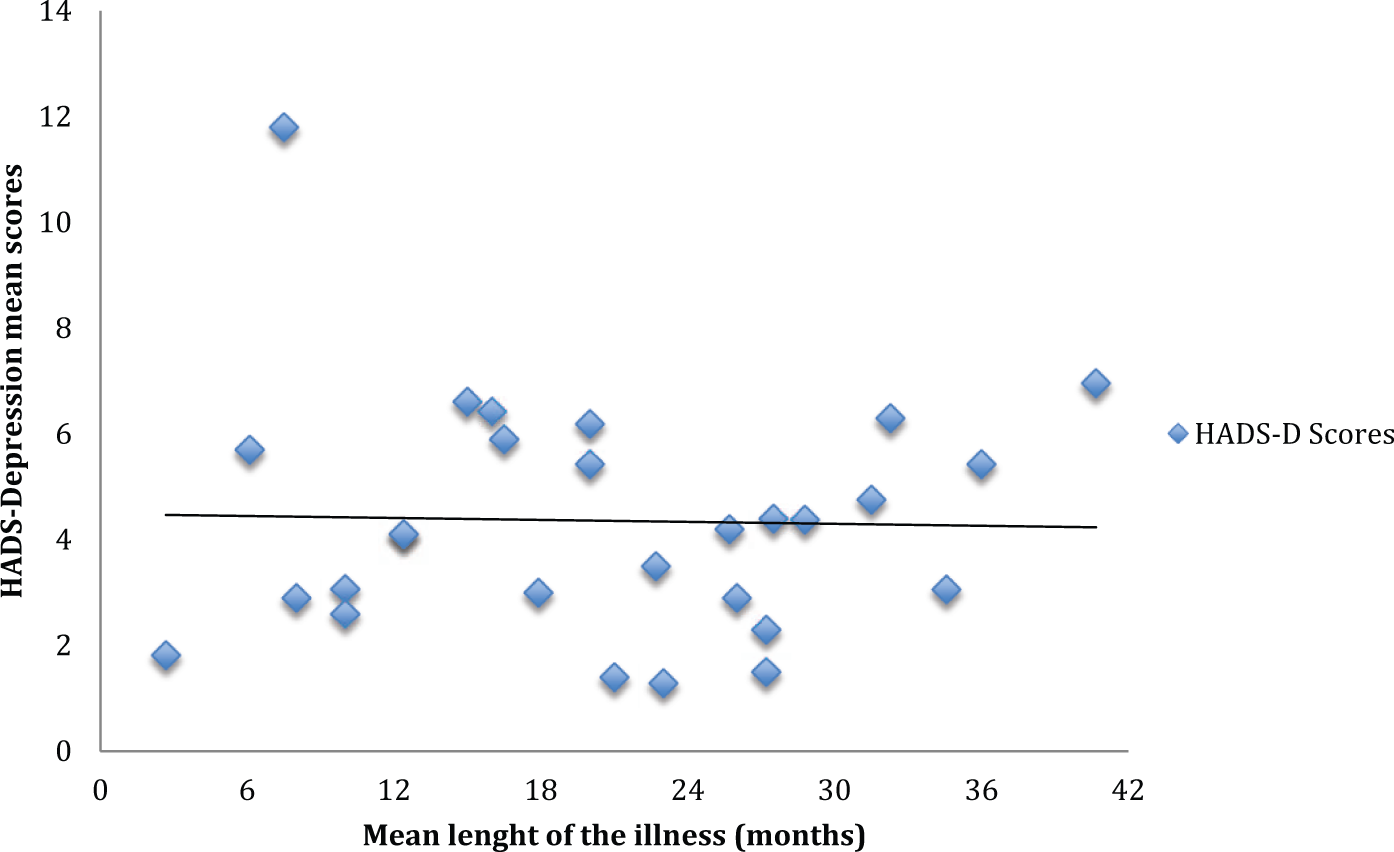
HADS-D mean scores and length of the illness.
Discussion
We have employed a meta-analytic approach to evaluate the confounding effect of time since symptom onset on the accuracy of depression measurement for patients with ALS. Data were extracted from a large number of research papers, with a final sample exceeding 3000. Our results suggest support the hypothesis that symptoms of ALS do interfere with the estimation of depression severity using commonly used questionnaire measures of depression. This effect was much greater where measurements were made using the BDI and was still present in studies that employed the HADS, which aims to avoid assessment of somatic symptoms of depression.
Despite confounding with physical symptoms of illness, the average scores of both HADS and BDI do not indicate a strong presence of depressive disorders in the sample, in a general level. Our analysis indicates that the mean depressive score of the HADS is only slightly above the average without a significant difference compared to a non-clinical sample (the average HADS-D score for general population is 3.68 (Crawford et al., 2001)). Both BDI average scores (BDI and BDI-II) fall near the cut-off (13) for “mild depression” (Beck et al., 1996).
The meta-regression indicates that HADS scores are less influenced by the time since symptom onset, while a high percentage of the variance of the BDI and the BDI-II is related to the time since the beginning of the illness. ALS is a progressive generative disorder; therefore, the increasing physical disability tends to worsen through time (Kimura et al., 2006). Our results show that the BDI and the BDI-II are highly influenced (more than 50% of the variance) by level of physical impairment. These instruments wrongly increased depression scores with the progression of the disease. This consideration is coherent with previous studies (Goldstein et al., 2002; Robbins et al., 2001; Simmons et al., 2000) and suggestions (Pagnini et al., 2012a, 2012c).
A direct clinical implication of these results is that the diagnosis in a person with ALS cannot be done with the DSM-IV criteria tout court. This classification includes many physical elements, represented also in the BDI, that are very useful in the general population, but significantly increase the risk of false positives when employed to populations with significant physical impairment.
It is surprising, given the wording of items on the BDI that assess somatic symptomology, that the instrument is so widely used for disabling long-term and acute conditions. We suggest that questionnaire measures are always assessed for face validity, using rigorous psychometric methodologies, such as item response theory (e.g. the Rasch model; Rasch, 1960), prior to use in populations with significant functional impairment.
Measurement error can strongly influence study results and result in poor clinical decisions being taken to treat patients with the disease. Increased estimates of depression in functionally impaired populations may lead to an increase in false positive diagnoses, which can be traumatic to patients who are trying to adapt and cope with a terminal diagnosis. In addition, many depression medications may cause unwanted side-effects that can be particularly problematic for patients with ALS (e.g. loss of balance and dizziness) (Gibbons and Young, 2012).
In comparison to the BDI scores, HADS ones result less influenced by the time since symptoms onset, highly related to physical impairment level. The relationship between HADS-D scores and time passed is not significant, although there is a tendency (19% of the explainable variance) in this direction. Gibbons et al. (2011) investigated the measurement properties of the HADS-D using Rasch analysis and discovered that the HADS-D instrument overestimated the prevalence of case-level depression by 36 percent due, in part, to the inclusion of the item “I feel as though I am slowed down.” Data gathered in our study do not facilitate HADS-D scores with or without this item, precluding a meta-analytic investigation of this issue. However, similar considerations made about the BDI may suggest that the inclusion of a “somatic” item may prevent accurate assessment of depression for ALS patients. It seems advisable that new cut-off for the use of the HADS-D in ALS, without this item, would be provided. Moreover, disease-specific measures for ALS do exist (i.e. Hammer et al., 2008) and may increase measurement accuracy (Gibbons and Young, 2012) and be a valuable support during a clinical interview. Interestingly, these instruments do not appear to be widely used in research studies, as we found only few works that used them. That may be related, in our view, to a lack of knowledge of their existence, to a lack of familiarity from a clinical perspective or to the perception that relying on newer disease-specific measures may preclude important comparisons with previous research studies that relied on older generic measures of depression. Qualitative and projective assessments (i.e. Rorschach ink test, Thematic Apperception Test (TAT)) may be useful tools to assess depressive features in ALS (Palmieri et al., 2010b) and such approaches merit further exploration.
As recently suggested (Gibbons and Young, 2012), considering the limits of the assessment questionnaires that are readily available, our results suggest that clinicians should refer to a clinical interview, in any case there is the suspicion of a depressive disorder.
Physical impairment in ALS is often significant, and self-reported health status is much worse in the disease when compared to other long-term conditions, including chronic pain (McGuire et al., 1996). That is not to say that functional impairment will always impede accurate measurement and diagnosis using self-reported questionnaire depression screens. Research is warranted to explore the extent to which variance in depression scores is explained by severity of illness in other functionally impairing conditions. Moreover, we were not able to consider the role of the cognitive impairment on the development of depression and on its influence on the diagnostic process. Further studies should take this element under consideration, both as a possible predictor of depressive symptoms and potential bias in the assessment process.
Our study is limited insofar as we had to rely on a proxy measure of physical ability, given the heterogeneous methods and inconsistent reporting of direct functional status data in the papers that were included in the study. Despite this shortfall, time since symptom onset correlates very strongly with functional impairment, and may be seen as a good proxy measure in lieu of high-quality functional status information (Kollewe et al., 2008).
As indicated by our results, the estimation of depression prevalence among ALS patients remains problematic. The lack of valid generic measures for this population precludes a direct comparison between ALS patients and those in the general population, or with other disabling conditions. On the other hand, the development of specific instruments or the adaptation of the existing ones requires the definition of ranges or cut-off, a process which must be conducted carefully if accurate estimates are to be gained in the future. Given that criteria provided by DSM-IV are difficult to apply successfully to this population, it appears critical that clinicians and researchers in the ALS field would provide a modification of these criteria, helping to unveil the real extent of depressive disorders in ALS.
In case clinicians or researchers still intend to refer to the BDI or to the HADS for depression assessment, they should be aware that these two instruments tend to overestimate depression in ALS. These scores are highly influenced by the physical impairment of the patients, in particular, those from the BDI; therefore, they are not directly comparable to general norms. We refer to data presented in this study, for normative comparison: the average score from our data is 4.59 (SD: 3.16) for the HADS-D subscale and 11.37/12.97 for the BDI/BDI-II (SD: 7.39/7.15). The meta-analysis does not allow to infer the distribution of scores in the ALS population, which may be non-normally distributed. Further studies are required to better understand the presence of depressive issues, in the light of a confounding effect of physical impairment.
Conclusion
This study uses meta-regression to explore the negative effect of functional limitation on the accurate assessment of depression for patients with ALS. Support was found for our hypothesis that depression measurement in ALS is confounded by the presence of physical disease, creating an erroneous linear relationship between depression and disease duration for some measures, and not for others.
Footnotes
Funding
Dr. Pagnini acknowledges the Italian Ministry of Health and Regione Lombardia for the support received with the “Young Researcher” Grant No. GR-2009-1607388”.