
Abstract
Compared to the general pediatric population, children with autism have higher rates of co-occurring medical and psychiatric illnesses, yet very little is known about the general health status of adults with autism. The objective of this study was to describe the frequency of psychiatric and medical conditions among a large, diverse, insured population of adults with autism in the United States. Participants were adult members of Kaiser Permanente Northern California enrolled from 2008 to 2012. Autism spectrum disorder cases (N = 1507) were adults with autism spectrum disorder diagnoses (International Classification of Diseases-9-Clinical Modification codes 299.0, 299.8, 299.9) recorded in medical records on at least two separate occasions. Controls (N = 15,070) were adults without any autism spectrum disorder diagnoses sampled at a 10:1 ratio and frequency matched to cases on sex and age. Adults with autism had significantly increased rates of all major psychiatric disorders including depression, anxiety, bipolar disorder, obsessive–compulsive disorder, schizophrenia, and suicide attempts. Nearly all medical conditions were significantly more common in adults with autism, including immune conditions, gastrointestinal and sleep disorders, seizure, obesity, dyslipidemia, hypertension, and diabetes. Rarer conditions, such as stroke and Parkinson’s disease, were also significantly more common among adults with autism. Future research is needed to understand the social, healthcare access, and biological factors underlying these observations.
Introduction
Autism spectrum disorders (ASDs) are a heterogeneous group of complex neurodevelopmental conditions apparent in early childhood, characterized by persistent deficits in social communication and social interaction and restricted, repetitive patterns of behavior, interests, or activities (APA, 2013). While a small minority of individuals develop sufficient adaptive skills that they no longer meet criteria for an ASD diagnosis, ASDs are generally considered lifelong developmental disabilities (Anderson et al., 2014; Fein et al., 2013). The prevalence of ASD has been rising since the 1980s as the definition has evolved and awareness has increased. The most recent estimate suggests that 1 in 68 children in the United States are on the autism spectrum (CDC, 2014). As the number of children diagnosed with ASD increases, the number of autistic children entering adulthood will continue to rise. To date, however, very little is known about ASD in adults, including their health status and healthcare needs (Mandell, 2013).
Children and adolescents with ASD have been reported to have many medical and psychiatric conditions, including seizure, sleep disorders, gastrointestinal (GI) disorders, metabolic disorders, hormone dysfunction, obesity, nutritional deficits, anxiety, depression, attention deficit hyperactivity disorder (ADHD), and oppositional defiant disorder (Bauman, 2010; Bradley and Bolton, 2006; de Bruin et al., 2007; Ghaziuddin et al., 1998; Joshi et al., 2010; Levy et al., 2010; Leyfer et al., 2006; Schieve et al., 2012; Simonoff et al., 2008). Robust estimates of the rate of medical and psychiatric conditions among adults with ASD are largely lacking from the scientific literature. In the only study to examine the prevalence of co-occurring conditions across multiple organ systems among a large sample of adults with ASD, Kohane et al. reported a higher prevalence of epilepsy, schizophrenia, inflammatory bowel disease, central nervous system (CNS)/cranial anomalies, diabetes mellitus type I, muscular dystrophy, and sleep disorders among autism cases compared to controls (Kohane et al., 2012). Only major conditions shown to be associated with ASD in previous studies were included in the Kohane study, and the study population was restricted to young adults <35 years of age.
The objective of this study was to determine the prevalence of psychiatric and medical conditions, including those not previously associated with ASD, among a large population of adults with ASD of all ages. A better understanding of health status may identify specific targets for intervention and lead to improvements in the delivery of appropriate and effective healthcare and quality of life for this growing population of adults.
Methods
Setting
This study was set within Kaiser Permanente in Northern California (KPNC), the largest and oldest group model pre-paid, integrated healthcare delivery organization in the United States providing healthcare to over 3 million residents (approximately 25%–30%) of the San Francisco and Sacramento metropolitan areas and surrounding counties. KPNC members are broadly representative of the local and statewide population in terms of sociodemographic characteristics, except for the extremes of the income distribution (Krieger, 1992). KPNC membership provides health insurance coverage for inpatient and outpatient medical and mental health services delivered at KPNC clinics and hospitals and approved outside facilities. All patient interactions with the healthcare system are recorded in a comprehensive electronic medical record (EMR) system and summarized in several clinical databases.
Study population
All adults ⩾18 years of age as of January 2008 who were members of KPNC for at least 9 months in each calendar year from January 2008 to December 2012 were eligible for inclusion (N = 1,578,657). Cases (N = 1507) were defined as adults with ASD diagnoses (Autism: International Classification of Diseases-9-Clinical Modification (ICD-9-CM) 299.0; Asperger’s Disorder (ICD-9-CM 299.8), Pervasive Developmental Disorder, Not Otherwise Specified (PDD-NOS) (ICD-9-CM 299.9)) recorded in KPNC EMRs on at least two separate occasions anytime through December 2012.
A comparison population (N = 15,070) was randomly sampled at a 10:1 ratio from among all adult members who did not have any ASD diagnoses recorded in KPNC medical records by December 2012. Controls were frequency matched to cases on sex and 5-year age group.
Medical and psychiatric conditions
Medical and psychiatric conditions documented in KPNC medical records between January 2008 and December 2012 were identified by electronically searching the KPNC outpatient and inpatient clinical databases. The definition of specific conditions was based on algorithms using ICD-9 diagnostic codes (used in assigning diagnostic and procedure codes associated with inpatient, outpatient, and physician office utilization in the United States), laboratory results and medication reports previously validated for KPNC data, or groupings of ICD-9 codes used by phenotype-wide association studies (PheWAS; Denny et al., 2010; see Supplementary Table 1 for definitions of each condition). Diabetes and cancer diagnoses were considered present if the study participant was included in the KPNC diabetes or cancer registries, respectively, by 31 December 2012. The KPNC diabetes registry was established in 1993 and is updated annually by searching multiple clinical data sources including pharmacy, laboratory, hospitalization, and outpatient records to identify patients with diabetes (Karter et al., 2002). The KPNC cancer registry was established in 1994 and collects data on all cases of invasive and in situ cancer, except non-melanoma skin cancer, diagnosed in KPNC members since 1947. Obesity (body mass index (BMI) ⩾ 30) was defined by the average BMI recorded in medical records in the 5-year study period.
Statistical analysis
The prevalence of each specific medical and psychiatric condition was compared between ASD cases and controls using chi-square tests. Comparisons with p values less than 0.01 were considered statistically significant. A separate multivariate logistic regression model was run for each condition to compare the odds of the condition between ASD cases and controls after controlling for sex, age, and race/ethnicity. Only conditions for which at least 14 cases were diagnosed are shown in tables. All study procedures were approved by the KPNC Institutional Review Board.
Results
Among the 1507 adult patients identified with ASD, 37.2% had a diagnosis of autistic disorder, 29.7% Asperger’s syndrome, 30.7% PDD-NOS, and for the remaining 2.3% the specific ASD diagnosis could not be determined. Approximately one-fifth (19.2%) of adults with ASD also had a diagnosis of intellectual disability (12.8% mild, 3.1% moderate, 6.2% severe, 77.9% level not specified). Intellectual disability is a condition for which patients in our system are not routinely tested or receive treatment. Demographic characteristics of the study sample are shown in Table 1. The mean age of the study population was 29 years (standard deviation 12 years). Approximately half (52%) were between 18 and 24 years, and 9.5% were 50 years or older. The overall male/female ratio was 2.7. Adults with ASD were more likely to be White, non-Hispanic and less likely to be Asian than controls. The mean length of membership in KPNC since 1980 was 21.5 years for cases and 16.7 years for controls. Healthcare expenses were covered by Medicaid for 24.9% of the case group but only 1.3% of controls.
Characteristic of study population: adults 18 years and older from the Kaiser Permanente Medical Care Program in Northern California.

ASD: autism spectrum disorder; SD: standard deviation; KP: Kaiser Permanente.
Psychiatric conditions
More than half (54%) of adults with ASD were diagnosed with a psychiatric condition—29% diagnosed with anxiety, 11% with bipolar disorder, 26% with depression, 8% with obsessive–compulsive disorder (OCD), 8% with schizophrenia (Table 2). After adjusting for sex, age, and race/ethnicity, the risk of most psychiatric conditions was significantly elevated in adults with ASD—from 2.9-times higher for depression to 22-times higher for schizophrenia—compared to controls (Table 2). The risk of suicide attempts was fivefold higher in adults with ASD compared to unaffected controls. While the rate of suicide attempt was higher among adults with ASD with a diagnosis of depression (3.6%) compared to adults with ASD without a diagnosis of depression (1.2%), only 14/27 adults with ASD who attempted suicide had a diagnosis of depression. By contrast, adults with ASD were significantly less likely to be diagnosed with alcohol abuse/dependency (Table 2) and to self-report alcohol use (17.8% vs 55.3%) and tobacco use (11.9% vs 28.9%).
Prevalence of psychiatric conditions in adults with ASD and controls.
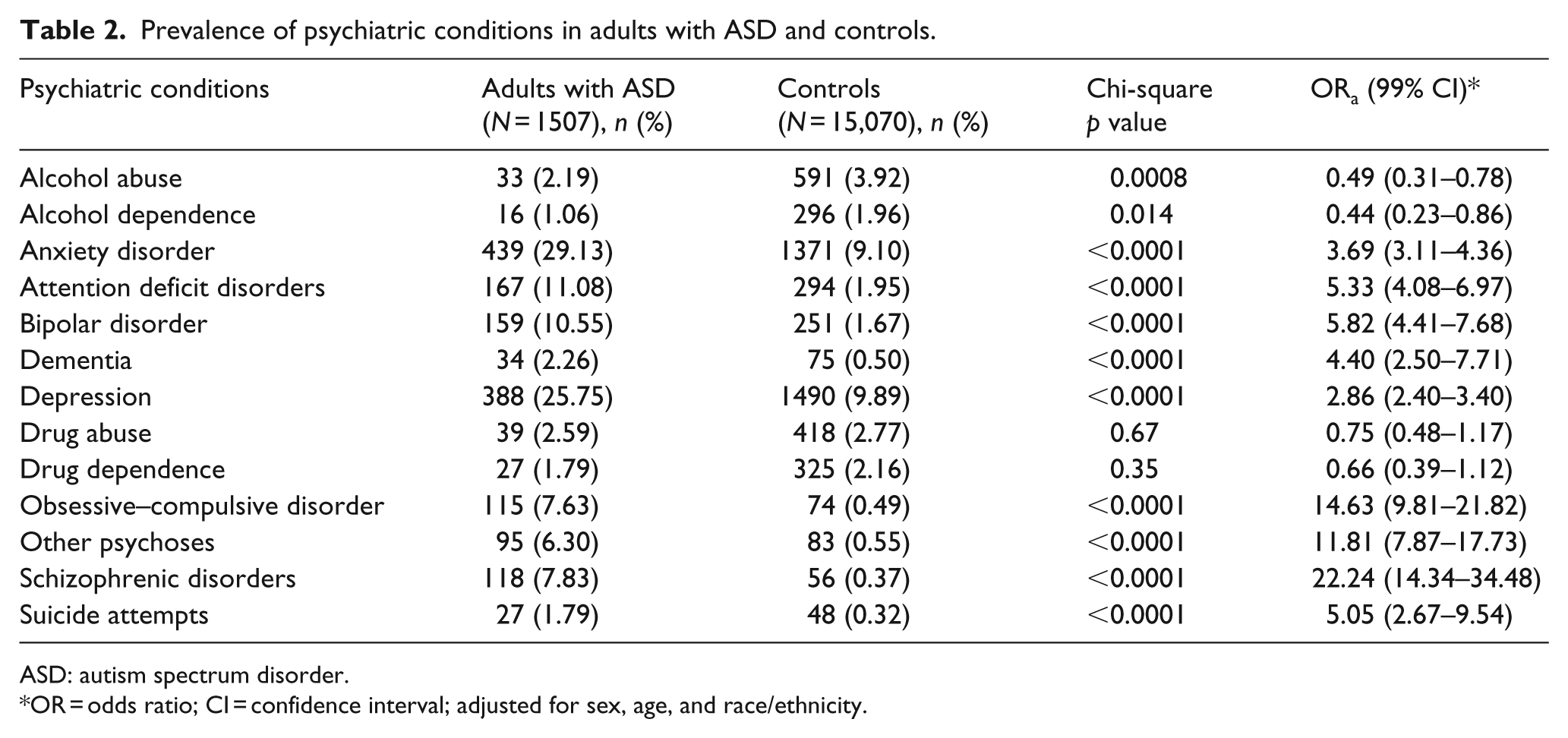
ASD: autism spectrum disorder.
OR = odds ratio; CI = confidence interval; adjusted for sex, age, and race/ethnicity.
Women with ASD were diagnosed more often than men with anxiety (36.3% vs 26.5%), bipolar disorder (13.8% vs 9.3%), dementia (3.2% vs 1.9%), depression (34.1% vs 22.7%), schizophrenic disorders (10.4% vs 6.9%), and suicide attempts (2.7% vs 1.45%), but less often with OCD (6.2% vs 8.2%), attention deficit disorder (8.6% vs 12.0%), alcohol abuse (0.74% vs 2.7%), drug abuse (1.74% vs 2.9%), and drug dependence (1.0% vs 2.1%). Both men and women had increased risks of most psychiatric conditions compared to sex-matched unaffected controls (Table 3). However, compared to sex-matched unaffected controls, risks were much higher among women than men with ASD for dementia, other psychoses, and schizophrenic disorders, and risk was much higher for men than women with ASD for OCD (Table 3).
Variation in prevalence of psychiatric conditions among adults with ASD by gender.
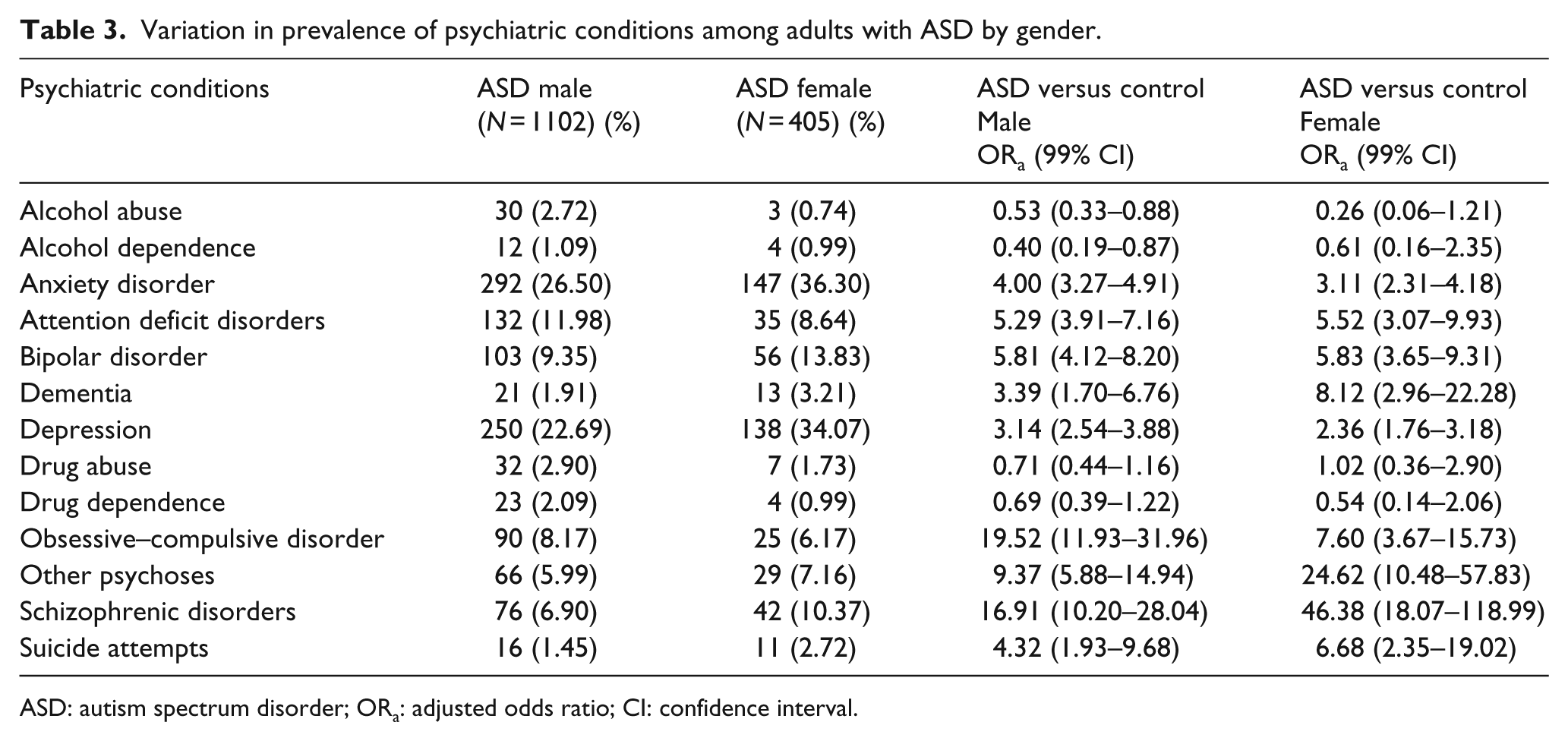
ASD: autism spectrum disorder; ORa: adjusted odds ratio; CI: confidence interval.
Medical conditions
Nearly all major chronic medical conditions were significantly more common in adults with ASD than controls (Table 4). These included conditions previously associated with ASD in children, such as autoimmune conditions (13.9% among ASD vs 10.8% among controls), allergy (36.3% vs 28.7%), GI disorders (34.7% vs 27.5%), sleep disorders (17.6% vs 9.6%), and seizure (11.9% vs 0.73%). In addition, adults with ASD had significantly higher prevalence of common chronic medical conditions, including dyslipidemia (22.8% vs 15.1%), hypertension (25.6% vs 15.6%), diabetes (7.6% vs 4.3%), obesity (33.9% vs 27.0%), and thyroid disease (7.0% vs 3.1%). Rarer conditions, such as stroke, Parkinson’s disease, vitamin deficiency, vision and hearing impairments, and genetic disorders were also significantly more common among adults with ASD than controls (Table 4). Interestingly, only a few conditions were diagnosed less often among adults with ASD; these included infections and genitourinary disorders (Table 4).
Prevalence of medical conditions among adults with ASD and controls.

CVD: cardiovascular disease; ASD: autism spectrum disorder; CNS: central nervous system; GERD: gastroesophageal reflux disease; GI: gastrointestine.
OR = odds ratio; CI = confidence interval; adjusted for sex, age, and race/ethnicity.
Most medical conditions were diagnosed more frequently among females with ASD compared to males with ASD (Table 5). However, both men and women had increased risks of most conditions compared to unaffected controls, except for autoimmune diseases and GI disorders, which were significantly elevated only among men with ASD, and stroke, which was significantly elevated only among women with ASD (Table 5).
Variation in prevalence of medical conditions among adults with ASD by gender.
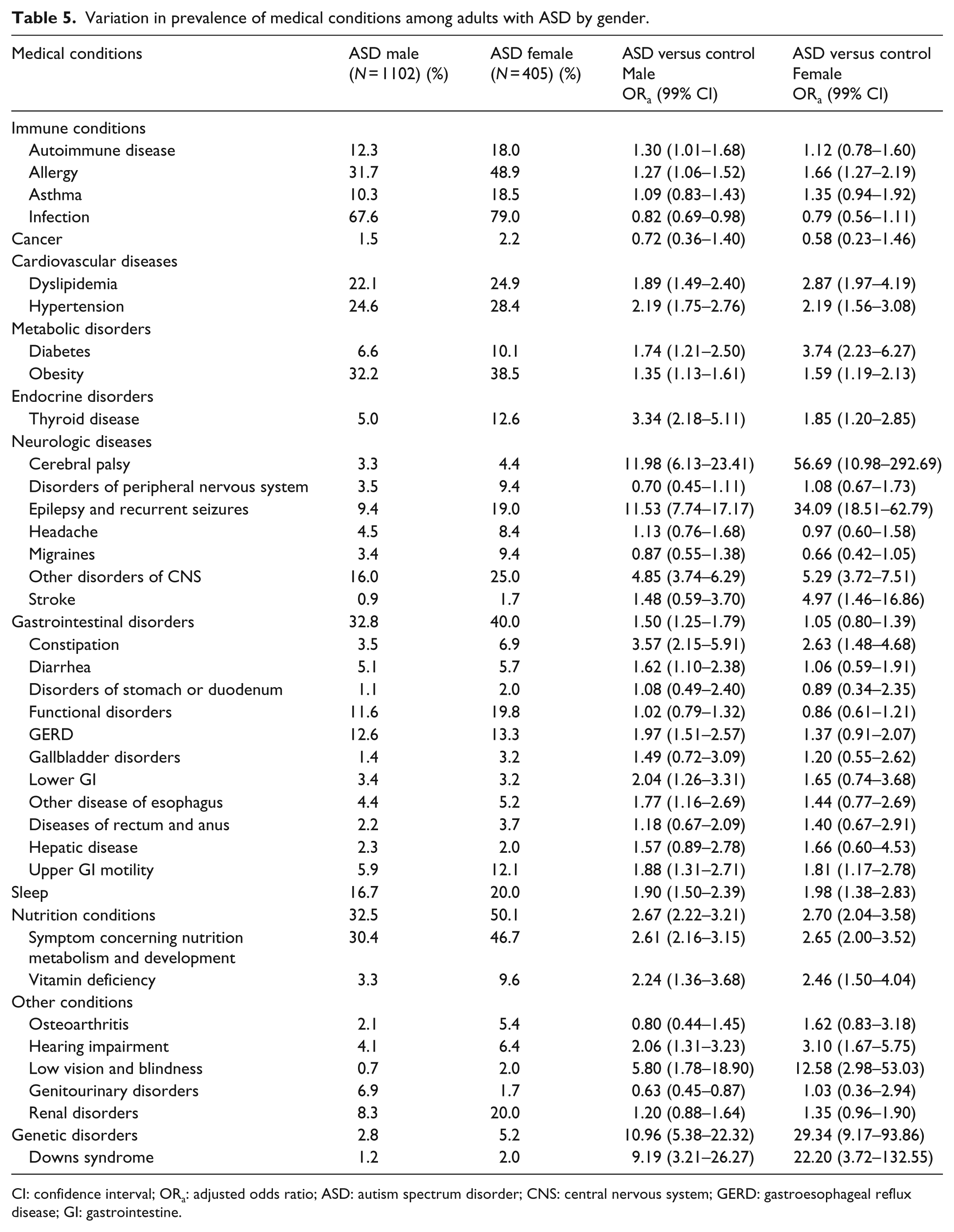
CI: confidence interval; ORa: adjusted odds ratio; ASD: autism spectrum disorder; CNS: central nervous system; GERD: gastroesophageal reflux disease; GI: gastrointestine.
Discussion
In a large and diverse population of adults insured within the same integrated health delivery system, the rates of most major psychiatric and chronic medical conditions were high among adults with ASD and significantly elevated compared to controls. These included conditions previously reported to be elevated in children and adolescents with ASD and conditions which generally have onset in adulthood. The exceptions were alcohol abuse/dependency, infections, and genitourinary disorders, which were diagnosed less often among adults with ASD than controls. In general, gender differences in the prevalence of psychiatric and medical disorders observed in the ASD group mirrored differences in the general population, resulting in similarly elevated risks for men and women with ASD compared to controls.
Our findings of high prevalence of psychiatric disorders, including depression, anxiety, psychoses, OCD, bipolar disorder, and attention deficit disorder, are consistent with previous studies which typically included fewer than 200 cases and focused on young adults (Buck et al., 2014; Eaves and Ho, 2008; Gillott and Standen, 2007; Hofvander et al., 2009; Joshi et al., 2013; Kanne et al., 2009; Lugnegard et al., 2011; Morgan et al., 2002; Russell et al., 2005; Sterling et al., 2008; Vannucchi et al., 2014). As in the study by Kohane et al. (2012), schizophrenia was diagnosed significantly more often in adults with ASD in our study population, especially among women. An association between autism and schizophrenia has been suggested in a few other studies in adult populations (Daniels et al., 2008; Mouridsen et al., 2008; Sprong et al., 2008; Stahlberg et al., 2004).
Of particular concern is the fivefold higher rate of diagnosed suicide attempts we observed among adults with ASD compared to controls. Nearly half of the adults with ASD with a diagnosis of attempted suicide did not also have a diagnosis of depression, suggesting that depression may be underdiagnosed in the autistic population, resulting in lack of needed treatment. Our findings are consistent with the few previously published studies of suicidal ideation and attempt among small clinical samples of individuals with ASD (Cassidy et al., 2014; Mayes et al., 2013; Paquette-Smith et al., 2014; Raja et al., 2011; Storch et al., 2013), which reported rates in the range of 11%–40%. The rate in our study (1.8%) was substantially lower, likely because it reflected suicide attempts only (not ideation) in a 5-year period, and not lifetime experiences.
In terms of medical conditions, two prior studies compared rates of several conditions between adults with and without ASD using data stored in EMRs. Similar to our findings, Tyler et al. (2011) reported significantly elevated rates of hyperlipidemia, epilepsy, and constipation among 108 autistic adults (average age 29 years) receiving primary care through the Cleveland Clinic in 2005–2008 compared to age, sex, race, and insurance status matched controls. Kohane et al. (2012) studied adults aged 18–34 years receiving care in three general hospitals and reported higher rates of epilepsy, bowel disorders, diabetes, and sleep disorders in adults with ASD compared to unaffected controls.
Children and adolescents with autism have also been found to have higher rates of overweight and obesity than population controls (Broder-Fingert et al., 2014; Curtin et al., 2010). Obesity increases the risk of many chronic diseases including diabetes, cardiovascular disease, and cancer (Guh et al., 2009), and in our study population, adults with ASD did have elevated rates of diabetes, hypertension, and dyslipidemia, but marginally lower rates of cancer. A recent review of the genetic and developmental bases of autism in relation to genes and pathways associated with cancer risk concluded that cancer risk may be altered in autism (Crespi, 2011). Further epidemiologic research in large populations is needed to elucidate the association between autism and chronic conditions including cancer and identify explanatory factors for our observed associations.
There are several possible explanations for our observations of increased rates of psychiatric and medical conditions among adults with ASD. First, the communication and social impairments and deficits in sensory processing that define core features of ASD may prevent individuals from accessing preventive healthcare, or accurately reporting pain or localizing discomfort, leading to missed or delayed diagnoses and opportunities for prevention or early treatment. Tactile sensitivities may interfere with routine medical exams, further leading to delayed diagnosis and treatment of medical conditions (Bauman, 2010). Social isolation, discrimination, and difficulties with communication may lead to psychiatric disorders such as anxiety and depression. In an Internet survey of 209 autistic adults and 228 adults with other disabilities, adults with ASD reported poorer doctor–patient communication, lower scores on general healthcare and chronic condition self-efficacy, and significantly higher levels of unmet healthcare needs related to physical and mental health and prescription medications, and they were less likely to have received preventive healthcare (Nicolaidis et al., 2013).
Second, the core impairments in autism and lack of health education, supports, and accommodations may result in lifestyle factors that are known risk factors for many psychiatric and medical conditions. For example, sensory sensitivities could lead to a limited diet with poor nutritional value (Kral et al., 2013). Lack of accommodation for social and language impairments can create barriers to participating in organized sports and physical activity (Pan and Frey, 2006). Poor, restricted diets and lack of exercise are risk factors for obesity, which in turn is associated with increased risk of many major chronic conditions (Guh et al., 2009). Interestingly, smoking and alcohol use, social behaviors known to increase risk of chronic medical conditions (Ezzati and Riboli, 2013), were significantly less often reported by adults with ASD than controls.
Third, ASD and other psychiatric and medical conditions may share similar genetic factors. For example, a recent study of genome-wide single-nucleotide polymorphism (SNP) data in over 60,000 individuals in the Psychiatric Genomics Consortium identified specific variants in calcium-channel activity genes which were shared between ASD, ADHD, bipolar disorder, major depressive disorder, and schizophrenia (Cross-Disorder Group of the Psychiatric Genomics Consortium, 2013).
Fourth, medications used to treat psychiatric and neurologic comorbidities may raise the risk of other conditions. For example, obesity and hyperlipidemia may be a consequence of the cardiometabolic risks associated with psychoactive medications (Correll, 2009) which are commonly used in adults with autism (Buck et al., 2014). Antipsychotics use in autistic children has been associated with significantly increased weight gain compared to placebo controls (McCracken et al., 2002; Shea et al., 2004). Antiepileptics have been associated with osteoporosis (Srikanth et al., 2011) and sleep problems (Van de Wouw et al., 2012) both of which were observed to be elevated in the autistic population.
Several study limitations deserve mention. ASD status and presence of psychiatric and medical conditions were determined by diagnoses recorded in EMRs and were not validated by standardized clinical exam. While the validity of electronic health record data in primary care has been found to be good overall (Thiru et al., 2003), diagnoses of some chronic conditions are less reliable when not linked to medications or procedures (Tyler et al., 2011). Grouping of ICD-9 codes into phenotypic categories may have resulted in misclassification. Only 21% of our study population had a recorded diagnosis of intellectual disability. Given that intellectual disability is a condition for which patients in our system are not routinely tested or receive treatment, it is likely that the diagnosis is under-reported in our medical records.
This study had several strengths. The large, ethnically diverse study population was representative of an insured population, and also included a significant percentage of patients who received healthcare through government health insurance (Medicaid). This is the first study to include adults of all ages across the full range of intellectual functioning. Information on psychiatric and medical conditions were derived from comprehensive data collected prospectively and recorded by healthcare providers in EMRs, which avoided biases due to self- or care-giver report. Cases and controls were matched on length of enrollment in the same health plan during the most recent 5-year period, and all had at least 9 months of membership in each study year. Thus, our data captured the vast majority of healthcare encounters occurring for this population. Finally, the large size of the study enabled us to address low-prevalence conditions.
Conclusion
In this large, insured population, we see significantly increased rates of medical and psychiatric conditions among adults with ASD. These findings indicate an urgent need for the development of improved strategies for delivering effective health education and healthcare to this growing population (Nicolaidis et al., 2014). A better understanding of the possible mechanisms leading to poorer health status will enable improved patient care and ultimately enhance the quality of life for adults on the autism spectrum.
Footnotes
Acknowledgements
We thank the members of the KPNC ASD in Adults Workgroup for their valuable insights and generous input regarding study design, data analysis, and interpretation of study results. No compensation was received for these contributions. The members include Stephen Rich, MD, Scott Rich, MA, Opal Thornton, MD, Clarissa Kripke, MD, Agnes Amistoso, MA, Elizabeth Dixon, LCSW, Chuck Trumble, MFT, Stephen Sidney, MD, Ousseny Zerbo, PhD, Maria Massolo, PhD, Carmen Ancinas-Gee, MFT and Neeraja Maramreddy, MD.
Funding
This study was funded by a grant from the Special Hope Foundation, who had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.