
Abstract
Previous studies on autism have shown a lack of motor anticipation in children and adults with autism. As part of a programme of research into early detection of autism, we focussed on an everyday situation: spoon-feeding. We hypothesize that an anticipation deficit may be found very early on by observing whether the baby opens his or her mouth in anticipation of the spoon’s approach. The study is based on a retrospective analysis from family home movies. Observation of infants later diagnosed with autism or an autism spectrum disorder (ASD) (n = 13) and infants with typical development (n = 14) between 4 and 6 months old show that the autism/ASD group has an early anticipation deficit.
Introduction
According to the DSM-IV-TR criteria, autism appears within the first 3 years of life (American Psychiatric Association, 2004). Nevertheless, children are diagnosed at an average age of 5.7 years (SE 0.08 years) (Shattuck et al., 2009). Diagnosis is usually not obtained before the age of 76 months in Germany (Noterdaeme and Hutzelmeyer-Nickels, 2010) and 36 months in France (Chamak et al., 2011). For over two decades now, researchers have been working at identifying early signs of autism. The earlier the diagnosis, the earlier the care, and the better the prognosis (Corsello, 2005; Fenske et al., 1985; Harris and Handleman, 2000). Thus, there may be a relationship between early symptoms and later impairment. Early therapy, including support and advice to family members, could prevent autistic withdrawal and improve later development (Boyd et al., 2010; Makrygianni and Reed 2010; Rogers, 1998). Parents of autistic children most frequently worry about language and social relationships and report early medical problems and sleep or mealtime difficulties more often than parents of typical children (Chawarska et al., 2007).
Mealtime involves social interaction, requiring a child’s adaptation to another person. Indeed, this kind of structured interactive situation leads the infant to integrate social routines and to detect contingencies to choose the best response to an adult’s stimulation. Typically developing infants are sensitive to the repetition of an event (Watson and Ramey 1972) and are able modify their behaviour according to events’ relationships (Rose and Desrochers, 2008). Contingency detection allows the infant to anticipate behaviour or respond to someone else’s overtures. During mealtime, infants predict spoon approach and anticipate by opening their mouths because they have learned the contingency between spoon approach and feeding. It is usually described as infants’ motivation to control the environment. It would be informative to observe this specific situation in infants with autism.
Autism and anticipation
Kanner (1943) and Ornitz et al. (1977) wrote that very young children with autism had a delay or a lack of anticipatory behaviour. When adults attempt to hold a child with autism in their arms, the child does not anticipate by greeting them with open arms as typical children do (Kanner, 1943). Sauvage (1988) observed that these infants do not protect themselves by putting their arms in front of them when falling. Once again, they do not anticipate the consequences and adapt their behaviour. Several studies on anticipatory function (Martineau et al., 2004; Schmitz et al., 2003) have shown, in a bimanual load-lifting task, that infant with autism had major anticipation difficulties. Unlike typical children, they do not anticipate the unloading by stabilizing their posture.
Many explanations of this anticipation deficit have been proposed. The deficit may be the result of a motor disorder, such as dyspraxia. Children with autism know what to do but are not able to plan the sequence of actions or execute the movements (Damasio and Maurer, 1978; Rogers et al., 1996; Hughes 1996; Forti et al., 2011). They might also need more time to initiate the movement. Another reason may be that they need more time to understand what they have to do to learn social contingency. Several studies have shown social contingency deficits in children with autism from 6 to 36 months (Chin, 2009; Rozga, 2009). If they have difficulties in understanding social contingency, it may be because the development of active self-and-other awareness is impaired (Hobson and Lee 1999; Hobson 1990).
Another explanation is that the movements involved in social contingency are difficult for them to perceive. Indeed, slowing down movements can lead to better understanding of social environment (Gepner and Feron, 2009; Tardif et al., 2007).
Although the reasons behind anticipation difficulties remain unknown, anticipation and adaptation impairments are strongly evident in children with autism. The aim of this study is to show that these difficulties can be detected in the first months of life, especially during mealtime. To do this, we chose a retrospective methodology, analyzing family home movies.
Early signs and family home movies
In the 1970s, Massie (1977) first used family home movies to study interaction dysfunction in mother-infant dyads. Family home movies are important sources of information but cannot be used crude because of the extreme variability of what is recorded. Home movies are not made for research purposes but, rather, to record memories of the child’s early years. That is why researchers have to select specific and comparable situations before doing the analysis. However, the technique of using home movies as data allows the researcher to observe infants in their own environment without interfering. It also enables the researcher to watch the movie repeatedly and in slow motion, which ensures very detailed coding. Family home movies have shown very early motor, hypotonic and postural abnormalities in infants later diagnosed with autism (Adrien et al., 1993; Teitelbaum et al., 1998). The lack of anticipatory behaviours has also been observed as early as the first 6 months of life (Maestro et al., 2002, 2001).
To our knowledge, no study in the field of early sign detection has focused on feeding situations in the first 6 months of life. Given the anticipation problems children with autism experience later in life, we hypothesize that infants with autism would show less anticipatory mouth opening than typical infants when the parent approaches with the spoon.
Method
Population and family home movies collection
The research was approved by the appropriate research ethics committee. The first step of the study was to collect a large number of family movies. This was done simultaneously in two different sites: psychologists’ offices in France (French-speaking) and an institution for people with autism in Flanders (the Dutch-speaking part of Belgium). Parents received a letter explaining the purpose of the study and signed a consent form. They were then were asked to provide any videotapes they had recorded. Films were copied and the original was given back to the parents.
Videos from 94 children were collected: 48 children with autism or an autistic spectrum disorder (ASD) (autism n = 41; ASD n = 7) and 46 children with typical development (TD). Diagnoses were made by trained psychiatrists, paediatricians, or an experienced multidisciplinary team. Their mental age was evaluated by trained psychologists, using standardized instruments commonly used in France and Flanders. Because the videos were collected over the course of several years, a number of different instruments were used. Eight out of the 13 had a mental retardation (IQ < 75). The comparison group consisted of 14 children (eight boys and six girls) with typical development with no pervasive disorder, mental retardation or learning disabilities.
We selected feeding situations from these videos. Videos with bad quality or on which the baby was not easy to observe were rejected. For example, breastfeeding situations where the baby is often nestled against the mother were not selected. We chose to focus on spoon feeding situations because it is a new interactive situation for all the infants, and we are able to see how they integrate this social routine and how they adapt themselves to this new situation.
We also excluded videos in which children encountered spoon-feeding for the first time as well as sequences in which we were unable to see the adult holding the food out to the infant. Every time the adult approached the spoon close to the baby’s mouth was counted as an attempt. If we recorded only one attempt, the data were not included in the research.
Based on the above criteria, we kept only 31 videos among the 59 listed feeding situations (13 ASD infants: 15 videos; 14 TD infants: 16 videos). The movies were sorted into four age-brackets: infants at 3, 4, 5 and 6 months of age. In both the ASD and TD groups, only two infants had useful feeding situations in more than one age period. Table 1 shows the distribution of the participants in the different age ranges.
Distribution of the feeding videos

The 13 participants (all boys) in the ASD group had received formal diagnoses of autistic disorder (n = 8) or ASD 1 (n = 5) according to established criteria (DSM-IV-TR; American Psychiatric Association, 2004).
Design and procedures
Coding of infants’ anticipation behaviours was performed by psychologists and researchers experienced with infants. A very simple coding grid was created (Table 2). For each attempt, the coder indicates whether the infant opens the mouth when the parent approaches the spoon.
Coding grid example

The judgment criteria were the following: tick yes when the infant opened his or her mouth before the spoon touched it. Attempts were defined as each time the parent held the spoon out to the infant’s mouth with the aim of feeding them. Sequences in which the adult tried to salvage the food that the infant spat out were not counted. We also did not count times when the parent tried to make the infant open their mouth by making them laugh. Moreover, occasions when the infant appeared not to see the spoon coming close because they were watching something else were excluded because of ambiguity. In addition, when the infant clearly refused the food, this could have been because they did not like it or because they were no longer hungry, and not because of a lack of anticipation. Therefore we also did not count these as attempts. Finally, cases in which the baby’s mouth was not visible were excluded.
Results
The two coders were blind to diagnoses. The first coder analysed all 31 movies. A second coder coded 50% of the videos to calculate the coder agreement. The inter-coder reliability was excellent (kappa = .79; Cohen, 1960).
For each infant, we obtained a percent of success of mouth-opening anticipation, corresponding to the ratio of correct anticipations to attempts (Table 3). The Student t-test for independent measures were performed to compare anticipation success in TD and ASD groups (data normalized by taking the arcsine of the square root). Means by age bracket were then calculated to see the global evolution (Table 4). Given the small number of participants in each age group, we report only descriptive statistics on these results.
Individual scores of anticipation
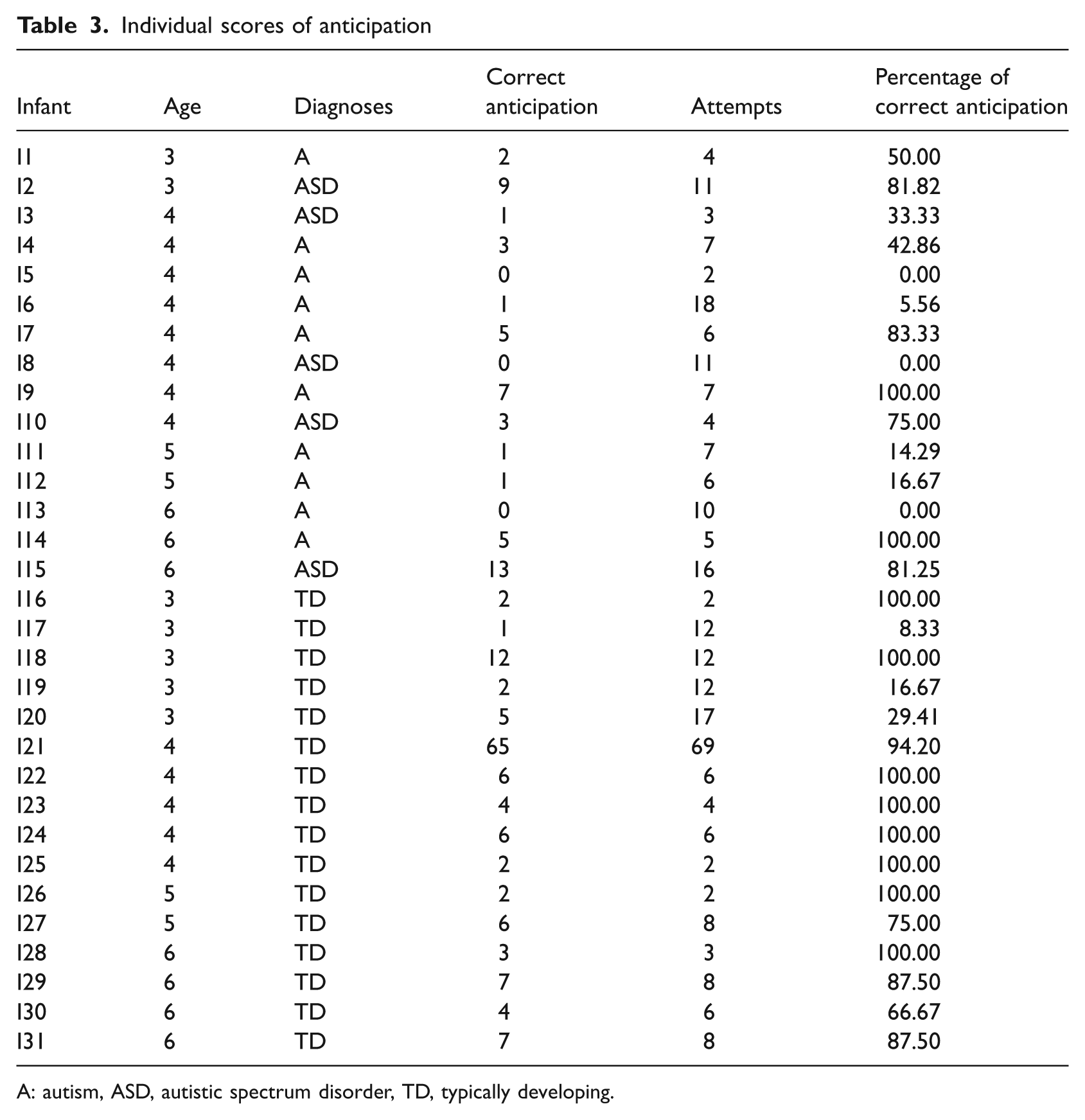
A: autism, ASD, autistic spectrum disorder, TD, typically developing.
Percentage success of mouth opening by group and age bracket

There is no difference between the two groups concerning the number of attempts and the age. The difference between ASD and TD infants is significant (t(29) = −2.86; p = 0.008).
Focusing on development, results reveal that TD infants who at first had had difficulties with anticipation quickly learned to anticipate. This was not the case for the ASD infants.
Because of the variability between infants, it is more appropriate to reason about individuals rather than about groups. Infants from both diagnostic groups were sorted according to whether or not they anticipated more than 50% of the feeding attempts (Table 5).
Distribution of infants from 3 to 6 months whose scores are more than or less than 50% of correct anticipation
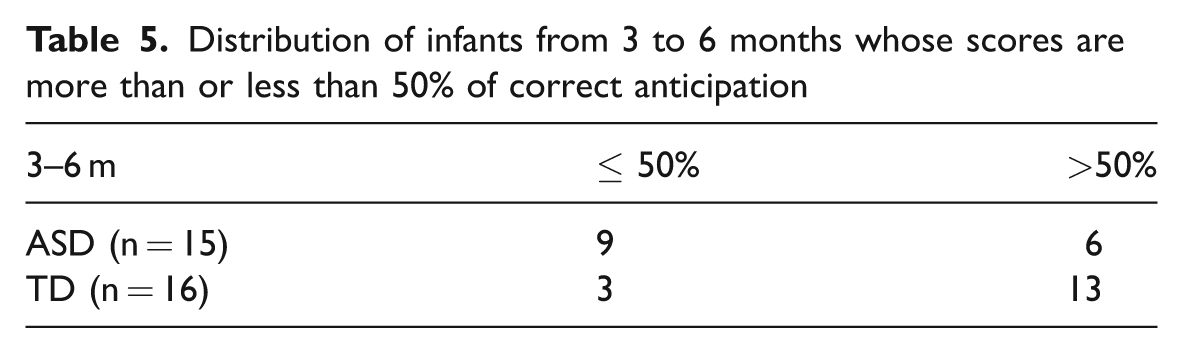
A non-parametric inferential test was computed (χ2 with the Yates correction for small samples). The anticipation success significantly depends on group (χ2(1) = 3.95; p = 0.047): there are fewer infants that succeed in anticipating in the ASD group than in the TD group.
If we only examine the 4–6 months age bracket (the mean age of the weaning period), the criterion of 50% success is even more discriminative (χ2(1) = 7.57; p < .01) (Figure 1).
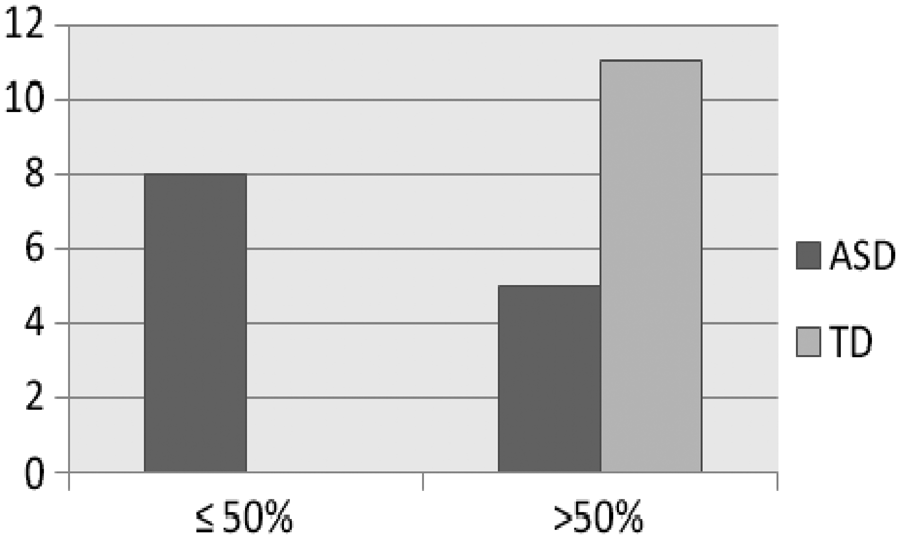
Distribution of infants of 4–6 months whose scores are more than or less than 50% of correct anticipation.
Discussion
The aim of this study was to examine anticipation disorders in 3- to 6-month-old infants with autism during mealtimes. Results showed that, despite variability between participants, infants with ASD have a deficit in mouth-opening anticipation in feeding situations. These difficulties can be observed in the very first months of life and ASD children improve gradually but not as fast as TD infants.
Surprisingly, ASD infants performed relatively well at 3 months and have lower scores at 4 and 5 months, going from 65.91 to 15.48. We must be very careful when interpreting these data because of the small number of participants in each group, especially at 3 months, for which only two infants are included. This evolution could be seen as a regression, but it needs to be replicated.
The criterion of 50% of good anticipation seems to be appropriate to distinguish between ASD and TD infants, especially from 4 to 6 months. This particularity could be easily observed by parents, and paediatricians could ask parents to pay attention to this anticipation skill during the mealtimes without necessarily worrying them.
Of course, before this becomes a useful sign of autism, this study must be replicated so that the results can be confirmed on a larger sample. Other studies should control the chronology of the spoon feeding and ensure that they know for each infant whether they are examining the second, the tenth or the 19th mealtime with spoon feeding, which could be a better way of observing the evolution of this skill over time. It could also be interesting to compare an ASD group with another group of infants with mental retardation or motor disorders. In the present study, the two infants with mental retardation we observed behaved the same as the control group, but this is a very small sample.
Page and Boucher (1998) showed that 79% of their autism sample had oro-motor dyspraxia, versus 55% for manual dyspraxia. People with autism have specific oro-motor problems (Adams, 1998). However, we can rule out the motor explanatory hypothesis for the present study because, when we observed ASD infants during bottle feeding situations, they had less difficulty anticipating when the bottle was coming to them.
A possible explanation for our data is that ASD infants do not anticipate because they do not understand the contingency. We observed that ASD infants do not learn as the mealtime goes on.
Moreover, as the situation was repeated several times during the first months of life, TD infants can learn how to react when they see the ‘stimulus spoon’. Infants with ASD need more time to learn and maybe to better understand goal-directed behaviour (Hamilton, 2009). This hypothesis can be tested by observing over a longer period. Our own observations tend to confirm this assumption. Indeed, when we observed infants with ASD within the same age bracket during bottle feeding, a skill with which they have much more experience, we noticed that they could learn to exhibit the correct anticipation behaviour.
We could also interpret these data as an expression of resistance to change or lack of flexibility. These characteristics of autism might be present very early. When feeding changes from bottle to spoon, infants with ASD, who have some difficulties in modifying their behaviour, may need a longer developmental time to do it.
Conclusion
Infants with ASD showed significantly less anticipatory mouth opening in response to the approaching spoon. The 4–6 months age bracket seems to be a sensitive period in which to detect this anticipatory deficit in infants with ASD. This sign is easy to investigate and could be, after careful replication by several studies, one of the early red flags in ASD detection. An interesting study could be performed with siblings. Researchers could ask parents who have an infant at high risk for autism to film the infant during the spoon-feeding mealtime every month from weaning to the first year of age. Through this, the researchers would be able to observe the infants’ anticipation skills as well as the development of these skills.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.