
Abstract
Neurodevelopmental disorders, including autism spectrum disorder, are common in children and adolescents, but treatment strategies remain limited. Although repetitive transcranial magnetic stimulation has been studied for neurodevelopmental disorders, there is no clear consensus on its therapeutic effects. This systematic review examined literature on repetitive transcranial magnetic stimulation for children and adolescents with neurodevelopmental disorders published up to 2018 using the PubMed database. The search identified 264 articles and 14 articles met eligibility criteria. Twelve of these studies used conventional repetitive transcranial magnetic stimulation and two studies used theta burst stimulation. No severe adverse effects were reported in these studies. In patients with autism spectrum disorder, low-frequency repetitive transcranial magnetic stimulation and intermittent theta burst stimulation applied to the dorsolateral prefrontal cortex may have therapeutic effects on social functioning and repetitive behaviors. In patients with attention deficit/hyperactivity disorder, low-frequency repetitive transcranial magnetic stimulation applied to the left dorsolateral prefrontal cortex and high-frequency repetitive transcranial magnetic stimulation applied to the right dorsolateral prefrontal cortex may target inattention, hyperactivity, and impulsivity. In patients with tic disorders, low-frequency repetitive transcranial magnetic stimulation applied to the bilateral supplementary motor area improved tic symptom severity. This systematic review suggests that repetitive transcranial magnetic stimulation may be a promising intervention for children and adolescents with neurodevelopmental disorders. The results warrant further large randomized controlled trials of repetitive transcranial magnetic stimulation in children with neurodevelopmental disorders.
Keywords
Child and adolescent neurodevelopmental disorders are common and impairing conditions with limited, brain-based treatment approaches. In 2015, the prevalence rates of autism spectrum disorder (ASD), attention deficit/hyperactivity disorder (ADHD), and tic disorders in children and adolescents aged 5 to 17 years were 2.4%, 11.2%, and 0.52%, respectively (Scharf et al., 2015; U.S. Environmental Protection Agency, 2017). Timely intervention for children with neurodevelopmental disorders is critical because early disturbances in social or cognitive functioning globally impair subsequent development (Erskine et al., 2014; Sanchez-Valle et al., 2008). There are three major neurodevelopmental disorders: ASD, ADHD, and tic disorders. ASD is characterized by impairments in social interaction, communication deficits, restricted interests, and repetitive behaviors. Children with ADHD struggle with hyperactivity, impulsivity, and inattentiveness. Tic disorders, including Tourette syndrome, manifest as sudden, rapid, recurrent, and non-rhythmic motor movements and/or vocalizations (American Psychiatric Association, 2013).
Psychosocial interventions, such as applied behavior analysis or social skill training, are thought to be helpful for individuals with ASD, but the efficacies of these interventions are not well established (Virues-Ortega, Julio, & Pastor-Barriuso, 2013). Pharmacotherapy is often used to manage some symptoms (such as irritability) associated with ASD (Hirsch & Pringsheim, 2016). Common pharmacologic approaches have intolerable adverse effects, such as weight gain, insomnia, or sedation (Hirsch & Pringsheim, 2016; Storebo et al., 2015). The symptoms of ADHD, such as hyperactivity and inattention, can be treated with medications (Shang, Pan, Lin, Huang, & Gau, 2015). Stimulants, such as methylphenidate (Cortese et al., 2018), are very effective for improving ADHD symptoms in most patients. Unfortunately, 10% to 30% of ADHD patients do not benefit from these conventional therapies (Gomez et al., 2014) because patients and their families are often concerned with the associated risks and side effects (Kral, Lally, & Boan, 2017; Zhang et al., 2015). Tic disorders are often treated with antipsychotics (Weisman, Qureshi, Leckman, Scahill, & Bloch, 2013). However, the effects of medications on tic symptoms are often limited, and the side effects of antipsychotic medications are problematic in developing children. Considering the limitations of the currently available treatments for neurodevelopmental disorders, novel therapeutic and brain-based interventions with high tolerability are desperately needed for these disorders (Green & Garg, 2018).
Although the pathophysiology of neurodevelopmental disorders remains unclear, converging evidence suggests the involvement of the prefrontal cortex (PFC; Klein et al., 2017; Park et al., 2016). In particular, researchers have hypothesized that the PFC plays a major role in the pathophysiology of ASD and ADHD. Postmortem analysis has revealed enhanced neuronal density in the PFC and increased total brain weight in ASD children compared with healthy children (Courchesne et al., 2011). Furthermore, electroencephalogram (EEG) studies have indicated that children with ASD have reduced long-range connectivity in the alpha band between the frontal lobe and other brain regions. The findings could reflect a slower maturation process in children with ASD than in healthy controls (Gurau, Bosl, & Newton, 2017). A functional magnetic resonance imaging (fMRI) study indicated that less severely affected children and adolescents with ASD have higher frontal lobe activation associated with self-initiated interactions than typically developing individuals (Oberwelland et al., 2017). In addition, a voxel-based, whole-brain diffusion tensor imaging (DTI) analysis demonstrated that values of fractional anisotropy in the left dorsolateral prefrontal cortex (DLPFC) are negatively correlated with degrees of social impairment in children with ASD (Noriuchi et al., 2010). These findings suggest that structural and functional abnormalities in the PFC may underlie the clinical symptoms of ASD.
In addition, an EEG/event-related potential study using an oddball task indicated that activation in the anterior cingulate cortex and right DLPFC significantly decreases during the task in children with ADHD compared with that in healthy control subjects (Rubia, Smith, Brammer, & Taylor, 2007). An MRI study suggested that the maturation of cortical thickness lags behind approximately 3 years throughout the cerebrum in children with ADHD. Particularly, the delay in attaining peak cortical thickness is most prominent in the PFC in children with ADHD compared with healthy controls (Shaw et al., 2007). Furthermore, an fMRI study using the vigilance task demonstrated hypoactivation of the left DLPFC during the task in children with ADHD compared with healthy controls (Christakou et al., 2013). A recent meta-analysis indicated that children with ADHD have consistent functional abnormalities related to attention, as measured with fMRI, in the DLPFC, parietal cortex, and cerebellum (Hart, Radua, Nakao, Mataix-Cols, & Rubia, 2013). These findings suggest that the DLPFC plays a key role in the pathophysiology of ADHD.
The pathophysiology of tic disorders may diverge from that of ASD or ADHD. For example, the cortico-striato-thalamo-cortical circuits involving the supplementary motor area (SMA) have been implicated in the pathophysiology of Tourette syndrome (Neely, Garcia, Bankston, & Green, 2018; Peterson et al., 2001; Singer & Minzer, 2003; Stern et al., 2000). Furthermore, the SMA appears to be overactive when motor tasks are performed (Biswal et al., 1998). A recent magnetoencephalography study demonstrated that patients with chronic tic disorders have increased functional connectivity between the SMA and the motor cortex (Franzkowiak et al., 2012).
Repetitive transcranial magnetic stimulation (rTMS) is an emerging clinical treatment modality with minimal adverse effects. Conventional rTMS, such as high- and low-frequency stimulation, induces facilitatory and inhibitory modulation at the stimulated site, respectively. One of the primary advantages of rTMS is that it can stimulate specific brain areas in a non-invasive manner. To date, rTMS is primarily used as a therapeutic tool to treat depression in adults (Conelea et al., 2017; Gaynes et al., 2014; Lefaucheur et al., 2014; O’Reardon et al., 2007). Despite the increased number of clinical applications of rTMS in adult patients with neurodevelopmental disorders, a limited number of studies are available on the application of rTMS in children and adolescents with neurodevelopmental disorders (Oberman, Enticott et al., 2016). Some systematic reviews (Hameed et al., 2017; Krishnan, Santos, Peterson, & Ehinger, 2015) focused on safety aspects of rTMS application, and there is no consensus on the therapeutic effects of rTMS in children and adolescents with neurodevelopmental disorders.
Theta burst stimulation (TBS), a relatively new form of patterned rTMS, may induce therapeutic changes through neuroplasticity with lower stimulus intensities in less time than standard rTMS protocols (Huang et al., 2009), and clinical application of TBS is emerging worldwide (Suppa et al., 2016). Intermittent TBS (iTBS) induces facilitatory neuromodulation, whereas continued TBS (cTBS) induces inhibitory neuromodulation at the stimulated site. Recently, the efficacy of TBS in patients with depression has been indicated in several studies (Berlim, McGirr, Rodrigues Dos Santos, Tremblay, & Martins, 2017; Blumberger et al., 2018); however, few studies have investigated the efficacy of TBS in neurodevelopmental disorders (Abujadi, Croarkin, Bellini, Brentani, & Marcolin, 2017; Wu et al., 2014).
The present systematic review aimed to examine the therapeutic effects of rTMS and TBS in children and adolescents with neurodevelopmental disorders, such as ASD, ADHD, and tic disorders.
Methods
Search strategy
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009). A comprehensive search of articles published up to 7 February 2018 was conducted in PubMed. Terms related to transcranial magnetic stimulation (rTMS, transcranial magnetic stimulation, and repetitive transcranial magnetic stimulation) and neurodevelopmental disorders (ADHD, ASD, Asperger, attention deficit hyperactivity disorder, autism, autism spectrum disorder, childhood schizophrenia, neurodevelopmental disorders, PDD, and pervasive developmental disorder) were used in this study.
Study selection
The following inclusion criteria were applied: (1) written in English, (2) clinical studies with multiple rTMS sessions administered to patients with neurodevelopmental disorders, (3) studies including child and/or adolescent patients below 21 years of age, and (4) availability of the full-text article. The age range was extended to 21 years because individuals aged ⩽21 years are often defined as “children” (Sokhadze et al., 2012; Wang et al., 2016) or “adolescents” (Savolainen et al., 2018; Torres, Goyal, Burke-Aaronson, Gay, & Lee, 2017) according to common clinical practices in pediatrics and child psychiatry. Articles were excluded based on the following criteria: (1) animal model studies, (2) review articles, and (3) case reports.
Data extraction
Two investigators (F.M. and Y.N.) assessed the studies independently based on the eligibility criteria. The following data were extracted by F.M. and Y.N. independently from each study: study design, characteristics of participants, rTMS procedure/parameters, clinical/cognitive outcomes, medication, and adverse effects. Any discrepancies on data extraction were then reviewed, discussed, and resolved by F.M. and Y.N.
Quality assessment
There were 7 randomized controlled trials in 14 included studies. Risk of bias assessment was employed only for the randomized controlled trials using Review Manager 5.3 for the following factors: random sequence generation, allocation concealment, blinding for participants and personnel, blinding for outcome assessors, incomplete outcome data, selective reporting, and other bias (Supplemental Figure 1).
Results
The PRISMA diagram is shown in Figure 1. The PubMed search identified 264 articles, but only 14 articles met the eligibility criteria. Extracted data such as study design, stimulation protocols, and clinical effect in these studies are summarized in Tables 1 and 2. Among the 14 eligible studies, 12 used conventional rTMS (Table 1). Among the 12 studies, 8 were conducted in ASD patients (Casanova et al., 2012, 2014; Gomez et al., 2017; Panerai et al., 2014; Sokhadze et al., 2012; Sokhadze, El-Baz, Sears, Opris, & Casanova, 2014; Sokhadze, El-Baz, Tasman, et al., 2014; Wang et al., 2016); 2 were carried out in ADHD patients (Gomez et al., 2014; Weaver et al., 2012); and 2 were performed in patients with tic disorders (Bersani et al., 2013; Kwon et al., 2011). In addition, other 2 studies used TBS in patients with ASD (Abujadi et al., 2017) or chronic tic disorders (Wu et al., 2014) (Table 2).
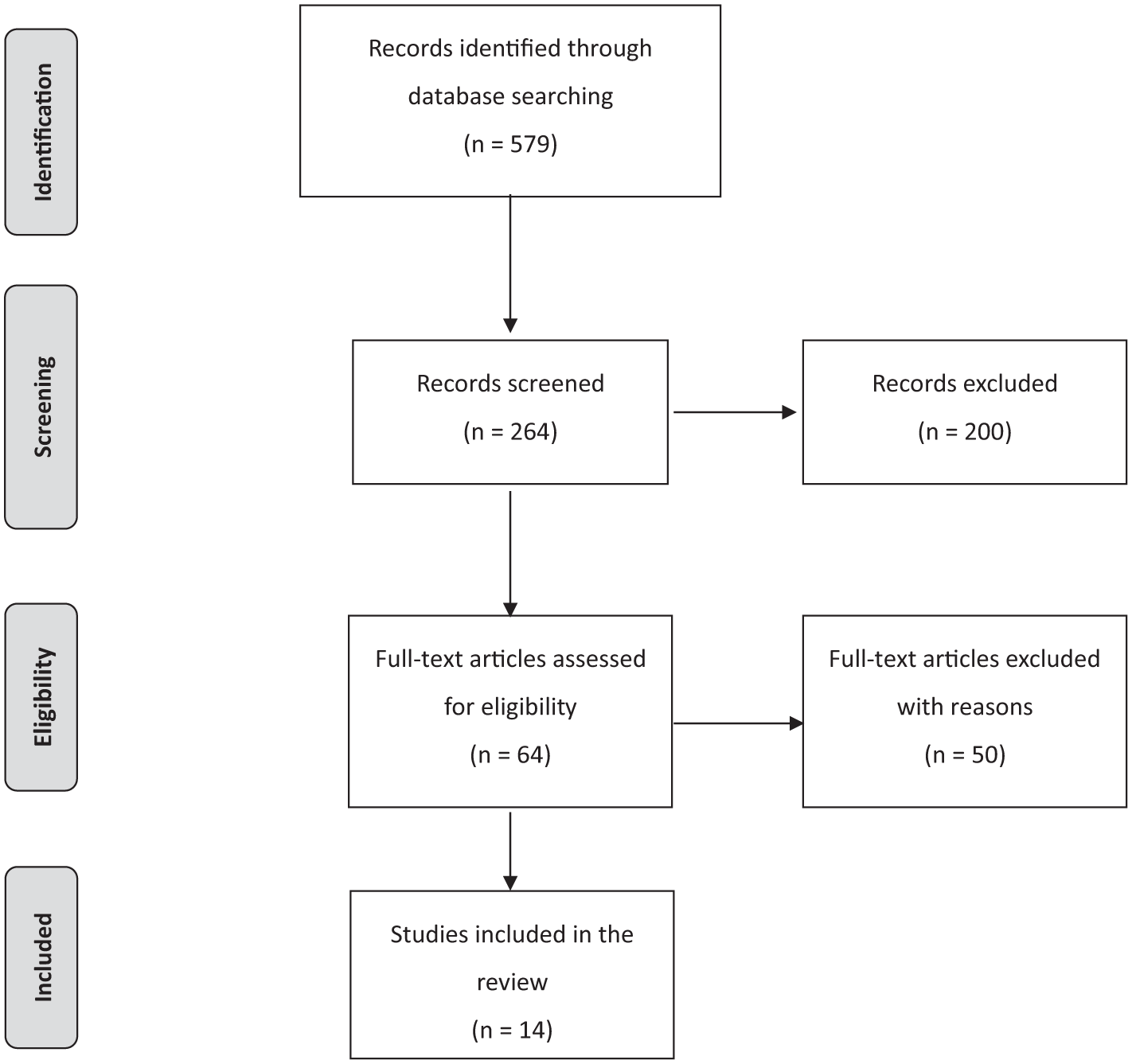
Flow diagram of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Conventional rTMS.
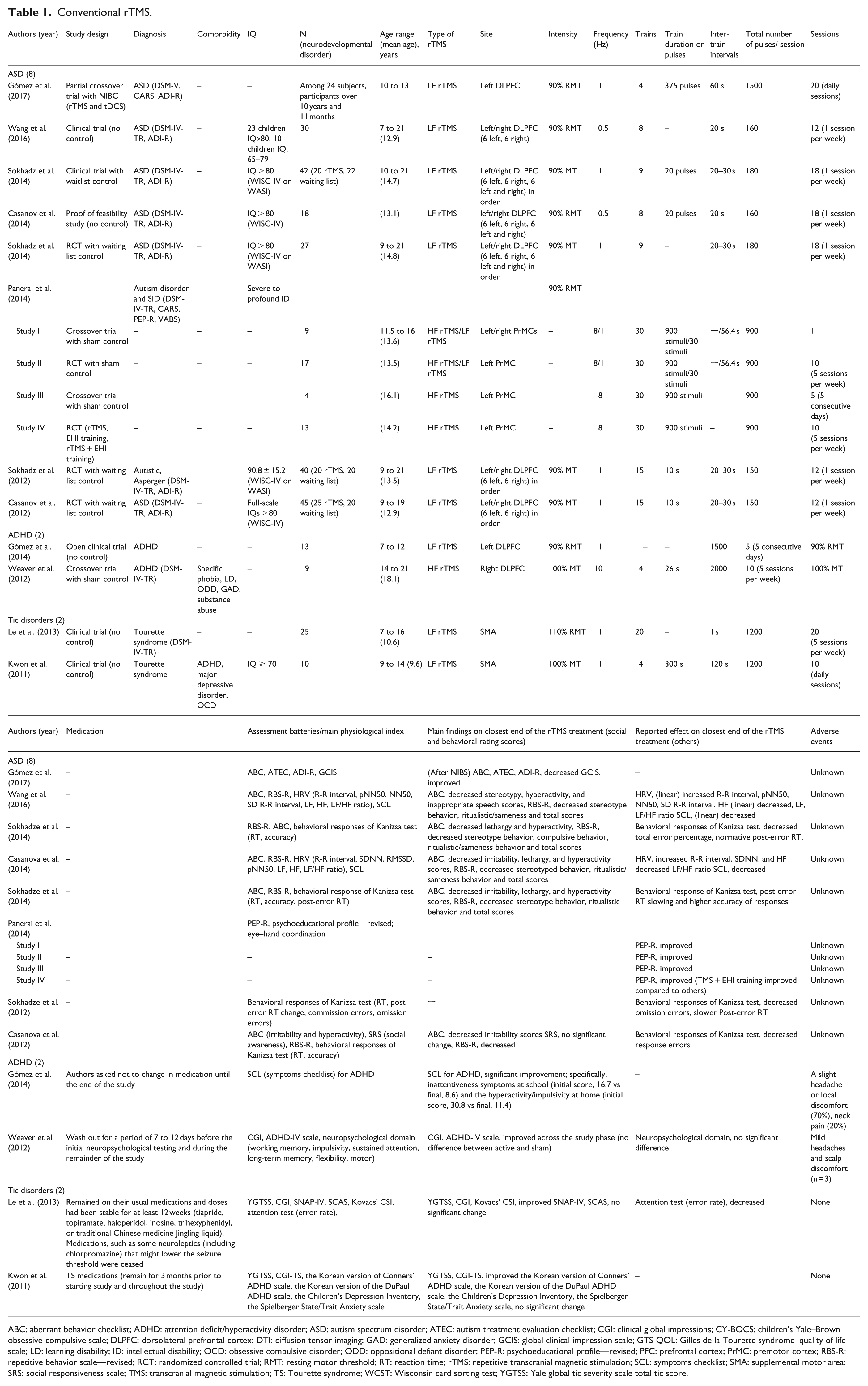
ABC: aberrant behavior checklist; ADHD: attention deficit/hyperactivity disorder; ASD: autism spectrum disorder; ATEC: autism treatment evaluation checklist; CGI: clinical global impressions; CY-BOCS: children’s Yale–Brown obsessive-compulsive scale; DLPFC: dorsolateral prefrontal cortex; DTI: diffusion tensor imaging; GAD: generalized anxiety disorder; GCIS: global clinical impression scale; GTS-QOL: Gilles de la Tourette syndrome–quality of life scale; LD: learning disability; ID: intellectual disability; OCD: obsessive compulsive disorder; ODD: oppositional defiant disorder; PEP-R: psychoeducational profile—revised; PFC: prefrontal cortex; PrMC: premotor cortex; RBS-R: repetitive behavior scale—revised; RCT: randomized controlled trial; RMT: resting motor threshold; RT: reaction time; rTMS: repetitive transcranial magnetic stimulation; SCL: symptoms checklist; SMA: supplemental motor area; SRS: social responsiveness scale; TMS: transcranial magnetic stimulation; TS: Tourette syndrome; WCST: Wisconsin card sorting test; YGTSS: Yale global tic severity scale total tic score.
Theta burst stimulation (TBS).

ABC: aberrant behavior checklist; ADHD: attention deficit/hyperactivity disorder; ASD: autism spectrum disorder; cTBS: continuous theta burst stimulation; CY-BOCS: children’s Yale–Brown obsessive-compulsive scale; DLPFC: dorsolateral prefrontal cortex; GTS-QOL: Gilles de la Tourette syndrome–quality of life scale; iTBS: intermittent theta burst stimulation; PUTS: premonitory urge for tics scale; RBS-R: repetitive behavior scale—revised; RCT: randomized controlled trial; RMT: resting motor threshold; RT: reaction time; rTMS: repetitive TMS; RVTRS: rush videotaped tic rating scale; SCL: symptoms checklist; SMA: supplemental motor area; TBS: theta burst stimulation; TMS: transcranial magnetic stimulation; TS: Tourette syndrome; WCST: Wisconsin card sorting test; YGTSS: Yale global tic severity scale total tic score.
Conventional rTMS for neurodevelopmental disorders
Findings of rTMS for ASD
A total of four different types of rTMS intervention methods were identified in the eight studies. Findings are organized according to the rTMS treatment protocols.
In three studies, low-frequency rTMS, which was applied to the left, right, and bilateral DLPFC in separate sessions (six sessions for each stimulation site), had positive effects on social and behavioral rating scores, as indexed with the aberrant behavior checklist (ABC) or repetitive behavior scale—revised (RBS-R) (Casanova et al., 2014; Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014). Symptoms such as irritability, hyperactivity, and lethargy (social withdrawal) on the ABC rating scale improved in all studies (Casanova et al., 2014; Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014). Among the three studies, two showed improved behavioral responses in the visual task of Kanizsa illusion figures, indicating the decreased response errors and normalized post-error reaction time (Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014).
Low-frequency rTMS was applied to the left and right DLPFC in separate sessions (six sessions for each stimulation site) in other three studies (Casanova et al., 2012; Sokhadze et al., 2012; Wang et al., 2016). Among the three studies, two showed positive effects on social and behavioral rating scores, as measured with the ABC (irritability, stereotypy, hyperactivity, and inappropriate speech scores) and RBS-R (stereotype behavior, ritualistic/sameness, and total scores) (Casanova et al., 2012; Wang et al., 2016). In addition, the behavioral and error responses in the visual task of Kanizsa illusion figures improved in two of the three studies (Casanova et al., 2012; Sokhadze et al., 2012). Furthermore, one study showed the normalized post-error reaction time (Sokhadze et al., 2012).
In one study, low-frequency rTMS, which was used to the left DLPFC, improved social and behavioral rating scores, as measured with the ABC and autism treatment evaluation checklist (Gomez et al., 2017). However, the RBS-R or behavioral responses were not investigated in this study.
In another study, high-frequency rTMS, which was applied to the left premotor cortex in ASD patients with severe intellectual disability, improved eye–hand coordination, as assessed with the psychoeducational profile—revised (Panerai et al., 2014). Notably, these studies did not find adverse events caused by rTMS for ASD. There was no description of concurrent medications during rTMS treatment in the eight studies focusing on ASD.
Findings of rTMS for ADHD
In total, two rTMS clinical trials were performed in children and adolescents with ADHD (Gomez et al., 2014; Weaver et al., 2012). Although the evaluation methods were different in the two studies, the behavioral rating scores improved compared with the baseline in both studies. In particular, in one study without controls, 1-Hz stimulation on the left DLPFC for five sessions improved the scores of the symptoms checklist (SCL) in patients with ADHD, especially in those with inattentiveness at school and hyperactivity/impulsivity at home (Gomez et al., 2014). Weaver et al. (2012) applied 10 sessions of 10-Hz rTMS over the right DLPFC as an active rTMS phase in a crossover design. Scores on the clinical global impressions (CGI) and ADHD-IV scale significantly decreased compared with the baseline, although no differences were observed between active and sham groups (Weaver et al., 2012). Notably, both studies found some mild adverse events (such as slight headache, local discomfort, or neck pain) associated with rTMS. With regard to medications, concomitant medications were fixed during one study (Gomez et al., 2014); however, medications were washed out for 7 to 12 days before another study, and the medication-free condition was maintained during the study (Weaver et al., 2012).
Findings of rTMS for tic disorders
To date, rTMS was applied in patients with tic disorders in two clinical trials (Bersani et al., 2013; Kwon et al., 2011). Scores on both the Yale global tic severity scale (YGTSS) and the CGI improved in these two studies. Particularly, 1-Hz rTMS was applied to the SMA with 1200 pulses per session for 20 sessions in one study (Bersani et al., 2013), and the same rTMS protocol with 10 sessions was used in another study (Kwon et al., 2011). In both studies, medications were maintained for at least 12 weeks prior to rTMS and at a steady dose throughout rTMS. In addition, the rating scales related to other symptoms, such as attention deficit or anxiety, did not change after rTMS treatment (Kwon et al., 2011). No adverse effects were observed in these studies.
TBS for children and adolescents with neurodevelopmental disorders
TBS was used in patients with ASD and chronic tic disorders in the remaining 2 studies among the 14 selected studies (Abujadi et al., 2017; Wu et al., 2014) (Table 2).
Findings of TBS for ASD
Abujadi et al. (2017) applied iTBS for children and adolescents with ASD, and scores of both RBS-R and Yale–Brown obsessive-compulsive scale improved after 15 sessions of iTBS over the right DLPFC. The executive function including perseverative errors and time for completion, which were respectively assessed with the Wisconsin card sorting test and Stroop test, improved in this study. Notably, no adverse effects were observed in this study. Medication information during the TBS treatment was not described in this study.
Findings of TBS for tic disorders
Wu et al. (2014) used cTBS with two sessions for two consecutive days over the SMA for children and adolescents with chronic tic disorders, and they assessed the clinical effects using rating scales such as the YGTSS and Gilles de la Tourette syndrome–quality of life. No significant differences were found between active and sham TBS groups. In total, three participants complained of mild adverse events: abdominal pain, headaches, and dry eyes. However, there was no description of the causality of adverse events during cTBS treatment in this study. Medications were administered mostly in 10 days before the cTBS treatment and maintained during the treatment.
Discussion
This systematic review demonstrates the potential clinical effects of rTMS in some children and adolescents with neurodevelopmental disorders. In patients with ASD, low-frequency rTMS applied to the left DLPFC or iTBS applied to the right DLPFC had beneficial effects on stereotypy, hyperactivity, inappropriate speech scores, irritability, and lethargy. In patients with ADHD, low-frequency rTMS applied to the left DLPFC improved hyperactivity, impulsivity, and inattentiveness. In patients with tic disorders, low-frequency rTMS applied to the SMA ameliorated tic symptoms. A few mild adverse effects were identified in the present systematic review.
The optimal rTMS protocol for ASD or ADHD may be different from that for depression despite the same stimulation site, the DLPFC. In general, high-frequency rTMS is applied to the left DLPFC in most studies (Conelea et al., 2017; Gaynes et al., 2014) based on the assumption that neuroplasticity declines in the DLPFC in patients with depression (Crabtree et al., 2017; Noda et al., 2018; Zheng & Zhang, 2015). In contrast, neuroplasticity is hypothesized to increase in patients with neurodevelopmental disorders, particularly in those with ASD (Oberman, Ifert-Miller et al., 2016; Oberman & Pascual-Leone, 2014). Thus, the differences in presumed pathophysiology account for differences in rTMS protocols used in neurodevelopmental and depressive disorders. In addition, low-frequency rTMS induces inhibitory neuromodulation, while high-frequency rTMS induces facilitatory neuromodulation at the stimulated site (Funke & Benali, 2011; Lozeron et al., 2016). It has been recently demonstrated that ASD patients have decreased cortical inhibition (Banerjee et al., 2013; Enticott, Rinehart, Tonge, Bradshaw, & Fitzgerald, 2010; Vattikuti & Chow, 2010), which could result in cortical excitation/inhibition (E/I) imbalance. Therefore, we speculate that low-frequency rTMS may increase inhibitory function at the stimulated site, leading to improved symptoms in children and adolescents with ASD.
Therapeutic effects of rTMS and TBS in ASD
This study found that low-frequency rTMS to the left DLPFC and iTBS to the right DLPFC had positive effects on behaviors in children and adolescents with ASD. These different therapeutic interventions have been thought to cause similar effects through transcallosal inhibition, and they improve symptoms (such as irritability, hyperactivity, repetitive behaviors, and lethargy) that tend to be resistant to pharmacotherapy (Hirsch & Pringsheim, 2016). As mentioned in the introduction, children and adolescents with ASD are assumed to have increased numbers of cortical columns and neurons in the PFC (Ameis & Catani, 2015), resulting in greater total brain weight in ASD children than in healthy controls (Courchesne et al., 2011). Furthermore, the neuroanatomical alterations may induce inappropriate overactivation in the PFC, thus leading to dysfunctional connectivity in the PFC in children and adolescents with ASD. Indeed, Uddin and colleagues proposed that over-connectivity in the default mode network involving the PFC is more prevalent in children and adolescents with ASD (Uddin, Supekar, Lynch et al., 2013; Uddin, Supekar, & Menon, 2013). Therefore, suppressive effects of low-frequency rTMS on the DLPFC could normalize functional connectivity in the PFC in children and adolescents with ASD. Interestingly, the positive effects of conventional rTMS on repetitive behaviors were noted in children and adolescents with ASD in the included studies. Repetitive behaviors are hypothesized to be related to the pathophysiology of the reward system involving the striatum (Kohls, Yerys, & Schultz, 2014; Langen et al., 2014). Kohls et al. (2014) proposed that overvaluation of the reward system may contribute to excessive routine behaviors, which cause resistance to changes. Accumulating evidence suggests that the striatum is functionally connected to the DLPFC (Avissar et al., 2017; Biswal et al., 1998; Haber & Knutson, 2010; Jarbo & Verstynen, 2015). Strafella and colleagues demonstrated that high-frequency rTMS administered to the DLPFC could increase the release of endogenous dopamine from the caudate nucleus (Strafella, Paus, Barrett, & Dagher, 2001; Strafella, Paus, Fraraccio, & Dagher, 2003). Conversely, suppressive effects of low-frequency rTMS on the DLPFC could induce dopaminergic neuromodulation in patients with ASD, thus alleviating symptoms such as repetitive behaviors.
Previous studies suggest that the effect of the pharmacological intervention on lethargy is limited, although pharmacotherapy may improve other symptoms of ASD, including irritability, hyperactivity, and repetitive behaviors (Hirsch & Pringsheim, 2016). However, rTMS can improve irritability, hyperactivity, repetitive behaviors, and lethargy (Casanova et al., 2014; Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014). All currently available antipsychotics, including risperidone and aripiprazole, block postsynaptic D2 receptors and inhibit excessive transmission of dopamine in the mesolimbic system, thus alleviating the psychotic symptoms (Miyamoto, Duncan, Marx, & Lieberman, 2005) and improving repetitive behaviors in ASD (McDougle et al., 1998). In addition, low-frequency rTMS over the left DLPFC may stabilize the dopamine release at the stimulated site (Strafella et al., 2001, 2003), possibly leading to beneficial effects on lethargy in ASD (Casanova et al., 2014; Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014). Therefore, unlike antipsychotics, rTMS may exert the therapeutic effect on social lethargy by modulating other neurotransmitter-related systems such as GABAergic and glutamatergic functions (Baeken, Lefaucheur, & Van Schuerbeek, 2017; Dlabac-de Lange et al., 2017; Dubin et al., 2016). However, based on the findings in previous studies, the impact of DLPFC rTMS on social impairment in ASD remains elusive. For example, three studies indicate the positive effect of rTMS on lethargy (Casanova et al., 2014; Sokhadze, El-Baz, Sears, et al., 2014; Sokhadze, El-Baz, Tasman, et al., 2014), whereas two studies suggest the negative impact of DLPFC rTMS on lethargy (Wang et al., 2016) or social awareness (Sokhadze et al., 2010). Therefore, it is premature to conclude that rTMS has positive effects on lethargy.
Therapeutic effects of rTMS and TBS in ADHD
This systematic review found that low-frequency rTMS to the left DLPFC and high-frequency rTMS to the right DLPFC improved symptoms, such as inattentiveness, in children and adolescents with ADHD. The study by Gomez et al. had no control subjects, and the study by Weaver et al. did not find significant differences between patients and sham controls; therefore, it is difficult to conclude whether rTMS has beneficial effects on ADHD based solely on the findings in these two studies. Moreover, these two studies have some limitations, including small sample sizes and short-term study durations. Therefore, more rigorous studies are warranted. However, Gomez et al. demonstrated that scores on the SCL decreased by half in patients with ADHD following rTMS treatment. Given the findings in previous studies that used placebo controls (Goodman et al., 2017; Philipsen et al., 2015), there might be some therapeutic effects of rTMS beyond placebo effects. In addition, only subjects with active rTMS showed improved symptoms during the second phase of study after crossover.
Findings in imaging studies seem to warrant further studies on rTMS application in ADHD. Using fMRI, Rubia et al. (2007) found decreased activation of the right DLPFC during an oddball task. Moreover, using fMRI, Chrstakou et al. (2013) found decreased activation of the left DLPFC during a vigilance task in ADHD children compared with healthy controls. Children with ADHD showed improved inattentiveness and hyperactivity/impulsivity in one study in this review (Gomez et al., 2014). Although hyperactivity or impulsivity declines with age, inattentiveness is suggested to be persistent over a lifetime (Biederman, Mick, & Faraone, 2000; Larsson, Lichtenstein, & Larsson, 2006). Therefore, effective treatments for inattention throughout the life cycle are needed. Compared with healthy controls, children with ADHD show dysfunction in the left DLPFC during the sustained attention task (Christakou et al., 2013). Because the DLPFC is considered to be involved in the top-down attentional control (Silton et al., 2010), persistent dysfunction of the DLPFC may account for the pathophysiology of ADHD (Hart et al., 2013). Regarding TBS treatment, He et al. (2013) found that iTBS to the right DLPFC induced a significant improvement in the alerting and executive control efficiency on the attention network test in healthy young adults, suggesting the beneficial effects of iTBS on attentional ability. Taken together, these findings support the speculation that stimulation of the DLPFC may improve inattention in children and adolescents with ADHD. Notably, these two forms of rTMS, low-frequency rTMS and iTBS, induce opposite effects at the same stimulation site. However, because there is a transcallosal inhibition between the left and the right DLPFC through the corpus callosum (Fleming & Newham, 2017), low-frequency rTMS to the left DLPFC could induce facilitatory effects on the contralateral stimulation site (i.e. the right DLPFC), while iTBS to the right DLPFC could induce inhibitory effects on the contralateral stimulation site (i.e. the left DLPFC). Therefore, from a neurophysiological point of view, low-frequency rTMS to the left DLPFC and iTBS to the right DLPFC may confer similar effects.
Moreover, previous DTI studies have consistently demonstrated that white matter anomalies are present in the corpus callosum in children with ADHD (Aoki, Cortese, & Castellanos, 2018; Gilliam et al., 2011). Recently, Kaller et al. found that stronger connectivity between the left and the right DLPFC through the corpus callosum was associated with poorer planning performance in post-adolescents (Kaller et al., 2015). Thus, rTMS to the DLPFC might attenuate impulsivity in children with ADHD through improving their planning ability, in which the DLPFC is involved.
Therapeutic effects of rTMS and TBS in tic disorders
Two studies showed that low-frequency rTMS to the SMA improved tic symptoms in children with Tourette syndrome (Bersani et al., 2013; Kwon et al., 2011).
However, because both are open-label studies, more rigorous studies are needed to confirm these findings. Hyperactivation of the SMA or increased functional connectivity between the SMA and the motor cortex (Biswal et al., 1998; Franzkowiak et al., 2012) could be suppressed by low-frequency rTMS. Furthermore, dopaminergic disturbances in the subcortical basal ganglia are considered to be involved in tic disorders (Godar, Mosher, Di Giovanni, & Bortolato, 2014; Maia & Conceicao, 2017). Thus, rTMS may modulate the dopaminergic system involved in the reward system (Stanford et al., 2013).
The findings are inconsistent with those obtained in previous rTMS studies in adults with tic disorders, which suggest that rTMS has no beneficial effects (Landeros-Weisenberger et al., 2015; Münchau et al., 2002; Orth et al., 2005). Liu et al. (2013) found that a longer duration of tic symptoms was related to abnormalities in the anterior thalamic radiations. Therefore, the inhibitory pathways in the circuits could be differently impaired in different ages of patients, and the speculation may account for the differences in the effects of rTMS between children and adults.
In addition, inhibitory cTBS to the SMA had no significant impact in this population (Wu et al., 2014). However, because this study applied only two cTBS sessions in six subjects diagnosed with different tic disorders (Landeros-Weisenberger et al., 2015), it is difficult to conclude that cTBS is not effective in this population. Thus, further studies are needed to examine the clinical effects of cTBS over the SMA in patients with tic disorders.
Limitations
This study has several limitations. First, we searched articles only in PubMed because it was the only available search engine in our institution. Second, this systematic review focused on the clinical effectiveness of rTMS, indexed mainly with social and behavioral rating scores, in children and adolescents with neurodevelopmental disorders. Thus, biological measures, such as physiological indexes, were not investigated in this review. Third, this study reviewed the clinical effectiveness of rTMS only in children and adolescents with neurodevelopmental disorders, and the studies on neurodevelopmental disorders in adults were not included in this review. Notably, one randomized controlled trial showed a significant improvement in social function–related symptoms in adults with ASD following active rTMS (Enticott et al., 2014). However, the effectiveness of rTMS treatment in adults with neurodevelopmental disorders is controversy. Therefore, further studies are needed to summarize rTMS studies on neurodevelopmental disorders in adults. Fourth, we focused on clinical studies that consisted of multiple sessions of rTMS in patients with neurodevelopmental disorders, and clinical and/or cognitive effects induced by a single session of rTMS were not covered in this study. Fifth, most included rTMS studies targeted at the PFC in patients with neurodevelopmental disorders. Therefore, further studies are needed to investigate pathophysiological bases at the cortical areas other than the PFC and examine the clinical effectiveness of rTMS to the other cortical areas in patients with these disorders. Sixth, the sample sizes in these included studies were small. The small number of patients in each study might prevent meaningful conclusions from being drawn about the impacts of disease severity, adjunctive medications and interventions, and treatment duration on rTMS outcomes. Because adequate controls and blinding for outcome assessors and participants were lacking in the included studies, the findings in this systematic review should be considered preliminary and interpreted with caution. Therefore, more rigorous assessments are warranted to determine the potential efficacy. Seventh, mixed pediatric and adolescent patients were included in some studies, despite potential differences in brain development and function between the two groups of patients. Eighth, some studies did not assess clinical scores. Even if ratings were conducted, a few studies did not report subscale scores in detail.
Future directions
Early intervention with rTMS for children and adolescents with treatment-resistant neurodevelopmental disorders could improve some key symptoms of these disorders. Therefore, further well-designed studies addressing current limitations and knowledge gaps are warranted.
To date, most of the previous rTMS studies focused on only one particular disorder (ASD, ADHD, or tic disorders). However, there are significant similarities in the symptoms among these disorders. Such similarities might indicate common underlying pathophysiology among these disorders. Therefore, it may be helpful to assess the neurobiological mechanisms of these neurodevelopmental disorders with transdiagnostic approaches, comprehensive clinical and cognitive batteries (Funabiki, Kawagishi, Uwatoko, Yoshimura, & Murai, 2011), and reliable biological measures. Therefore, further studies are needed to determine the neural bases of specific symptom clusters, and the findings could allow scientists to target specific symptoms with rTMS intervention and pave the way for personalized medicine in the future.
In addition, TBS was only used in two included studies. However, considering the improved time burden for patients and families, TBS seems to be worth further investigation as a promising treatment option. TBS has less inconvenience and greater feasibility especially in children and adolescents who have daily activities. In addition, TBS possibly benefits children with hyperactivity characteristics because they often have difficulty sitting in the same place for a long time.
Conclusion
This systematic review indicates beneficial effects of rTMS in children and adolescents with neurodevelopmental disorders. The present findings suggest that rTMS may ameliorate ASD symptoms (such as lethargy) that conventional treatments have failed to address to date. The results warrant further rTMS studies with larger sample sizes and systematic clinical assessments (including neurophysiological markers) in patients with neurodevelopmental disorders.
Supplemental Material
AUT822502_Lay_Abstract – Supplemental material for Clinical effectiveness of repetitive transcranial magnetic stimulation treatment in children and adolescents with neurodevelopmental disorders: A systematic review
Supplemental material, AUT822502_Lay_Abstract for Clinical effectiveness of repetitive transcranial magnetic stimulation treatment in children and adolescents with neurodevelopmental disorders: A systematic review by Fumi Masuda, Shinichiro Nakajima, Takahiro Miyazaki, Ryosuke Tarumi, Kamiyu Ogyu, Masataka Wada, Sakiko Tsugawa, Paul E Croarkin, Masaru Mimura and Yoshihiro Noda in Autism
Supplemental Material
AUT822502_Supplemental_material – Supplemental material for Clinical effectiveness of repetitive transcranial magnetic stimulation treatment in children and adolescents with neurodevelopmental disorders: A systematic review
Supplemental material, AUT822502_Supplemental_material for Clinical effectiveness of repetitive transcranial magnetic stimulation treatment in children and adolescents with neurodevelopmental disorders: A systematic review by Fumi Masuda, Shinichiro Nakajima, Takahiro Miyazaki, Ryosuke Tarumi, Kamiyu Ogyu, Masataka Wada, Sakiko Tsugawa, Paul E Croarkin, Masaru Mimura and Yoshihiro Noda in Autism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.