
Abstract
An autism spectrum disorder can result in considerable stress and confusion for parents as they attempt to understand their child’s problems and obtain a diagnosis. Few studies have explored the parental experience in the context of Chinese culture. The purpose of this study was to understand the experiences of parents in Taiwan of children diagnosed with autism spectrum disorder. In total, 15 parents, 1 father and 14 mothers, were recruited by purposive sampling. This qualitative study used semi-structured interviews and descriptive phenomenological analysis. The findings indicated that parents of children diagnosed with autism spectrum disorder underwent five coping experiences during the diagnostic process: (1) uncertainty and difficulty understanding their child’s behaviour, which occurred during the pre-diagnosis phase; (2) obligation to obtain professional services; (3) anxious searching for a second opinion, which occurred during the diagnosis phase; (4) acceptance and fortitude and (5) further adjustment during the post-diagnosis phase. Our findings add to our understanding of how parents experience the diagnostic process, which could improve medical professionals’ counselling and support for parents at the stage of obtaining a diagnosis for their children.
Introduction
Autism spectrum disorder (ASD) is a complex neurological condition characterized by limitations in communication, social interaction, restricted interests and repetitive behaviours. The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) revised the diagnosis of ASD to include the following pervasive developmental disorders (PDDs): autistic disorder, Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorder–not otherwise specified (PDD-NOS) (American Psychiatric Association, 2013). Thus, symptoms in the category of ASD can vary in severity and functional impairment, ranging from the severe symptoms of classical autism to milder symptoms of no cognitive impairments or developmental delays, such as Asperger syndrome. The prevalence of ASD worldwide has increased from 1 in 150 in 2000 to 1 in 68 in 2012 (Centers for Disease Control and Prevention (CDC), 2016). The prevalence rate of ASD in Taiwan in 2007 was slightly more than 1 in 100 persons (Hsu et al., 2012).
Obtaining a diagnosis of ASD can be difficult due to the complexity of the developmental and behavioural symptoms of ASD. Many parents of children with ASD report dissatisfaction with the diagnostic process, which has been reported for parents in France (Chamak et al., 2011), the United Kingdom (Crane et al., 2016), the United States (Estes et al., 2009), Hong Kong (Ho et al., 2014), as well as in Taiwan (Lin et al., 2008). Dissatisfaction often results from delays in diagnosis, which may be attributed to (1) the heterogeneity in the clinical presentation and development of autism in different children, (2) limitations of assessment (inadequate assessment methods, time required for assessment, reliance on parental reports), and (3) lack of available specialized services (Crane et al., 2016). Delays in receiving a definite diagnosis can lead to lower levels of parental satisfaction (Howlin and Moore, 1997), which can further affect the support and intervention strategies needed by these children and their family (Webb et al., 2014). These factors that contribute to dissatisfaction with the diagnostic process can lead to frustration and stress for the parents. A lengthy or delayed diagnostic process can also cause parents to experience increased anxiety as well as distrust towards healthcare providers (Harrington et al., 2006; Ho et al., 2014).
Although parents are typically aware there is a ‘problem’ with their child, it often takes multiple referrals before obtaining a diagnosis of ASD and the average delay between parents first seeking help for their child and receiving a diagnosis is 2–3 years (Chamak et al., 2011). Crane et al. (2016) reported that the average delay in the United Kingdom is 3.5 years. In Taiwan, all newborns and toddlers are followed at well baby clinics for routine vaccinations and regular health checks, which are reimbursed by Taiwan’s National Health Insurance Programme. If a developmental delay is noted, the paediatrician will refer the child to a child psychiatrist for further assessment and diagnosis. In Taiwan, a registered child psychiatrist is the only professional eligible to issue formal certified documents for a diagnosis of ASD. However, due to an insufficient number of child psychiatrists in most parts of Taiwan, parents seek assessments and confirmative diagnoses from general psychiatrists and doctors in rehabilitation departments (Taiwan Society of Child and Adolescent Psychiatry (TSCAP), 2016). Diagnoses after 2013 are based on criteria established by the DSM-5. However, these developmental delays may not be immediately identified.
A reliable diagnosis of ASD can be obtained for children as young as 2 years of age; however, most children are not diagnosed until after 4 years of age (Christensen et al., 2016). The type of ASD can also influence the mean age at which a diagnosis is made: autistic disorder: 3 years, 10 months; PDD-NOS: 4 years, 1 month; and Asperger syndrome: 6 years, 2 months (Christensen et al., 2016). In children without intellectual disability or other coexisting impairments, the disorder may not be recognized and identified until school age or adulthood, when their impairment in social function becomes obvious as a result of more social interactions (Coleman and Gillberg, 2012).
Most parents emphasize the need for a quicker and easier route to diagnosis (Osborne and Reed, 2008). Confirmation of ASD allows parents to begin the process of acceptance of their child’s diagnosis; they can begin to acquire appropriate treatment plans, obtain interventional services and restructure their lives to accommodate the challenges of parenting a child with ASD (Mansell and Morris, 2004).
The culture in Taiwan differs from Western cultures and these differences may contribute to a delay in diagnosis. Social skills in childhood are not as highly valued as cognitive development in Taiwanese culture, thus delays in social development may not be an immediate concern for parents of children with ASD (Wang et al., 2012). Taiwan is a Han-Chinese culture, which is deeply influenced by Confucianism. Therefore, the process of accepting a diagnosis of ASD for parents in Taiwan may be more difficult as a result of values associated with ‘filial piety’ (Tait et al., 2014). Less than half of Taiwanese parents perceive genetics as the cause of their child’s ASD (Chen et al., 2015); therefore, the concept regarding the aetiology of autism may be cultural, as people with genetic/genomic disorders are socially stigmatized in Chinese cultures (Sleeboom-Faulkner, 2010).
The process leading up to and arriving at a diagnosis of ASD requires unique coping mechanisms for parents of children with ASD (Ludlow et al., 2011). Studies on the coping experiences of parents of children with ASD in Asian cultures and Taiwan are limited. Wang et al. (2011) found that in China, coping strategies of parents of children with ASD included acceptance, active coping, planning and ‘help-seeking’. Lin et al. (2008) studied the coping mechanism of parents in Taiwan with children who had been recently diagnosed with autism and found personal adjustments, initiating effective treatments for their child and strong social support helped them to cope. Studies on the experience during the diagnostic process are even more limited. Ho et al. (2014) studied the parent–professional partnership in Hong Kong during the process of seeking a diagnosis of ASD and noted parents expressed feeling ‘lost’ and ‘frustrated’. Another qualitative study conducted in Sweden explored how parents experience the diagnostic process for children with ASD prior to diagnosis and at a 2-year follow-up (Carlsson et al., 2016). Parents expended considerable energy assessing and reassessing their knowledge about their child’s disorder while simultaneously ‘seeking knowledge’, ‘trusting and challenging experts’ and feeling ‘empowered but alone’.
The responsibility of raising a child is heightened when the child has a disability, and stress is significantly greater for parents of children with ASD than other disabilities (Wang et al., 2011). Because the process of accepting a diagnosis of ASD differs in Taiwan, coping with the process of diagnosis may differ as well. Currently, there are few studies on the experience of obtaining a diagnosis for children with ASD in Han-Chinese society. Therefore, the aim of this study was to understand how parents in Taiwan experienced the diagnostic process prior to, during and after their child was diagnosed with ASD in order to understand their experiences of emotional coping, acceptance of the diagnosis of ASD and behavioural changes. We focused on intellectually able children with ASD because studies suggest parental stress may be greater for parents with children who demonstrate fewer developmental and behavioural problems (Crane et al., 2016; Huang et al., 2014; Siklos and Kerns, 2007). We believe an understanding of the experiences of coping with the diagnostic process could improve support and guidance from healthcare professionals for parents of children with ASD.
Method
Ethical approval
Ethical approval was obtained from the Institutional Review Board of the Research Committee of Chang Gung Memorial Hospital (103-6377B) prior to conducting the study.
Qualitative design
This retrospective qualitative study employed a descriptive phenomenological design. The aim of this study was to understand the parent’s subjective experience, emotions and adjustments encountered before, during and after the process of obtaining a confirmed diagnosis of ASD for their child. A descriptive phenomenological methodology was applied (Giorgi, 2012), which involves ‘direct exploration, analysis, and description of particular phenomena, as free as possible from unexamined presuppositions, aiming at maximum intuitive presentation’ (Spiegelberg, 1975: 57).
Participants
We recruited a purposive sample of 15 parents from the outpatient child psychiatry clinic for children with ASD at a medical centre in northern Taiwan. This outpatient clinic has nine psychiatrists and serves approximately 1000 patients monthly; approximately 10%–15% are children with ASD. Parents of children with ASD who were intellectually able were invited to participate in the research by the children’s physician during the interval of the study. If the parents agreed to participate, a research assistant contacted them. Parents were further selected if they not only met the inclusion criteria but also represented a broad range of socioeconomic status (SES) and age of children with ASD, so as to obtain a more diverse population base. Inclusion criteria were the parent’s child was diagnosed with ASD, the child was in school and between the ages of 6 and 19 years and the parent could communicate in Mandarin. Children were diagnosed using the Diagnostic and Statistical Manual of Mental Disorder (4th ed.; DSM-IV), which differentiated subclasses of ASD, or the DSM-5. Parents were excluded if their child had intellectual or language impairments. Parents were assured of anonymity and confidentiality and the right to terminate the interview or withdraw from the study at any time and for any reason prior to obtaining written consent. The 15 participants included 14 mothers and 1 father; mean (M) age was 42.13 years (range = 34–52 years; standard deviation (SD) = 4.50 years); 11 (73.3%) were in partnered relationships and most (n = 14) had greater than a high school education. Participants had 16 children with ASD, aged 6–19 years (M = 13.25 years, SD = 4.05 years), 13 males and 3 females (two of the children were fraternal twins). Details of the participants and the children are shown in Table 1. The name of the participant’s child was replaced with a pseudonym.
Demographic data of parents and demographic and clinical data of children with autism spectrum disorder.
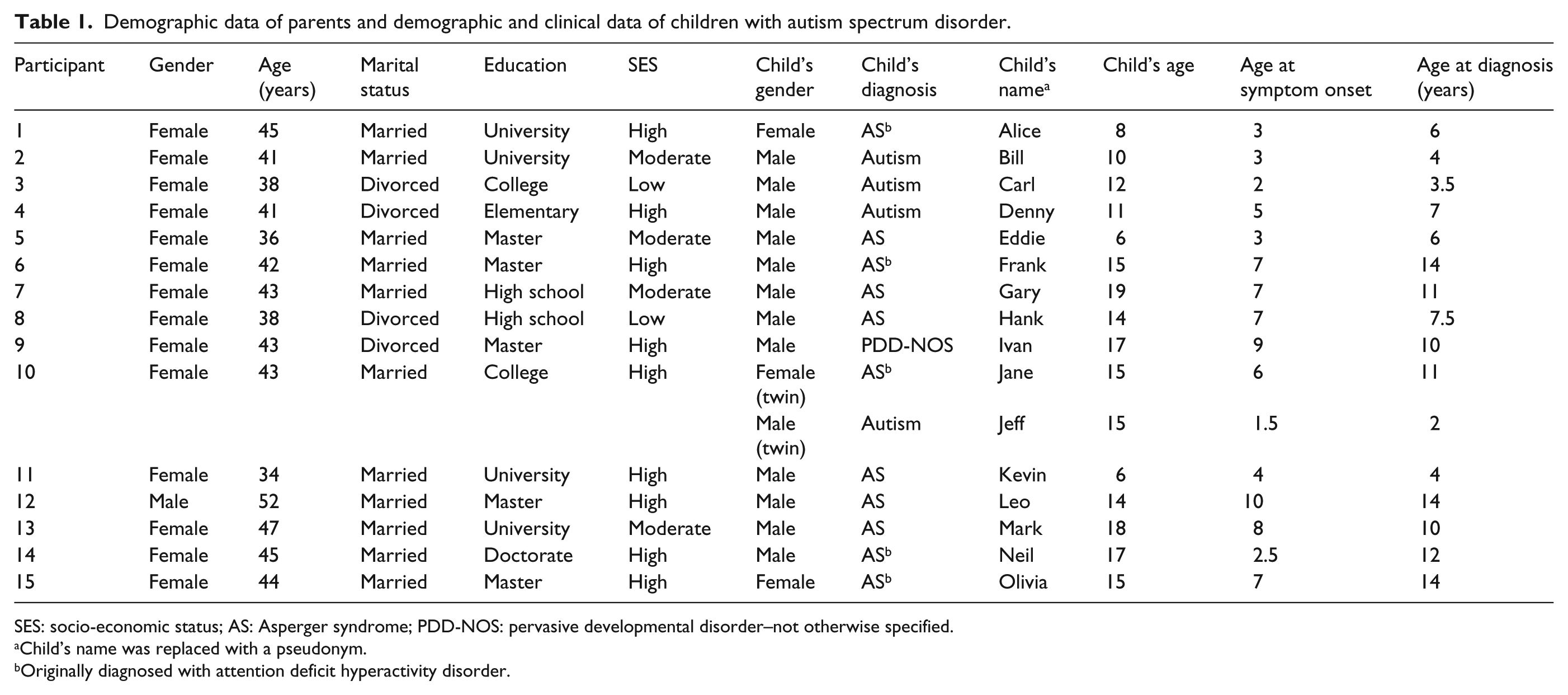
SES: socio-economic status; AS: Asperger syndrome; PDD-NOS: pervasive developmental disorder–not otherwise specified.
Child’s name was replaced with a pseudonym.
Originally diagnosed with attention deficit hyperactivity disorder.
Data collection
Data were collected with semi-structured face-to-face in-depth interviews. Participants were contacted via telephone and a date was scheduled for the interviews. Interviews were conducted within 2 weeks of telephone contact at a medical centre in Linkuo, Taiwan where the children were diagnosed and treated for ASD. All interviews were conducted in a private hospital interview room by the first author (K.-Y.C.). Interviews were audiotaped and transcribed verbatim within 48 h. We obtained clinical data for each child from his or her parent. In order to accurately transcribe the audiotaped interviews, no more than two participants were interviewed each week.
Four experts in ASD developed a semi-structured interview guide: two paediatric psychiatrists and two PhDs, a psychologist and a nurse. The guide was revised following a pilot study with two parents. The interviews followed a format exploring the experience of parents during the process of their child’s diagnosis of ASD. The interview guide was used to guide the participants’ responses, rather than the researcher’s preconceived ideas of the experience. The interviewer provided a supportive and empathetic attitude and was genuinely interested in the participants throughout the interview. This format allowed the researcher to build rapport with the participants, which facilitated an open and free exchange about the participants’ experiences, both positive and negative.
The interview started with an open-ended question: ‘When did you start to notice that your child was different from other children?’ Additional questions were asked in response to answers given to the above question, and the format of the interview was developed according to the participant’s responses. Participants were asked about their experience of the diagnostic process prior to, during and after diagnosis. Follow up questions included ‘What steps did you take then?’ and ‘Were there any problems you encountered during the process of diagnosis?’ These questions were asked in order to gain an in-depth understanding of the phenomenon and to understand the situation participants encountered during the diagnostic process. The interview took an average of 50–70 min. The last four participants were interviewed two weeks following their first interview to confirm data saturation (Strauss and Corbin, 1998) had been reached with the 15 participants; no new themes were revealed, and therefore, no new participants were recruited. Data were collected from Chang Gung Children’s Hospital in Taiwan between March 2015 and January 2016.
Data analysis
The steps of analysis were based on the descriptive phenomenological approach developed by Amedeo Giorgi (2012), which is a process allowing researchers to clarify and interpret interview data. During this process, K.-Y.C performed the following steps: (1) all written transcripts were read in order to obtain a sense of the whole; (2) the transcripts were reread to determine significant statements (meaning units) regarding the phenomenon of ‘the parental experience of their child being diagnosed with ASD’; (3) significant statements were transformed into psychological expressions related to what the participants said and converted to the third person; (4) these third-person statements were converted to descriptive expressions of how the participant experienced the phenomenon, which is known as ‘imaginative variation’ and finally, (5) descriptions of the qualities of the raw data, or the essence of the common coping experiences of the parents, was formulated into five themes. A bilingual expert in qualitative research, H.-L.C., translated the quotes and themes from Mandarin to English. All authors validated the equivalence of the Mandarin and English themes by discussion with H.-L.C.
Trustworthiness
Trustworthiness of the data was maintained using criteria outlined by Lincoln and Guba (1985). K.-Y.C. conducted all interviews, had 20 years of experience caring for children and adolescents in paediatric nursing and published a qualitative study on a related topic, which increased credibility of the data. Data analysis was discussed periodically with two child psychiatrists, one of which had 30 years of experience caring for children and adolescents. This allowed for input from multiple perspectives regarding the meaning units, themes, definitions and descriptions that emerged from the data.
Transferability of the data was increased by the heterogeneity of the participants’ children: different gender, developmental age (preschool, primary school and adolescent stages), age at diagnosis and various comorbidities such as ASD only, ASD with attention-deficit hyperactivity disorder (ADHD) or ASD with obsessive–compulsive disorder (OCD), for example. Regarding the dependability and confirmability, formal audit trails were established during the analysis; one paediatric nurse and two psychiatrists audited the raw data, meaning units and themes.
Findings
Clinical characteristics of the children with ASD
The mean age when symptoms were initially noticed by the parents (symptom onset) was 5.31 years (range = 1.5–10 years; SD = 2.67 years); mean age at diagnosis was 8.5 years (SD = 3.90 years) (Table 1). The mean delay in obtaining a diagnosis was 3.19 years (SD = 2.75 years, range <1–9.5 years). The children had been diagnosed with autism (n = 4), PDD-NOS (n = 1) or Asperger syndrome (n = 11). Diagnostic delays were seen in eight children (range = 3–9 years), and five of these children had originally been diagnosed with ADHD.
Themes
Five main themes emerged from the analysis of the interview data, which described the parents’ experience of their child being diagnosed with ASD. Diagnosis of ASD involves three stages: pre-diagnosis, diagnosis and post-diagnosis (Mansell and Morris, 2004). The experience during the pre-diagnosis stage involved trying to make sense of their child’s behaviour in order to find out of ‘what was my kid’s problem’. The diagnosis stage occurs when a specialist in ASD examines the parent’s child in order to obtain a confirmative diagnosis. In the post-diagnosis stage, the child is referred for further treatment and special education. Participants experienced a variety of stresses when their children began to manifest unexpected developmental or behavioural problems, even before any diagnosis was given. Although each parent reacted to the stresses in a unique and individual manner, we noticed that all parents in this study experienced a similar trend of changes on the route to a definitive diagnosis of ASD for their child.
The first theme, which occurred during the pre-diagnosis phase, was ‘uncertainty and difficulty understanding’. Two themes emerged during the diagnosis phase: ‘obligation to obtain professional services’ and ‘anxious searching’. The post-diagnosis phase involved ‘acceptance and fortitude’ and ‘further adjustment’.
Uncertainty and difficulty understanding
In the pre-diagnosis phase, parents experienced uncertainty about their child’s development, cognition and behaviours when compared to other children. It was difficult for them to accept that there might be ‘something wrong’ with their child. They experienced anxiety because their child was not developing or behaving like other children. Parents reported confusion and doubt about the seriousness of the problem. Rather than accept the fact that their child might need medical attention, many parents demonstrated an attitude of denial.
For some parents, this uncertainty was a result of inadequate knowledge about typical variations in child development. These parents were unaware there was a problem, and warning signs were initially overlooked. The concept of ASD is relatively new in Taiwan, and public awareness of symptomology is limited. This lack of knowledge is reflected in the following comments:
I was busy at work then, and I thought there is nothing serious … just visit the doctor for a couple of times and he will be okay. I did not take his problem seriously … (Jeff’s mother) He was our first kid, I did not know about the usual development process of a kid. Like what can he do at certain months? I just did not know. (Denny’s mother) You know this kid was more stubborn than others, but then we just kept observing. You know she is different, but we just could not tell what was different. (Alice’s mother)
Parents were uncertain about the seriousness of their child’s inability to behave, communicate or learn relative to other children. Some parents thought their child’s problems with conduct or cognition was due to the child’s temperament, a childhood behavioural disorder or merely a trivial lag in the typical developmental process. Olivia’s mother thought her child was ‘difficult’, and the mother of Hank thought her son had Tourette syndrome. Sometimes, the complex nature of ASD puzzled doctors or teachers unfamiliar with it, resulting delays in referrals for assessment:
We brought him to visit a doctor, and the doctor gave us some questionnaires. The doctor said he was borderline ADHD, and said all we had to do was wait and see. So, we did not care about his problem anymore … (Ivan’s mother) He would just insist on reading books, but I did not observe any other problems. The teacher noticed that he had some problems with pronunciation, but he was okay in other aspects, it was like he had a learning disorder. (Gary’s mother) We underwent many evaluations, and talked to the doctor. He said the teacher was just complaining about his personality traits. And I thought the kid was just very smart, and not [a problem] so we just kept observing. (Frank’s mother)
Some parents chose to avoid admitting their child might have a specific developmental disorder, despite observing delays or impaired social behaviour, which prevented them from understanding the underlying aetiology of their children’s problems. These parents adopted a ‘common sense’ approach to manage the situation, procrastinated on visiting a doctor or believed their child had a conduct problem. Kevin’s mother noticed her son was slow in development and said ‘(we) had thought about taking him to visit a doctor, but eventually we did nothing’. Other parents shared similar experiences:
I was worried about his development since he was two years old. But every time I want to bring him to the doctor’s place, my husband and my father-in-law would stop me, saying that I worry too much. (Bill’s mother) They asked us to send the kid to a special education system. You know, the place for those kinds of kids. My husband was angry and told them we didn’t need their help. We have our own way. (Jeff’s mother)
Parents experienced anxiety when they could not understand whether their child’s atypical development was just ‘different’ or if there was a biological explanation. This uncertainty was stressful, and one parent wondered whether her child’s behaviour was a result of poor parenting. Alice’s mother described her experience of uncertainty:
You know this kid was very stubborn, she was different, but we did not know what was wrong; so we just kept observing her … I know every kid is different. My kid was ok in speech development, but she would just listen quietly, play by herself quietly. This is very different from other children. At those moments, you would become very scared … One doctor told us that she was not a case of ASD. Then I would think, if she is not an ASD kid, then she should act like other children, she should be able to empathize with people, to have appropriate behaviour during group activities, but she just could not meet the standard. Then I started to wonder if it was a parenting problem … yes, you would start to wonder if it is your own problem. I wish we had known about the right diagnosis earlier, which would have been a relief! (Alice’s mother)
Obligation to obtain professional services
Although the National Health Insurance in Taiwan provides convenient and inexpensive access to professional help for children with ASD from paediatric psychologists, child psychiatrists, physical and occupational therapists or speech therapists, parents were reluctant or unaware of the importance to seek out assistance specific for ASD prior to receiving a confirmative diagnosis. When parents could no longer cope with the behaviours and developmental delays manifested by their children, it was then that they understood they had an obligation to seek professional help in order to gain an understanding of the underlying aetiology of their child’s symptoms and obtain a confirmative diagnosis of ASD for their child.
The acceptance of professional services was sometimes a result of external pressure for some of the participants. When behavioural problems were too severe and disruptive at school, teachers often demanded that a professional assessment and consultation be obtained. Therefore, for these parents, it was the external pressure from school that initiated their search for professional help:
He was expelled from the kindergarten, twice, for his behavior. Only then did I realize how serious the problem was. So I quit my job to stay by him, and when I really understood how severe his problem was afterward I became a volunteer worker and involved in his school activity. Finally, the school authority could not cover up the strong demand from other parents, and told us about the seriousness of his problem. (Jeff’s mother) Why did we come to the hospital for help? When my kid was punished at school for his behavior for the first time, I decided to bring him for diagnosis. (Frank’s mother)
Some parents were motivated by internal pressure to look for a diagnosis for their child because they had finally accepted that something was ‘wrong’ with their child. This awareness would allow them to gain insight and better understand their child’s problems. It was at this point parents could acknowledge their child needed medical attention. Olivia’s mother said, ‘… I really sensed that this kid had a problem’. Hank’s mother said, ‘Things happened one by one, so we decided to bring him to a child psychiatrist’s place for diagnosis’. Alice’s mother said,
You know she was very fidgety, had a low tolerance for frustration. She would become very moody all of a sudden, and could not do her homework; there is nothing you can do. She had tantrums, was very irritable, or not okay with something. I knew she was different. I wanted to know why she was like that.
Parents’ obligation to accepting professional services was influenced by external demands and criticisms of others. Parents either hesitated to understand the underlying aetiology of their child’s atypical cognitive and behavioural development or demonstrated high tolerance and attributed the situation to something ‘he will grow out of’ or ‘it is normal’.
Anxious searching
When a diagnosis was given to the parents, they did not always agree with the specialist’s assessment. Some parents wanted a second opinion before they could accept the diagnosis. Parents searched for information that might refute the diagnosis, typically seeking ‘expert’ opinions from other specialists:
I started doctor shopping then. I bought a book by that famous professor, the one who wrote books about autism and developmental delay. (Denny’s mother)
The self-help-type parents looked for information on the Internet or from the library or they attended parent groups or lectures to gather information about their children that would suggest they did not have ASD:
He had so many problems then. No one can give me an explanation; I had to look over his problems in the books. (Jane’s mother)
Other parents travelled in desperation of obtaining help or new information. They would travel long distances for a consultation with a well-known physician, they considered non-traditional medical help and treatment and participated in alternate treatment programmes. Denny’s mom said,
I would take a train to see this doctor at I-Lan … and … what was the place I said we went for classes? Little Sun class and … what was its name again? I went to so many places; there were a total of four clinics! I would take him to different classes. Eight classes per week, and you have no idea how exhausted I was.
Parents who were desperate for a different diagnosis had children who did not respond well to the prescribed treatments for ASD. They were willing to let their child to participate in treatment, but had a pessimistic attitude that their child would improve; they did not have faith in medical help. Some parents demonstrated a wish-fulfilling fantasy: the unrealistic expectation of a complete cure:
We know there is no quick fix. If anyone can help us, it is fine. If not, it does not make any difference. Really, we are just treating a dead horse as if it was still alive. … Then we brought him to a doctor. No matter what the doctor prescribed, there was no improvement in his symptoms. We were very helpless then. We had tried every way, and on the brink of giving up … We were out of ways. This is the saddest part, we had no idea what to do next, we wanted to give up. All the doctors said he was hyperactive, hyperactive, hyperactive, but medication is just no use. (Ivan’s mother)
Anxious searching for a second opinion sometimes ceased when parents became satisfied with the doctor’s comments, attitude, explanation or support:
I once consider travel to the medical centre was too time consuming. But I thought the doctor we were seeing there was smarter, more exact in interpretation. Now I think the medical centre is really not that far away. (Frank’s mother)
The search for a second opinion ceased either when parents were satisfied with the service or help the doctor provided or simply because parents or their child were exhausted, ran out of energy, time or money.
Acceptance and fortitude
During the post-diagnosis phase, participants accepted their child and the diagnosis of ASD and were less anxious and uncertain about the difficulties they encountered, which allowed them to accept their role as a parent of a child with ASD. Although many parents said they knew all along that their child fit somewhere on the autism spectrum, getting an official diagnosis for families was the beginning of a new era. An official and confirmative diagnosis provided the parents with new concepts and alternative views regarding their children; some parents eventually developed new perspectives and attitudes regarding ASD. Understanding the reasons for behavioural disruptions and developmental delays gave them a sense of relief:
After we acquired the confirmative diagnosis, the teacher and I were both relieved. (Frank’s mother)
The newly acquired knowledge and facts about ASD, along with the sense of responsibility of caring for a child with a known aetiology, ASD, provided emotional strength, which also empowered participants in their role as a parent of a child with ASD:
Once you know that some of his symptoms are just due to his ASD problems, you can accept him more. Otherwise, you would just keep on asking yourself, why he behaves this or that way. (Hank’s mother) You now know that those symptoms are just his ASD symptoms, then you are more ready to accept him. Yes, otherwise, you will just keep on asking yourself, why is he acting that way? Why? (Gary’s mother)
Parents also became aware that they were not alone; they and their children belonged to a community. Now that the diagnosis was confirmed, parents could acquire more accurate information, professional assistance and support from support groups. They were able to develop skills to better communicate and handle their child’s behavioural problems. Some parents ceased blaming themselves for their child’s ASD and experienced a sense of relief. Leo’s fathers said, ‘The big issue is still on the medical side … once this problem is solved, it is a great relief for the parents’. Other parents said,
I cried for three months in the beginning, but after that I was better, and started to put myself together. Yes, you must let it go off your head. Of course there are stresses, but once you set it in your mind that there must be things that you can do to help him, you are ok. (Jeff’s mother) I want to thank the teacher for sending out his information. After the diagnosis was confirmed, I feel that his environment is friendlier towards him. He is accepted. And after he is accepted, he has less aggression. (Ivan’s mother)
Part of the change in attitude for participants was a sense of empowerment. Parents discarded their mixed feelings towards their child’s disorder: the feeling of guilt about their child’s ‘unknown situation’, which many blamed on parenting or environmental causes, and uncertainty about what to do next. Parents were empowered by the arrival of a confirmative diagnosis and developed new strengths and visions about a brighter future. They began to ‘take things into their own hand’:
I really did not know what ASD was. After he was diagnosed, I started to Google things about ASD, and was more able to understand what the doctor was talking about. (Denny’s mother) I would always tell the teacher first. The teacher must know beforehand about her problem. So what with the labeling. Just in case our kid encounters a big problem at school, at least people know she did not do that on purpose. (Alice’s mother)
Not all parents were able to readily accept the diagnosis of ASD, and family members did not always have the same experience during the post-diagnosis phase. Carl’s mother reported that her experience of her son’s diagnosis was different from her husband’s. Although she accepted the diagnosis and had a better understanding of her son, her husband ‘kept him away from his friends’.
Further adjustment
Post-diagnosis, parents made further adjustments as they transitioned from ‘what is wrong with my kid’ to acknowledging they had a child with ASD. Further adjustments included making long-term goals, having appropriate responses to challenging behaviours and developing more realistic planning for treatment outcomes. Participants adapted treatment perspectives that were goal oriented because of their concrete concept of ASD. The journey for long-term treatment programmes and realistic future planning began at this stage. Parents typically focused on three areas: planning for the future, adjusting expectations and initiating new hopes.
Planning for the future included their child’s schooling, career and social adjustments, and parents’ attitudes improved as their child progressed with treatment. Carl’s mother said, ‘I want to give him as much treatment as he can get, as it makes a lot of difference if you start treatment early’. Other parents said,
Medical help gave us a sense of direction. We now know we are on the right track. We know that the doctor’s observation is helpful. We are now more able to predict what we should expect next. (Leo’s father) I would let him have as much as therapy as he can. He is still young, and you know, treatment at young age makes lots of differences. (Carl’s mother) I found out that my kid started to improve after I got involved, so I became more enthusiastic in his treatment. I would go on the Internet to look for things related to his illness. (Jeff’s mother) You have to let her out into society. You cannot tie her up at home for the rest of her life. So, I was very active in fighting for her right to enter school. (Alice’s mother)
Adjusting expectations occurred as participants gained more knowledge about ASD and understood the capabilities of their child; they were more accepting of their child. Frank’s mother said, ‘I know he still has his good part, but you just cannot expect him to be like other kids’. Carl’s mom understood he needed to acquire abilities to become independent, saying ‘I want to help him develop more skills, because he will be on his own in the future, I cannot leave him much money after I die, he will be on his own’.
Initiating new hope may have been the most important step in coping with having a child diagnosed with ASD. Accepting the diagnosis of ASD allowed parents to adopt a new and hopeful vision for their child’s future. Confirmation of ASD allowed parents to understand the aetiology of the disorder and they were better able to envision the future hurdles they would need to overcome. As parents became aware of their child’s capabilities, their own negative emotions diminished. Focusing on their child’s capabilities, parents were better able to face and cope with stresses, use resources more effectively and set realistic goals for their children. Leo’s father was hopeful about his son’s ability to progress in school:
I now know that he will only be more mature after high school … getting more mature then. Right now he is really lagging behind in terms of interpersonal skill … He is so way behind other kids in social skills now.
Mark’s mom expressed an optimistic, hopeful attitude about her son’s future when she discovered her son was interested in cooking:
We do not expect him to study in a famous school, we just hope he will learn a skill, and maybe open up a small business. His father wants to open up a small restaurant, so, I told him that after he graduates, he can work with his father, taking care of plants, and also work in the restaurant. (Mark’s mother)
Some parents had not reached the final stage of ‘further adjustment’ at the time of the interviews. One boy (Eddie) had only recently received a diagnosis of ASD and his mother reported her husband was still in denial, saying, ‘I don’t think he has any problem’. Another parent obtained a diagnosis for her son 5 years earlier. Neil’s mother expressed her continuing stress in the following statement:
I told my husband once that I hoped he (Neil) died in a car accident so we had no responsibility for parenting. I admitted I had that kind of thought once but I found my way to overcome it. I know I still had to live in reality. (Neil’s mother)
These parents vacillated between feeling secure and optimistic about the future; while at other times feeling lost and full of anger, not knowing what to do with their child with ASD.
Discussion
The experiences of parents of children with ASD following diagnosis have previously been reported (Mancil et al., 2009; Wang et al., 2011). In contrast, our study focused on parents’ experiences during the three phases of obtaining a diagnosis of ASD: pre-diagnosis, diagnosis and post-diagnosis. To our knowledge, this is the first study to explore the experiences of Taiwanese parents over the full spectrum of the diagnostic process. Five themes described how 15 parents experienced while obtaining a confirmative diagnosis of ASD for their child.
Participants experienced uncertainty and difficulty understanding during the pre-diagnosis stage, which involved parents’ attempts to determine what constituted a ‘normal’ child. Most parents were aware their child had behavioural or developmental difficulties as early as 3 or 4 years of age; however, the average delay before a confirmed diagnosis was obtained was 3.19 years. This is similar to the time delay reported by Crane et al. (2016) for children with ASD in the United Kingdom. Parents lacked understanding their child’s behaviour due to insufficient knowledge about ASD, underestimating the seriousness of their child’s difficulties and avoidance. The overlapping symptoms of ASD with other disorders, such as Tourette syndrome, ADHD, OCD and other anxiety disorders, add to the difficulty in obtaining an accurate diagnosis.
Most parents experienced bewilderment or confusion towards their child’s conduct and developmental delays, which was stressful. Fear and anxiety regarding impending truth are universal in many illnesses, and our participants’ experiences are similar to those of others faced with major difficulties (Benson, 2010; Mancil et al., 2009). However, the extended interval of uncertainty and ambiguity may be a complication of the Chinese culture in Taiwan and may have added to the lengthy pre-diagnosis phase. Studies suggest Chinese families of children with developmental disabilities (Lam and Mackenzie, 2002) and ASD (Tait et al., 2014) use avoidance as the dominant coping strategy. Shyu et al. (2010) reported Taiwanese parents of children with ASD also frequently employ avoidance. Wong (2009) noted that ASD is still considered a disorder with a strong stigma in Chinese society, which could also contribute to a delay in seeking a confirmed diagnosis. Taiwanese mothers of male children with ASD feel they are to blame when their child is diagnosed with ASD (Hsu et al., 2015). Chinese culture emphasizes the importance of lineage prolongation and expansion, and sons carry the name of the family (Liu, 2001). In our study, 70% of the participants were mothers of male children. Avoidance of obtaining a confirmative diagnosis and maintaining uncertainty about their son’s diagnosis may have allowed mothers to avoid self-blame or doubts and criticism from other family members about the possibility that their son was unable to maintain the family lineage.
The subtle behaviour and developmental symptoms of ASD can also contribute to a delay in a confirmed diagnosis (Chamak et al., 2011; Crane et al., 2016). When a developmental disorder has more obvious or detrimental symptoms than autism, parents are prompt in seeking medical help and obtaining a diagnosis. However, the children in our study had no intellectual or language impairments and parents had no knowledge about the aetiology of their child’s behavioural or social interaction problems, which may have lengthened the pre-diagnostic phase. In Chinese culture, children manifesting behavioural problems in public are viewed as a parental failure and a disgrace to the family name (Chou and Palley, 1998). Thus, when children manifest behavioural, social or maladjustment problems, parents often seek traditional and religious help to monitor their children’s behaviour, possibly as a step towards avoiding the additional stigmatization of a psychiatric disorder (Wong, 2009).
In spite of public health promotions for awareness of developmental disorders in Taiwan, cultural beliefs and influences are still deeply rooted in Taiwanese parents. Parents in Taiwan have multiple explanatory models for these children that might not be in accordance with western medicine; rather than accept a diagnosis of ASD, parents attribute behavioural problems to a birth injury, nutritional deficiency or a food allergy (Shyu et al., 2010), or ASD-related genetic information is obtained from non-health professionals (Chen et al., 2015). Medical care in Taiwan may also contribute to the delay. Physicians in Taiwan allow only short visits for each patient, the so-called ‘three-minute patient visit’ (Chen, 2003). Thorough, in-depth interviews and histories are essential for obtaining a correct diagnosis of ASD, and this fee-driven practice style could result in physicians overlooking a diagnosis of ASD.
The diagnosis phase often occurred at a point when parents could no longer ignore their child’s disruptive behaviour or the developmental delays were more apparent. Motivation to obtain a confirmed diagnosis often resulted from an external force such as a teacher’s demand. Once the child was enrolled in school, behavioural and social difficulties were more difficult to ignore: their child’s symptoms may disrupt the classroom environment or their impaired social interactions were more obvious. Thus, external pressure from classroom teachers eventually forced our participants to bring their child to a specialist for diagnosis. For other parents, their child’s symptoms at home were too significant to ignore, and internal motivation prompted the participants to obtain a diagnosis. Although most participants accepted treatment programmes after obtaining a diagnosis of ASD for their child, some began anxiously searching for a second opinion. The search for an alternate diagnosis involved self-help, travelling to other cities to seek help or looking for new information. Being provided with resources and knowledge was considered to be most useful for helping parents face their child’s problems. The participants seeking information through the Internet, or reading books to identify or understand their children’s problem, is similar to experiences of parents reported by Mackintosh et al. (2012).
In Taiwan, children with developmental delays have access to treatment in accordance to their parents’ decision or a doctor’s referral. Treatment modalities can be implemented based on the ‘problems’, not the diagnosis and parents in our study engaged in multiple treatment strategies for their children. The Disabled Persons Welfare Law, enacted in 1980, and the Physically and Mentally Disabled Citizens Protection Act (1997) provide financial support for treatment of children with disabilities, which makes it easy to obtain relatively low-cost medical care. However, availability of treatment programmes for children with ASD is low and long waiting lists can delay enrolment for more than 6 months. While waiting for placement in day hospital programmes or intensive behavioural treatment groups designed for children with ASD some parents use alternative therapies, such as sensory integration or play therapy for their children, which can incur a significant out-of-pocket expense and can add an additional burden for parents of children with ASD (Shyu et al., 2010). Addressing the core symptoms of ASD requires specific multidisciplinary care guided by qualified healthcare professionals. Thus, obtaining a confirmative diagnosis as early as possible would enable children with ASD to acquire the needed treatment at an earlier stage of development.
The experiences of coping with the diagnostic process were similar to the coping mechanisms described by Lazarus and Folkman (1984/2011): problem-focused and emotion-focused coping. Problem-focused coping involves problem solving strategies and changing the source of stress. Social support can help with problem-focused coping, and after the diagnosis, support for treatment of their children’s ASD reduced some of the anxiety parents had experienced. Emotion-focused coping, which reduces or manages feelings of distress associated with the stressor, is better at addressing sources of stress that cannot be controlled, such as disorder. The majority of the experiences of coping with the diagnostic process in our study was emotional. One reason may be that the culture of Asian families is collectivistic, which emphasizes the value of unity, cohesion and avoidance of shame and losing face (Lui and Rollock, 2013). Individuals in collectivistic cultures have been shown to rely more heavily on emotion-focused coping strategies (Lam and Zane, 2004).
Thus, we noted that in our study, once parents accepted the diagnosis, they were able to move to the post-diagnosis phase, which incorporated acceptance and fortitude and eventually evolved into further adjustment. In this study, we noted that parents underwent stressful psychological changes in the process of diagnosis. The initial experiences of the participants prior to their child’s diagnosis of ASD (bewilderment, depression and a sense of desperation) were similar to experiences of coping with loss described by Kubler-Ross (2005). The process of acceptance differed, however. When parents accepted the diagnosis of ASD, they experienced hope and resilience, which was a powerful advantage. Parents planned for the future, adjusted expectations and ‘initialized new hope’. This difference might be attributed to the fact that parents have the responsibility for their child’s future and must establish a stable foundation for their children. A positive attitude regarding the uncertainty of their child’s future may be the underlying strength for our parents.
When a confirmed diagnosis of ASD was received, parents revised their plans for the future. Hope has been demonstrated to be a protective factor against psychological stress in mothers of children with diabetes; mothers with higher hopes had lower levels of anxiety (Mednick et al., 2007). Although ASD and diabetes are very different, they are both lifelong illnesses with no known cure. ASD might be more complicated, as these children manifest behavioural and cognitive difficulties, which are both crucial issues during the stages of childhood and adolescent development. Therefore, the existence of hope in the parents of these ASD children is very encouraging.
Clinical implications
Despite the promotion of public awareness of ASD in Taiwan, participants experienced hesitation, anxiety and denial when confronted with symptoms of ASD in their children. Therefore, we suggest information regarding ASD be made available to parents when they visit a healthcare professional with concerns about their infant’s developmental delays or questions regarding their young child’s social behaviour. Providing parents with accurate information about ASD could foster discussions about the ramifications of a possible diagnosis of ASD and referral to a specialist for further evaluation. Adequate support and guidance could help parents successfully transition in order to begin to make realistic future plans for their child’s future.
The importance of social welfare cannot be overlooked. In our study, we interviewed parents of children whose symptoms of ASD were less obvious, thus making the diagnostic process lengthier than for children with obvious developmental delays. We believe the positive outcome experienced by the participants in our study in the post-diagnostic phase was facilitated by access to treatment and the financial support from the National Health Insurance in Taiwan. Participants’ concern regarding their child’s future could be addressed by providing additional social and financial support for adults with ASD. This would ease the burden of long-term care for parents and reduce the stress of raising a child with ASD.
Limitations
One limitation of our study is only one participant was male; therefore, caution should be used regarding the generalizability of these findings to fathers. A second limitation is the participants were parents of children with ASD who had already gained access to medical or rehabilitation resources. Supportive systems were already in place, which might have given them a more optimistic view of their child’s prognosis. Thus, our results might not generalize to all parents of children with ASD. Parents of children with ASD who do not have easy access to medical care could encounter greater difficulties with daily life and school adjustment. For those parents, the final stage of initiating new hope might be more difficult to achieve.
Supplemental Material
AUT680915_Lay_Abstract – Supplemental material for How Taiwanese parents of children with autism spectrum disorder experience the process of obtaining a diagnosis: A descriptive phenomenological analysis
Supplemental material, AUT680915_Lay_Abstract for How Taiwanese parents of children with autism spectrum disorder experience the process of obtaining a diagnosis: A descriptive phenomenological analysis by Kuo-Yu Chao, Hsueh-Ling Chang, Wei-Chih Chin, Hsin-Mei Li and Sue-Hsien Chen in Autism
Footnotes
Acknowledgements
The authors would like to thank the participants for sharing their perspectives.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chang Gung Memorial Hospital (CMRPF1F0021).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.