
Abstract
The diagnosis of autism is often delayed, which translates into a missed opportunity to provide treatment during a critical developmental period. This study reviews studies that assessed factors associated with age at autism spectrum disorder diagnosis and provides recommendations on future research, programs, and policies to improve early detection. A search for all peer-reviewed articles containing the words autism, age, and diagnosis in either the title or abstract was performed. A total of 42 studies published from January 1990 through March 2012 were identified. Mean age at diagnosis for all autism spectrum disorders ranged from 38 to 120 months and has decreased over time. Factors associated with earlier diagnosis included greater symptom severity, high socioeconomic status, and greater parental concern about initial symptoms. Family interactions with the health and education systems prior to diagnosis also influenced age at diagnosis. Geographic variation in age at autism spectrum disorder diagnosis was identified in a number of studies, suggesting that community resources and state policies play a role in early identification. Early detection efforts should include enhanced parental and provider education on the early recognition of developmental problems, interventions aimed at streamlining the process from first concern to eventual diagnosis, and strategies that target underserved populations.
Introduction
Autism spectrum disorders (ASDs), including autistic disorder, Asperger’s disorder, and pervasive developmental disorder–not otherwise specified (PDD-NOS), are chronic conditions that first appear in childhood and are characterized by impairments in communication and social interaction and the presence of stereotyped or repetitive behaviors (American Psychiatric Association, 2000). Studies have demonstrated that intensive, early intervention programs can improve cognitive and language abilities and adaptive behavior in children with ASDs (Dawson et al., 2010; Rogers and Vismara, 2008; Vismara and Rogers, 2010).
Research supports that autistic disorder can be reliably diagnosed as early as 24 months of age (Johnson et al., 2007); however, many studies have found that a significant proportion of children are not diagnosed until school age (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2000 Principal Investigators and Centers for Disease Control and Prevention, 2007; Autism and Developmental Disabilities Monitoring Network Surveillance Year 2002 Principal Investigators and Centers for Disease Control and Prevention, 2007; Autism and Developmental Disabilities Monitoring Network Surveillance Year 2006 Principal Investigators and Centers for Disease Control and Prevention (CDC), 2009; Mandell et al., 2005; Shattuck et al., 2009). These studies have examined associations between age at diagnosis and several child-, family-, and community-level characteristics. Many factors associated with delayed diagnosis are modifiable or can be targeted for intervention with the ultimate goal of earlier detection. Indeed, one major goal established by the Interagency Autism Coordinating Committee’s (IACC) 2010 Strategic Plan for Autism Research is to identify children at risk for ASDs before behavioral symptoms manifest (IACC, 2010). To assist in this process, we provide here an examination of research to date that has assessed disparities in age at diagnosis and associated factors. In this study, disparities are defined as differences in age at ASD diagnosis by population characteristics, such as gender, race and ethnicity, and socioeconomic status. We apply an ecological approach by taking into consideration child, family, and community factors. The objectives of this study are to review studies that have assessed age at ASD diagnosis and associated factors in the last two decades and to provide recommendations on areas to target for future initiatives aimed at early detection.
Methods
A search for all peer-reviewed articles containing the words autism, age, and diagnosis in either the title or abstract was performed in PubMed. The search was limited to studies published in English from January 1990 through October 2010. An additional search was performed for articles published online between October 2010 and March 2012. A final search for studies containing the aforementioned keywords in the title only was performed using Google Scholar. In addition, references from all relevant articles were reviewed for studies that may have been missed during the initial search, especially since the original keyword search used “autism” only, and a number of studies, including “Asperger’s” and “PDD-NOS” could have been missed.
A study was included in this review if it (1) estimated age at diagnosis for any ASD and (2) examined the association between age at ASD diagnosis and at least one factor. The initial PubMed search yielded 388 studies, 23 of which met inclusion criteria for this review. An additional eight studies were identified through a search for recently published, online-only articles; four additional studies were identified through a review of references from relevant articles; and four more were identified in Google scholar (including two dissertations). An additional three studies did not meet the first inclusion criterion but nonetheless examined factors associated with early versus later detection and were therefore included in this review: one compared children in late versus early diagnosis groups (Twyman et al., 2009), the second compared a group of children diagnosed between ages 3 and 4 years with another group diagnosed between 5 and 6 years (Fernell and Gillberg, 2010), and the third reported the proportions of children falling into specific age at diagnosis categories (Levy et al., 2010). Altogether, findings from 42 studies are summarized in this review. Estimates of age at ASD diagnosis and the extent to which child-, family-, and community-level characteristics were associated with age at diagnosis were extracted from each study. Wherever possible, findings on the adjusted association (i.e. those that controlled for other factors) between the predictor and age at diagnosis are reported here.
Results
Study characteristics
Characteristics of included studies are provided in Table 1 and presented and labeled numerically in order of publication date. In the interest of space, included studies are subsequently referenced in brackets, in the text, using the numeric labels from Table 1. Of the 42 studies, 19 were conducted in or published using data from the United States, 9 in the United Kingdom, 6 from other European countries, 3 in Canada, 2 in India, 1 in Taiwan, and 1 in Australia. One study included data from five different countries. All except 5 studies were published in the last 10 years.
Characteristics of included studies (n = 42).
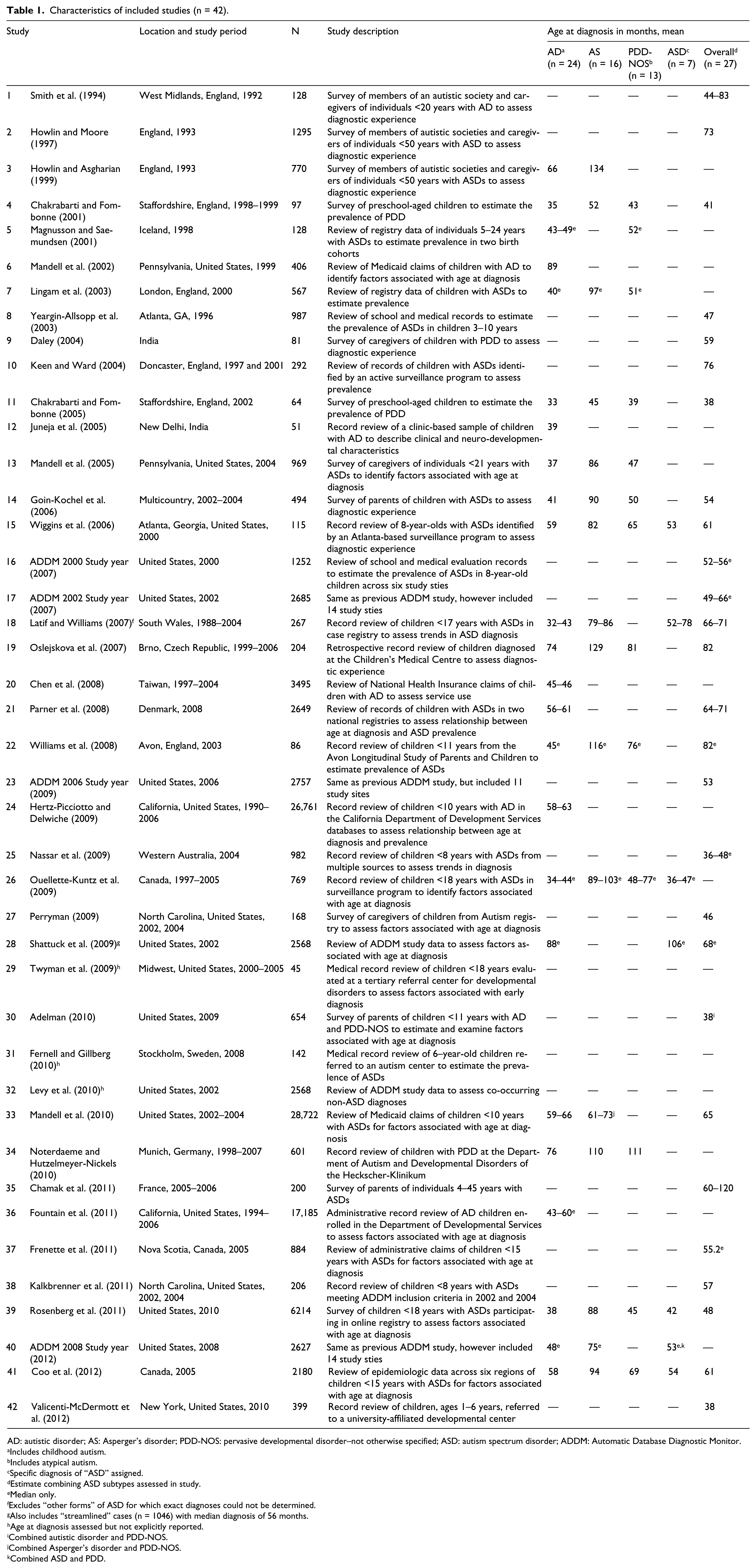
AD: autistic disorder; AS: Asperger’s disorder; PDD-NOS: pervasive developmental disorder–not otherwise specified; ASD: autism spectrum disorder; ADDM: Automatic Database Diagnostic Monitor.
Includes childhood autism.
Includes atypical autism.
Specific diagnosis of “ASD” assigned.
Estimate combining ASD subtypes assessed in study.
Median only.
Excludes “other forms” of ASD for which exact diagnoses could not be determined.
Also includes “streamlined” cases (n = 1046) with median diagnosis of 56 months.
Age at diagnosis assessed but not explicitly reported.
Combined autistic disorder and PDD-NOS.
Combined Asperger’s disorder and PDD-NOS.
Combined ASD and PDD.
Age at diagnosis and differences across diagnostic subtypes
Each study’s estimated mean or median age at diagnosis for at least one ASD is presented in Table 1. Among studies reporting age at diagnosis for autistic disorder (n = 24), mean and median ages ranged from 32 [18] to 89 months [6] and 34 [26] to 88 months [28], respectively. Among studies reporting age at diagnosis for Asperger’s disorder (n = 16), mean and median ages ranged from 45 [11] to 134 months [3] and 89 [26] to 116 months [22], respectively. Among studies reporting age at diagnosis for PDD-NOS (n = 13), mean and median ages ranged from 40 [11] to 111 months [34] and from 48 to 77 months [26], respectively. Seven studies assessed the mean or median age at which a specific diagnosis of “ASD” (i.e. “ASD-NOS,” “general ASD,” etc.) was assigned; mean and median age at diagnosis estimates ranged from 42 [39] to 78 months [18] and from 36 [26] to 106 months [28], respectively. The “ASD-NOS” category was used in the Shattuck et al study. Among studies that reported combined estimates for all ASDs (n = 27), mean and median estimates ranged from 38 [11 and 42] to 120 months [35] and from 36 [25] to 82 months [22], respectively.
Differences in mean or median age at diagnosis across ASD subtypes were examined in nearly half of all studies (n = 19). All studies that assessed age at diagnosis for Asperger’s disorder found that it was diagnosed later than all other ASDs [3, 4, 11, 14, 15, 13, 18, 19, 22, 26, 31, 33, 34, 39, 40, and 41]. Similarly, all but one study [5] found that age at PDD-NOS or “ASD” diagnosis was made later than autistic disorder [4, 11, 14, 15, 18, 21, 22, 28, 31, 33, 34, 39, 40, and 41].
Factors associated with age at ASD diagnosis
A summary of study findings on specific factors associated with age at diagnosis is provided in Table 2. Findings were grouped loosely by the following categories: (1) clinical characteristics, (2) sociodemographic characteristics, (3) parental concern, (4) health-care and education systems interactions, (5) geographic region and associated characteristics, and (6) cohort and period effects.
Characteristics associated with age at autism spectrum disorder diagnosis. a

ADDM: Automatic Database Diagnostic Monitor.
Numbers in parentheses reference included studies described in Table 1.
Not included here are specific differences across geographic region identified in the following studies: ADDM Network 2002 Principal Investigators, 2007; ADDM Network 2006 Principal Investigators, 2009; and ADDM Network 2008 Principal Investigators, 2012; Frenette et al. (2011); Howlin and Moore (1997); Ouellette-Kuntz et al. (2009); and Shattuck et al. (2009).
Clinical characteristics
Several studies found that having more autism-specific symptoms was associated with earlier diagnosis [13, 15, 27, 36, and 42]. Two additional studies found that developmental regression was associated with earlier diagnosis, defined in one study as moderate to severe social or communication skill loss before the age of 3 years [39], and in the other as a period of typical development in the first 1–2 years of life followed by a loss of previously acquired skills [28]. Other health conditions, including hearing impairment [13] and co-occurring psychiatric and neurologic conditions [32 and 37], were linked to later age at diagnosis. One study found that children who received a non-ASD diagnosis prior to the ASD diagnosis were diagnosed later [30].
Findings regarding the association between cognitive impairment and age at ASD diagnosis were mixed: two studies found that intellectual disability, defined as mild to moderate or severe intellectual disability [34] or low IQ [28], was associated with earlier age at diagnosis, and one found comorbid intellectual disability to be associated with later age at diagnosis [39]. Four studies found no association between cognitive impairment and age at ASD diagnosis [13, 15, 36, and 37].
Sociodemographic characteristics
In all, 13 of the 17 studies that assessed the association between sex and age at ASD diagnosis found no association [6, 9, 13, 19, 22, 26, 33, 34, 29, 36, 37, 39, and 41]. Among the remaining studies, one found that females [15] and three found that males were diagnosed earlier [8, 14, and 28].
The majority of studies that examined the association between race or ethnicity and age at diagnosis were US-based studies. Five studies found no association between race and age at ASD diagnosis [13, 14, 15, 27, and 30]. Three studies found African-American children to be diagnosed later than White children [6, 39, and 42], one found non-Whites to be diagnosed later [36], and one found children of “other races” to be diagnosed later [28]. In contrast, one study found White children to be diagnosed later [33], and a Canadian study found children in the “visible minority” group to be diagnosed earlier [41]. Among the seven studies investigating the role of ethnicity, three found no association [13, 30, and 39], three found Hispanic children to be diagnosed later than White children [28, 36, and 42], and one study found the opposite association [33]. While not presented in Table 2, one study found that among children with intellectual disability, African-American race was associated with later age at ASD diagnosis compared with other racial/ethnic groups [15].
A total of 11 studies examined the association between measures of socioeconomic status (SES) and age at ASD diagnosis. Two studies found greater family or household income [14 and 13] and four found higher parental education [14, 28, 36, and 39] to be associated with earlier diagnosis. Six studies found no association between SES measures and age at diagnosis, including three studies using samples from outside of the United States [22, 27, 29, 30, 34, and 42].
With respect to other factors, a recent California study found that children of immigrant mothers and of mothers whose deliveries were paid for by Medicaid were diagnosed at later ages than other children [36], and another study linked child eligibility for Medicaid due to disability versus other eligibility types to ASD diagnosis at a later age [33]. While one study found no association between age at diagnosis and having other children with ASDs in the family [29], a second study found children in homes in which another child was already diagnosed with ASD to be diagnosed earlier [30]. In general, parental age was not associated with age at diagnosis [28, 29, 36, and 42]; however, one study found older maternal age was associated with younger age at ASD diagnosis [37]. Among the six studies that assessed the association between birth order and age at diagnosis, two found no association [29 and 42], one found firstborn children to be diagnosed earlier [12], and three found firstborn children to be diagnosed later [36, 37, and 39].
Parental concern
Parental attribution of the child’s condition to non-autism-specific behavioral difficulties [30] or behavioral problems (defined as being spoiled, stubborn/disobedient, requiring more discipline, or having a difficult personality) was associated with later age at diagnosis [27]. Children of parents who were first concerned with a potential medical problem (e.g. seizures) versus a developmental or autism-specific problem were also diagnosed later [9]. Conversely, concern about social skills development and atypical behavior [29] and having a higher level of worry about initial symptoms [27] were linked to earlier age at ASD diagnosis.
Systems interactions
Eight studies assessed the relationships between caregiver and child interactions with health and education systems prior to ASD diagnosis and age at diagnosis [9, 10, 13, 14, 15, 28, 29, and 30]. Three studies found that visiting a greater number of physicians [9 and 13] or professionals [14] prior to diagnosis was associated with later age at diagnosis. One study found that children who switched pediatricians in the first 5 years of life were diagnosed later [30]. A physician conducting developmental testing in response to concerns about the child’s development was not associated with age at diagnosis in one study [13] but was associated with earlier diagnosis in another [30].
Studies also found that children receiving specialty referrals [13], who were referred to early intervention [30], or who were referred from early intervention programs as opposed to physicians’ offices, schools, or parents were diagnosed at earlier ages [29]. One study found placement in educational settings designed to address learning difficulties versus mainstream school placement to be associated with later age at ASD diagnosis [10]. Children who received their initial ASD diagnosis at a nonschool setting (i.e. hospital, specialty center, etc.) were diagnosed at an earlier age than children diagnosed in school settings [15].
Geographic region and associated characteristics
Many studies examined differences in age at diagnosis by geographic region. An early UK study found significant differences in age at ASD diagnosis across nine regions [2]. In the United States, small differences in age at diagnosis (4-month range) across study sites were reported in the first Automatic Database Diagnostic Monitor (ADDM) Network Study in 2000 [16]. Age at diagnosis varied much more by study site in the subsequent ADDM study years [17, 23, and 40]. Differences in age at diagnosis across US Census regions have also been found [30 and 39]; for instance, Rosenberg and colleagues found that children living in the Northeast were diagnosed significantly earlier than children living in the other three US Census regions [39]. Finally, a recent study found significant differences across four regions in Canada in median age at diagnosis for PDD-NOS and ASD but not for autistic or Asperger’s disorder [26].
Among the six studies that assessed the relationship between urban/rural residency and age at diagnosis, three studies found living in a rural or nonmetropolitan area to be associated with later age at diagnosis [13, 20, and 39]. Two studies found no association [29 and 41], and the final study found that children from large urban or rural counties were diagnosed later than children from smaller urban or suburban areas [33].
Other community characteristics were examined in five studies, only one of which was located outside the United States [33, 36, 38, 39, and 41]. In one study, living in counties with more poor residents or in states with more stringent State Children’s Health Insurance Program eligibility criteria was associated with earlier age at diagnosis [33]. In another study, while living in areas with higher ASD prevalence rates was associated with earlier diagnosis, later diagnosis was linked to living in communities with higher educated populations, with higher median property values, and with a greater proportion of residents in poverty [36]. Both of the aforementioned studies found no relationship between the availability or concentration of child health professionals and age at diagnosis. Conversely, a recent study found that among residentially stable families, children living in areas with a greater number of neurologists or psychiatrists were diagnosed earlier [38]. The same study also found that children living in close proximity to a medical school were diagnosed earlier [38].
Cohort and period effects
Approximately half of all studies assessed the extent to which age at ASD diagnosis has changed over time; six of these studies were US based. All but one study [5] found that children from more recent birth cohorts were diagnosed significantly earlier than children from older birth cohorts [1, 2, 10, 11, 13, 14, 21, 24, 25, 30, 36, and 39]. Similarly, when year or period of diagnosis was examined, all but three studies [34, 39, and 41] found that children who were diagnosed more recently were diagnosed at significantly younger ages [7, 18, 26, 33, and 35].
Discussion
Forty-two studies published over the last 20 years have estimated and assessed factors associated with age at ASD diagnosis. They report mean and median ages ranging from 38 [11 and 42] to 120 months [35] and from 36 [25] to 82 months [22], respectively. Autistic disorder was diagnosed earliest followed by PDD-NOS and then Asperger’s disorder. Lack of delayed speech among children with Asperger’s disorder may explain much of the reason why the diagnosis occurs considerably later than a diagnosis of autistic disorder or PDD-NOS. Another consistent finding is that age at diagnosis is decreasing over time. This finding is encouraging as it suggests that more children are being identified early enough to confer the most benefit from intensive services.
Despite a trend toward earlier diagnosis, recent studies demonstrate that considerable disparities in age at diagnosis remain [13, 28, and 33]. In addition to highlighting differences in age at diagnosis by diagnostic subtype and time period, these studies have identified that disparities in age at diagnosis are associated with many child-, family-, and community-level characteristics. Factors consistently demonstrated to be associated with earlier age at diagnosis included greater symptom severity [13, 15, 27, and 29], higher socioeconomic status [14, 28, 33, 36, and 39], and greater parental concern [27 and 29]. In addition, many studies found that family interactions with the health and education systems prior to diagnosis played a considerable role in age at diagnosis.
Many of the observed differences may be attributable to discrepancies in study methods. For instance, findings from a number of studies were based on administrative data, such as Medicaid claims or health and education records, whereas other studies relied on primary data collection. Claims data, while offering access to a large and unselected sample, offer no measure of clinical presentation. There were also differences in sampling methods. Multiple studies relied on convenience samples from clinic-based studies or use of snowballing techniques, whereas others sampled from registry data. A likely additional contributor to observed differences across studies is that some limited the sample to children with a specific ASD diagnosis rather than including children with any ASDs, which may have influenced the distribution of associated characteristics such as symptom severity and comorbid conditions.
Conflicting findings with respect to the role of cognitive impairment, race/ethnicity, and birth order deserve further discussion. With respect to cognitive impairment, one study that found no association between cognitive impairment and age at ASD diagnosis only included children diagnosed with autistic disorder [36]. Studies that found an inverse association between cognitive impairment and age at diagnosis were based on children with greater symptom severity, which has also been linked to earlier diagnosis, and also may limit variability in IQ in the sample [28 and 34]. For one of the studies that found a positive association, it may be that because findings were based on a relatively older sample (which included children up to age 18); the ID diagnosis may have been made before increased awareness of ASDs or at a time when an ID resulted in the potential for more services and supports than an ASD diagnosis [39]. The conflicting race/ethnicity findings are more challenging to reconcile. The three studies that found that African-American children were diagnosed later than White children differed on a number of key factors from studies finding no association between race and age of diagnosis, such as study period, sampling procedure, sample, and location [6, 39, and 42]. Further examination of specific racial or ethnic disparities in age of first parental concern, referral processes, and age at diagnosis is needed. Of the studies examining birth order, four were based in the United States; the one study that found that firstborn children were diagnosed earlier was based in India [12]. Two studies examining this association had samples of approximately 50 subjects, which may not have provided the statistical power to identify an association [12 and 29]. The three studies that found that firstborn children were diagnosed later had larger samples (>800) and adjusted for a number of factors [36 and 39], which may lend support to the validity of the observed association.
It is also important to note that not all studies found an inverse association between greater community wealth and age at diagnosis. Studies that found that children living in lower-income areas were diagnosed earlier illustrates the complexity of the relationship between community-level measures of SES and age at diagnosis. The strength of this relationship diminished over time in one study [36] and was examined from 2001 through 2004 in another [33], which may indicate that the present-day influence of community poverty on age at diagnosis is not as strong relative to family-level SES.
Findings of these studies suggest that factors other than clinical presentation may be driving diagnosis, which warrants a more fine-grained analysis of factors that impede or expedite age at diagnosis. One framework to consider in evaluating these findings is that developed by Kilbourne and colleagues (2006) for advancing research on health disparities. The authors propose that research should start with the identification of disparities in health and health care, then follow with an attempt to understand factors that underlie such disparities, and finally, develop and implement interventions designed to reduce the disparities (Kilbourne et al., 2006). In developing interventions, particular attention should be paid to both factors most amenable to change and to subgroups of the population who are at the greatest risk of delayed diagnosis.
One potential area to target is parent education and awareness. Research has suggested that lack of awareness with respect to characteristic “red flags” of ASDs may explain why parents attribute children’s developmental issues to behavioral problems or other medical concerns [9, 27, and 29]. It is also possible that medical concerns may mask ASDs, which may lead a parent or clinician to focus attention elsewhere. Numerous studies have demonstrated that a significant lag exists between when parents first become concerned about their child’s development, to when treatment is first sought, to when the child ultimately receives an ASD diagnosis [15, 19, and 39]. Providers may benefit from greater training on how to respond to parental concerns, including advising parents to contact early intervention programs as soon as such concerns arise. Fortunately, over the past decade, a number of tools such as Autism A.L.A.R.M (American Academy of Pediatrics, 2010) and programs such as First Signs (First Signs, Inc., 2012) and the Centers for Disease Control’s “Learn the Signs. Act Early” campaign (Daniel et al., 2009) have been developed to educate parents and providers with the ultimate goal of reducing the age at which ASD is diagnosed. These programs should be evaluated to assess their effectiveness and, if demonstrated effective, scaled up to ensure that such programs are reaching the maximum numbers of families.
Findings from this review indicate a number of potential points of intervention as children and their caregivers interact with the health-care, education, and early intervention systems. For instance, several studies found that visiting or consulting a greater number of physicians or professionals prior to diagnosis was linked to later diagnosis of ASD [9, 13, and 14]. These and other studies have demonstrated that the pathway to ASD diagnosis is not always a straight one and that families experience a number of challenges along the way (Osborne and Reed, 2008; Siklos and Kerns, 2007). In these instances, clinicians may not feel adequately trained to assign a diagnosis, may be adopting a “wait and see approach,” or are not referring the child to professionals trained to evaluate children for ASDs. Conversely, children may lack a usual source of care, a medical home, or a trusting relationship with a primary care provider. Whatever the explanation, efforts to enhance provider knowledge around parental concern, screening, and appropriate and timely referral to both early intervention and evaluation services may reduce the number of professionals families see prior to ASD diagnosis, which has the potential to result in earlier age at diagnosis.
One study found that whether a physician conducted developmental testing had no influence on age at diagnosis but that physician referral to a specialist was linked to earlier diagnosis [13]. Another study demonstrated that children who were referred to a tertiary care center from an early intervention program as opposed to a physician’s office, school, or parents were diagnosed earlier [29]. Current guidelines on the assessment and treatment of children with ASDs recommend that children suspected of having an ASD be referred concurrently to early intervention and for comprehensive evaluation (Johnson et al., 2007). Findings from these studies underscore the importance of taking a multipronged approach that includes educating primary care providers on the early signs of autism and steps to take after parents express a concern as well as developing strong linkages between the health and early intervention systems.
Additionally, the fact that a number of studies highlighted delayed diagnosis among racial and ethnic minorities, families with low SES, and those living in under-resourced or rural areas suggests that efforts at lowering age at diagnosis should expressly target these particular groups. Indeed, studies from both developmental disabilities and child health research have tested and implemented a number of strategies to enhance early detection among underserved communities. For instance, the Assuring Better Child Health and Development (ABCD) Project is an initiative that works at the provider and state systems level to reduce disparities among underserved groups (Berry et al., 2008; Earls, 2009; Earls and Hay, 2006; Klein and McCarthy, 2009). Targeted to Medicaid-enrolled families, the overall goal of ABCD is to improve child developmental screening and referrals to early intervention, and findings from research conducted to date demonstrate increased provider screening for developmental delay and enhanced referrals and enrollment to early intervention programs among participating states (Earls, 2009; Klein and McCarthy, 2009).
One area yet unexamined is the role of regular pediatric care in the early identification of ASDs. Well-child care, especially in the preschool period, can provide the ideal context for early identification of chronic childhood conditions like autism. As well-child care is the primary means through which children receive developmental and preventive health care in the United States (Moyer and Butler, 2004), a logical next step is the examination of how regular well-child care affects age at ASD diagnosis. In addition, little is known about how parent–clinician interactions influence referrals and diagnosis. The content and nature of these interactions have been shown to influence satisfaction and outcomes with respect to child discipline (Wissow et al., 2008) and preventive care (Cooper et al., 2003; Roter and Hall, 2006) and to account for many racial and ethnic disparities in some forms of care. ASD researchers may benefit from adapting and testing models that have been developed for other populations to improve parent–provider communication in primary health care (Cooper et al., 2003; Roter and Hall, 2006; Wissow et al., 2008).
Finally, the regional variation in age at ASD diagnosis suggests that local policies and resources may influence age at ASD diagnosis. And yet, among the studies reviewed here, only four (all US based) attempted to identify factors at the community or state levels that may explain this variation [33, 36, 38, and 39]. Only one of these studies found an association between the availability of health professionals and age at diagnosis [38]. It may be that a focus on community resources is too narrow and that consideration of the interactions between resources and systems and policies is needed. Clearly, where children live is critical to understanding when they are first diagnosed; however, previous studies have failed to identify specific place characteristics that may explain regional variation in age at diagnosis. Finally, there is a need for further research on the role of national and regional policies, both within and across countries, in promoting the earlier identification of ASDs.
Footnotes
Funding
This work was supported by the National Institute of Mental Health grant F31MH091833.