
Abstract
Autism spectrum disorder diagnoses sometimes change due to misdiagnosis, maturation, or treatment. This study uses a probability-based national survey—the Survey of Pathways to Diagnosis and Services—to compare currently diagnosed (n = 1420) and previously diagnosed (n = 187) children aged 6–17 years based on retrospective parental reports of early concerns about their children’s development, responses to those concerns by doctors and other healthcare providers, the type of provider who made the first autism spectrum disorder diagnosis, and the autism spectrum disorder subtype diagnoses received (if any). Propensity score matching was used to control for differences between the groups on children’s current level of functioning and other current characteristics that may have been related to diagnosis loss. Approximately 13% of the children ever diagnosed with autism spectrum disorder were estimated to have lost the diagnosis, and parents of 74% of them believed it was changed due to new information. Previously diagnosed children were less likely to have parents with early concerns about verbal skills, nonverbal communication, learning, and unusual gestures or movements. They were also less likely to have been referred to and diagnosed by a specialist. Previously diagnosed children were less likely to have ever received a diagnosis of Asperger’s disorder or autistic disorder.
Introduction
Autism spectrum disorders (ASDs) are a set of neurodevelopmental disorders that are characterized by functional impairments in a child’s social interaction and communication, as well as the presence of restricted repetitive behavior problems. For the most part, ASDs are considered to be chronic and permanent conditions (Charman et al., 2005). There is, however, notable variability in symptomatology and functioning over a lifetime (Fountain et al., 2012; Hedvall et al., 2014), with recent research identifying a group of children who improve substantially and obtain social and communicative functioning that is within the normal limits of typically developing children (Fein et al., 2013). These children who achieve a normal range of cognitive, adaptive, and social skills are considered to have achieved an “optimal outcome” (Fein et al., 2013). Given their level of functioning, their clinical presentation may no longer be consistent with ASD; parents and doctors may say that these children have lost the diagnosis.
Early and intensive therapy is one mechanism by which a child may be able to achieve optimal outcome and lose his or her ASD diagnosis (Fein et al., 2013), but treatment effects alone are unlikely to account for the substantial number of children who appear to have lost the diagnosis in recent studies. For example, in longitudinal studies of small clinic-based samples of children diagnosed with ASD at 2 years of age, 18% (Sutera et al., 2007) and 37% (Turner and Stone, 2007) of the children did not show signs of autism 2 years later. A review of earlier studies with long-term outcomes suggests that between 3% and 25% of children with an ASD diagnosis eventually lose their diagnosis (Helt et al., 2008). Moreover, a nationally representative telephone survey based on parent report revealed that among children aged 3–17 years who reportedly had been previously diagnosed with ASD by a healthcare professional, 38% did not have the diagnosis at the time of the survey (Kogan et al., 2009).
Other mechanisms by which a child can lose the diagnosis have been suggested. Children may be initially misdiagnosed (e.g. Angkustsiri et al., 2014; Williams et al., 2001), perhaps because of difficulties differentiating young children with ASD from children with other health conditions and other developmental delays (Ohta et al., 1987; Siegel et al., 1988). There is the additional possibility that a new diagnostic picture may emerge as the child matures (e.g. Fein et al., 2005; Zappella, 2002) or a child may receive an ASD diagnosis as a placeholder in order to receive necessary services, and the diagnosis is later changed or removed when no longer needed (Daniels et al., 2011; Hyman, 2013).
Several studies have identified children who are most likely to lose their ASD diagnosis, including children with higher IQs (>70), early communication and language abilities (Luyster et al., 2007), and those who have received earlier and more extensive interventions (e.g. Lovaas, 1987; Orinstein et al., 2014). There has also been considerable attention paid to the ASD subtype diagnosis initially received by the child, with children diagnosed with pervasive developmental disorder—not otherwise specified (PDD-NOS) (Rondeau et al., 2011; Soke et al., 2011) and Asperger’s disorder (Cederlund et al., 2008) being more likely to move off the spectrum than children diagnosed with autistic disorder.
This study further explores who is more likely to lose their ASD diagnosis and why, and it is the first to use parent-reported data from a probability-based national survey for these purposes. The majority of studies dedicated to this topic have relied on small, clinical samples in specific geographic regions that may not be representative of children with ASD across the United States. This study explores these questions in the largest national sample to date, and it explores questions of lost diagnoses in greater detail. This includes an examination of retrospective parental reports about the characteristics of their children around the time of the initial ASD diagnosis, how the initial diagnosis of ASD was obtained, and who provided the initial diagnosis, to determine whether these items predict future loss of ASD diagnosis in statistical models that control for current functioning and ASD symptomatology. The study is also the first to describe parents’ perceptions of the reasons their children lost an ASD diagnosis.
Methods
Data source
Data come from the 2011 Survey of Pathways to Diagnosis and Services (referred to as Pathways hereafter), a national survey about school-aged (6–17 years) children with special healthcare needs (CSHCN) who had ever been diagnosed with an ASD, intellectual disability, or a developmental delay. Pathways was sponsored by the National Institute of Mental Health (NIMH) of the National Institutes of Health (NIH) and was administered as a follow-up survey to the 2009–2010 National Survey of Children with Special Health Care Needs (NS-CSHCN), a population-based random-digit-dial survey about CSHCN. Both Pathways and the NS-CSHCN were conducted by the Centers for Disease Control and Prevention’s National Center for Health Statistics (NCHS) as modules of the State and Local Area Integrated Telephone Survey (SLAITS).
The primary goal of Pathways was to better understand the path to diagnosis for children with developmental disabilities and the experiences of parents and children seeking and receiving related services. Parents or guardians of CSHCN who reported in the 2009–2010 NS-CSHCN that their children had ever been diagnosed with one of the three eligible conditions were re-contacted for a follow-up telephone interview and then an additional mailed questionnaire. Of those with eligible CSHCN, 71% were successfully re-contacted, 87% of them agreed to participate in the telephone interview, and 75% of them returned the mailed questionnaire. Despite the high completion rates, the overall Pathways response rate (16%) was low due to the initial 26% response rate of the NS-CSHCN.
More information about both Pathways and the NS-CSHCN can be found at http://www.cdc.gov/nchs/slaits.htm. The NCHS Research Ethics Review Board and the federal Office of Management and Budget (PRA#0920-0406) approved all data collection procedures.
Measures
Diagnostic criteria
At the time of the Pathways survey, parents were asked to confirm that they had been told by a “doctor or other health care provider” that their child ever had “autism, Asperger’s disorder, pervasive developmental disorder, or [an]other autism spectrum disorder” as was indicated when they completed the NS-CSHCN interview. Of the 1766 parents re-contacted, 1638 (93%) confirmed the previous information and were asked additional questions about the child’s ASD.
During the Pathways interview, these parents were asked the following question: “To the best of your knowledge, does [your child] currently have autism or ASD?” From hereafter, CSHCN currently diagnosed with ASD will be referred to as “currently diagnosed children” while CSHCN who had previously been diagnosed with an ASD but no longer had a current diagnosis (based on parent report) will be referred to as “previously diagnosed children.” The full sample for this study included 1420 currently diagnosed children and 187 previously diagnosed children. Data for the 31 children whose parents did not know or refused to say whether the child currently had ASD were excluded from further analysis.
Parents of children ever diagnosed with ASD were also asked whether “a doctor, health care provider, or school professional ever told you that [your child] did not have autism or ASD” and whether that professional told the parent that the child “had some other developmental, learning, emotional, or mental health condition.” If the parent confirmed this was the case, the parent was asked, “What conditions were you told that [your child] had?” Responses to these questions were examined for previously diagnosed children, but were not used to classify children as previously diagnosed.
Additional questions enquired about ASD subtypes, “Did the doctors, health care providers, or school professionals ever tell you that [your child] had any of the following autism spectrum disorders,” which included “Asperger’s disorder,” “pervasive developmental disorder,” or “autistic disorder.” Parents could endorse multiple diagnoses, but children whose parents did not endorse any were labeled as having no ASD subtype. Parents were also asked about co-occurring psychiatric conditions (“intellectual disability or mental retardation,” “depression,” “anxiety problems,” “attention-deficit disorder or attention-deficit/hyperactivity disorder (ADHD),” or “behavioral or conduct problems”), which were first identified in the NS-CSHCN as having been diagnosed by a doctor or other healthcare provider and then in Pathways were determined to be current to the best of the parent’s knowledge.
Type of first concern
Parents were informed that “there are many reasons why a parent might be concerned about their child’s development” and were asked whether they were concerned about 17 different behaviors, problems, or delayed milestones when they “first wondered if there might be something not quite right with [his/her] development.” To reduce the scope of the analyses, like concerns were grouped by the authors into seven categories including verbal communication, medical problems, nonverbal communication, motor problems, behavioral difficulties, learning and understanding difficulties, and the presence of unusual gestures or movements.
Parent report of provider response
After a parent indicated that they had sought out professional help concerning their child’s development, parents were asked “how did that doctor or health care provider respond to your concern?” Responses included “conducted developmental tests,” “made a referral to a specialist,” “suggested that you discuss the concern with the school,” “said nothing was wrong, the behavior was normal,” “said it was too early to tell if anything was wrong,” and “said that your child ‘might grow out of it’.”
Diagnosing provider
Parents were asked “What type of doctor or other health care provider first told you that [your child] had autism or ASD?” The responses were subsequently grouped by the authors into four categories: (1) medical provider—generalist, which included pediatricians or generalists (e.g. family practice or general practice); (2) medical provider—specialist, which included developmental specialists; (3) mental health provider, which included non-school psychologists, psychiatrists, and neurologists; and (4) school/other provider, which included school psychologists, team of professionals, school nurses, and physical, occupational, or speech therapists.
Ages of first parental worry, first reported concern, ASD diagnosis, and first services
Parents reported how old their child was when they “first wondered if there might be something not quite right with [his/her] development,” “first talked to a doctor or other health care provider about their concerns” about their child’s development, and when a doctor or healthcare provider first told them their child had ASD. Parents were also asked at what age(s) their child began receiving specific services to meet his or her developmental needs. The services initiated when the child was the youngest were considered their first service. Services included the use of physical therapy, social skills training, occupational therapy, speech or language therapy, behavioral intervention or modification services, sensory integration therapy, and cognitive-based therapy. These services could occur before the child received a formal ASD diagnosis and may have been for symptoms unrelated to the child’s ASD. Parents had the opportunity to report age in either years or months if the age was before the child’s third birthday, but only in years if the child was 3 years old or older. To accommodate this varying response specificity when calculating means, an age that was reported in years was converted to an age in the middle of that year (e.g. 5 years of age was converted to 5.5 years); this minimizes bias because ages for children who recently had a birthday are rounded up whereas ages for children who were close to their next birthday are rounded down.
Demographics
Child demographics included child’s age, sex, race/ethnicity, health insurance coverage type (at the time of the NS-CSHCN interview), and whether the child had younger or older biological siblings. Household characteristics included income (recoded as a percentage of the federal poverty level (U.S. Department of Health and Human Services, 2011)), educational attainment of the highest educated caregiver, and family structure (two biological, adoptive, or step-parents vs all other family structures).
Child functioning
Parents were asked whether their child is able to “go to the bathroom by [himself/herself],” “feed [himself/herself],” “dress [himself/herself],” and “ask for things [he/she] needs or wants,” with responses grouped into “can do independently” or “can do with help” versus “cannot do.” The Children’s Social Behavior Questionnaire (CSBQ) captured the child’s current level of autism symptomatology. The CSBQ is a 49-item instrument developed to determine the presence and severity of social or behavior problems within the autism spectrum (Hartman et al., 2006). Parents were asked how frequently during the past month their child had engaged in specific behaviors with the possible responses of “does not apply or occur,” “somewhat or sometimes applies,” or “clearly or often applies.” The CSBQ was validated in the Netherlands with outpatient samples of children with various emotional, behavioral, and developmental psychiatric problems, along with mentally retarded and typically developing children recruited from elementary schools (Hartman et al., 2006). It has high internal consistency, inter-rater reliability, and test–retest reliability (Hartman et al., 2008). With the developer’s assistance, the CSBQ was modified slightly for administration in the United States. A single-factor solution with adequate fit was generated using all items of the CSBQ and higher scores on this factor indicated a greater overall level of autism symptomatology. The CSBQ factor score is the only measure captured from the mailed questionnaire portion of Pathways.
Reasons for lost diagnosis
Parents who indicated that their child no longer had a current ASD diagnosis were asked a series of questions pertaining to the reasons their child may have lost his or her diagnosis. These included “treatment helped the condition go away,” “the condition seemed to go away on its own,” “the behaviors or symptoms changed,” “a doctor or health care provider changed the diagnosis,” “with more information, the diagnosis was changed,” “the diagnosis was given so that [your child] could receive needed services,” or “you disagree with the doctor or other health care provider about his or her opinion that [your child] had ASD.” Parents could endorse multiple reasons and also had the opportunity to list other reasons his or her child had lost their diagnosis.
Statistical analysis
All estimates were calculated using Stata 12.1 (StataCorp, 2011), which accounted for the complex survey design and the population weights. First, differences in demographics, current functioning, other current diagnoses, and ages of diagnosis-related events were explored in the full sample between children previously diagnosed with ASD and those currently diagnosed with ASD using corrected χ2 that accounted for the survey design (presented as F-values) or t-tests. Parents’ perceptions of the reasons for a lost diagnosis were then explored among the population of children previously diagnosed.
The next analyses considered differences between previously diagnosed and currently diagnosed children in the characteristics of the children around the time of the initial diagnosis and in how the initial diagnosis was obtained. To maximize statistical power, we wanted to match previously diagnosed and currently diagnosed children on demographics, current autism symptomatology, functional limitations, and psychiatric comorbidities and then look for differences between the matched pairs. Because of the limited size of the pool of possible matches and the many matching variables, propensity score matching (PSM) was used to control for these differences between children previously diagnosed and those currently diagnosed. Conceptually, PSM is a statistical attempt to replicate a randomized controlled trial—with the only difference being some children had lost their ASD diagnosis while others were still currently diagnosed—despite using observational and cross-sectional data (Stuart, 2010). The propensity score itself was the probability that a given child had been previously diagnosed with an ASD but no longer carried the diagnosis, which was estimated through a logistic regression adjusting for covariates that would predict the likelihood a child lost their diagnosis.
Propensity scores were calculated using the MatchIt package (Ho et al., 2011) in R with the optimal command in a 2:1 match. This command created matched pairs with the smallest distance between individuals in order to minimize bias (Austin, 2011). The covariates included in the generation of propensity scores were child characteristics such as age, race/ethnicity, health insurance coverage type, number and type of siblings, ASD symptoms, current co-occurring diagnoses (intellectual disability, ADHD, depression, anxiety problems, conduct/behavioral problems, developmental delay), and functional abilities, as well as household characteristics (highest education level, poverty level, family structure, parents’ ages). Missing data for household income, caregiver education, children’s race/ethnicity, and mothers’ and fathers’ age were multiply imputed and provided by NCHS (Centers for Disease Control and Prevention (CDC), National Center for Health Statistics, State and Local Area Integrated Telephone Survey, 2012).
Children selected for PSM were those with parents who completed the mailed questionnaire that included the CSBQ (n = 1105). The subset sample included 129 previously diagnosed children. The final matched sample consisted of 372 children: 124 had previously been diagnosed with an ASD and 248 had a current ASD diagnosis. Missing data on remaining covariates (those for which imputations were not available) prevented five previously diagnosed children from being matched.
Propensity scores and matches were exported to Stata 12.1 for analysis, which accounted for the complex survey data and population weights. Logistic regressions compared children currently diagnosed with children previously diagnosed on type of reported parental concern, provider response to reported concern, diagnosing provider, and subtype of ASD diagnosis. Finally, linear regressions evaluated differences on ages of first parental worry, first reported concern, ASD diagnosis, and first services. All models were adjusted using the same covariates used to calculate the propensity score in order to create a doubly robust estimation that increases the likelihood of obtaining an unbiased effect estimator by increasing the likelihood of correctly specifying the model (Bang and Robins, 2005; Funk et al., 2011). These models used Taylor series linearization and the svyset command for the calculation of confidence intervals (CIs). The use of survey weights as predictors in the PSM model and as weights in regression models for key outcomes helps decrease the bias in a given estimation and extends the coverage of the sample (i.e. increasing its representativeness of the total population) (DuGoff et al., 2014).
Results
Characteristics of the population
Table 1 presents estimates of the characteristics of children previously diagnosed with ASD and those currently diagnosed with ASD, based on weighted data from the full sample (n = 1607). Of the children ever diagnosed with ASD, 13.1% (95% CI: 8.9%–18.7%) were estimated to have lost the diagnosis. Children previously diagnosed closely resembled children currently diagnosed with respect to both child and household demographics. Furthermore, children did not differ in age of first service or the age of ASD diagnosis. Parents of children previously diagnosed had not worried about their child’s development at younger ages nor did they report a concern to their child’s doctor earlier than parents of children currently diagnosed. The key differences between the two groups were found in clinical characteristics, namely, the functioning of the child. Children with a previous diagnosis were more likely to currently possess essential daily living skills such as using the bathroom by themselves, feeding themselves, and asking for things or information (if needed) than children currently diagnosed. Children currently diagnosed had a higher mean factor score on the CSBQ, indicating a higher level of autism symptomatology than children previously diagnosed.
Characteristics of children aged 6–17 years previously and currently diagnosed with autism spectrum disorder.
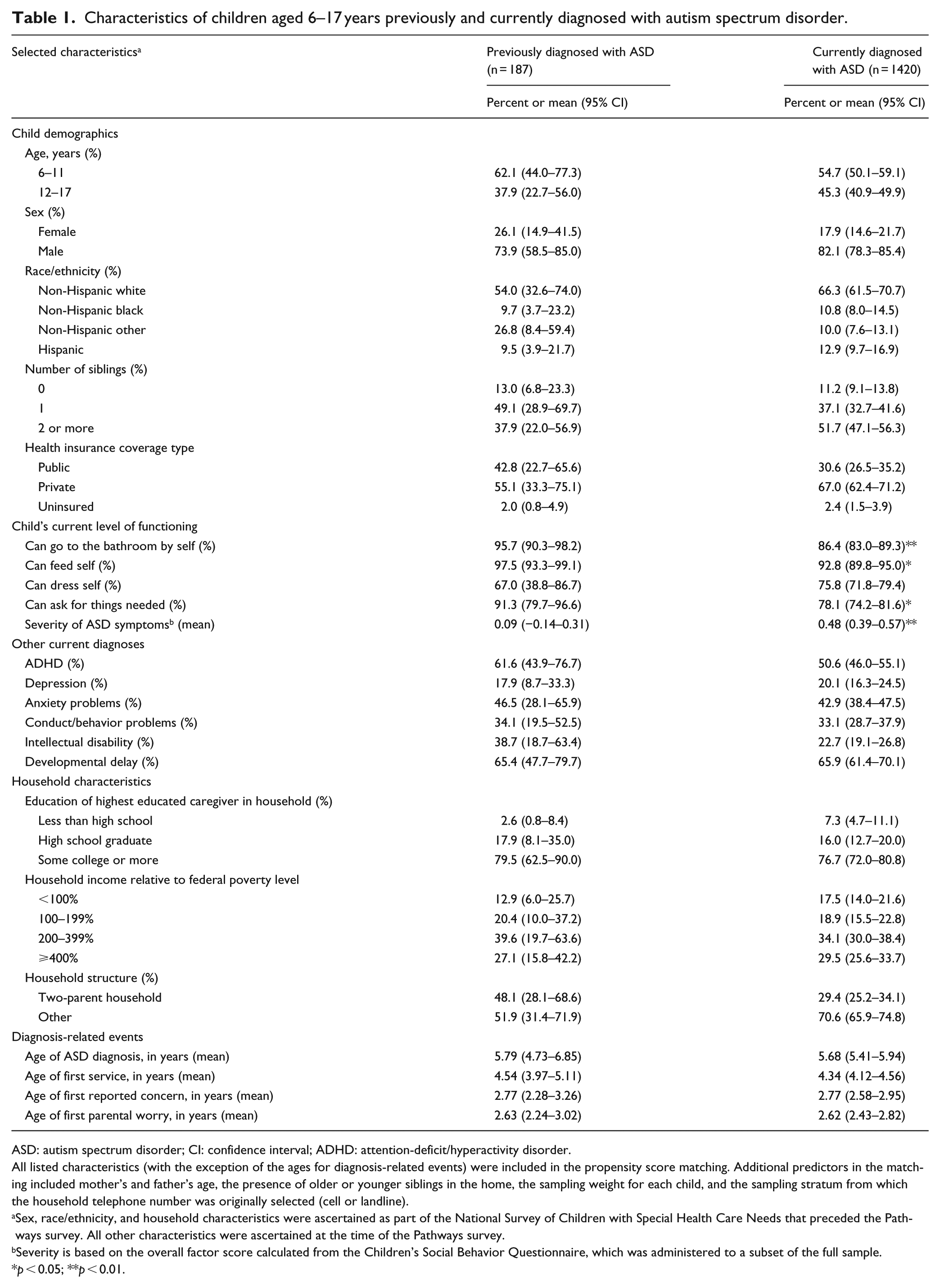
ASD: autism spectrum disorder; CI: confidence interval; ADHD: attention-deficit/hyperactivity disorder.
All listed characteristics (with the exception of the ages for diagnosis-related events) were included in the propensity score matching. Additional predictors in the matching included mother’s and father’s age, the presence of older or younger siblings in the home, the sampling weight for each child, and the sampling stratum from which the household telephone number was originally selected (cell or landline).
Sex, race/ethnicity, and household characteristics were ascertained as part of the National Survey of Children with Special Health Care Needs that preceded the Pathways survey. All other characteristics were ascertained at the time of the Pathways survey.
Severity is based on the overall factor score calculated from the Children’s Social Behavior Questionnaire, which was administered to a subset of the full sample.
p < 0.05; **p < 0.01.
Parent-reported reasons for lost diagnoses
Table 2 presents parents’ perceptions of the reasons their children had lost their ASD diagnosis. As parents could endorse multiple reasons, there was substantial overlap between some categories. The most common perceived reason for a lost diagnosis was a change due to new information (73.5%). Approximately one in four children who lost their ASD diagnosis were said to have never had the condition but to have received the diagnosis due to a need for a diagnosis to receive services (24.2%). The next most common reason for a lost diagnosis was treatment or maturation (21.0%). A small proportion of previously diagnosed children had parents who simply believed that their child’s ASD diagnosis had been incorrect despite the doctor’s judgment (1.9%).
Reasons parents gave for their child’s lost autism spectrum disorder diagnosis, among children aged 6–17 years who were previously diagnosed.

CI: confidence interval; ASD: autism spectrum disorder.
Percentages sum to more than 100% because parents could give more than one reason.
The Pathways survey included questions about replacement diagnoses only when parents reported being explicitly told by a doctor, healthcare provider, or school professional that the child did not have ASD but did have some other developmental, learning, emotional, or mental health condition. This was the case for half (48%) of the previously diagnosed children whose diagnosis was said to have changed due to new information. Thus, the sample size for this analysis (n = 83) is restricted and estimates should be interpreted cautiously; to illustrate, the unweighted sample counts are provided here with the weighted estimates. ADHD was the most common replacement diagnosis (45.9%; n = 36), followed by a sensory, auditory, or processing disorder (22.6%; n = 9); anxiety (17.4%; n = 16); depression (12.9%; n = 8); behavioral or conduct problems (9.2%; n = 8); and learning disability (7.0%; n = 14). Only 4% of previously diagnosed children had a doctor or other professional who said the child did not have ASD and did not have any other developmental, learning, emotional, or mental health condition (n = 8).
For the other previously diagnosed children whose diagnosis was said to have changed due to new information—that is, those whose parents were not explicitly told that the child did not have ASD—replacement diagnoses are unknown. However, when their current diagnoses are considered, most of these children (85.8%) were said to currently have ADHD. This rate was significantly higher (p = 0.01) than the prevalence of current ADHD among those whose parents were explicitly told they did not have ASD (44.3%).
Parental concerns and provider response
The following results represent the statistical analyses incorporating the matched individuals derived from the PSM. Figure 1 compares previously diagnosed and currently diagnosed children by the types of developmental concerns their parents first had. Within the matched sample, previously diagnosed children were less likely to have parents who were first concerned about verbal communication (adjusted odds ratio (AOR) = 0.17, 95% CI: 0.08–0.39), nonverbal communication (AOR = 0.30, 95% CI: 0.11–0.81), learning (AOR = 0.41, 95% CI: 0.21–0.81), and the presence of unusual gestures or movements (AOR = 0.35, 95% CI: 0.16–0.77) than were children currently diagnosed. Table 3 presents the responses of doctors or healthcare providers when a parent first reported concern about their child’s development. Children previously diagnosed were less likely to have had a doctor who made a referral to a specialist than children currently diagnosed (AOR = 0.46, 95% CI: 0.22–0.95).
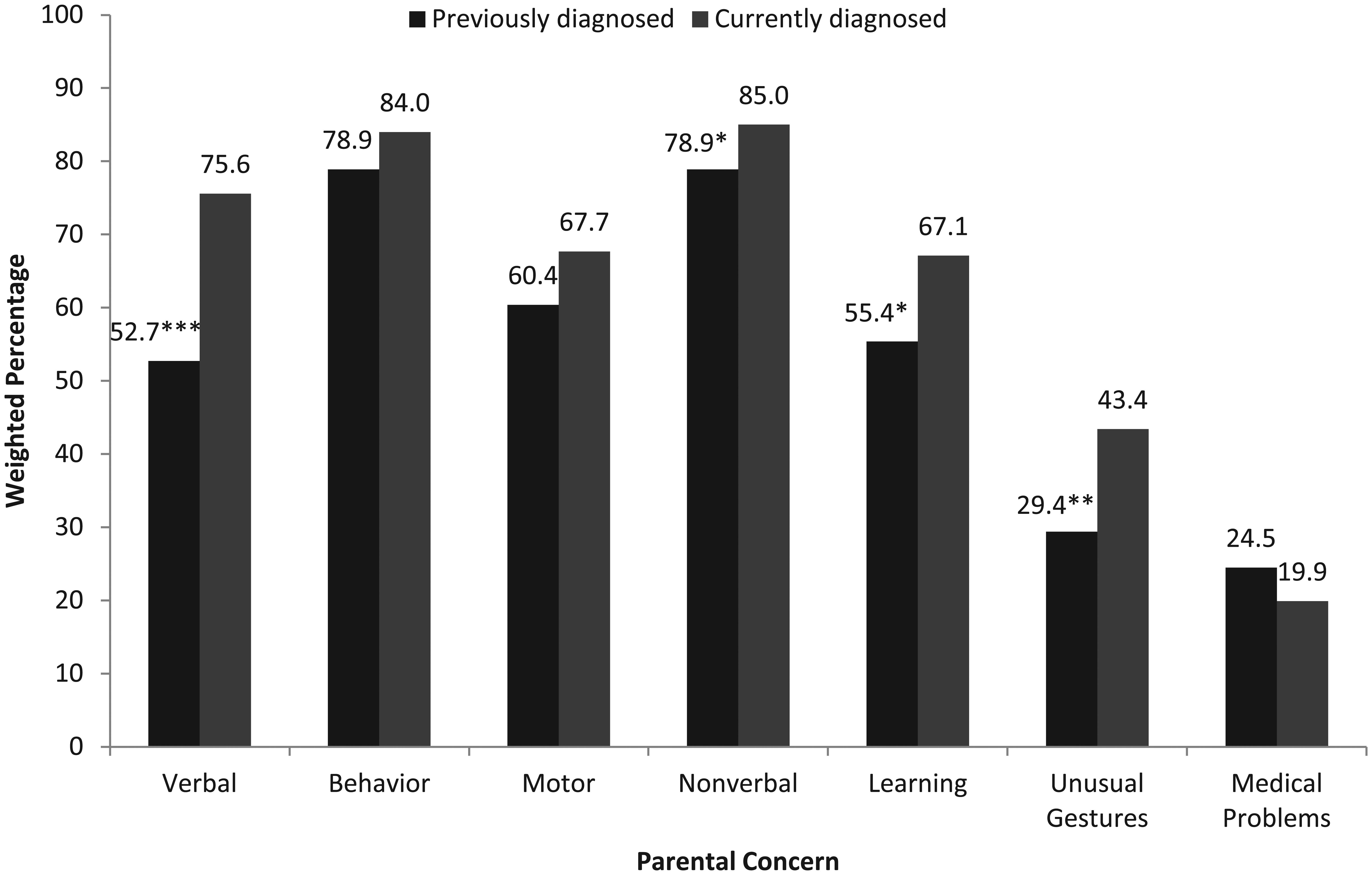
Proportion of propensity-score-matched children aged 6–17 years whose parents were first concerned about specific behaviors, problems, or delayed milestones, by ASD diagnostic status.
Parents’ perceptions of doctor or healthcare provider response to parental concerns, by parent-reported ASD diagnostic status, for propensity-score-matched children aged 6–17 years.
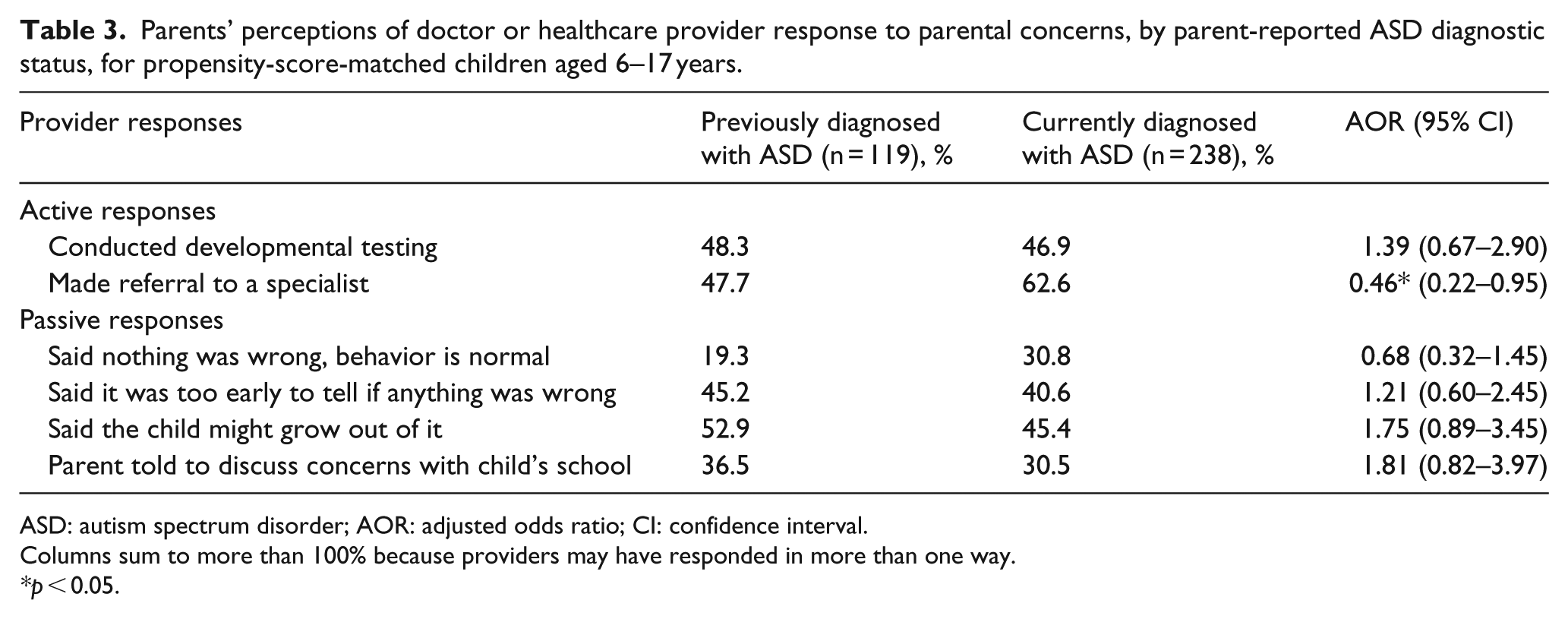
ASD: autism spectrum disorder; AOR: adjusted odds ratio; CI: confidence interval.
Columns sum to more than 100% because providers may have responded in more than one way.
p < 0.05.
Diagnosing provider
Figure 2 displays the percent distribution of the types of providers who made the children’s first ASD diagnosis. Within the matched sample, previously diagnosed children were less likely than currently diagnosed children to have first received the diagnosis from a specialist medical provider (AOR = 0.34, 95% CI: 0.15–0.76). Children previously diagnosed were as likely as currently diagnosed children to have first received the diagnosis from a pediatrician or generalist (AOR = 1.84, 95% CI: 0.64–5.27), mental health provider (AOR = 1.25, 95% CI: 0.64–2.47), or a school/other provider (AOR = 1.11, 95% CI: 0.53–2.34).
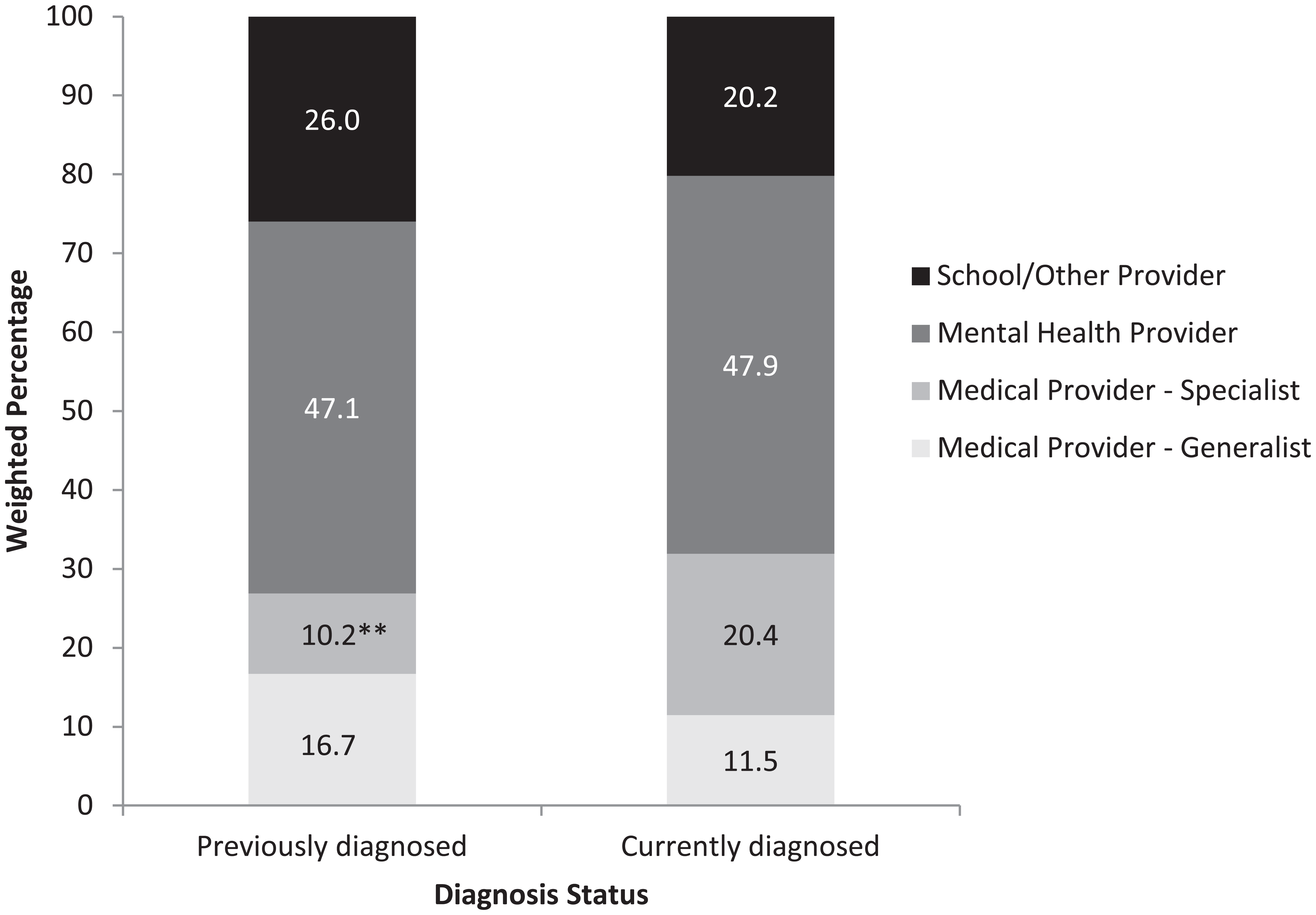
Percent distribution of types of providers making first diagnosis of autism spectrum disorder, by diagnosis status, for propensity-score-matched children aged 6–17 years.
ASD subtypes
Figure 3 presents estimates of the percent of previously and currently diagnosed children ever diagnosed with each of three ASD subtypes. As children could be given multiple ASD diagnoses, the categories are not mutually exclusive. Within the matched sample, 32.2% of children had received more than one ASD subtype diagnosis. In fact, children diagnosed with more than one diagnosis were more likely to be currently diagnosed than previously diagnosed (AOR = 4.72, 95% CI: 2.11–10.57). Additionally, children currently diagnosed were more likely to have been diagnosed with autistic disorder (AOR = 1.99, 95% CI: 1.04–3.82) or Asperger’s disorder (AOR = 6.29, 95% CI: 2.74–14.43) than children previously diagnosed. In general, children previously diagnosed were less likely to have received an ASD subtype diagnosis (AOR = 0.27, 95% CI: 0.12–0.62) than children currently diagnosed.
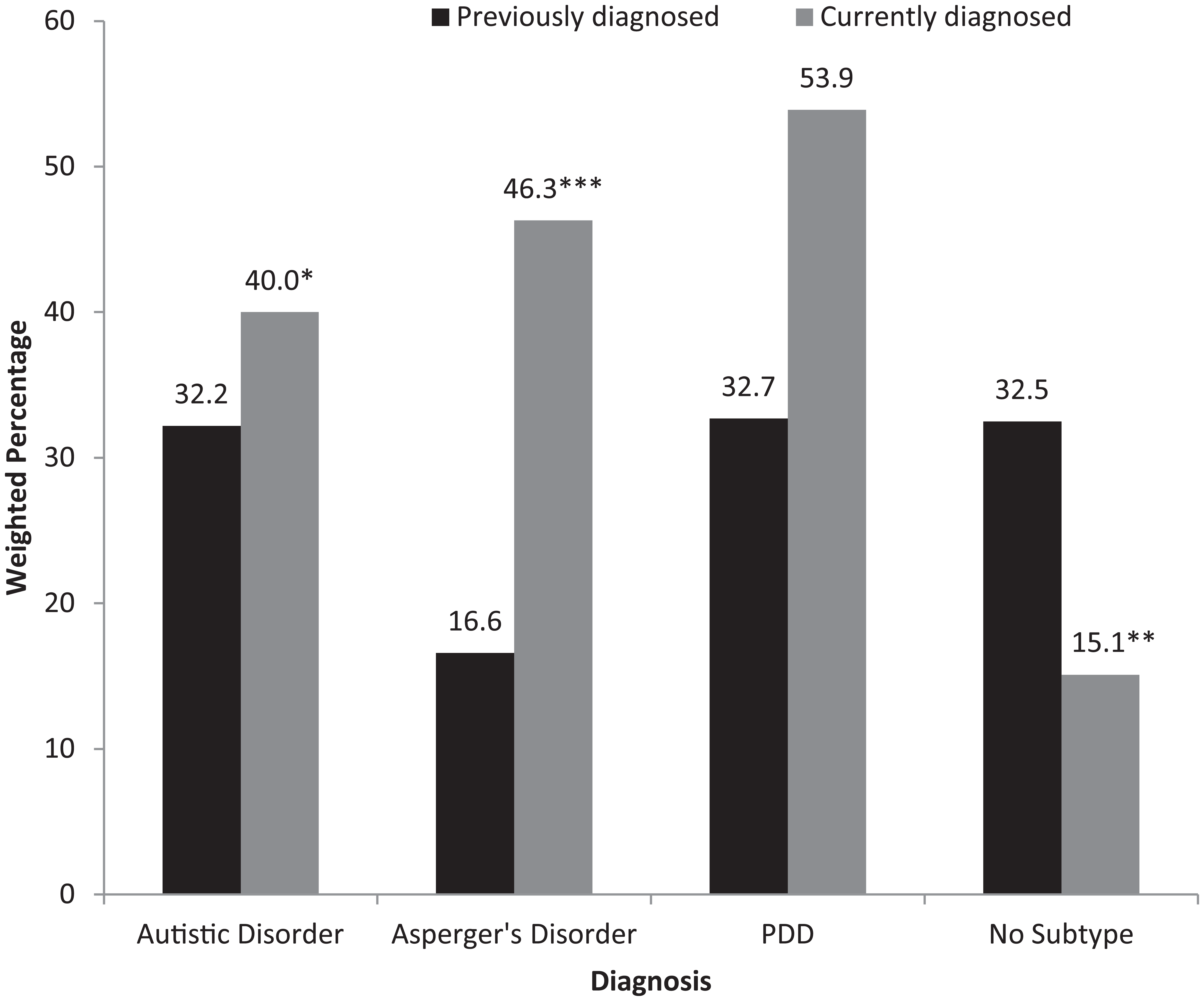
Proportion of propensity-score-matched children aged 6–17 years who were ever diagnosed with specific ASD subtypes, by ASD diagnostic status.
Age of diagnosis-related outcomes
Finally, the mean age of children for the four diagnosis-related outcomes was examined in the matched sample. Previously diagnosed children and children currently diagnosed did not vary in age of first parental worry (β = −0.05, 95% CI: −0.49 to 0.38), first reported parental concern (β = −0.01, 95% CI: −0.49 to 0.46), ASD diagnosis (β = 0.53, 95% CI: −0.14 to 1.21), and first services (β = 0.47, 95% CI: −0.05 to 0.99).
Discussion
Research focused on the stability of the clinical ASD diagnosis has suggested that moving off the spectrum may be the product of maturation, intervention, or overdiagnosis at an early age (Kleinman et al., 2008). The reasons may be varied, but this study reveals that the most common—at least according to the parents of three-fourths of children with a lost diagnosis—is that the diagnosis was changed due to new information. The high percentage of children in this study who lost an ASD diagnosis because it was changed (73.5% of 13.1%, or over 9% of all school-aged CSHCN ever diagnosed with ASD) suggests overdiagnosis may be more common in this population than expected. Overdiagnosis could be the result of difficulty distinguishing children with ASD from children who possess language delays or global developmental delays (Lord, 1995) and because variability in the quality of screening and evaluation practices confound diagnostic precision (Fenikile et al., 2014).
Although an ADHD diagnosis was no more common among children previously diagnosed with ASD than among children currently diagnosed, a large percentage of children who had their ASD diagnosis changed to a new diagnosis had their diagnosis changed to ADHD. It is possible this is the result of the high overlap between the symptoms of these disorders (Rao and Landa, 2014; Taurines et al., 2012). As language and social skills deficits are addressed, hyperactivity and inattentiveness may become more obvious and be diagnosed as ADHD (Fein et al., 2005). For some children, this may be a replacement diagnosis, but for other children, it may be an additional diagnosis reflecting problems in attentional flexibility beyond what is typical for children with ASD (Polderman et al., 2013).
Overdiagnosis may also occur if ASD diagnoses are substituted for other learning disabilities because of the availability of greater resources for treatment of ASD (Shattuck, 2006). Parents in this study confirmed that some children who reportedly did not have ASD—approximately one in four who lost their ASD diagnosis or 3% of all school-aged CSHCN ever diagnosed with ASD—were given the diagnosis due to their need for services. Early intervention programs can hasten the attainment of developmental milestones critical for continued social, emotional, and educational success, even if the child does not have ASD (Silverstein et al., 2006). Accordingly, the American Academy of Pediatrics (AAP) recommends that pediatric primary care physicians refer children with positive screening tests to receive intervention services for children with ASD before the results of a comprehensive ASD evaluation are known (Johnson and Myers, 2007).
Few children ever diagnosed with ASD were said to have actually had and recovered from ASD. Only 21% of children with a lost diagnosis (or less than 3% of all school-aged CSHCN ever diagnosed with ASD) were said to have lost it due to treatment or maturity. The true rate of recovery may be even smaller if some of these children were incorrectly thought by their parents or doctors to have lost their ASD because they now have well-developed coping skills and other strengths.
Differences between previously diagnosed and currently diagnosed children
In addition to describing parents’ perceptions of the reasons their children lost an ASD diagnosis, this study also examined differences between children previously and currently diagnosed with an ASD. Based on data from the full sample, children previously diagnosed were higher functioning with fewer ASD symptoms (i.e. social and behavioral problems). It is unsurprising that a direct comparison of children with previous or current ASD reveals a key difference in the children’s current level of functioning. Children with ASD who achieve the normal range of cognitive, adaptive, and social skills described as the “optimal outcome” are significantly more likely to have a higher cognitive ability as well as fewer symptoms associated with ASDs than other children with ASD (Fein et al., 2013; Troyb et al., 2014).
To focus on differences around the time of the initial diagnosis, it was necessary to control for the children’s current level of functioning and other current characteristics related to diagnosis loss. This was done with a matched analysis comparing children with equivalent propensity to have lost their diagnosis based on demographics, functioning, and ASD symptoms. In this analysis, children who were previously diagnosed were less likely than children who were still currently diagnosed to have parents who had early concerns about their verbal skills, nonverbal communication, learning, and unusual gestures or movements. This is consistent with previous literature (e.g. Turner and Stone, 2007) that found children with greater language and social problems at an early age having higher diagnostic stability. Children previously diagnosed were also less likely to have been diagnosed with either Asperger’s disorder or autistic disorder than children currently diagnosed.
In the matched analyses, previously diagnosed children were also less likely than currently diagnosed children to have received the diagnosis from a specialist. Some might conclude from that result that specialists are better than other healthcare professionals at making accurate diagnoses, perhaps because of the difficulty in correctly differentiating children with ASD from children with other health conditions and other developmental delays (Ohta et al., 1987; Siegel et al., 1988). However, previously diagnosed children were also less likely to have been referred to a specialist. Children receiving a referral often have more severe symptoms, so these results may simply highlight that children with greater verbal and learning problems at an early age had higher diagnostic stability, even when compared to children matched on current level of functioning. This is consistent with findings that children with milder autism at an earlier age are more likely than other children with ASD to achieve the “optimal outcome” (Fein et al., 2013).
Strengths and limitations
The majority of previous studies on optimal outcome and ASD diagnosis loss have utilized clinical samples that are typically restricted to a single geographic region. A major strength of this study is the large probability-based community sample of children diagnosed with ASD. The sample represents a clinically diverse national population that rivals any current study dedicated to the topic of lost diagnosis. The use of PSM further enhanced this study by reducing the risk for bias that could have been introduced by logistic regressions with unbalanced distributions of covariates, uneven sample sizes, and unequal variances of given covariates between groups (Rubin, 2001). The use of PSM also reduces the risk of bias that may have occurred because the data were drawn from a telephone survey with a low response rate conducted only in English. The impact of selection biases resulting from sampling, nonresponse, and lack of coverage of non-English speaking households and households without telephones is unknowable, but they are less likely to influence the magnitude of comparisons between matched pairs than absolute estimates of a population prevalence. Still, due to the low response rate, generalizing the results beyond the sample should be done with caution.
Furthermore, PSM is not without its own set of limitations. A PSM is only as powerful as the variables used in the match, and unmeasured confounding could be a significant problem if variables that would affect a child losing their ASD diagnosis are not included. Studies with small sample sizes are also more likely to have an imbalance of such covariates (Shadish et al., 2002). Additionally, in this study, many variables were measured at one time point and have the potential to vary as the child ages and matures. It was only possible to capture a current picture of children that may not accurately reflect the children at the age when they lost their diagnosis.
The study also needs to be viewed in light of limitations specific to the survey design and sampling. The Pathways sample consisted only of CSHCN, defined as requiring health or related services beyond those required by children generally (McPherson et al., 1998). Nearly all children (95%) currently diagnosed with ASD have special healthcare needs, but only 75% of children previously diagnosed do (National Survey of Children’s Health, 2011–2012). Special healthcare needs status, diagnostic criteria, and the reasons for the loss of the diagnosis among the previously diagnosed children were based on parent report and not confirmed with medical records or independent evaluation. It is not known what types of new information led to changed diagnoses or where this new information originated. It is also not known which children truly do (or did) meet formal criteria for having ASD, and none of the survey measures offers diagnostic confirmation or can be considered reliable screening tools. It should be further noted that the follow-up question asking about a current diagnosis only referred to “autism or ASD.” Some parents of children with a current diagnosis of PDD-NOS or Asperger’s disorder may have said their children did not have a current diagnosis if they did not recognize these conditions as ASD, but the number is likely to be few because (as shown in Figure 3) previously diagnosed children were still less likely than currently diagnosed children to have ever been diagnosed with these subtypes. Finally, Pathways was a cross-sectional survey; thus, it is not possible to determine the directionality of associations or the existence of causality.
Conclusion
The results of this study suggest that some children with developmental delays, attentional flexibility problems, or other conditions may be receiving provisional yet inaccurate diagnoses of ASD from nonspecialists, even when their parents do not present with concerns about verbal skills, nonverbal communication, learning, and unusual gestures. This could be a natural consequence of changes in ASD awareness among healthcare professionals and the push by national organizations such as the AAP to increase the use of developmental screening tests by general pediatricians with all young patients regardless of parents’ presenting concerns (CDC, 2014b; Johnson and Myers, 2007; National Center for Medical Home Implementation, 2012). However, this cross-sectional study cannot be used to determine whether overdiagnosis and other reasons for lost diagnoses have recently become more common. It should also be noted that their estimated prevalence is too low to explain recent increases in the estimated prevalence of ASD (Blumberg et al., 2013; CDC, 2014a). Nevertheless, this study confirms that ASD diagnoses can and sometimes do change as children mature and overcome delays, and as new information is assimilated by their healthcare providers. These changes over time can complicate the use of surveys and retrospective surveillance methods to estimate the current prevalence of ASD, the characteristics of children who currently have ASD, and the adequacy of services for this population.
Footnotes
Declaration of conflicting interests
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, the University of Washington, the National Institutes of Health, or the Health Resources and Services Administration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.