
Abstract
This study describes medical conditions experienced by a population-based cohort of adults with autism spectrum disorder whose significant developmental concerns were apparent during childhood. As part of a 25-year outcome study of autism spectrum disorder in adulthood, medical histories were collected on 92 participants (N = 69 males) who were first ascertained as children in the mid-1980s, 11 of whom were deceased at the time of follow-up. Questionnaires queried medical symptoms, disorders, hospitalizations, surgeries, and medication use. Median age at follow-up was 36 years (range: 23.5–50.5 years), and intellectual disability co-occurred in 62%. The most common medical conditions were seizures, obesity, insomnia, and constipation. The median number of medical conditions per person was 11. Increased medical comorbidity was associated with female gender (p = 0.01) and obesity (p = 0.03), but not intellectual disability (p = 0.79). Adults in this cohort of autism spectrum disorder first ascertained in the 1980s experience a high number of chronic medical conditions, regardless of intellectual ability. Understanding of these conditions commonly experienced should direct community-based and medical primary care for this population.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder on a continuum of symptom severity. It is characterized by deficits in social communication and interaction, as well as restricted patterns of behavior, interests, and/or activities (American Psychiatric Association (APA), 2013). The Centers for Disease Control and Prevention’s (CDC) Autism and Developmental Disabilities Monitoring Network (ADDM) has estimated ASD prevalence as 1 in 68 children in the United States and 1 in 54 children in Utah (CDC ADDM, 2014). Today’s adults with ASD who were identified during childhood with significant developmental concerns provide important information regarding increased susceptibility to multiple medical comorbidities, particularly for individuals with more severe manifestations of ASD. For these adults, general health status can be inseparable from quality of life, yet coexisting communication impairment interferes with their capacity to describe sources of discomfort or distress. Identifying common comorbid conditions associated with ASD throughout the lifespan will inform providers of key areas in which to focus their medical assessment of this special-needs population, including prevention of common medical concerns.
Multiple prior studies have described common medical conditions experienced by children with ASD (Doshi-Velez et al., 2014; Kohane et al., 2012; Schieve et al., 2012). The most common conditions include seizures (7.6%−77.5%; Bolton et al., 2011; Danielsson et al., 2005; Hara, 2007; Kohane et al., 2012), sleep disorders (1.25%−76.3%; Kotagal and Broomall, 2012; Patzold et al., 1998; Polimeni et al., 2005; Wiggs and Stores, 2004), weight problems (both overweight and underweight; Bölte et al., 2002; Broder-Fingert et al., 2014; Curtin et al., 2010; Egan et al., 2013; Mouridsen et al., 2002, 2008; Phillips et al., 2014; Rimmer et al., 2010), and gastrointestinal (GI) problems (12.2%−70.0%; Adams et al., 2011; Chaidez et al., 2014; Erickson et al., 2005; Hsaio, 2014; Ibrahim et al., 2009; McElhanon et al., 2014; Valicenti-McDermott et al., 2006). Children with ASD also experience higher rates of asthma, seasonal and food-related allergies, eczema, chronic headaches, and limited mobility (Schieve et al., 2012).
Although these medical conditions may persist into adulthood, their prevalence and sequelae are poorly understood in adults with ASD. Medical comorbidity studies report seizures in 21%−38% of adults with ASD, the majority of whom experienced their first seizure after 10 years of age (Bolton et al., 2011; Danielsson et al., 2005; Giovanardi et al., 2000). Most adult ASD studies of sleep disturbance report rates between 75% and 80% (Oyane and Bjorvatn, 2005; Tani et al., 2003). The presence of obesity is far less consistent, however: European studies demonstrated lower than expected body mass indexes (BMIs) among young adult males with ASD (Bölte et al., 2002; Mouridsen et al., 2002, 2008), while US studies of adults with ASD report obesity rates (35%−42%; Eaves and Ho, 2008; Tyler et al., 2011) meeting or exceeding the background US population norm (34.9%; Ogden et al., 2014). Increased prevalence of neurologic disorders, bowel disorders, diabetes mellitus type I, autoimmune diseases, and muscular dystrophy have also been identified in adults with ASD (Kohane et al., 2012). Fracture risk is also increased in both children and adults with ASD, although it is unclear whether this is related to use of specific medications (Neumeyer et al., 2015).
Population-based studies are needed to describe the medical comorbidity burden, medication use, and major medical events (hospitalizations and surgeries) experienced by adults with ASD, and to explore variable risk associated with gender, age, and co-occurring intellectual disability (ID). This study examines these issues through active participation by adults and their caregivers during an ASD adult follow-up study. Participants were initially identified during childhood in the mid-1980s with significant developmental concerns, thus representing today’s population of adults with severe ASD.
Methods
Participants
Participants were first assessed as children during the UCLA-University of Utah epidemiologic survey of autism (Ritvo et al., 1989, 1990). This sample was re-contacted between 2006 and 2011 for participation in an adult outcome study. Records collected during the original study were re-examined using Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000)-based CDC ADDM methodology for participants who did not meet Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III) autism criteria (APA, 1980). Individuals who were reclassified based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria could have met an ASD, Asperger’s, or pervasive developmental disorder (PDD) diagnosis. The details of the reclassification study have been previously published (Miller et al., 2013). For this study, participants were eligible if they were identified with DSM-III autism during the original study or reclassified as having ASD based on DSM-IV-TR during the reclassification study.
Of the 305 individuals with ASD case status (241 with DSM-III autism, 64 with DSM-IV-TR ASD classification), 92 participated in the medical comorbidity component of the adult outcome study. There are no statistically significant differences between the participants in the medical comorbidities follow-up group and the remaining ASD cases in regard to gender and intellectual functioning; however, the median age of this cohort in the medical comorbidities follow-up study is significantly higher than that of the larger ASD cohort (36.1 vs 33.2 years, p = 0.02, respectively). The majority of the original participants were lost to follow-up. The cohort included three sets of siblings, none of whom were twins. Medical information from those who were deceased at the time of the follow-up (11 individuals out of 92) was not used in the medication analysis as no current medications were taken, nor in the BMI analysis as measurements were not available. Comorbidities, surgeries, and hospitalizations relating to the deceased were included in descriptive analyses. All information for this subgroup was provided by a living caretaker after the participants’ demise. Characteristics and medical comorbidities for this segment are included in Tables 1 and 2. A full mortality evaluation of the original cohort has previously been published (Bilder et al., 2013).
Characteristics of deceased participants (N = 11).
SD: standard deviation.
Frequency of medical conditions, hospitalizations, and major surgeries among deceased participants (N = 11) identified with ASD in Utah. a

ASD: autism spectrum disorder.
Per caregiver report.
Procedures
Permission to conduct this study was obtained from the University of Utah and the Utah Division of Services for People with Disabilities’ Institutional Review Boards. Contact information for eligible individuals was obtained from the original epidemiological survey data from the 1980s, public records databases, or available telephone directories. Participants if able, or their caregiver, completed forms querying medical history (medical problems, treatment, hospitalizations, surgeries, current medications) and a semi-structured medical review of systems (ROS) of current and prior symptoms (Supplement 1, available online). The questionnaire was created by a medical doctor (MD) and registered nurse (RN) based on a basic ROS and medical history that was adapted to meet common conditions often found in individuals with ASD. A follow-up interview was conducted if needed for further clarification on symptoms/conditions with the caregiver and participant (if able) in participants’ homes. Collected information was based entirely upon recall of the individual with ASD and/or caregiver. Medical diagnoses were based on prior physician-provided diagnoses, whereas the ROS was based on individual or caregiver report of symptoms. BMI was calculated on 58 participants for whom current height and weight were available through measurement by study personnel. Interview raters were familiar with the components and appropriate use of the assessment tools and had clinical experience with individuals with developmental disorders. Information was collected over a half-day period, and participants were compensated for their time.
Intellectual functioning
Assessments completed for intellectual ability included the Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV; Wechsler, 2008), and the Stanford–Binet Intelligence Scale, Fifth Edition (SB-5; Roid, 2003). In some cases, individuals were deemed untestable after attempting to administer either the WAIS-IV or SB-5. Two individuals were unable to participate in IQ testing due to travel limitations and blindness, respectively, and their IQ classification was considered missing.
Statistical analysis
Descriptive statistics were calculated for demographic variables, IQ scores, and comorbidities and symptoms. Goodness-of-fit tests were used to test for differences in the frequencies of categorical variables. Fisher’s exact tests were used in cases where cell frequencies were less than five. Mann–Whitney U tests were used to test for differences among variables measured on the interval or ratio scale such as psychotropic medication use frequency between participants with and without cardiovascular risk factors (i.e. hypertension, hyperlipidemia, and diabetes). Differences in the frequencies of medication use and hospitalizations were tested across intellectual ability and BMI categories. Differences in the frequencies of medical conditions by BMI category were compared including cardiovascular, GI, neurological, respiratory, endocrine, musculoskeletal, and sleep disturbance. In addition, we explored differences in the mean number of comorbidities by gender, intellectual ability, age, and BMI. Two-tailed hypothesis tests were used with statistical significance assessed at an alpha less than 0.05. As the dataset contained three sets of siblings, a sensitivity analysis was conducted in which all sibling pairs were removed and the analyses described above were repeated. Statistical analyses were run in SPSS Version 21.0 and SAS software version 9.3.
Results
Subject characteristics
Table 3 summarizes the descriptive statistics of the study population. In total, 75% (n = 69) of the participants were male. The median age at follow-up was 36.1 years (range: 23.5–50.5 years). In all, 29% (n = 27) of participants had IQ scores above 70; 24% (n = 22) had mild ID (IQ: 50–69); and 38% (n = 35) were classified as having severe ID (<50).
Subject characteristics among adults (N = 92) identified with ASD in Utah. a

ASD: autism spectrum disorder; SD: standard deviation.
Deceased individuals included.
Mann–Whitney U or Kruskal–Wallis test.
Signifies statistical significance.
The median number of chronic medical conditions for each participant was 11 (range: 0–33). Females had more comorbid conditions than males (median 16 vs 10, p = 0.01, respectively), and the mean number of co-occurring conditions varied by BMI category (p = 0.03) with obesity associated with the highest number of conditions.
Burden of chronic medical conditions
Table 4 displays the frequency of medical conditions and symptoms in our study population, along with medication use, hospitalizations, and major surgeries. GI (59%) and neurological (59%) conditions were the most common, followed by ear, nose, and throat (57%) and sleep disturbances (41%). Constipation was the most common GI complaint, affecting 36% of the total cohort, while 14% reported problems with chronic diarrhea. Seizures were endorsed by 27 (29%) participants at some time in their lives, although most participants could not identify an exact age of onset. No differences were found by intellectual functioning category in regard to frequencies of previous major surgery or hospitalization for life-threatening illness (Table 5).
Frequency of medical conditions, medication use, hospitalizations, and major surgeries among adults (N = 92) identified with ASD in Utah. a

ASD: autism spectrum disorder.
Reported medical conditions, hospitalizations, and surgeries are both historical and current; medications listed are for current use.
Medication information from deceased participants was not used as there is no current medication use.
Many anti-epileptic drugs also have mood stabilization effects.
Serotonin/norepinephrine/dopamine reuptake inhibitors, tricyclic antidepressants, or serotonin receptor binders.
Most common hospitalization for life-threatening conditions include pneumonia (commonly recurrent), status epilepticus and seizure work-up, and severe dehydration from infection.
Most common major surgeries include orthopedic fracture repair, inguinal hernia repair, and urologic reconstructions.

ASD: autism spectrum disorder.
Comparison does not include deceased participants.
Due to the small sample size of those without ID, this analysis is underpowered to detect a true difference.
Chi-square test.
Signifies statistical significance.
Medication use
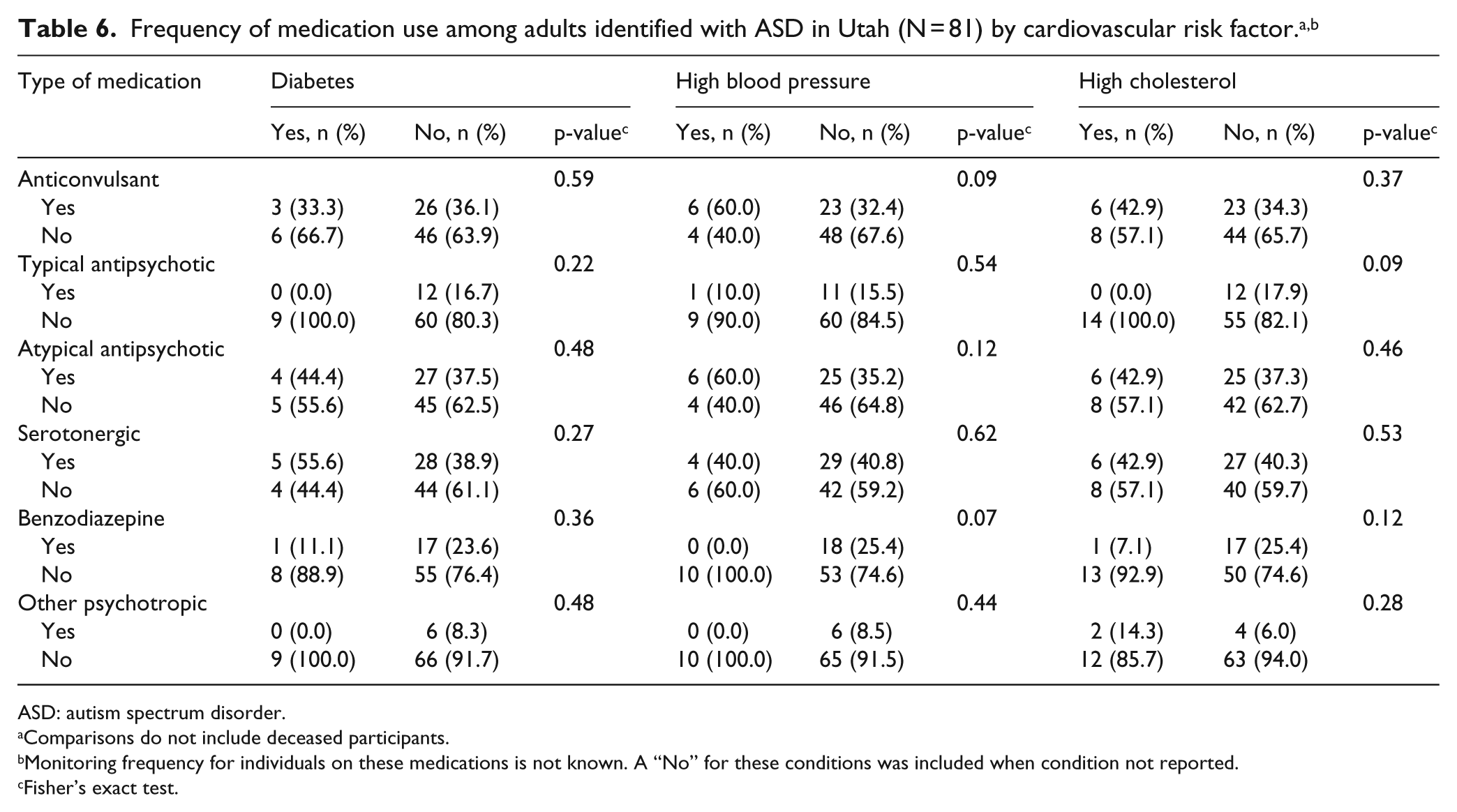
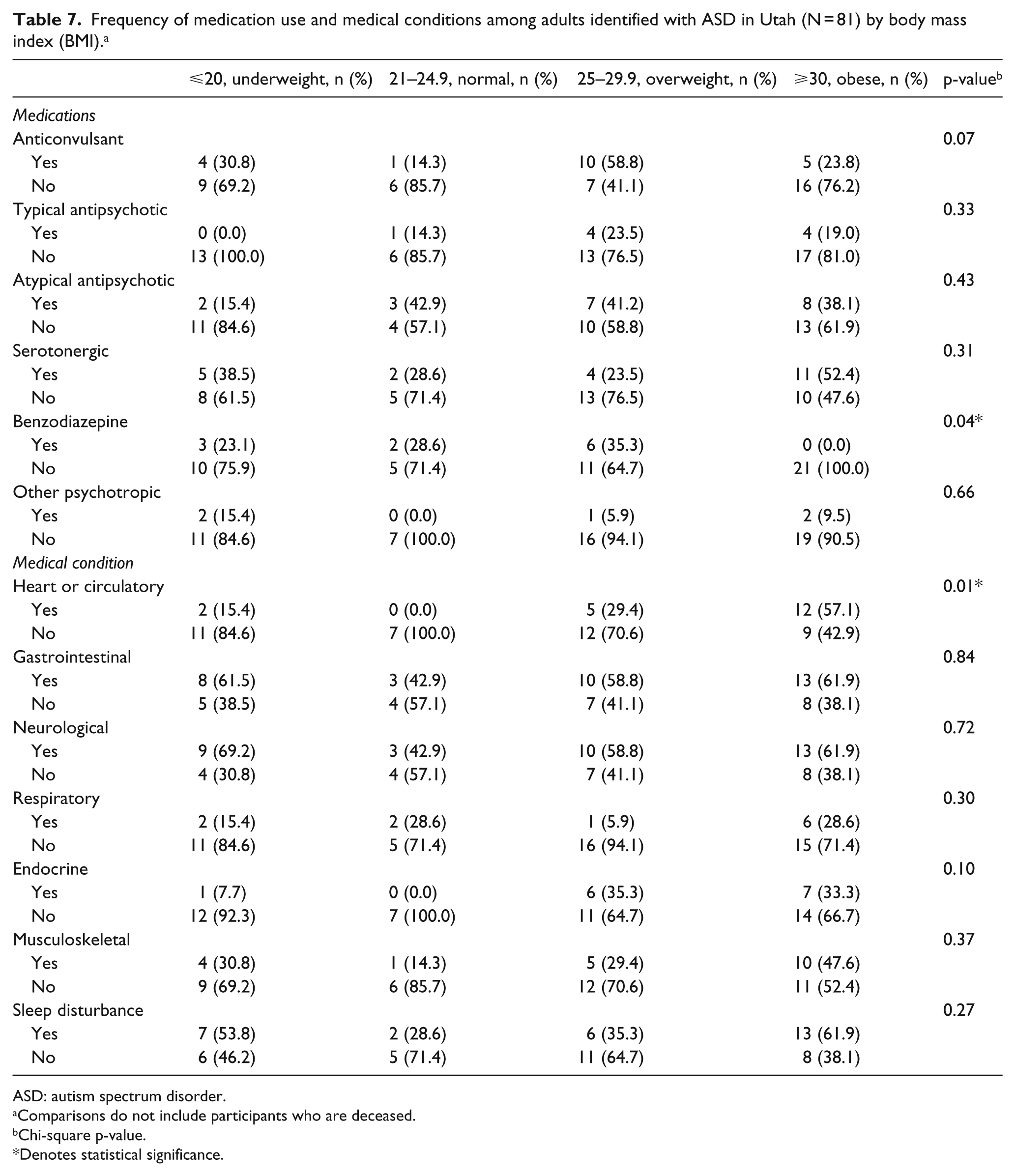
Table 4 describes general medication use by study participants. In all, 15 individuals (18.5%) did not use any medications, while 44 (54.3%) used four or more medications routinely. There were no differences in the frequency of medication use across intellectual abilities, with the exception of higher benzodiazepine use in those with severe ID (p = 0.01, Table 5). There were no statistically significant differences in the frequency of current psychotropic medication use between individuals with and without hypertension, hyperlipidemia, diabetes mellitus, or by BMI category (all p values >0.05, Tables 6 and 7). Finally, the sensitivity analysis showed that results did not change when siblings were removed.
ASD: autism spectrum disorder.
Comparisons do not include deceased participants.
Monitoring frequency for individuals on these medications is not known. A “No” for these conditions was included when condition not reported.
Fisher’s exact test.
Frequency of medication use and medical conditions among adults identified with ASD in Utah (N = 81) by body mass index (BMI). a
ASD: autism spectrum disorder.
Comparisons do not include participants who are deceased.
Chi-square p-value.
Denotes statistical significance.
Medical conditions by BMI
In all, 25 (27%) participants were obese, 17 (18%) were overweight, and 17 (18%) were underweight. Table 7 shows that the frequency of cardiovascular conditions varied by BMI category with 57% of obese individuals experiencing a heart or circulatory condition (=0.01). No differences were detected in the frequencies of other medical conditions including neurological or GI conditions by BMI category.
Discussion
This descriptive study examines medical conditions affecting adults with ASD as part of a population-based, longitudinal follow-up evaluation of individuals in Utah first ascertained in the 1980s. As such, this study represents a unique opportunity to describe the presence of chronic and acute medical problems experienced by a population of adults with ASD in the United States whose symptom severity is on the higher end of the autism spectrum, based on the increased prevalence of ID in this group as compared to national averages. Participants experienced a high frequency of medical conditions, hospitalizations for life-threatening conditions, and major surgeries, indicating a significant medical comorbidity burden faced by adults with ASD. Comorbidity burden was elevated in females and those with obesity, representing two subgroups who have especially high medical needs. This disease burden underscores the importance of ongoing access to primary and preventive care for this population.
Several medical conditions frequently endorsed by participants are also commonly identified in children with ASD, including seizures, GI symptoms, sleep disorders, extremes in BMI, and motor imbalance. This underscores the chronicity of these conditions with persistent elevated risk extending into adulthood for individuals with ASD. Other conditions, such as an elevated rate of asthma in children with ASD, were dramatically reduced in this adult population. The rate of seizures in this cohort (29%) is comparable to the 22%−38% reported in previous studies (Bolton et al., 2011; Danielsson et al., 2005; Giovanardi et al., 2000). Sleep disorders were seen in a smaller portion of participants (41%) than in two previous studies (75%−80%), which may reflect the differences in sample size and symptom query (Oyane and Bjorvatn, 2005; Tani et al., 2003). In all, 59% of participants experienced some form of GI symptom in this study—more than twice the rate of GI symptoms in the general adult US population (22%; National Institutes of Health, US Department of Health and Human Services, 2009), although few previous studies of adults with ASD have addressed this concern.
To our knowledge, only two previous studies identified obesity rates specific to adults with ASD, ranging from 35% to 42% (Eaves and Ho, 2008; Tyler et al., 2011). While the rates of obesity and overweight in this population (27% and 18%, respectively) were lower than those of the general US adult population (35% are obese and 33% are overweight; Flegal et al., 2012), they exceed Utah’s adult obesity rate of 24% (CDC, 2012). These rates may not fully represent this population as BMI information was unavailable in 27% of participants due to barriers of geography and mortality. Psychotropic medication use can increase obesity risk; however, BMI category appeared unaffected by psychotropic medication use in this study. There were also no differences detected in the use of psychotropic medications among individuals with and without cardiovascular risk factors, such as hypertension, hyperlipidemia, or diabetes mellitus. The rate of diabetes mellitus in our sample was similar to that in the general US adult population (10% vs 12%), while hypertension was significantly less common among participants (11%) than in the US adult population (33%; Ford, 2013). The proportion of adults who were underweight in our study (18%) exceeded the adult national average of 2% (Fryar and Ogden, 2012). This is consistent with a recent study that reported a higher frequency of obesity and underweight classes among adolescents with ASD compared to unaffected peers (Phillips et al., 2014). BMI extremes in either direction highlight the need for proper nutrition and physical activity for all individuals with ASD, including frequent medical follow-up to optimize weight and health.
This cohort includes individuals across the range of intellectual functioning meeting DSM-III and/or DSM-IV-TR criteria for ASD; however, the percentage of individuals with ID in this study significantly exceeds that of recent, population-based ASD prevalence studies in children (CDC, 2014). Although participants who met exclusively DSM-IV-TR ASD criteria were included, study participation remained limited to those adults with ASD ascertained as children based on social developmental concerns recognized at that time. Thus, many high-functioning individuals with ASD were likely missed (Buck et al., 2014).
Severe ID has been shown in other studies to be one of many manifestations of neurodevelopmental injury affecting multiple additional organ systems. ID severity was not, however, associated with any other indicators of physical illness, such as number of comorbid medical conditions, polypharmacy, hospitalizations for life-threatening conditions, or history of major surgery. Categories of medical conditions (e.g. seizures, GI complaints, sleep disorders) also did not differ by ID presence or severity. This may be related to a small proportion of individuals without ID as this study is underpowered to detect a difference that may be present in other cohorts of individuals with ID. However, this is the largest sample for a US population-based follow-up study evaluating medical conditions in adults with ASD.
Another study limitation is the absence of medical record information to provide collateral medical history. Caregiver or self-reported data are subject to issues of misunderstanding medical questions and recall bias. The inclusion of lifetime conditions makes their timeframe challenging to determine. However, the inclusion of a systematic and extensive ROS through direct engagement with study participants provided an opportunity to capture a breadth of medical aliments of varying severity not commonly captured through medical or billing records review alone. It is possible that the information obtained had varying accuracy based on who filled out the questionnaire, although the reporter of the information was not documented. Also, the identification of genetic disorders may be underrepresented in this sample as testing for these conditions becomes more sophisticated, widely available, and recommended for initial work-up of individuals with ASD.
The consistency between this study findings and previous ASD studies exploring medical conditions in both children and adults suggests that many medical conditions first experienced in childhood extend into adulthood and require ongoing attention from caregivers and health care providers. While this population-based sample is specific to Utah, the individuals included are a fair representation of the larger ASD population, particularly those with ID, who commonly engage in medical care. These results may assist medical providers in identifying pertinent components of the medical history and ROS for adults with ASD, whether providing preventative health care maintenance or assessing an acute concern.
Footnotes
Funding
This work was supported in part by the National Institute of Mental Health R01 MH094400 and Autism Speaks.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.