
Abstract
This study examined the longitudinal associations between child behavior problems, coping strategies, social resources, and parenting stress in mothers of young children with autism spectrum disorder. Participants were 283 mothers who completed self- and child-report measures at the time of diagnosis and 2 years later. Hierarchical multiple regression was conducted to predict overall parenting stress. At diagnosis, the final model indicated that high levels of social support and mothers’ use of active engaged coping strategies were associated with lower levels of parenting stress. Conversely, high levels of child externalizing behavior problems, family dysfunction, and mothers’ use of disengaged coping strategies were associated with higher parenting stress. Two years later, high levels of parenting stress at diagnosis predicted increased parenting stress. In addition, high or increasing levels of social support predicted a decrease in parenting stress, while high or increasing levels of family dysfunction predicted increased stress. Finally, increased use of disengaged coping strategies and decreased use of active coping strategies over time predicted higher levels of parenting stress. Results are discussed in terms of their implications for the provision of targeted supports that are designed to enhance the personal and social resources available to mothers of children with autism spectrum disorder.
Introduction
Parenting stress can be defined as an “aversive psychological reaction to the demands of being a parent” (Deater-Deckard, 1998: 315). Abidin (1995) proposed that parenting stress is created by a mismatch between the perceived demands of parenting and the personal and social resources available to meet those demands. Children with autism spectrum disorder (ASD) present with social communication symptoms that are often combined with problem behavior (e.g. anxiety, screaming, and aggression)—a combination that can be difficult to manage, especially when there is uncertainty about how to intervene effectively (Kuhn and Carter, 2006). In a recent meta-analysis, Hayes and Watson (2013) reported significantly higher levels of parenting stress among parents of children with ASD compared to parents of typically developing children and children with Down syndrome, in particular.
Parents of children with ASD begin to experience stress prior to diagnosis, when they start to seek help because of concerns about their child’s failure to interact or communicate (see Reed and Osborne, 2012 for a review). There is also evidence that parenting stress persists over the course of a child’s early development (Herring et al., 2006; Zaidman-Zait et al., 2014) and extends into adolescence and adulthood (Smith et al., 2010). Understanding the factors that contribute to (or ameliorate) parenting stress is important because such stress is potentially detrimental to the long-term well-being of both the parents and their children (Crnic and Low, 2002). For children with ASD, negative effects can include sub-optimal treatment outcomes (Osborne et al., 2008) and increased behavior problems (Lecavalier et al., 2006). For parents, stress increases the risk of poor mental health (Hastings, 2003), maladaptive parenting practices (Osborne and Reed, 2010), and difficulty with the implementation of behavioral interventions for their children (Kazdin, 1995).
Numerous studies have identified child-related factors that are associated with parenting stress (see Karst and Van Hecke, 2012 for a review). These include ASD symptom severity (Falk et al., 2014; Lyons et al., 2010), as well as children’s cognitive and communication abilities (Bebko et al., 1987), adaptive behavior (Hall and Graff, 2011), externalizing and internalizing problem behavior (Zaidman-Zait et al., 2011, 2014), and restricted and repetitive behaviors (Gabriels et al., 2005). However, the characteristics of children with ASD are not the only variables that influence stress; parents’ personal and social resources may also have an impact, although they have not been examined as extensively as child behavioral issues. Such resources may be valued in their own right, may assist in the acquisition of other valued resources, or may facilitate stress reduction (Hobfoll, 2002). According to Hobfoll’s (1989) Conservation of Resources (COR) theory, people mobilize resources in the face of stressful events to offset ongoing challenges, improve their condition, maintain well-being, and adjust successfully to stressors. Hobfoll posited that resource loss or gain is the primary operating mechanism driving stress reactions. When faced with a resource demand such as parenting a child with ASD, resource loss may render an individual vulnerable to stress and lead to a downward spiral. Conversely, resource gain in the face of a challenge may enhance an individual’s ability to overcome the threat of a stressor.
Two of the main sources of coping with stress are personal and social resources (Hobfoll, 2002; Holahan et al., 1997; McCubbin and Patterson, 1983). Personal resources are aspects of the self, such as an individual’s coping style and strategies. Coping is an active, purposeful process that includes behavioral, emotional, and cognitive attempts to manage the demands imposed by a stressor (Lazarus, 1998; Lazarus and Folkman, 1987). Among parents raising children with ASD, specific coping strategies have been found to be associated with either reduced or elevated levels of parenting stress. For example, Hastings et al. (2005) found that active, avoidant coping strategies (i.e. taking steps aimed at eliminating or avoiding a stressor) and religious/denial-based coping strategies (i.e. denying the existence of a stressor or turning to religion in times of stress) were associated with increased parent stress. In contrast, Benson (2010) found that the use of cognitive reframing (a coping strategy that is aimed at viewing a stressor in a positive light) was associated with increased well-being. In another study, Smith et al. (2008) found that both decreased emotion-focused coping strategies (aimed at reducing or managing feelings of distress) and increased problem-focused coping strategies (aimed at solving a problem or changing the source of stress) were associated with increased adjustment among mothers of preschoolers with ASD, regardless of ASD symptom severity. However, only one study to date has examined the longitudinal impact of parental coping strategies on maternal adjustment. In this study, Benson (2014) found that both proactive problem-focused coping and cognitive reframing predicted a reduction in maternal distress over time, while maternal distraction (i.e. a coping strategy aimed at diverting attention away from the stressor) was significantly linked to increased distress.
Consistent with COR theory, both familial and extra-familial social supports represent a source of potential resource gain that can help parents to manage the demands associated with raising a child with ASD. In most cases, parenting a child with ASD is not an individual, isolated endeavor; parenting usually occurs in a family and community context. Families are social systems wherein each individual or subsystem is influenced by the others. Thus, when families function well, family members are able to resolve problems, support one another, communicate effectively, and respond empathetically to challenges that arise (Byles et al., 1988). Similarly, when community supports are available (e.g. from friends, community resources/professionals, and support groups), caregivers feel less isolated, more optimistic, and experience higher life satisfaction overall (Ekas et al., 2010). In contrast, family dysfunction has a detrimental effect on caregivers’ well-being and can result in resource loss, which in turn diminishes parents’ ability to manage their caregiving responsibilities and hinders their overall well-being. Unfortunately, some researchers have found that family dysfunction is more prevalent in families of children with ASD compared to other families (Rao and Beidel, 2009). Parents of children with ASD also report less access to social support from friends and more reliance on support from paid professionals than parents of children without ASD (Weiss, 2002). For these parents, whose resources may already be depleted due to the ongoing challenges associated with raising a child with ASD, a combination of family dysfunction and lack of community social supports may exacerbate parenting stress.
Overall, previous studies have demonstrated that personal and social resources can have a significant impact on stress in parents of children with ASD (Benson, 2010, 2014; Hall and Graff, 2011; Hastings et al., 2005; Smith et al., 2008; Tehee et al., 2009). However, with the exception of Benson (2014), who examined the impact of coping strategies on maternal adjustment over time, past research has used cross-sectional designs and/or small sample sizes and has overlooked the influence that changes in resources over time might have on parenting stress. In addition, when examining the effect of personal and social resources, ASD-related symptoms and behavior of the child must also be taken into account, given that past work has found these to be important predictors of parenting stress. Thus, the aims of this study were to examine: (1) whether personal (i.e. coping strategies) and social resources (both familial and community-based) were associated with parenting stress at the time of ASD diagnosis and (2) whether changes in personal and/or social resources predicted a change in parenting stress over a 2-year period. In addressing these goals, we controlled for child-level variables that included ASD severity, adaptive behavior, language comprehension, expressive communication, internalizing and externalizing behavior problems, and repetitive behavior, based on past research indicating that such variables may be important predictors of parenting stress (see Karst and Van Hecke, 2012).
Method
Participants
Data for this study were drawn from Pathways in ASD, a large Canadian multisite longitudinal study examining the developmental trajectories of children with ASD in an inception cohort recruited across five Canadian provinces. The study was approved by the Research Ethics Boards at all participating sites and all families gave active informed consent to participate in this study. To participate in the Pathways study, children had to meet the following inclusion criteria: (1) be between ages 2;0 and 4;11 (years; months) at the time of diagnosis and (2) have a recent (within 4 months) diagnosis of ASD, assigned by an experienced clinician, according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association (APA), 2000) and confirmed by both the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2002) and the Autism Diagnostic Interview–Revised (ADI-R; Rutter et al., 2003).
The children were primarily boys (83.7%) whose mean age at diagnosis (Time 1, T1) was 38.9 months (standard deviation (SD) = 8.6). At T1, mean receptive and expressive language standard scores on the Preschool Language Scale, 4th edition (PLS-4; Zimmerman et al., 2002) were 66.8 (SD = 21.2) and 71.4 (SD = 18.2), respectively, reflecting significant deficits in both language domains. Cognitive development was assessed at T1 for 238 of the children (83.8%) using the Merrill-Palmer-Revised Scales of Development (M-P-R; Roid and Sampers, 2004). The children’s mean developmental index (DI) standard score on the M-P-R was 59.1 (SD = 27.3). The DI is a general index (comparable to an intelligent quotient (IQ)) that comprises subtests measuring cognition, fine motor, and receptive language abilities.
In the current analysis, data were obtained from two waves of family data that were collected approximately 2 years apart. The T1 assessment included 283 mothers whose children with ASD were diagnosed within the previous 4 months. Families’ demographic information at T1 is summarized in Table 1. The second wave of parent data (T2) was collected approximately 24 months later from 191 mothers, all of whom completed the parenting stress measure used in the study. Of the 92 mothers for whom parenting stress data were missing, 30 had withdrawn from the study (10.6% of the T1 sample) and the others were unavailable for participation. There were no statistically significant differences between families who did and did not participate in T2 assessments with regard to T1 parenting stress t(281) = −0.53, p = 0.60; child’s age of diagnosis t(281) = 0.69, p = 0.49; child’s autism severity score t(281) = −1.73, p = 0.08; or mothers’ level of education, t(281) = −1.52, p = 0.13. However, mothers who reported higher annual household income levels at T1 were more likely to participate at T2, t(154.24) = −3.88, p < 0.001. For all 191 mothers who completed the parenting stress measure at T2, we also obtained a second assessment of the personal and social resources.
Participant (mothers’) demographics.
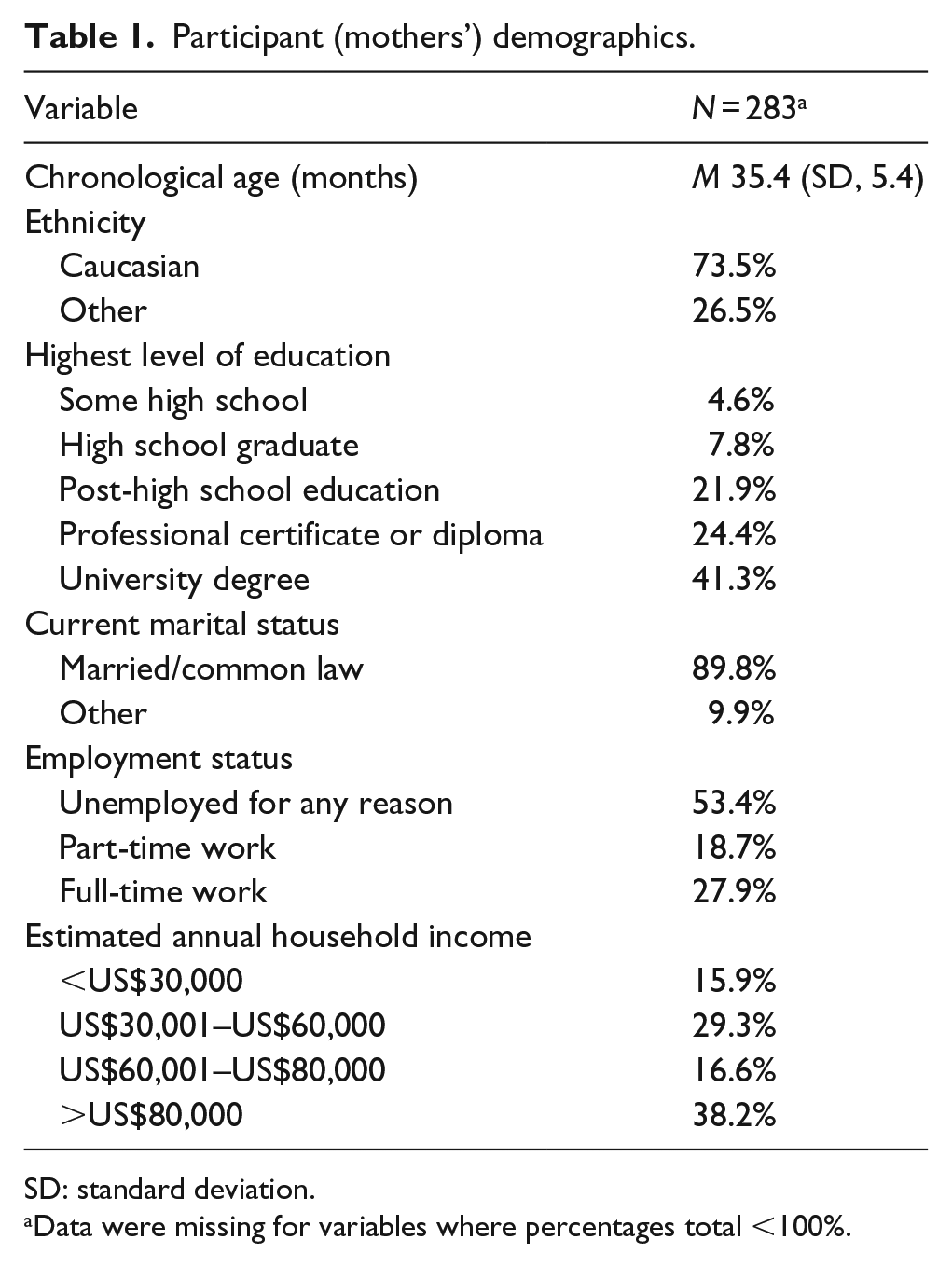
SD: standard deviation.
Data were missing for variables where percentages total <100%.
Measures
Family demographics
Information about families’ annual household income and mothers’ chronological age, ethnicity, level of education, and employment status was gathered at both T1 and T2 using the Family Background Information Questionnaire (Hambly and Fombonne, 2005) developed for the Pathways study. In the analyses, annual household income was treated as a continuous variable, ranging from less than CAN$5000 to more than CAN$80,000, as was maternal education, which ranged from some high school to an earned doctorate. Ethnicity was treated as a dichotomous variable (Caucasian and other), as was marital status (married/common law and not married).
Parenting stress
Mothers completed the Parenting Stress Index: Short Form (PSI-SF; Abidin, 1995) at both T1 and T2. Based on previous psychometric work on the PSI-SF among parents of children with ASD (Zaidman-Zait et al., 2011), we used the combined score of the General Distress and Parenting Distress subscales, which contained 13 items overall (α = 0.90, in this study), with higher scores indicating increased parenting stress. Parents rate each of the items on a 5-point scale ranging from strongly disagree (1) to strongly agree (5). Example items include not being able to “handle things” and feeling “trapped by parenting responsibilities.” We restricted our analysis to the combined score across these two subscales in order to avoid content overlap between our measure of child behavior and the other factors that reflect child-rearing stress. The use of selected subscales from the PSI-SF has a precedent in previous studies of children with ASD (e.g. McStay et al., 2013).
Family functioning
The General Family Functioning (GFF) subscale of the McMaster Family Assessment Device (Byles et al., 1988), an overall measure of family health/pathology, was used to assess self-reported family functioning. The subscale consists of 12 items that were rated on a 4-point Likert scale on which 1 = strongly agree and 4 = strongly disagree. Example items include “We confide in each other” and “We don’t get along well together.” Composite scores can vary between 0 and 36, with higher scores indicating more family dysfunction (α = 0.92, in this study).
Parent social support
The Social Support Scale (SSS) of the Canadian National Longitudinal Survey of Children and Youth (Statistics Canada, Special Surveys Division, 2007) was used to measure mothers’ perceived social support. This scale consists of six items that were rated on a 4-point Likert scale on which 1 = strongly disagree and 4 = strongly agree. Example items include “I have family and friends who help me feel safe, secure and happy.” The six items were combined to create a total score for perceived social support (α = 0.88, in this study).
Parent coping strategies
Maternal use of coping strategies was assessed using the Ways of Coping Questionnaire (WoC; Folkman and Lazarus, 1988). The WoC includes 66 items that were divided into eight subscales and rated on a 4-point Likert scale (0 = does not apply/do not use to 3 = used a great deal) that reflected how frequently respondents reported that they employ various coping strategies. Although there are different conceptualizations of coping styles, the WoC scales are usually consolidated into two main categories. The first, engaged or problem-focused coping, refers to the extent to which individuals actively attempt to solve problems and cope with affiliated emotions. The second, disengaged or avoidant coping, refers to the extent to which individuals attempt to avoid problems and affiliated emotions (Lazarus and Folkman, 1987).
To base our coping style categories in the context of mothers of children with ASD, maternal responses on the eight WoC theoretically derived subscales were subjected to a principal component analysis (PCA) using SPSS, version 22.0. PCA is an appropriate method when the goal is data reduction for better categorization of a multidimensional measure (Norris and Lecavalier, 2010). We used multiple methods to decide the number of factors to extract, including the eigenvalues-greater-than-one rule, the scree-test criterion (Cattell, 1966), and parallel analysis (O’Connor, 2000), in conjunction with the content of the subscales and the corresponding construct of interest (Norris and Lecavalier, 2010; Russell, 2002). We then employed a simple-structure interpretation of the factor loadings after oblique rotation, with a minimum factor loading of 0.40 (Stevens, 2009). To aid in interpretation, we also followed Russell’s (2002) recommendation that items should not load higher than the acceptable minimum factor loading on more than one factor (i.e. no cross loadings), to ensure adequate identification. Findings indicated a two-factor solution explaining 61.03% of the common variance (the first three eigenvalues were 3.61, 1.27, and 0.74). The first factor, labeled Active Engaged Problem-focused Coping, refers to the extent to which mothers used active efforts to solve the problem, get help, or construct positive meaning. This factor included three WoC subscales: Planful Problem-Solving (six items, e.g., “I made a plan of action and followed it”), Seeking Social Support (six items, e.g., “I talked to someone to find out more about the situation”), and Positive Reappraisal (seven items, e.g., “I rediscovered what is important in life”), loadings ranged from 0.73 to 0.86 (α = 0.86). The second factor, labeled Disengaged Emotion-focused Coping, refers to mothers’ attempts to distance, avoid, or minimize the stressor and associated negative emotions. It included five WoC scales: Distancing (six items, e.g., “I tried to forget the whole thing”), Escape-Avoidance (eight items, e.g., “I slept more than usual”), Self-Control (seven items, e.g., “I tried to keep my feelings to myself”), Accepting Responsibility (four items, e.g., “I criticized or lectured myself”), and Confrontive Coping (six items, e.g., “I let my feelings out somehow”), loadings ranged from 0.62 to 0.85 (α = 0.87). As expected, the two factors were correlated (r = 0.36, p < 0.001).
Autism severity
The Autism Diagnosis Observation Schedule (ADOS; Lord et al., 2000) is a semi-structured, standardized assessment in which a trained examiner engages participants in activities that are designed to assess social and communication behavior indicative of Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR) symptoms of ASD. In this study, the severity metric was used (Gotham et al., 2009), with scores ranging from 1 to 10; higher scores indicate more severe ASD symptoms.
Child cognitive ability
The M-P-R (Roid and Sampers, 2004) can be used with individuals between 1 month and 6.5 years of age and was employed as a measure of cognitive development. In this study, the DI, which comprises scales measuring cognition, fine motor skills, and receptive language, was used to assess intellectual functioning.
Child language ability
The PLS-4 (Zimmerman et al., 2002) was used as a measure of both language comprehension and expressive communication. The PLS-4 is an individually administered test that can be used with children from birth through 6 years 11 months. In this study, raw scores for both the comprehension and expressive subtests were available for all participants and thus were used for data analysis.
Child adaptive behavior
Children were assessed with the Vineland Adaptive Behavior Scales, Second Edition Interview Form (VABS-II; Sparrow et al., 2005). The VABS-II is a semi-structured interview that is administered to a parent or caregiver. It assesses child adaptive behavior in the communication, socialization, daily living skills, and motor domains and expresses overall functioning in an adaptive behavior composite (ABC) score. A child’s performance on a given developmental task is rated on a scale from 0 (never) to 2 (usually). Higher scores indicate superior adaptive behavior skills.
Child behavior problems
The Child Behavior Checklist 1.5–5 (CBCL 1.5–5; Achenbach and Rescorla, 2000) is a well-standardized measure that was used to assess children’s externalizing and internalizing behavior. A parent responds to 99 items using a 3-point scale (0 = not true, 1 = somewhat/sometimes true, and 2 = very/often true). A recent study provided support for the factor structure of the CBCL 1.5–5 in a sample of 128 preschoolers with ASD (Pandolfi et al., 2009).
Child repetitive behavior
The Repetitive Behavior Scale–Revised (RBS-R; Bodfish et al., 2000) is a parent-report measure that was used to measure the presence and severity of a variety of restricted, repetitive child behavior. The RBS-R comprises 43 items that are distributed across six conceptually derived subscales: Stereotyped Behavior, Self-injurious Behavior, Compulsive Behavior, Routine Behavior, Sameness Behavior, and Restricted Behavior. Its factor structure was recently validated with children in the Pathways study (Mirenda et al., 2010). In this study, we used the RBS-R total mean score (α = 0.93).
Data analytic plan
Our first goal was to determine whether mothers’ personal (i.e. coping strategies) and social resources (both family and community-based) were associated with parenting stress at the time of ASD diagnosis (T1), beyond child-level variables. Accordingly, we first examined the independent relations between each of the child and parent variables at T1, using Pearson product–moment correlations. Next, we conducted a hierarchical multiple regression analysis. In step 1, we entered family demographic variables (annual household income and mothers’ ethnicity, level of education, and employment status) as covariates. In step 2, we entered all T1 child-level variables that were statistically significantly correlated with parenting stress; in step 3, we entered mothers’ personal and social resource scores from the GFF, SSS, and WoC at T1.
Our second goal was to examine whether changes in personal and/or social resources predicted a change in parenting stress over a 2-year period. Two statistical techniques are appropriate for examining change over time—analysis of change scores based on raw data and analysis of residualized change (Zumbo, 1999). We choose to use change scores for several reasons. First, we were interested in change among individual participants (i.e. mothers), as opposed to change in respect to the entire group, which is the focus when using residualized change. Second, analysis of change scores can be used to model individual-level change in situations where some participants’ scores increase while other participants’ scores decrease or stay static, which was the case in this data set. The reliability of change scores is maximized when reliability is high for each individual component measure and the correlation between component measures is moderate (Chiou and Spreng, 1996). In this data set, all personal and social resource measures had acceptable internal consistency at both time points, and correlations between T1 and T2 scores fell in the moderate-to-high range (r = 0.50–0.64).
In the analysis of change, we first entered the four T1 family demographic covariates described previously into a second hierarchical multiple regression. In the second step, we controlled for T1 parenting stress; in the third step, we entered the same T1 child variables that were entered in the T1 regression model, as well as all T1 parental personal and social resource measures (i.e. maternal coping, social support, and family functioning), to control for the effect of these predictors. We then computed change scores for the GFF, SSS, and WoC by subtracting T1 raw scores from T2 raw scores and entered these change scores in step 4 (thus, positive values indicate a score increase).
Results
Descriptive statistics for the key child and maternal variables included in the study at T1 and the bivariate correlations among the variables are presented in Table 2. Child behavior problems (both externalizing and internalizing) and restricted, repetitive behavior were moderately correlated with parenting stress. In contrast, children’s adaptive behavior, both expressive language and language comprehension, and cognitive ability were not correlated with parenting stress. Hence, they were not included in the subsequent regression analyses, in which our aim was to examine the contribution of mothers’ personal and social resources beyond the child-level factors that were significantly associated with parenting stress. In both child behavior domains, higher scores were associated with higher levels of parenting stress. In addition, mothers’ active engaged coping strategies and perceived social support were both significantly related to lower levels of parenting stress, whereas mothers’ disengaged coping strategies and family dysfunction were statistically significantly related to higher levels of parenting stress.
Bivariate correlations and descriptive statistics for child and family variables.
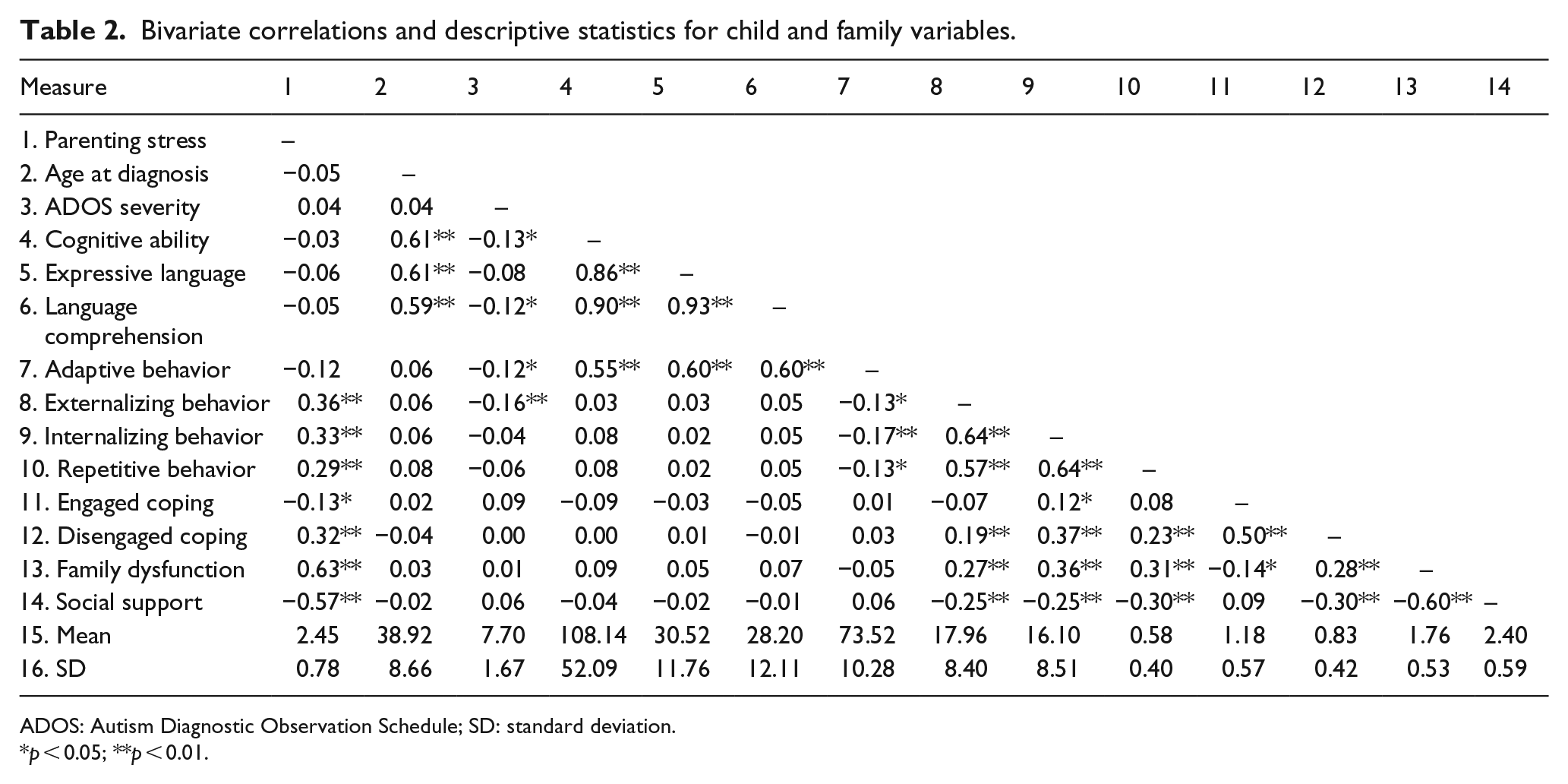
ADOS: Autism Diagnostic Observation Schedule; SD: standard deviation.
p < 0.05; **p < 0.01.
Time of diagnosis (T1)
The results of the T1 hierarchical multiple regression are summarized in Table 3. Findings indicated that the family demographic covariates entered in step 1 did not explain significant variance in parenting stress. In step 2, child variables that were found to be associated with parenting stress significantly accounted for 15% of the variance in parenting stress, R2Δ = 0.15, FΔ(3, 274) = 8.20, p < 0.001. In particular, mothers of children with high levels of externalizing behavior problems had higher levels of parenting stress, with externalizing behavior problems, the only child variable that was significant at this step. In step 3, parents’ personal and social resources together explained an additional 34% of the variance in parenting stress beyond child variables, FΔ(4, 270) = 47.13, p < 0.001. In this step, child externalizing behavior problems remained significant. In addition, mothers who reported high levels of social support and those who utilized more active engaged coping strategies reported lower levels of parenting stress, whereas mothers who utilized more disengaged coping strategies and reported high levels of family dysfunction reported higher levels of parenting stress. The overall model accounted for 51% of the total variance in parenting stress at T1, F(11, 270) = 25.87, p < 0.001.
Results of hierarchical multiple regression for child and family variables predicting parenting stress at T1.
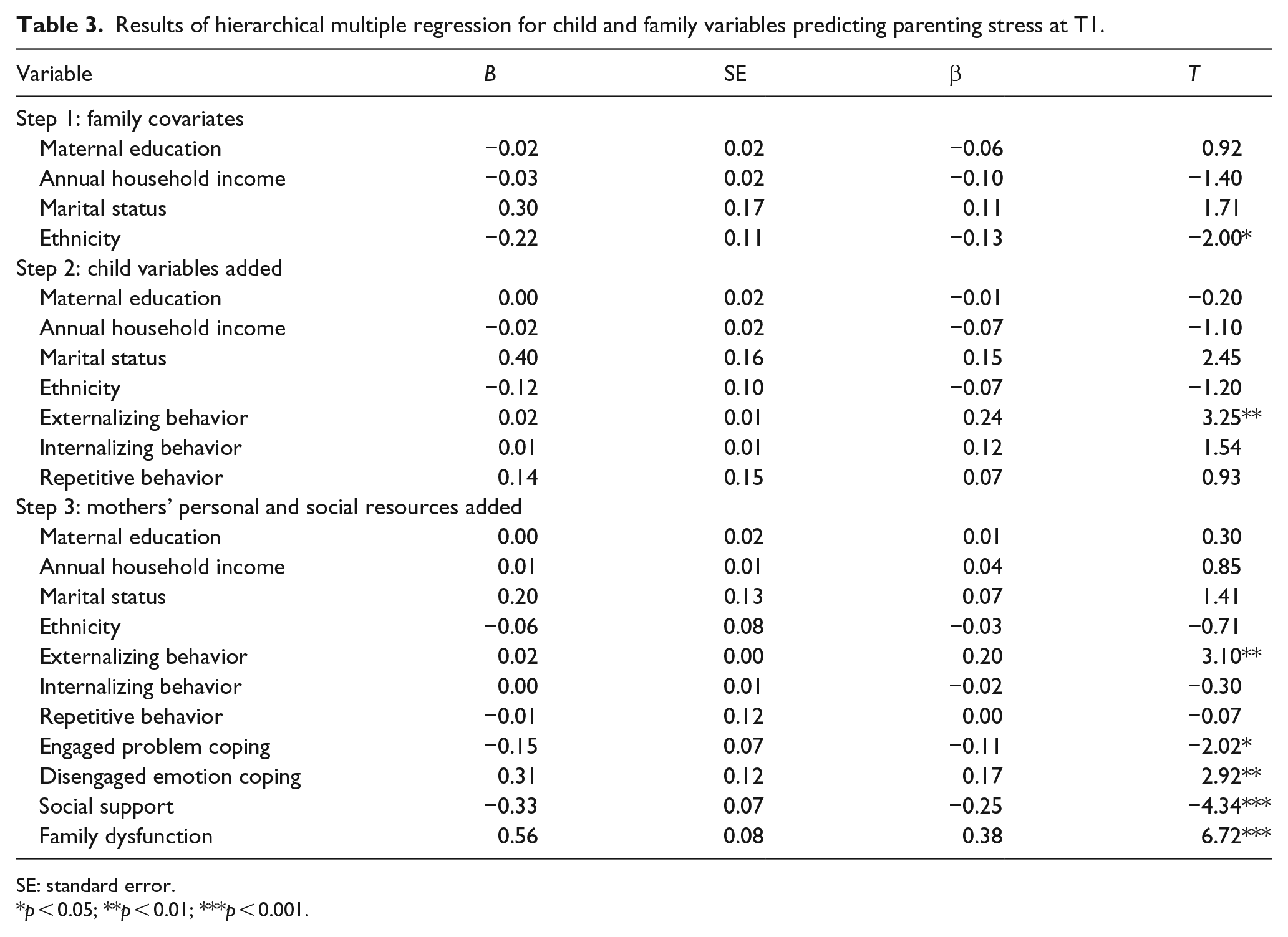
SE: standard error.
p < 0.05; **p < 0.01; ***p < 0.001.
Change over 2 years
Table 4 summarizes the results of the longitudinal hierarchical multiple regression analysis. After controlling for family demographic status in step 1, T1 parenting stress was entered at the second step and accounted for 44% of the variance in parenting stress at T2, FΔ F(1, 182) = 166.402, p < 0.001. The same child and family characteristics that were entered into the T1 regression were entered here at step 3 but failed to explain additional parenting stress variance at T2. Finally, changes over time in mothers’ coping strategies, social support, and family functioning were entered at step 4 and accounted for an additional 14% of parenting stress at T2, FΔ(4, 171) = 17.44, p < 0.001. According to this final model, high levels of parenting stress at T1 predicted increased parenting stress at T2. In addition, with regard to parents’ personal and social resources, higher levels of social support at T1 as well as increased social support over time predicted a decrease in T2 parenting stress. Conversely, higher levels of family dysfunction at T1 and an increase in this variable over time predicted increased stress at T2. In addition, an increase in the use of disengaged coping strategies and a decrease in the use of active coping strategies over time predicted higher levels of parenting stress. The overall model accounted for 69% of the total variance in parenting stress at T2, F(16, 171) = 23.66, p < 0.001.
Results of the final step of the hierarchical regression for child and family variables predicting parenting stress at T2.
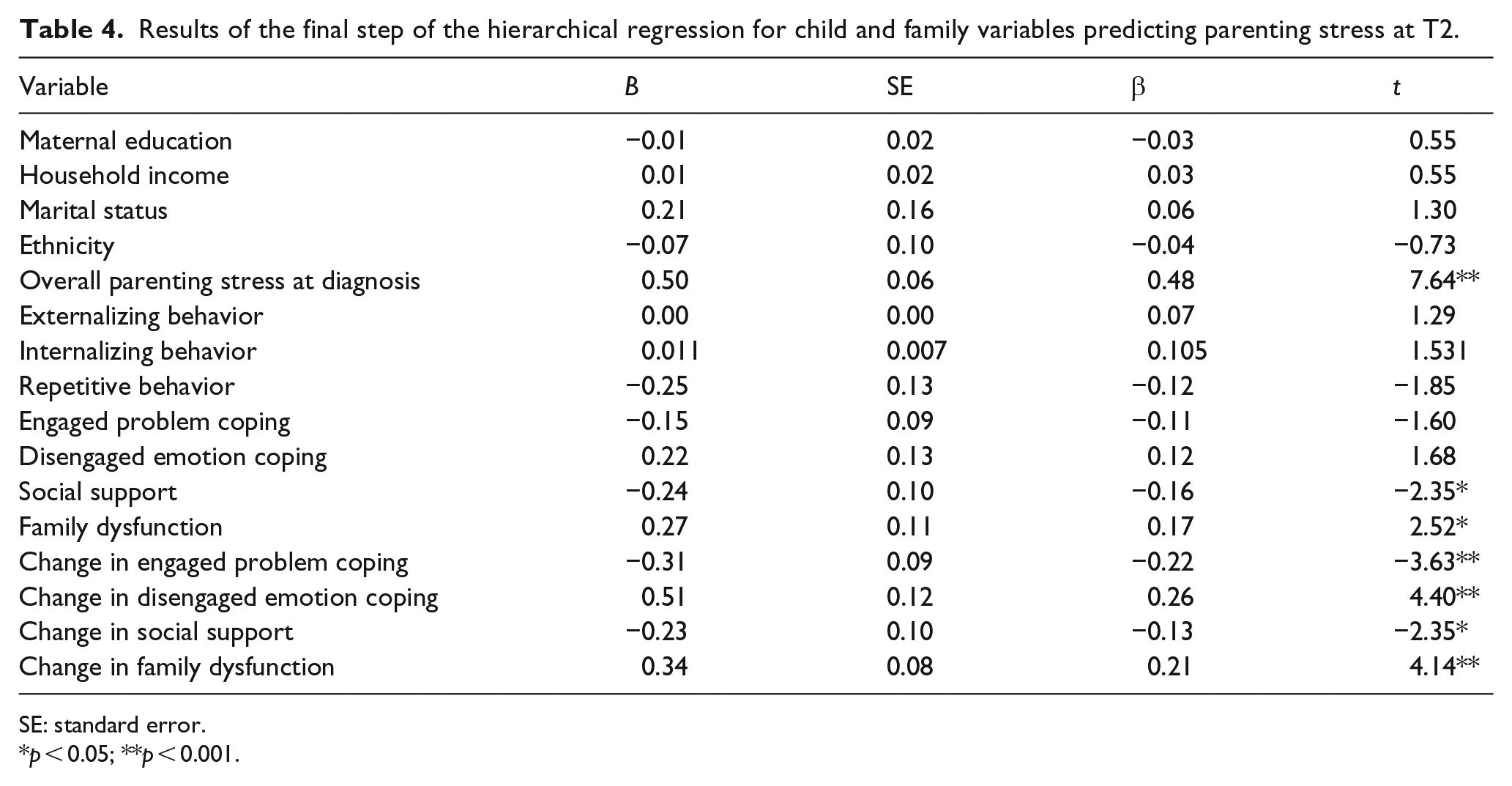
SE: standard error.
p < 0.05; **p < 0.001.
Discussion
The goal of this study was to elucidate the impact of personal and social resources over time on parenting stress in mothers of children with ASD, while taking into account family demographic and child factors that are known to be associated with stress. The results of this study add to our understanding of the complex relations among the child, family, and intrapersonal factors that influence the stress experienced by mothers of children with ASD. In addition, findings highlight that the expression of parenting stress is both multiply determined and dynamic.
Child behavior and parenting stress
Consistent with previous studies, children’s internalizing, externalizing, and repetitive behaviors at the time of diagnosis (T1) were highly inter-correlated, and each was independently associated with parenting stress (Gabriels et al., 2005; Hall and Graff, 2012; Hastings et al., 2006; Lecavalier et al., 2006; Zaidman-Zait et al., 2011). However, when these and other child characteristics were considered together, externalizing behavior was the only child variable that significantly predicted parenting stress at T1, accounting for 15% of the variance. This result echoes that reported in previous studies (Zaidman-Zait et al., 2011, 2014) and in many others that have found a robust association between children’s externalizing behavior and parenting stress (e.g. Hastings et al., 2005; Herring et al., 2006; Lecavalier et al., 2006). Understandably, children’s problems with self-regulation, noncompliance, and antisocial/aggressive behavior are likely to increase the demands of parenting and exacerbate parenting stress. Parents whose stress is primarily related to their children’s problem behavior may benefit from parent training that incorporates specific strategies aimed at increasing parent empowerment and self-efficacy while teaching use of evidence-based strategies for behavior management (e.g. Singh et al., 2014; Whittingham et al., 2009).
Personal and social resources
Consistent with COR theory (Hobfoll, 1989), the current findings also suggest that the persistent stress experienced by mothers of children with ASD is exacerbated in the face of insufficient personal and social resources. Mothers who utilized more active coping strategies (i.e. those aimed at solving a problem, getting help, or constructing positive meanings) and relied less on disengaged coping strategies (i.e. those aimed at avoiding problems and the emotions associated with them), either at the time of diagnosis or over time, experienced lower levels of parenting stress over a 2-year period. This is congruent with past cross-sectional work that identified similar coping style domains and documented their impact on parental pessimism, overall mental health, and, of course, stress (Hastings et al., 2005; Lyons et al., 2010; Pottie and Ingram, 2008; Zablotsky et al., 2013). Similarly, mothers with high levels of social/family support at T1 and those whose social/family supports increased over time experienced less parenting stress at T2. Conversely, mothers whose social/family systems were dysfunctional at T1 and those whose systems became more dysfunctional over time reported increased stress at T2. These results are similar to those reported in previous cross-sectional studies that highlight the important contributions of increased resource availability on parental mental health, mood, and both daily and cumulative stress (Falk et al., 2014; Weiss, 2002; Zablotsky et al., 2013).
These findings highlight the contribution of resource change in the stress process (Hobfoll, 1989). In this study, family functioning entailed open expression of emotions within the family context, collaboration between family members in decision-making processes, acceptance of family members, and the ability to solve problems cooperatively (Byles et al., 1988). Social support was characterized in terms of the perceived availability of family members and friends to assist and provide an emotional support (Weiss, 1974). Based on our findings, it seems that these resources enable mothers to meet the many challenges and demands associated with parenting a child with ASD without experiencing high levels of stress. In contrast, family dysfunction and lack of social support may lead mothers to divert energy away from the management of everyday living and their child’s ASD-related needs and intervention demands. This can leave them with insufficient resources to meet parenting demands, with increased stress as a consequence. Overall, the impact of changes in resources on mothers’ parenting stress emphasizes the importance of incorporating resource loss or resource gain (Hobfoll et al., 2003) as a central mechanism contributing to parenting stress. Moreover, our findings highlight the need to consider the entire family system in which caregiving takes place rather than viewing caregivers as individuals operating in isolation.
Clinical implications
The results of this study and others highlight the importance of personal and social supports that are available to the parents of children with ASD over time. Because some of these supports (e.g. cognitive behavior therapy to teach constructive problem-solving and marital counseling) may come at considerable financial cost, many families will be unable to access them unless they are funded through either public insurers (e.g. Medicaid in the United States) or government agencies. Nonetheless, it seems clear that this would be money well spent, as this study suggests that increases in such supports are associated with decreased parent stress which, in turn, has been found by others to be related to better child outcomes, at least during the early intervention period (Osborne et al., 2008).
The unique contribution of this study is that we were able to document that changes in the family and intrapersonal variables of interest contributed significantly to overall parent stress reduction or exacerbation over time. This suggests that specific, parent-focused interventions aimed at facilitating such changes need to be evaluated as an essential part of any early intervention program. Congruent with Hobfoll’s (1989) COR model, such interventions must have good “fit” with the demands experienced by parents of children with ASD—they cannot be “one-size-fits-all,” any more than child-focused interventions can be so. Parents whose stress is secondary to a reliance on disengaged coping strategies may benefit from interventions designed to teach active, problem-focused coping through mindfulness training or cognitive behavioral approaches (Cachia et al., 2015; Feinberg et al., 2014). Informal social supports can be made available in the form of online or in-person support groups (Clifford and Minnes, 2013; Elfert and Mirenda, 2015), and parents who are experiencing family dysfunction may benefit from marital or counseling services that specialize in this area (Meadan et al., 2010). Some studies have also found that formal social supports such as respite care can also contribute to increased marital quality and decreased parenting stress (Harper et al., 2013; Meadan et al., 2010). Ideally, the need for such targeted, parent-focused interventions should be identified at the time of diagnosis, either by offering parents a menu of supports and simply asking them what they need or by using a screening instrument designed to identify psychosocial risk in parents (e.g. Kazak et al., 2015). Early identification of parents’ needs can lead to early interventions that are designed to provide families with more individualized and appropriate support services.
Limitations and future research
The limitations of this study provide directions for future research. First, only self-report data were used in this study to measure parenting stress, family functioning, social supports, coping strategies, and child problem behavior. Arguably, this is appropriate because parents’ perceptions of both the quality and the quantity of these variables are important. However, some parents may either under- or over-report their own stress or other factors, for a variety of reasons. It would be useful for future studies to use direct observational methods to measure these variables, as a complement to parent-report measures. Second, we were not able evaluate the impact of changes in child behavior at T2 because we did not have child behavior data at this time point. Thus, future research is needed to examine the impact of changes in child problem behavior over time on parenting stress. Third, attrition occurred from T1 to T2, with mothers who continued in the study at T2 reporting higher annual household income. Although the T1 regression analysis failed to find an association between household income and parenting stress (Table 3), additional research is needed to clarify the extent to which socioeconomic status contributes to parenting stress. Finally, because this study only examined mothers’ parenting stress, future studies should gather similar information from fathers, as some studies suggest that paternal stress is influenced by different factors (e.g. financial concerns) than maternal stress (Falk et al., 2014).
Future studies that examine parenting stress over longer time periods are needed to understand the complex relations among child, family, and service delivery variables. Both quantitative and qualitative methods (e.g. Shepherd and Waddell, 2015) would be appropriate in this regard, in order to inform programs that aim to deliver family-centered intervention services about the supports that are needed to facilitate optimal outcomes for both children with ASD and their families. For example, forthcoming data from the Pathways in ASD longitudinal study will allow us to examine the relations among parenting stress, child variables, the services and supports provided to the child and family, and parents’ perceptions of the quality of care. Such longitudinal investigations are needed to understand the mechanisms underlying the developmental pathways of child, parent, and community characteristics and behavior (with implications for tailored interventions).
Footnotes
Acknowledgements
The authors thank all the children and families who participated in the Pathways in ASD study.
Funding
This study was supported by the Canadian Institutes of Health Research, NeuroDevNet, Autism Speaks, the Government of British Columbia, the Alberta Innovates Health Solutions, and the Sinneave Family Foundation.