
Abstract
A wait-list control experimental design was employed to investigate the effectiveness of a fundamental motor skill intervention at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with autism spectrum disorder (experimental n = 5, control n = 4); the impact of intervention intensity was also explored. The experimental group significantly improved their object manipulation and overall motor scores from pre- to post-intervention. The wait-list control design revealed no group-by-time interactions; however, with the groups combined time was a significant factor for all motor variables. There were no significant changes in adaptive behavior and social skills. These preliminary findings suggest that a fundamental motor skill intervention may benefit young children with autism spectrum disorder. Future research with larger samples is warranted.
Autism spectrum disorder (ASD) is a common developmental disability that occurs in approximately 1 in 68 children (Centers for Disease Control and Prevention, 2014). Children with ASD experience challenges with social communication and social interactions, and they exhibit a restricted pattern of behavior and interests (American Psychiatric Association, 2013). Given the significant challenges that children with ASD experience, early intervention is of the utmost importance. There are numerous intervention options for children with ASD; some are grounded in evidence, some are not; most interventions are expensive, and government-funded programs often have long wait times (Chasson et al., 2007; Eldevik et al., 2009; Lord et al., 2005; Matson and Smith, 2008). Therefore, it is important to create and implement evidence-based, cost-effective interventions for children with ASD that are beneficial to their overall development. One area that is often overlooked in the development of children with ASD is their fundamental motor skills (FMS). The primary focus of early intervention is traditionally on the core challenges in the social, communicative, and behavioral domains, not FMS.
FMS are the basic movement skills that are crucial for the future development of the more complex skills needed in games, dance, sports, gymnastics, active play, and recreational physical activities (Lubans et al., 2010; Payne and Isaacs, 2002). Research indicates that the motor skills of young children with ASD are significantly delayed and of poor quality (Landa and Garrett Mayer, 2006; Lane et al., 2012; Liu and Breslin, 2013; Lloyd et al., 2013; Matson et al., 2010; Ozonoff et al., 2008). For example, a large study measured the motor skills of 162 children with ASD between 12–36 months of age (Lloyd et al., 2013). Results indicated that the children’s gross and fine motor skills were significantly delayed for their age and became significantly more delayed with increasing chronological age even when non-verbal IQ was accounted for (Lloyd et al., 2013). Most of the studies of the motor skills of children with ASD focus on toddlers under the age of 3 years (Landa and Garrett Mayer, 2006; Lane et al., 2012; Lloyd et al., 2013; Matson et al., 2010) and school-age children (Pan et al., 2009; Staples and Reid, 2010), which leaves a significant gap in the literature concerning the motor skills of preschool-aged children with ASD. One of the few studies of motor development to include children in the 4- to 5-year-old age range directly measured the motor skills of 54 children aged 26–61 months with autism in comparison to 25 children with a developmental delay and 24 children with typical development (Ozonoff et al., 2008). Results indicated that the children with autism had significantly lower motor scores than the children with typical development; however, there were no significant differences between the children with autism and those with a developmental delay (Ozonoff et al., 2008). The significant motor delays that are experienced by young children with ASD justify the need to create early motor skill interventions in order to minimize motor delays and promote optimal overall development.
Motor skills have historically been ignored in psychology and developmental science (Rosenbaum, 2005); as such, they are often neglected in the early intervention literature for children with ASD. However, one study of the optimal outcomes for toddlers with ASD suggests that motor skill proficiency of children with ASD at the age of 2 years is one of the most predictive factors to have the best possible outcomes at 4 years of age (Sutera et al., 2007). Similarly, a recent study of 159 children aged 14–33 months with ASD demonstrated that fine and gross motor skills were a significant predictor of calibrated autism severity at that age, meaning that those children with better motor skills demonstrated fewer core symptoms of autism (MacDonald et al., 2014). Thus, motor skill interventions have the potential to improve the overall development of a child with ASD, not just their motor skills. A recent systematic review indicates that FMS interventions can be effective at improving FMS in preschool-aged children with developmental delays (Kirk and Rhodes, 2011). However, all the studies included in the systematic review excluded children with ASD and did not measure the impact of the intervention on adaptive behavior and social skills; thus, there is a critical gap in the literature pertaining to the effectiveness of FMS interventions for preschool-aged children with ASD.
Research has demonstrated that proficiency in FMS is positively associated with physical activity in children with typical development (Lubans et al., 2010); however, this relationship has not been established in children with ASD. In young children, physical activity is manifested in the form of active play (Burdette and Whitaker, 2005; Pellegrini and Smith, 1998). As movement is a primary element of active play, the motor delays that children with ASD experience may have negative consequences for play in this population; in other words, young children with ASD may not be physically able to engage in active play due in part to their poor motor skills (Gallo-Lopez and Rubin, 2012; Jobling and Virji-Babul, 2004). Play provides an opportunity for children to improve their executive functioning and problem-solving skills through the manipulation and use of objects and toys (Burdette and Whitaker, 2005; Gallo-Lopez and Rubin, 2012). Play is also essential for the development of joint attention, sharing, empathy, cooperation, and emotional regulation through the peer interactions that play can provide (Burdette and Whitaker, 2005; Gallo-Lopez and Rubin, 2012). Furthermore, functional play skills in early childhood are a significant predictor of language skills in adolescents with ASD (Sigman and McGovern, 2005). Thus, engagement in play is essential for the optimal development of any child; however, in order to engage in active play, one needs to be able to move effectively and efficiently throughout one’s environment (Pellegrini and Smith, 1998).
Children with ASD, by definition, experience significant delays in their social and communication skills (American Psychiatric Association, 2013), and they also have motor skills that are delayed and of poor quality (Liu and Breslin, 2013; Lloyd et al., 2013; Ozonoff et al., 2008). These skills are all required to engage in active play; yet, participation in active play also promotes the development of these skills. Therefore, developing proficient FMS may be even more important for children with ASD as it will provide them with an opportunity to engage in active play and reap the developmental benefits that play can provide.
The purpose of this study was to examine the effectiveness of an FMS intervention at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with ASD. A secondary objective was to determine whether an increased intensity of the motor skill intervention was more or less effective at improving the primary outcomes.
Method
Study design
Ethical approval was received from a University Research Ethics Board and a local Children’s Treatment Centre’s Research Committee and Quality Leadership Council; all parents provided informed consent prior to the onset of the study. This study employed a wait-list control experimental design which enabled the effectiveness of the intervention to be tested (children receiving the intervention in Group 1 while Group 2 acted as the control), as well as compare the effectiveness of two different intensities of the intervention (1 h/week for 12 weeks vs. 2 h/week for 6 weeks).
Regardless of group assignment, all children received the intervention for the exact same number of sessions and hours. Each group also attended three or four assessments, depending on group assignment, where motor skills, adaptive behavior, and social skills were assessed. Assessments 1 and 2 provided the pre- and post-assessment, respectively, of the experimental (Group 1) and control (Group 2) groups. Assessment 3 acted as the 6-week follow-up for Group 1 and the post-test for Group 2 following their intervention. Group 2 then attended a fourth assessment for their 6-week follow-up.
Sample
Inclusion criteria for the study required that participants have a diagnosis of ASD and be 4 years of age. Participants were recruited for this study through a mail out to the families (n = 65) of 4-year-old children with ASD who were on the waitlist for government-funded applied behavior analysis–based services for children and youth offered through the local Children’s Treatment Centre. In the province of Ontario, Canada, where this study took place, a written confirmation of ASD diagnosis must be provided by a family physician, pediatrician, psychiatrist, psychologist, or psychological associate in order for children to meet government eligibility requirements for these services; thus, all children targeted for recruitment had a confirmed diagnosis of ASD. Children were excluded from participating if their parents could not commit to bringing them to the assessments and intervention sessions. Only nine children were enrolled in the study by their parents and were randomly assigned to one of the two groups based on the order in which they enrolled (Group 1: n = 5; Group 2: n = 4). Group assignment was not concealed, and participants and the primary investigator were not blind to group assignment. Prior to enrollment in this study, five of the participants had received some form of motor intervention (i.e. physical therapy and/or occupational therapy) and eight of the participants had received other, non-motor, interventions (i.e. speech-language therapy, applied behavior analysis, etc.).
Procedures
All measurements were conducted in the researcher’s office with a parent or caregiver present. At the initial assessment, all parents completed a supplemental information form in order to provide demographic data and a brief developmental history of their child.
Anthropometric measurements
Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer (seca 222), and weight was measured to the nearest 0.1 kg using a digital scale (Tanita Digital HD351).
Motor proficiency
The Peabody Developmental Motor Scales-2 (PDMS-2) (Folio and Fewell, 2000) is a standardized motor skill assessment that is validated from birth to 6 years of age. The PDMS-2 was ideally suited for this study as it is normed down to infancy and therefore can more accurately capture the motor skills of children with ASD without a floor effect. The total motor quotient score provided by the results of the PDMS-2 was considered the primary outcome for this study and was administered at every assessment period. Internal-consistency reliabilities of the subtest and composite scores of the PDMS-2 ranged from 0.89 to 0.97, and the test–retest reliability coefficients ranged from 0.82 to 0.94 (Folio and Fewell, 2000).
The Movement Assessment Battery for Children-2 (MABC-2) (Henderson et al., 2007) was also used, but only at baseline (Assessment 1) in order to address the potential scope of motor impairment in these children at the onset of the study. The MABC-2 is a standardized motor skill assessment for children aged 3–16 years and is commonly used to identify children who experience significant delays in their motor development (Henderson et al., 2007). Internal-consistency reliabilities of the component and total test scores of the MABC-2 ranged from 0.73 to 0.84 (Henderson et al., 2007).
Adaptive behavior
Adaptive behavior is the degree to which an individual typically performs daily activities required for personal and social sufficiency; it is age-related, and for young children includes activities such as dressing and getting along with peers (Sparrow et al., 2005). To assess adaptive behavior, the Vineland Adaptive Behavior Scales-2 (VABS-2) (Sparrow et al., 2005) was completed by the child’s parents at each of the assessments. The VABS-2 helped to provide a broad overview of each participant’s level of functioning and helped to highlight participants’ strengths and weaknesses. Internal-consistency reliabilities of the domain and composite scores of the VABS-2 ranged from 0.77 to 0.97, and the test–retest reliability coefficients ranged from 0.75 to 0.94 for children of the age included in this study (Sparrow et al., 2005).
Social skills
The Social Skills Improvement System (SSIS) (Gresham and Elliott, 2008) is a standardized assessment used to measure a child’s social skills and problem behaviors. The SSIS requires parents to rate their child’s behavior on a scale from 0 to 3, with 0 meaning the behavior never occurs and 3 meaning it almost always occurs across a range of 12 subscales in order to provide a comprehensive social skills assessment (Gresham and Elliott, 2008). These subscales make up two scales, Social Skills and Problem Behaviors, that have a possible raw score range of 0–138 and 42–134, respectively. Internal-consistency reliabilities of the scale and subscale scores of the SSIS Parent Form ranged from 0.76 to 0.96, and the test–retest reliability coefficients ranged from 0.73 to 0.88 for children of the age included in this study (Gresham and Elliott, 2008).
Behavioral video coding
Each intervention session concluded with a 10-min free play period that allowed the participants to explore the equipment, practice newly learned skills, and engage in activities of their choosing. The free play period of the first and last intervention sessions (i.e. sessions 1 and 12) were videotaped using a Sony Handycam HDR-CX110, and these videos were coded by the principal investigator using Social Behavior Codes that were adapted from Hauck et al.’s (1995) Behavior Coding Scheme. None of the codes were removed from Hauck et al.’s (1995) original scheme; however, seven additional categories were added to better account for the nature of the group free play session: Appropriate Play, Inappropriate Play, Verbal Response, Non-verbal Response, Target of Initiation/Response—Adult, Target of Initiation/Response—Child, and Out of Frame. Behaviors were recorded at 15-s intervals for each child, and the target of their behavior (i.e. adult or child) was also recorded when appropriate. Inter-rater reliability was established with a trained research assistant on 27% of the videos with an average intraclass correlation coefficient of 0.922.
Motor skill intervention
Group 1 attended a 12-week FMS intervention for 1 h per week, while Group 2 acted as a control. Group 2 then attended a 6-week FMS intervention for 2 h each week (1 h per day on 2 separate days). Despite differences in intervention intensity, both groups received 12 h of direct instruction, and all sessions were the same between the two groups (i.e. the same instruction and content). All intervention sessions were conducted in a multipurpose room at the local Children’s Treatment Centre. Each intervention session was run by the primary investigator with assistance from trained undergraduate research assistants; the instructor-to-child ratio for both groups ranged from 1-to-2 to 1-to-1, depending on attendance. Each session followed the same format consisting of seven activities: warm-up, review of previously learned skill, direct instruction of new skill, practice of new skill, obstacle course, free play, and clean-up. Transitions between the seven activities were guided through a large Picture Exchange Communication System that was created for this study using task appropriate images for a motor skill intervention.
Each session focused on teaching one core skill, while integrating previously learned skills into the review period and obstacle course. Skills that were taught included both locomotor (running, hopping, leaping, etc.) and object control (throwing, catching, kicking, etc.) skills, and they progressed in difficulty over the intervention period (beginning with balance on Day 1 and ending with striking on Day 12). Instructions on how to perform the skills were given to the participants in single steps (e.g. “hold the ball,” “watch me,” “throw at the ‘x’,” etc.), and multiple demonstrations were made by the instructors on how to perform the skill. Additionally, physical prompts were provided to participants who needed assistance to understand how to hold a piece of equipment or perform the skills. Given our low instructor-to-participant ratio, all participants were engaged in the activities at the same time, with an instructor working closely with them to keep them on task and practicing. For example, while working on throwing the participants would be spaced out throughout the room with an instructor, various balls, and targets in order to individually learn and practice the skill. The obstacle course and free play then provided opportunities for the participants to engage more with one another, as opposed to an instructor.
Statistical analyses
Part 1: intervention effectiveness—experimental versus control group
Descriptive characteristics were calculated on all variables at Assessment 1 (baseline) for the experimental and control groups. An independent samples t-test was used to assess differences between the experimental and control groups at Assessment 1 on all continuous variables; Fisher’s exact test was used to assess differences in the sex distribution between the two groups. The magnitude of change from pre- to post-intervention for each participant in the experimental and control groups was calculated by subtracting their pre-intervention score from their post-intervention score on the raw subscale scores and quotient scores of the PDMS-2, as well as the raw subscale scores and domain scores of the VABS-2 and SSIS. The average magnitude of change was then calculated for both the experimental and control groups. A t-test was used to test for significant differences between the experimental and control groups on their magnitude of change from pre- to post-intervention for all variables. Effect sizes were also calculated on the average magnitude of change scores in the experimental and control groups for all PDMS-2, VABS-2, and SSIS variables. These analyses were used to determine the effectiveness of the motor skill intervention at improving motor skills, adaptive behavior, and social skills in the experimental group in comparison with the control group who did not receive the intervention.
Part 2: analysis of intervention intensity—Group 1 versus Group 2
In order to assess whether the effects of randomization had been maintained during the initial control period, descriptive characteristics were calculated for Group 1 and Group 2 at their respective pre-test prior to conducting analyses of the effectiveness of the two different intensities of the intervention. An independent samples t-test was used to assess whether there were any differences between Group 1 (Assessment 1 results) and Group 2 (Assessment 2 results) at their pre-test on all continuous variables; Fisher’s exact test was used to assess differences in the sex distribution between the two groups. Assumptions of skewness and kurtosis were met to conduct a two-way analysis of variance (ANOVA) with repeated measures on all PDMS-2, VABS-2, and SSIS variables at the pre-test, post-test, and 6-week follow-up assessments by group to assess group and group by time interactions (Group 1 = 1× per week for 12 weeks; Group 2 = 2× per week for 6 weeks). This analysis also provided us with a time interaction, which indicated the overall effect of the intervention with the groups combined.
Part 3: individual changes in adaptive behavior and social skills
Due to the variability in overall functioning of the complete sample, all adaptive behavior and social skill variables were examined for individual changes from pre- to post-intervention and to the 6-week follow-up. An increase in adaptive behaviors on the VABS-2 and social skills on the SSIS was seen as an improvement. In contrast, a decrease in maladaptive behaviors on the VABS-2 and a decrease in problem behaviors on the SSIS were recognized as an individual improvement.
Part 4: behavioral video coding
The frequency of social behaviors from the free play videos were examined for individual changes from the first to last intervention sessions. A paired t-test was employed to examine group differences on the social behaviors that occurred most frequently from the free play sessions of the first to last intervention session.
Power calculation
Given our current sample of nine participants, we have 59% power to detect statistical differences at an alpha level of 0.05 on our primary outcome measure, the PDMS-2 total motor quotient. In order to detect a clinically important difference on the PDMS-2 with 80% power and an alpha level of 0.05, we require a sample of 14 participants.
Results
Part 1: intervention effectiveness—experimental versus control group
Descriptive statistics of the participants at Assessment 1 are presented in Table 1. One participant in Group 2 was absent for the first assessment; however, he was present for the other three assessments, so is included in the analyses of intervention intensity (Part 2). All participants had motor skills that were very poor, poor, or below average on the gross, fine, and total motor quotients of the PDMS-2, and all participants had a MABC-2 total test score below the fifth percentile at Assessment 1, indicating significant movement difficulties. All participants had a standard score of 80 or below on the VABS-2 adaptive behavior composite at Assessment 1, indicating that their adaptive levels were in the low (standard score of ≤70) and moderately low (standard score of 71–85) categories. Finally, all participants had SSIS social skills scores at or below the 25th percentile at Assessment 1, indicating significant social impairments.
Descriptive characteristics, motor proficiency, adaptive behavior, and social skills by group at Assessment 1.
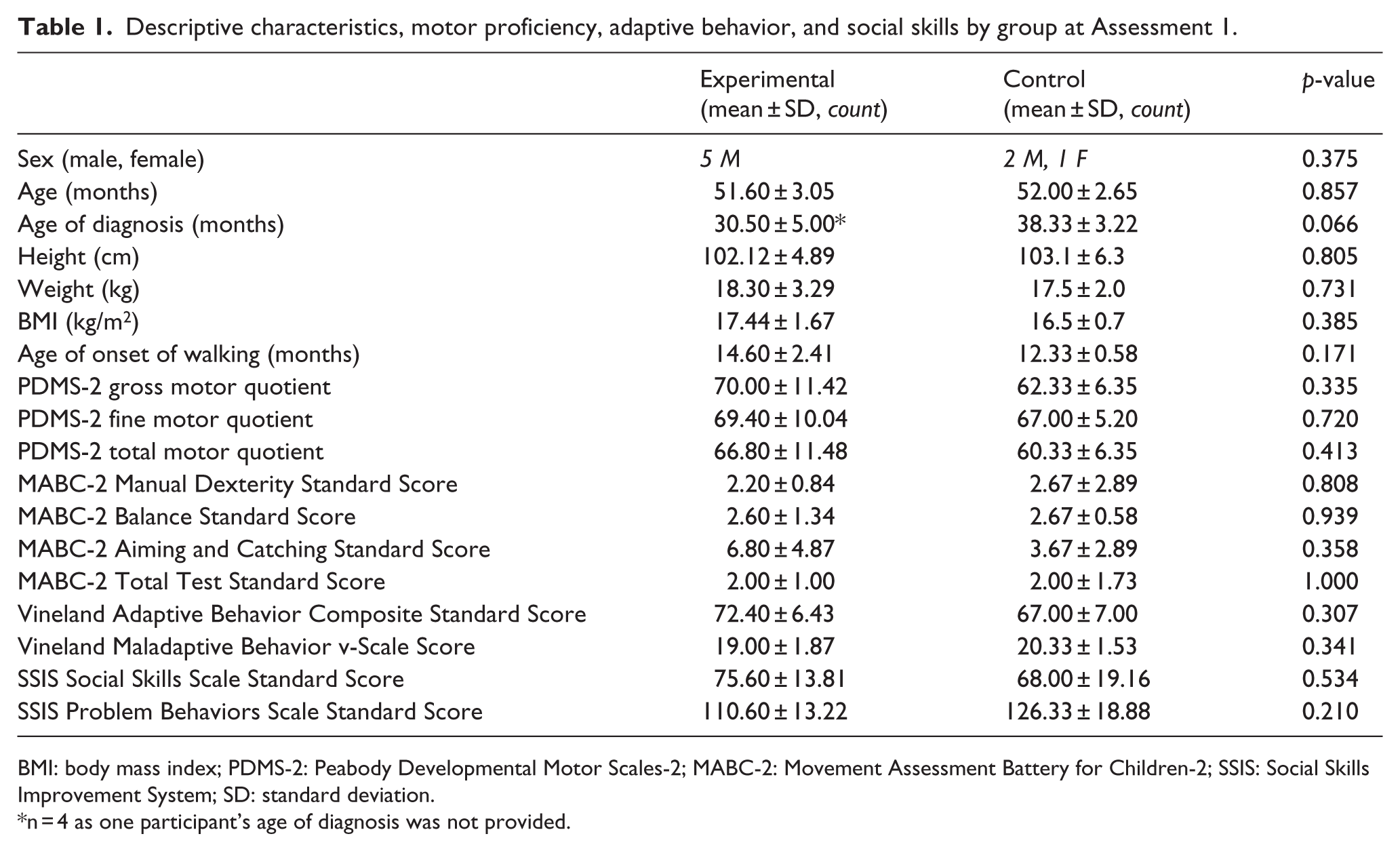
BMI: body mass index; PDMS-2: Peabody Developmental Motor Scales-2; MABC-2: Movement Assessment Battery for Children-2; SSIS: Social Skills Improvement System; SD: standard deviation.
n = 4 as one participant’s age of diagnosis was not provided.
The average magnitude of change from pre- to post-intervention was calculated for all PDMS-2, VABS-2, and SSIS variables in the experimental and control groups. Overall improvements were seen in the experimental group from pre- to post-intervention on all PDMS-2 variables. Significant differences in motor scores from pre- to post-intervention were found between the experimental and control group on the PDMS-2 object manipulation raw score and the PDMS-2 total motor quotient (Table 2). No significant differences were found between the experimental and control groups on the VABS-2 adaptive behavior composite (p = 0.136), maladaptive behavior index (p = 0.798), or any of the other VABS-2 variables following the intervention. Similarly, no significant differences were found on any of the SSIS variables, including the social skills standard score (p = 0.783) and the problem behavior standard score (p = 0.855) from pre- to post-intervention between the experimental and control groups.
Magnitude of change scores from pre- to post-intervention on the PDMS-2 in the experimental and control group.
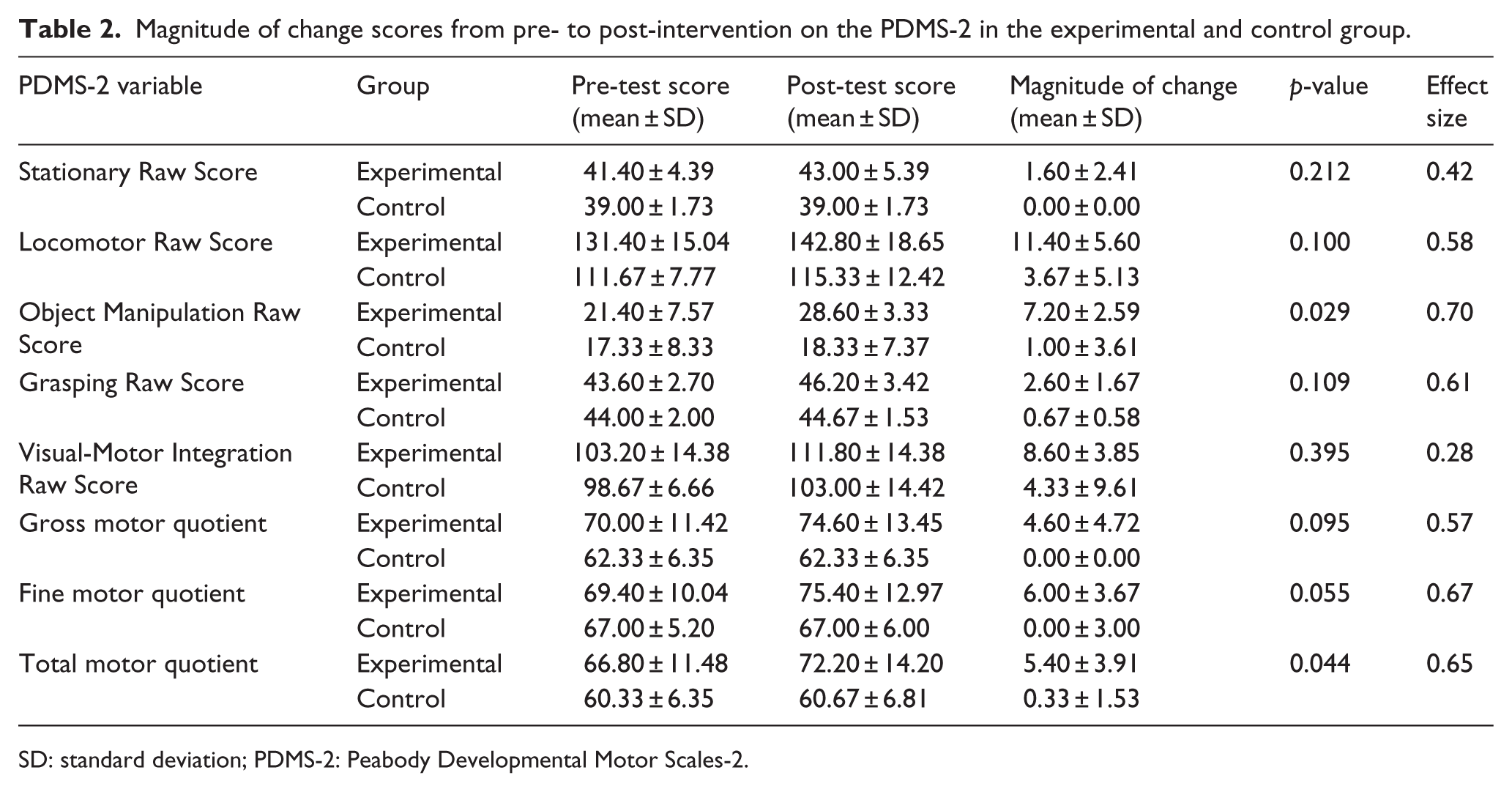
SD: standard deviation; PDMS-2: Peabody Developmental Motor Scales-2.
Part 2: analysis of intervention intensity—Group 1 versus Group 2
No significant differences were found between the groups with regard to their age, overall motor proficiency, adaptive behavior, and social skills at their respective pre-test (i.e. Group 1 during Assessment 1, Group 2 during Assessment 2), indicating that the effect of randomization was maintained following Part 1 of the analysis. The average attendance at the intervention sessions was 71.6% and 66.6% for Groups 1 and 2, respectively (t(7) = 0.541, p = 0.605). The results of the two-way ANOVA with repeated measures on the PDMS-2 variables from pre- to post-test to 6-week follow-up by group are presented in Table 3 and indicate no significant differences in outcomes between the two intervention intensities.
Pre-test, post-test, and 6-week follow-up PDMS-2 scores by group.
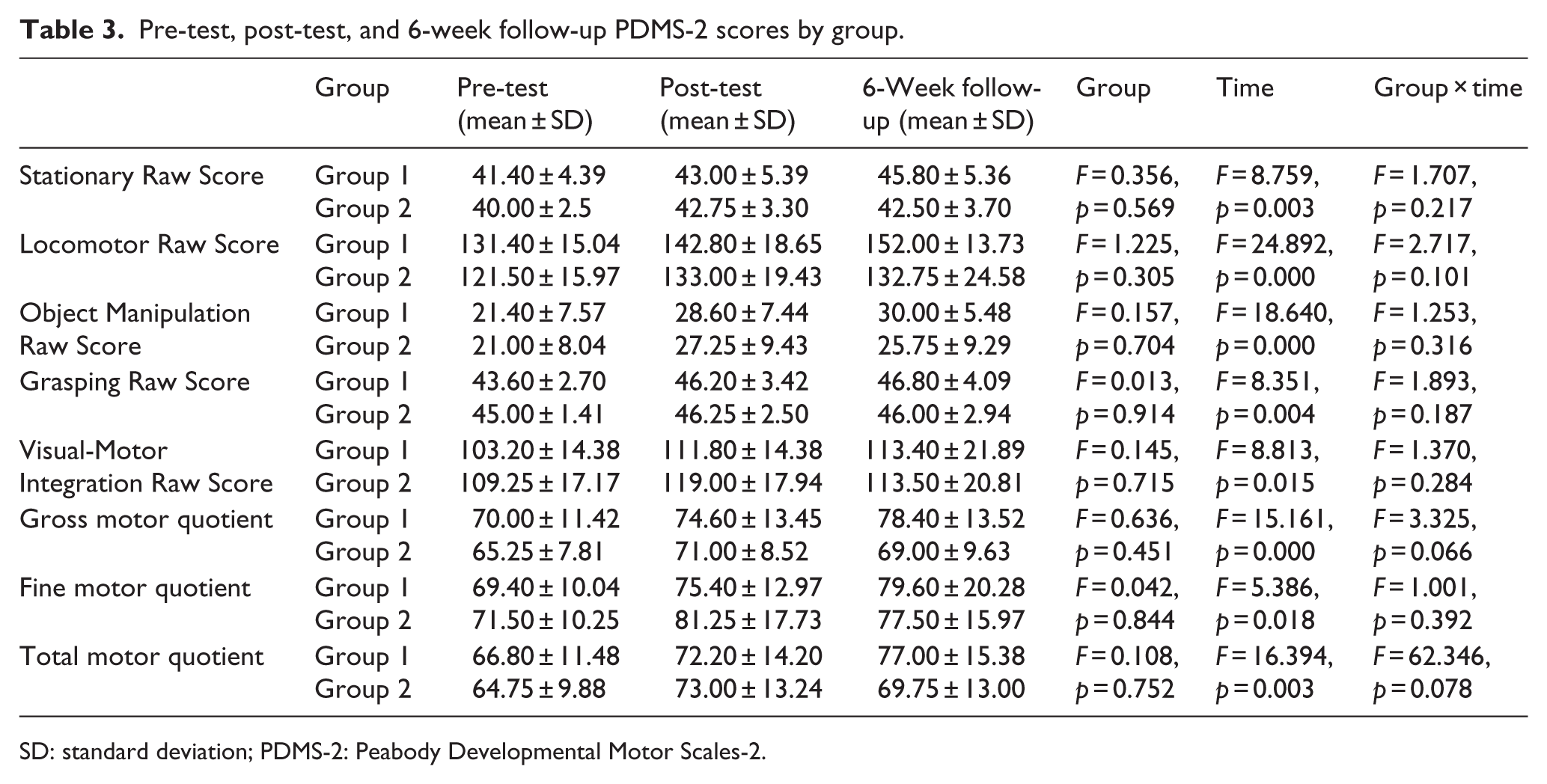
SD: standard deviation; PDMS-2: Peabody Developmental Motor Scales-2.
The two-way ANOVA with repeated measures also indicated that with the groups combined, time was a significant factor for all PDMS-2 variables; which means that there were significant differences between the pre-, post-, and 6-week follow-up assessments. Post hoc analyses with Bonferroni corrections revealed that for the complete sample, the PDMS-2 stationary raw score improved significantly between the pre-test and 6-week follow-up (p = 0.017). The PDMS-2 locomotor and object manipulation raw scores improved significantly from the pre- to post-test (p = 0.003 and p = 0.001, respectively) and from the pre-test to 6-week follow-up (p = 0.001 and p = 0.003, respectively). Furthermore, the PDMS-2 grasping and visual-motor integration raw scores significantly improved pre- to post-intervention (p = 0.043 and p = 0.000, respectively) and retained that improvement from the post-test to the 6-week follow-up (p = 1.000 and p = 1.000, respectively). The PDMS-2 fine motor quotient improved significantly from the pre- to post-test (p = 0.016) and did not decline at the 6-week follow-up (p = 1.000). Finally, the PDMS-2 gross and total motor quotients improved significantly from the pre- to post-test (p = 0.018 and p = 0.005, respectively) and from the pre-test to 6-week follow-up (p = 0.003 and p = 0.017, respectively).
In regard to adaptive behavior and social skills, time was not a significant factor on the VABS-2 adaptive behavior composite (F(2, 8) = 3.921, p = 0.065), maladaptive behavior index (F(2, 10) = 0.404, p = 0.678), or any other VABS-2 variables. Time was also not significant for the SSIS social skills standard score (F(1.084, 5.420) = 1.298, p = 0.308), problem behavior standard score (F(2, 10) = 1.108, p = 0.396), or any other SSIS variable. Furthermore, no group-by-time interactions were present on any of the VABS-2 variables including the adaptive behavior composite (F(2, 8) = 2.879, p = 0.114) and maladaptive behavior index (F(2, 10) = 0.505, p = 0.618). Similarly, no group-by-time interactions were evident on any of the SSIS variables including the social skills standard score (F(1.084, 5.420) = 4.425, p = 0.084) and the problem behavior standard score (F(2, 10) = 1.058, p = 0.383). Group assignment was significant for the VABS-2 daily living skills standard score (F(1, 4) = 24.590, p = 0.008), with Group 2 scoring significantly higher than Group 1; no other significant group differences were present.
Part 3: individual changes in adaptive behavior and social skills
Six participants had complete data on all domains of the VABS-2 and SSIS at the pre-test, post-test, and 6-week follow-up assessments. Three of these participants improved in at least half of the subdomains examined on the VABS-2 and the SSIS from the pre- to the post-test, and five of them improved in at least half of the subdomains from the pre-test to the 6-week follow-up. Furthermore, four of the participants with complete data for the VABS-2 adaptive behavior composite standard score improved this score from the pre- to the post-test, and all participants improved their VABS-2 adaptive behavior composite standard score from the pre-test to the 6-week follow-up. The VABS-2 individual subdomain raw scores were examined, and it was found that five participants improved in regard to “playing and using leisure time,” “using large muscles,” and “using small muscles” from pre-intervention to the 6-week follow-up. In regard to the SSIS, five participants improved from the pre-test to the 6-week follow-up on their “assertion” and “engagement” raw scores, as well as decreasing their number of “externalizing” and “internalizing” problem behaviors.
Part 4: behavioral video coding
Three of the participants in Group 1 were absent for their final intervention session; thus, we did not have complete pre- and post-behavioral videos for the free play sessions. Therefore, six of the participants were included in the analyses of behavioral changes. There were no statistically significant group changes in regard to the participant’s behavior pre- to post-intervention; however, functional improvements were made. The average percentage of time that the complete sample spent engaging in appropriate play, inappropriate play, and responding verbally, as well as the time they were out of frame, is presented in Figure 1.
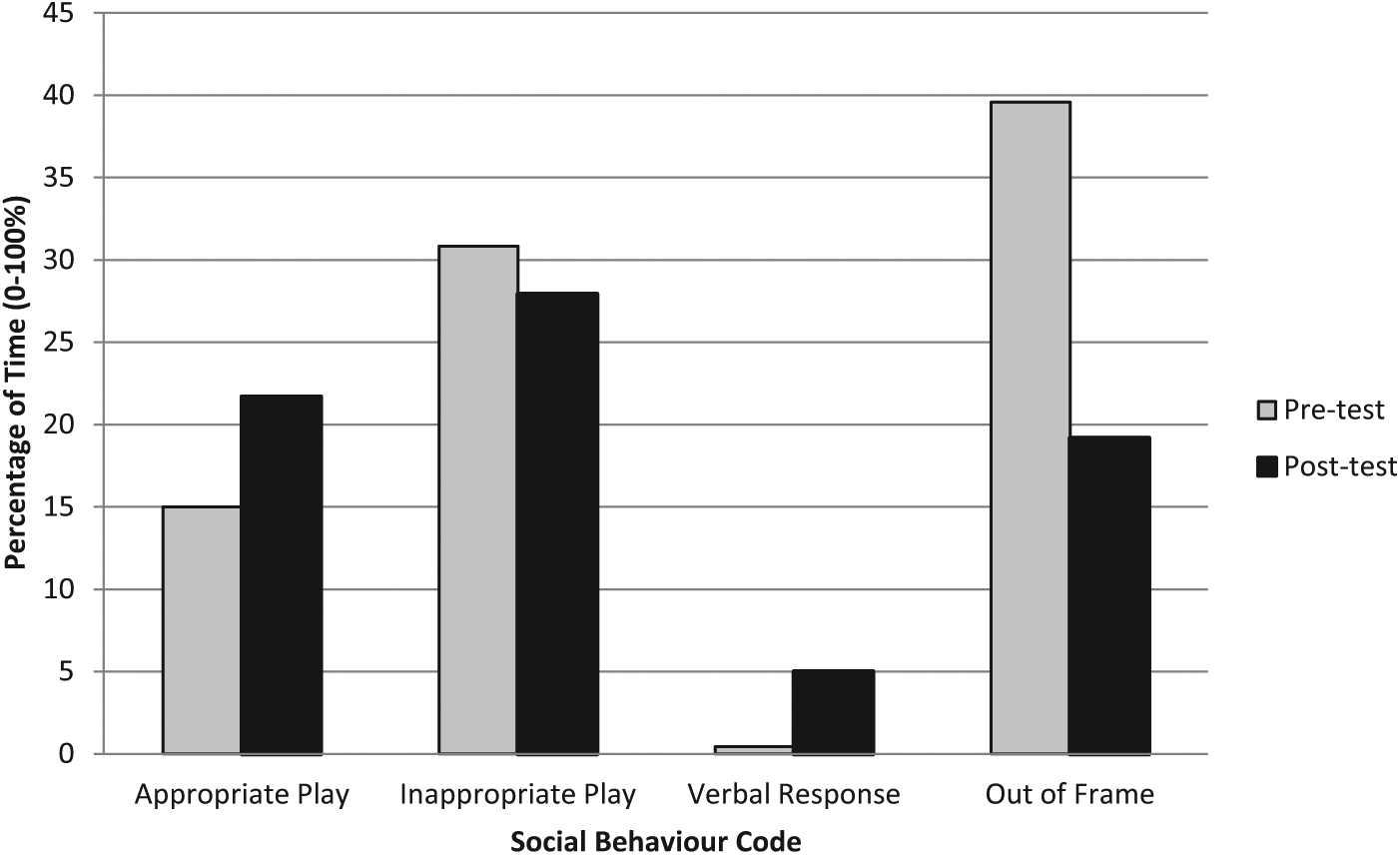
Average percentage of time engaged in select activities during the 10-min free play period pre- to post-intervention for the complete sample (n = 6).
Discussion
The purpose of this study was to investigate the effectiveness of an FMS intervention at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with ASD. Our results indicate that the motor skills of the experimental group significantly improved following the FMS intervention, in comparison with the control group who did not receive the intervention; however, no significant changes were evident in regard to adaptive behavior and social skills. The secondary purpose of this study was to investigate whether a higher intensity of the same intervention was more or less effective at improving our primary outcomes. Our results indicate that there were no significant differences between the two intensities in regard to motor skills, adaptive behavior, and social skills.
Previous studies have found that FMS interventions can be effective at improving the FMS of 3- to 5-year-old children with developmental delays, excluding children with ASD (Kirk and Rhodes, 2011). To date, no published studies have examined the effectiveness of FMS interventions for young children with ASD or explored the impact of an FMS intervention on adaptive behavior and social skills; thus, our study has provided insight into this gap in the literature. We found that the children in the experimental group significantly improved on the PDMS-2 object manipulation raw score and the total motor quotient following the intervention; however, the moderate to large effect sizes on the remaining PDMS-2 variables indicate the positive effect of the intervention and justify further study with a larger sample. The significant improvement in object manipulation skills following the intervention may be relevant for the overall functioning of a child with ASD. MacDonald et al. (2013) found that the object control skills of 6- to 15-year-old children with ASD significantly predicted their social communicative skills, meaning that those individuals with better object control skills were more likely to have better social communicative skills. The relationship between object control and social communicative skills is likely due to the social aspect of many object control skills, such as playing catch with a peer. The significant improvement in object control skills in this study may be partly attributed to the low ratio of instructors to participants in the intervention, which provided very intensive, and supportive, opportunities for skill practice. If we can improve the object control skills of young children with ASD through early intervention, they may have more opportunities for social communicative interactions (e.g. recess or playground play) throughout childhood.
All participants scored below the fifth percentile on the MABC-2 and were below average on the PDMS-2 at baseline, which is consistent with the previous literature (Liu and Breslin, 2013; Lloyd et al., 2013; Matson et al., 2010; Ozonoff et al., 2008); thus, any functional improvements in motor skills may be relevant for an individual child with ASD. These functional improvements are evident in our sample as many participants improved their PDMS-2 categorizations from the pre- to post-test to 6-week follow-up assessments. For example, six participants had a gross motor quotient score that was categorized as very poor at the pre-test; only four and three participants were categorized as very poor at the post-test and 6-week follow-up, respectively. Similarly, in regard to the total motor quotient, seven participants were in the very poor category at baseline, one was categorized as poor, and one as below average. By the 6-week follow-up, only four participants were categorized as very poor, two as poor, two as below average, and one as average; thus, many individual improvements in motor skills were made throughout the intervention. These individual improvements may provide our participants with the skills and ability to engage in active play with peers and siblings.
There were no statistical differences between the experimental and control groups on the VABS-2 and SSIS variables. One potential reason for this finding may be the heterogeneity of our sample and our small sample size. Previous research has also demonstrated large differences and variability in the individual responses of children with ASD to various interventions (Lord et al., 2005; Magiati et al., 2011; National Research Council, 2001). Furthermore, social and behavioral skills are very complex to measure in children with ASD, and there are no measures that are universally recognized as being the gold standard for assessment of these skills (Dowd et al., 2010), which can make it difficult to measure and detect group changes in a research or clinical setting. Finally, it is unlikely that we would see significant changes in adaptive behavior and social skills over the course of this relatively short study duration (i.e. 12–18 weeks). Therefore, these findings justify a need not only for further investigation with a larger sample and longer follow-up but also to examine our results on an individual basis to look for functional changes in each participant.
The secondary purpose of this study was to investigate whether a higher intensity of the FMS intervention was more or less effective at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with ASD. Our results from the two-way ANOVA with repeated measures indicate that there were no group-by-time interactions for any of the variables, which demonstrates that there was no difference between the two intensities of the intervention. This finding is relatively consistent with the previous literature that has found large variability in both the intensity (i.e. the frequency of sessions) and dosage (i.e. number of sessions) of motor skill interventions for preschool-aged children with typical development and developmental delays—all of which seem to be moderately effective at improving motor skills but have failed to measure the ensuing impact on adaptive behavior and social skills (Kirk and Rhodes, 2011; Riethmuller et al., 2009). As intervention intensity was not significant in this study, we recommend that future research investigate the role of intervention dosage on study outcomes.
We did find time to be a significant factor for all PDMS-2 variables, indicating that the complete sample significantly improved in all subdomains of the PDMS-2, regardless of the intensity. Motor improvements at the post-test were retained at the 6-week follow-up in Group 1, although slight declines were evident from the post-test to 6-week follow-up in Group 2. Skill retention is an essential element of program effectiveness, and our results suggest that skills were retained in Group 1; however, it is possible that a longer follow-up period could demonstrate differences in skill retention following the two intensities of intervention. We recommend that future studies include a longer follow-up to better understand the impact of the intervention, and its intensity, on skill retention.
No significant group changes in adaptive behavior and social skills were evident following the intervention or at the 6-week follow-up; however, there were individual improvements in adaptive behavior and social skills following the intervention, as well as individual reductions in maladaptive behaviors. These individual improvements can be interpreted as functional gains for the individual child, which may have clinical relevance and implications for overall functioning. For example, improvements in assertion and engagement as noted in the SSIS results may help a child become more involved at home and school. Improvements in playing and using leisure time combined with reductions in maladaptive behavior on the VABS-2 may make it easier for a child to engage in play and be included by peers and siblings. More research is required to better understand the implications of an FMS intervention on adaptive behavior and social skills.
The results of the behavioral video coding further demonstrate the functional improvements in behavior that were made by the participants over the course of the intervention. For example, there was an increase in the time spent participating in appropriate play (e.g. playing catch with a peer) and a decrease in the time spent in inappropriate play (e.g. engaging in self-stimulatory activities) from the first to last intervention session. Furthermore, there was a decrease in the number of instances that participants were out of frame from the first to last intervention session, indicating a reduction in off-task behavior. Given the size of the room and the camera placement, out of frame activities were typically off-task behaviors such as sitting alone in a corner or attempting to leave the room. The changes seen in the behavioral video coding are considered to be positive outcomes from the intervention as appropriate play skills may be essential for the ability of a child to engage in social activities with peers.
The ability to engage with peers may be important for further overall development as a child with ASD gets older. For example, a study of the developmental progression of adolescents with autism who had been assessed in preschool and middle school found that language skills in adolescence could be predicted by functional play skills, responsiveness to others, and the frequency of requesting behaviors in early childhood (Sigman and McGovern, 2005). The individual gains in adaptive behavior and social skills, including the increased time spent in appropriate play following this motor skill intervention, may provide a platform for future engagement in play and social interactions and warrants further research.
Early intervention is of utmost importance for children with ASD, and there are a wide range of services available to these children (Myers and Johnson, 2007). However, these services can be cost prohibitive (Chasson et al., 2007) and typically only focus on the core deficits of ASD (Matson and Smith, 2008). In contrast, this motor skill intervention was implemented with minimal funding and in a community setting; it likely could also be implemented through recreation programs and integrated into physical education classes. It is well documented that children with ASD experience challenges in the motor domain (Liu and Breslin, 2013; Lloyd et al., 2013; Ozonoff et al., 2008); however, motor skills are often neglected in the intervention literature. The positive gains that were made in motor skill proficiency may have important implications for the ability of participants to become more engaged with their peers, family, and community throughout their life. For example, Titus and Watkinson (1987) noted that providing a brief period of segregated motor skill instruction to a small group of 5 to 10-year-old children with moderate intellectual disabilities contributed to the children’s ability to keep up, physically and socially, with their peers with typical development in an integrated free play setting; which can have positive implications for playground inclusion throughout childhood. Similarly, being able to move efficiently can help a child participate during family outings and activities, such as going to the park or for a bike ride. Motor skills are also essential for community participation such as attending a camp, playing on a sports team, or participating in individual physical activities within a community organization. These increased opportunities that stem from motor skill proficiency can in turn provide a platform for the development of social and communicative skills, thus positively impacting the overall development of an individual with ASD.
Limitations
As with all studies, there are limitations to these findings. The first limitation is our small sample size, which limits our statistical power. The small sample led to a higher risk for false-negative results which is corroborated by results with moderate to large effect sizes that did not reach (but approached) the level of significance (p < 0.05). A larger sample was not feasible due to the scope and resources of this pilot study. A second limitation stemming from our small sample size is that we would have ideally had a third group that was a true control throughout the entire study and been able to run the two different intensities of the intervention simultaneously. This would give us an even better indication of the effectiveness of the intervention, as well as the differences in intervention intensity on the study outcomes. Unfortunately, including a third group was not plausible for this study due to limited resources, and there are ethical questions of not providing control participants with a presumably effective treatment.
A third limitation is the group imbalance and that there was only one female in the study. Ideally, there would be equal numbers of participants, by sex, in each group; we included the lone female in the analyses due to the already small sample size, the heterogeneity of symptoms that children with ASD experience, and to remain representative of the overall sex ratio in ASD. We also found that the small group worked well in terms of group dynamics, while still providing opportunities for social interactions. We recommend that future FMS interventions for young children with ASD include a larger sample, but deliver the intervention in multiple small groups (e.g. 4–6 children) in order to maintain a controlled environment.
There is a potential selection bias in our sample as participants were recruited through a local Children’s Treatment Centre and parents had to be able and willing to bring their child to the intervention sessions. Thus, it is possible that the participants may have had a higher socioeconomic status and more motivated parents than the general population of 4-year-old children with ASD. Another limitation is our relatively low attendance rates (71.6% and 66.6% for Groups 1 and 2, respectively), given that there were only 12 intervention sessions. One possible reason for these low rates of attendance is that due to space constraints at the Children’s Treatment Centre the majority of our sessions were held on weekday afternoons. This time slot made it challenging for some parents to bring their child to all sessions due to commitments with work and school, as some participants were attending part-time junior kindergarten. We recommend that future intervention sessions be scheduled in the early evening on weekdays or during the weekend in order to improve attendance rates.
A final limitation to this study is that baseline IQ was not measured. We know that IQ is related to motor skill proficiency (Lahtinen et al., 2007; Vuijk et al., 2010) and overall functioning in children with ASD (Klin et al., 2007; Perry et al., 2009; Sigman and McGovern, 2005); thus, it may have had an impact on the intervention outcomes. We suggest that future research assess and control for IQ in order to better understand its impact on motor skills, adaptive behavior, and social skills. Despite these limitations, we still found significant group improvements in motor skills and individual gains in adaptive behavior and social skills following the intervention. These findings are promising, particularly as this is the first study to investigate the effectiveness of an FMS intervention at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with ASD.
Conclusion
The aim of this study was to examine the effectiveness of an FMS intervention at improving the motor skills, adaptive behavior, and social skills of 4-year-old children with ASD and to explore potential differences between two intensities of the intervention. Our results indicate that the FMS intervention was effective at improving the motor skills of the children in our experimental group when compared to the control group. Furthermore, all children on average had improvements in motor skills from the pre- to post-test and retained their improvements at the 6-week follow-up. No significant group differences were evident in regard to adaptive behavior and social skills; however, we found individual improvements in these areas. The functional gains in motor skills, adaptive behavior, and social skills following this intervention may have important implications for the overall functioning of a young child with ASD, including their ability to engage in active play. These findings suggest that an FMS intervention can be effective at improving the motor skills of 4-year-old children with ASD; more research is required to further explore the implications for adaptive behavior and social skills.
Footnotes
Funding
This research was supported by a Queen Elizabeth II Graduate Scholarship in Science & Technology and a Canadian Institutes of Health Research Canada Graduate Scholarship awarded to the first author for work conducted during her Master’s degree.