
Abstract
The Hong Kong Chinese version of the Autism-Spectrum Quotient-Child and Autism-Spectrum Quotient-Adolescent were examined for their psychometric properties and specificity on screening autism spectrum disorder against attention-deficit/hyperactivity disorder. This study recruited three groups of participants: typically developing children; children with autism spectrum disorder and children with attention-deficit/hyperactivity disorder. Both the Autism-Spectrum Quotient questionnaires demonstrated satisfactory psychometric properties in terms of internal consistency, test–retest reliability and area under receiver operating characteristics curve in discriminating the autism spectrum disorder group from the attention-deficit/hyperactivity disorder and typically developing groups, separately and jointly. The optimal cutoff scores for both the Autism-Spectrum Quotient questionnaires were identified to be 76, with satisfactory sensitivity and specificity, for differentiating the autism spectrum disorder group from the typically developing group and from the typically developing and attention-deficit/hyperactivity disorder groups combined. On the contrary, both Autism-Spectrum Quotient questionnaires could not effectively differentiate the attention-deficit/hyperactivity disorder group from the typically developing group, or in other words, they did not misclassify attention-deficit/hyperactivity disorder as autism spectrum disorder because of their phenotypic overlap in social difficulties. These findings supported that both the Autism-Spectrum Quotient questionnaires were not general measures of child and adolescent psychopathology, but could claim to be more specific measures of autism spectrum disorder, given their success in identifying the autism spectrum disorder group from the attention-deficit/hyperactivity disorder/typically developing groups, while failing to differentiate the latter two groups.
Lay abstract
The Autism-Spectrum Quotient is a 50-item questionnaire developed to assess autistic symptoms in adults, adolescents and children. Its original version and others in different countries are known to be effective tools in identifying individuals with autism spectrum disorder. This study examined whether the Hong Kong Chinese versions of the Autism-Spectrum Quotient-Child and Autism-Spectrum Quotient-Adolescent were effective in identifying autism spectrum disorder children and adolescents. On top of comparing them with their typically developing peers, this study also included a group of children/adolescents with attention deficit/hyperactivity disorder, a disorder with similar social difficulties as autism spectrum disorder. Results showed that both the Autism-Spectrum Quotient questionnaires were effective in differentiating the autism spectrum disorder group from the typically developing and attention-deficit/hyperactivity disorder groups, separately and jointly. On the contrary, they could not identify the attention-deficit/hyperactivity disorder group from the typically developing group so that they were not misclassifying attention-deficit/hyperactivity disorder as autism spectrum disorder. These findings supported that both the Autism-Spectrum Quotient-Child and Autism-Spectrum Quotient-Adolescent were not general measures of child and adolescent psychopathology, but could claim to be specific measures of autism spectrum disorder. Such capability would enormously enhance their utility in clinical practice for identifying autism spectrum disorder children/adolescents from their typically developing peers and from those with attention-deficit/hyperactivity disorder. This is because, the latter is a common neurodevelopmental disorder frequently presented to child psychiatric clinics alongside with autism spectrum disorder.
Keywords
Autism spectrum disorder (ASD) has been conceptualized dimensionally with the diagnosis referring to conditions that represent upper extremes of autistic traits from a single autism spectrum (Kunihira et al., 2006). Under this spectrum conceptualization of ASD, the Autism-Spectrum Quotient-Adult (AQ-Adult) was developed to measure and quantify autistic traits of an adult with normal intelligence along an ASD continuum (Baron-Cohen et al., 2001). Subsequently, the child and adolescent versions of the AQ (AQ-Child & AQ-Adol) were developed (Auyeung et al., 2008; Baron-Cohen et al., 2006). Both are 50-item, parent-report questionnaires on a range of autistic traits displayed by children/adolescents. Their items are adapted from the original adult version with age-appropriate revisions. The binary scoring system of the adult version is retained in the AQ-Adol, producing a total score ranging from 0 to 50. Meanwhile, a 4-point Likert-type scale is employed for the AQ-Child to provide additional assessment of the severity of symptoms, producing a total score ranging from 0 to 150. Both the AQ-Child and AQ-Adol were found to be reliable and valid screening tools for respective age groups. The cutoff scores for the AQ-Adol and AQ-Child were respectively suggested at 30 (Baron-Cohen et al., 2006) and 76 (Auyeung et al., 2008). High internal consistency (α = 0.79–0.97) and test–retest reliability (r = 0.85–0.92) were reported in both versions (Auyeung et al., 2008; Baron-Cohen et al., 2006). Two cross-cultural validation studies were conducted for the AQ-Adol/AQ-Child, one in Japan (Wakabayashi et al., 2007) and one in France (Sonié et al., 2013). In both studies, the ASD group scored significantly higher than the control, and the mean difference between them showed an almost identical 20-point difference as in case of the two original studies in the United Kingdom (Auyeung et al., 2008; Baron-Cohen et al., 2006).
The original AQ-Adult reported satisfactory internal consistency of five subscales: Social Skill (α = 0.77); Attention Switching (α = 0.67); Attention to Detail (α = 0.63); Communication (α = 0.65); and Imagination (α = 0.65; Baron-Cohen et al., 2001). However, their factorial validity is not adequately established in some other studies. Factor analysis mostly confirmed only two to four factors, namely, Social Skills, Attention to detail, Communication and Imagination (Austin, 2005; Hoekstra et al., 2008; Hurst et al., 2007; Kloosterman et al., 2011; Stewart & Austin, 2009). Lau and colleagues (2013) examined the use of the AQ-Adult on a sample of parents with children having ASD. They proposed a new 5-factor model with five subscales, namely, Socialness, Mind-reading, Patterns, Attention to Details and Attention Switching. However, parents of children with ASD are only presumed to have autistic traits. This methodological concern limits the generalizability of this study’s results. Regarding the AQ-Adol and AQ-Child, factorial validity is only examined in the AQ-Child. One study reported a 4-factor structure with Mind-reading, Attention to Detail, Social Skills and Imagination subscales, which were found to be highly correlated with four subscales of the original AQ-Adult, respectively, that is, Communication, Attention to Detail, Social Skills and Imagination (Auyeung et al., 2008).
The above studies on the AQ mainly focus on testing its validity against a typically developing (TD) group, supporting its capability in discriminating children with ASD from normal children. Yet, the validity and utility of the AQ would be considerably enhanced, if it could be demonstrated to differentiate ASD from other common childhood disorders which display close symptomatology and thus offer challenges to differential screening. Attention-deficit/hyperactivity disorder (ADHD) is one such potential candidate with a prevalence of about 5% in Chinese and Westerners alike (Leung et al., 2008; Polanczyk et al., 2007), higher than the 1%–2% prevalence of ASD (Baron-Cohen et al., 2009; Sun et al., 2019). Both disorders are among the most common referrals to child and adolescent psychiatric clinics (Yuen, 2017). Children with ADHD are also reported to experience a lot of social difficulties, similar to children with ASD (Gardner & Gerdes, 2015; Ros & Graziano, 2018). On the contrary, other researchers propose that the two disorders are conceptually distinct and empirically separable and the resemblance in social difficulties may be superficial (Ronald et al., 2014). It would be important to evaluate if the AQ could distinguish ASD from ADHD, despite their symptomatic overlap of social difficulties, superficial or not. The capability of the AQ in doing so will further confirm its status as a more specific measure of ASD and not of other neurodevelopmental disorders such as ADHD. Furthermore, ADHD is commoner and thus provides a frequent challenge to the AQ’s differential screening capability.
Given a lack of validation of the AQ-Child and AQ-Adol for Chinese children/adolescents, the first aim of this study is to validate their Hong Kong Chinese version, that is, the AQ-Child-HK and AQ-Adol-HK. Second, this study will include a second psychiatric comparison group of ADHD, in addition to a usual TD group, to test whether the AQ-Child-HK and AQ-Adol-HK can distinguish ASD from ADHD – a more demanding requirement for an assessment tool. In other words, it should not only be capable in differentiating cases from non-cases, but it should also distinguish the targeted disorder from another common disorder for differential screening. Such capability significantly enhances the validity and utility of an assessment tool.
Methods
Measures
The AQ-Child and AQ-Adol are respectively parent-report, dimensional rating scales on ASD for childhood (4–11 years) and adolescence (12–17 years) (Auyeung et al., 2008; Baron-Cohen et al., 2006). Each contains 50 items spreading across five subscales, namely, Social Skills, Attention Switching, Attention to Detail, Communication and Imagination. However, most existing factor analytic studies fail to produce a 5-factor model which replicates the five subscales. Instead, most can only identify two to at most four subscales, that is, either Social Skill, Attention to Detail, Communication, or Imagination (Gomez et al., 2019; Kloosterman et al., 2011; Stewart & Austin, 2009). Given the uncertainty regarding the factor validity of the AQ, this study will only focus on the analysis of the total score from all 50 items.
The Chinese AQ-Child-HK and AQ-Adol-HK were translated by the Hong Kong Working Group on ASD. The standard procedure of translation and back-translation was followed. The Chinese version was finalized, using a panel consensus approach after a panel of clinical psychologists had carefully examined any discrepancies between the original, the translation and the back-translation.
The scoring of the AQ-Child-HK and AQ-Adol-HK in this study would follow that of the English AQ-Child with a 4-point Likert-type scale to capture further the dimensionality of ASD traits (Auyeung et al., 2008).
Participants
This study recruited three groups of participants in Hong Kong with an age range covering those for the AQ-Child-HK (age 4–11) and AQ-Adol-HK (age 12–17): (1) TD children (n = 1196 for AQ-Child-HK; n = 809 for AQ-Adol-HK); (2) children with ASD (n = 124 for AQ-Child-HK; n = 78 for AQ-Adol-HK), and (3) children with ADHD (n = 82 for AQ-Child-HK; n = 51 for AQ-Adol-HK). Demographic characteristics of the three groups are summarized in Table 1.
Demographic and diagnostic profiles of participants (standard deviation in parentheses).
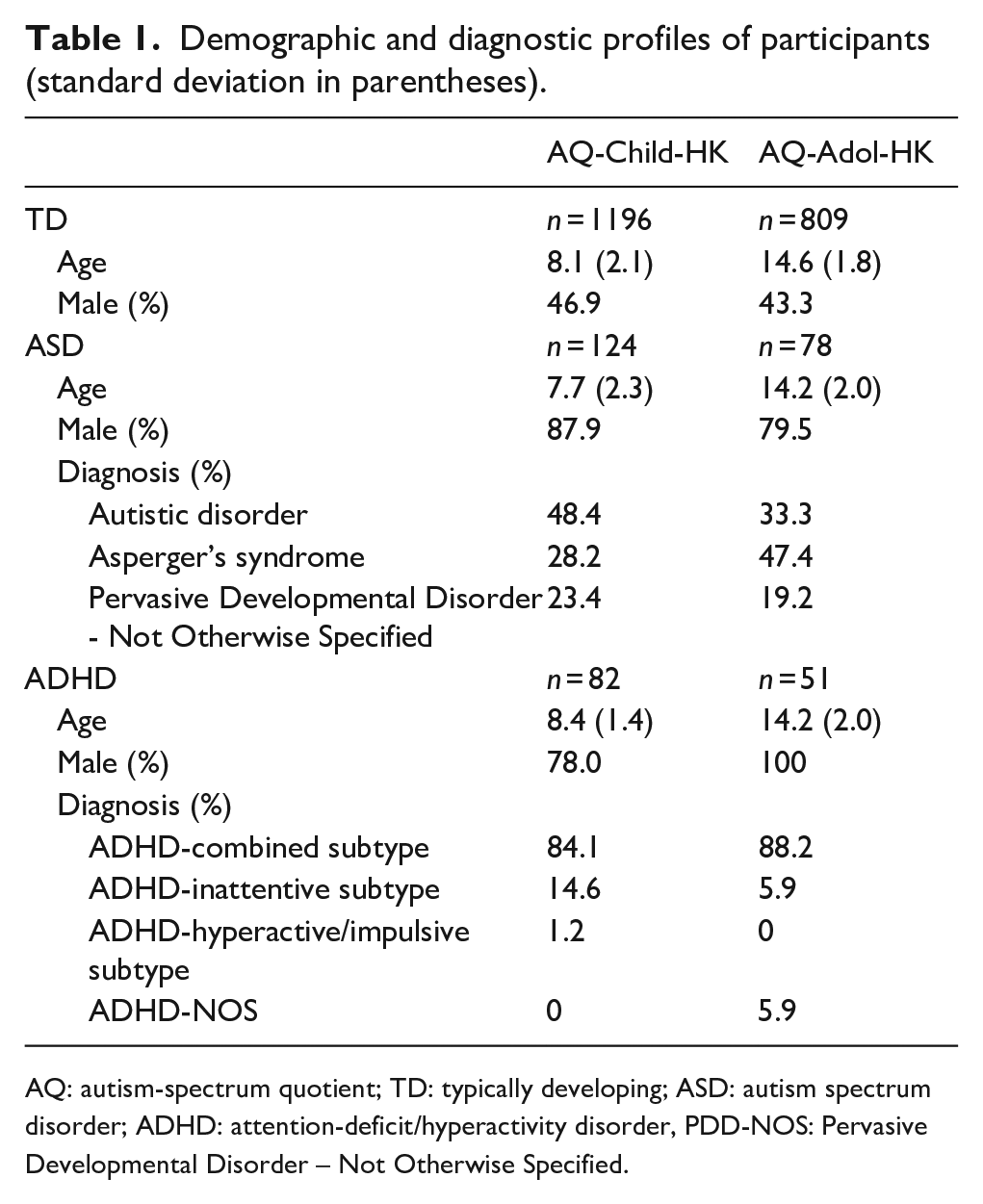
AQ: autism-spectrum quotient; TD: typically developing; ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder, PDD-NOS: Pervasive Developmental Disorder – Not Otherwise Specified.
Participants in the TD group were recruited from three mainstream kindergartens, three primary schools, and three secondary schools. Mainstream schools in Hong Kong are meant for children/adolescents with normal intelligence. Students who were known cases of neurodevelopmental or specific learning disorders were excluded. For the rest, four screening questions on emotional and behavioural problems were administered. Students whose parents endorsed any of the four items were also excluded to ensure the absence of psychiatric problems in this TD group.
Participants of the ASD and ADHD groups were recruited from two child assessment centres and one child/adolescent psychiatric clinic. Those with a diagnosis of intellectual disability (ID) in medical records or were studying in schools for children with ID were excluded. The diagnosis of ASD or ADHD was conferred by psychiatrists or clinical psychologists using Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition (DSM-IV-TR) criteria (APA, 2000). Those with a comorbid diagnosis were excluded. A substantial number of the participants, particularly those at adolescent ages, had received various types of intervention at different times. Yet, the attending psychiatrists or clinical psychologists confirmed that the severity of their condition at the time of this study still reached a diagnosable level, whether the disorder being ASD or ADHD.
Procedure
Approval had been obtained from relevant institutional ethics committees. For the TD group, students from each grade of the participating schools were recruited in order to ensure an even spread of different ages, with parents signing informed written consent on their behalf. Copies of the AQ-Child-HK or AQ-Adol-HK were thus distributed to the recruited students, and they were told to return them within 2 days. A subsample of students from each class was randomly selected for retest. These students were given copies of the retest questionnaire 2 weeks after their return of the first ones and were asked to return them within 2 days. A total of 207 copies of the AQ-Child-HK and 97 copies of the AQ-Adol-HK were then collected, which constituted 17.3% and 12.0% of the TD group for the AQ-Child-HK and AQ-Adol-HK, respectively.
For the ASD and ADHD groups, parents of recruited children were invited to complete the AQ-Child-HK or AQ-Adol-HK during their children’s follow-up visit to the child psychiatric clinic or assessment centres, after they had signed the informed written consent on behalf of their children. As for the retest, copies of the retest questionnaire were given to parents on the day of their completion of the first ones. They were instructed to complete and return them 2 weeks later by post. Altogether, for the AQ-Child-HK, 24 participants from the ASD group (19.4%) and 21 participants from the ADHD group (25.6%) returned the retest questionnaire. For the AQ-Adol-HK, 35 participants from the ASD group (44.9%) returned the retest questionnaire.
Statistical analysis
All statistical analysis in this study, including analysis of variance (ANOVA), Cronbach’s alpha test, exploratory factor analysis (EFA), and receiver-operating characteristics (ROC) curve analysis, was conducted using IBM SPSS Statistic 24. The exception was confirmatory factor analysis (CFA), which was conducted using EQS 6.4.
There was no community involved in this study.
Results
Effect of age, sex and socioeconomic status
In all three groups, age was not significantly associated with the total scores of the AQ-Child-HK (TD: r = 0.02, p = 0.45; ASD: r = –0.04, p = 0.64; ADHD: r = 0.02, p = 0.89), or of the AQ-Adol-HK (TD: r = –0.05, p = 0.15; ASD: r = –0.02, p = 0.84; ADHD: r = 0.18, p = 0.20).
Two-way ANOVA showed that there was also no significant main effect of gender (AQ-Child-HK: F(1, 1384) = 3.13, p = 0.08; AQ-Adol-HK: F(1, 876) = 0.29, p = 0.54) or interaction effect of group by gender (AQ-Child-HK: F(2, 1384) = 0.10, p = 0.91; AQ-Adol-HK: F(1, 876) = 0.96, p = 0.33). It should be noted that the adolescent ADHD group was excluded in this analysis for the AQ-Adol-HK since the group comprised of males only.
The total scores of the AQ-Child-HK and AQ-Adol-HK were respectively not correlated with indices of socioeconomic status (SES) such as household monthly income (r = –0.04, p = 0.15; r = 0.05, p = 0.13), father’s education level (r = –0.03, p = 0.27; r = 0.01, p = 0.73) and mother’s education level (r = –0.04, p = 0.18; r = 0.03, p = 0.38). Similar results were found in a separate analysis by group (due to space limitation, detailed figures available upon request).
Group comparison
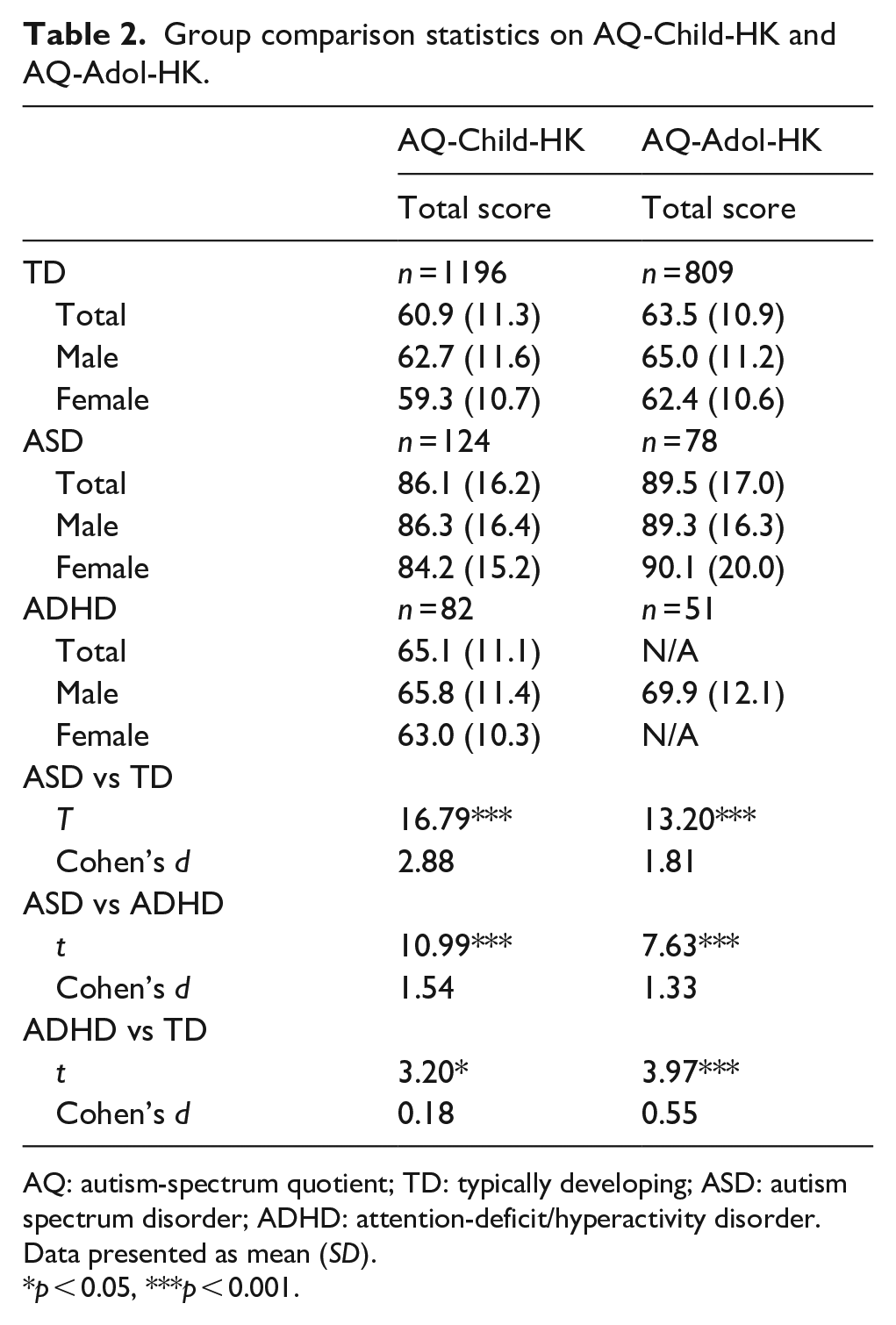
Using one-way ANOVA, significant between-group differences of the total score were indicated on both the AQ-Child-HK (F(2,1399) = 255.08, p < 0.001) and AQ-Adol-HK (F(2,935) = 179.09, p < 0.001). These tests were followed by pairwise comparison between groups (t-test) and effect size computation (Cohen’s d) (See Table 2 for details).
Group comparison statistics on AQ-Child-HK and AQ-Adol-HK.
AQ: autism-spectrum quotient; TD: typically developing; ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder.
Data presented as mean (SD).
p < 0.05, ***p < 0.001.
For both the AQ-Child-HK and AQ-Adol-HK, the total score was highest for the ASD group, which was significantly higher than those of the ADHD and TD groups with very large effect sizes (d = 1.33–2.88). Although the total score of the ADHD group was also significantly higher than that of the TD group on both the AQ-Child-HK and AQ-Adol-HK, the effect sizes were much modest (d = 0.18–0.55). Such effect sizes were unlikely to allow the two AQ measures to differentiate the ADHD group from the TD group effectively, as demonstrated by the ROC curve analysis reported below.
Internal consistency and test–retest reliability
The internal consistency (Cronbach’s alpha) of the AQ-Child-HK and AQ-Adol-HK was high at 0.80 and 0.82, respectively. Two hundred and fifty-two test–retest pairs on the AQ-Child-HK (TD = 207; ASD = 24; ADHD = 21), and 132 test–retest pairs on the AQ-Adol-HK (TD = 97; ASD = 35) were assessed for test–retest reliability. The intra-class correlation (ICC) coefficients were high, 0.80 for the AQ-Child-HK and 0.93 for the AQ-Adol-HK.
Factorial validity
AQ-Child-HK
The theoretical 5-factor structure proposed by Baron-Cohen et al. (2001) for the AQ-Child-HK was tested with CFA. The goodness of fit indices were poor (The Goodness-of-Fit Index (GFI) = 0.898, the Adjusted Goodness-of-Fit Index (AGFI) = 0.888, the Normed Fit Index (NFI) = 0.157, the Nonnormed Fit Index (NNFI) = 0.150, the Comparative Fit Index (CFI) = 0.192).
An EFA was subsequently conducted on the AQ-Child-HK to explore alternative factor structures. Given that the Kaiser–Meyer–Oklin value was satisfactory (0.90) and the result of the Bartlett’s test of sphericity was significant (χ21225 = 15376, p < .001), the assumption criteria for EFA were considered met. A principal component analysis with an oblique rotation was conducted, following the procedure of the original study of the AQ-Child (Auyeung et al., 2008). A forced 5-factor solution was performed. The rotated 37-item solution explained a total of 37.36% of the variance (see Table 3). The internal consistency of the first three factors was high, ranging from 0.70 to 0.85. They could be named as Social Skills, Attention to Details, and Communication. They were found to be highly correlated with the original AQ subscales of Social Skills (r = 0.87), Attention to Detail (r = 0.93) and Communication (r = 0.86), respectively. Thus, three out of the five original factors could be considered to be replicated in the AQ-Child-HK, excluding the factors of Attention Switching and Imagination. The last two factors of this EFA were uninterpretable with a mixture of items of diverse contents.
Factor structure of the AQ-Child-HK and AQ-Adol-HK.
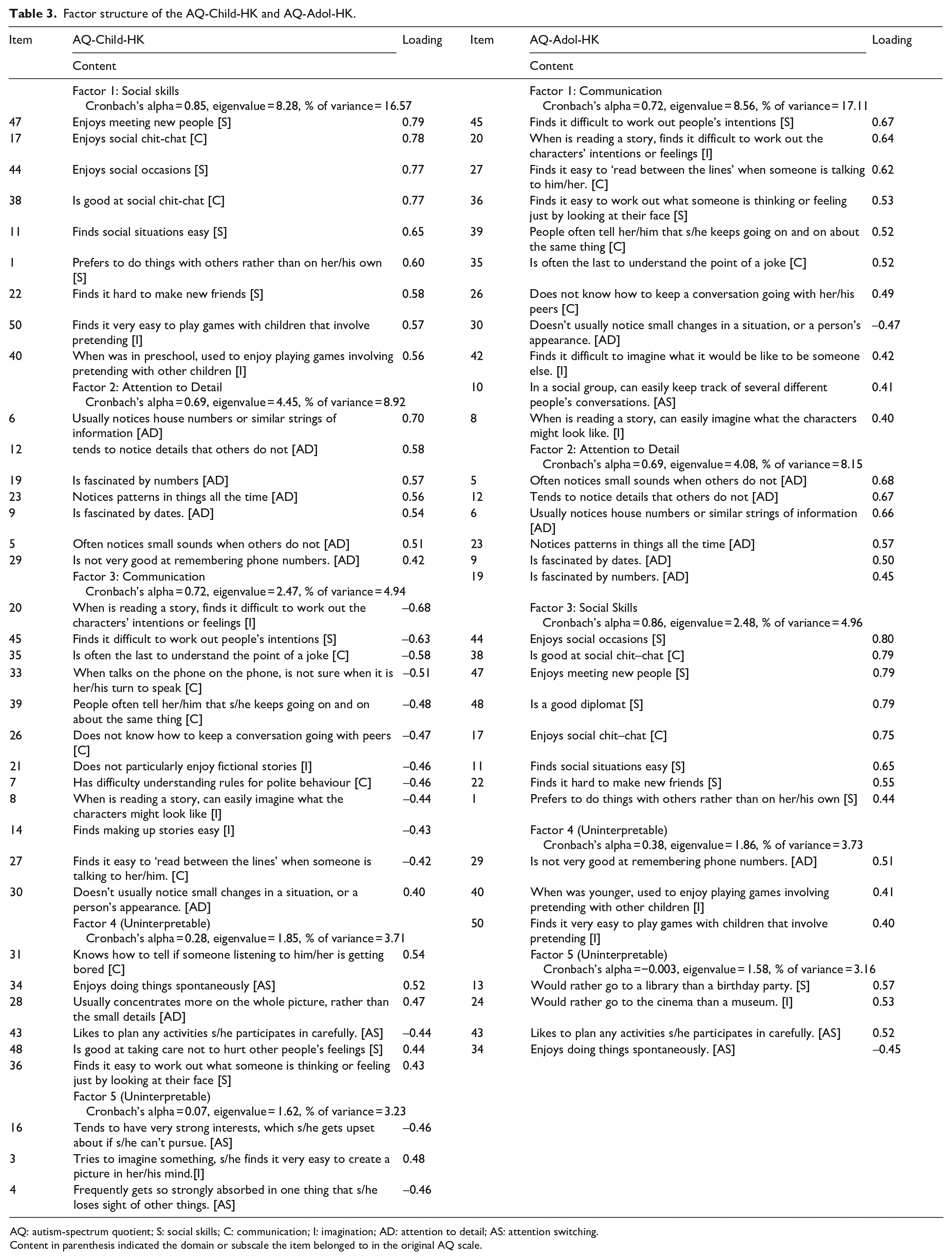
AQ: autism-spectrum quotient; S: social skills; C: communication; I: imagination; AD: attention to detail; AS: attention switching.
Content in parenthesis indicated the domain or subscale the item belonged to in the original AQ scale.
AQ-Adol-HK
The theoretical 5-factor structure proposed by Baron-Cohen et al. (2001) for the AQ-Adol-HK was tested with CFA. The goodness of fit indices were unsatisfactory (GFI = 0.711, AGFI = 0.683, NFI = 0.547, NNFI = 0.588, CFI = 0.608).
An EFA was subsequently conducted on the AQ-Adol to explore alternative factor structures. Given that the Kaiser–Meyer–Oklin value was satisfactory (0.89) and the Bartlett’s test of sphericity was significant (χ21225 = 10836 p < .001), the assumption criteria for EFA were met. A principal component analysis with an oblique rotation was conducted, forcing 5-factor solution. The rotated 31-item solution explained a total of 37.11% of the variance (Table 3). The internal consistency of the first three factors was high, ranging from 0.69 to 0.85. They could be named Communication, Attention to Detail, and Social Skills, with the last two factors being uninterpretable. The former three factors were highly correlated with the original AQ subscales of Communication (r = 0.82), Attention to Detail (r = 0.86), and Social Skills (r = 0.92), respectively. Therefore, three out of the five original factors could be considered as replicated in the AQ-Adol-HK, except for the factors of Attention Switching and Imagination subscales.
Cutoff scores
Receiver-operating characteristics (ROC) curve analysis was conducted to examine the sensitivity and specificity of the AQ-Child-HK and AQ-Adol-HK. The Areas under ROC Curve (AUCs) were summarized in Table 4.
Area under ROC curve (AUC) in AQ-Child-HK and AQ-Adol-HK.
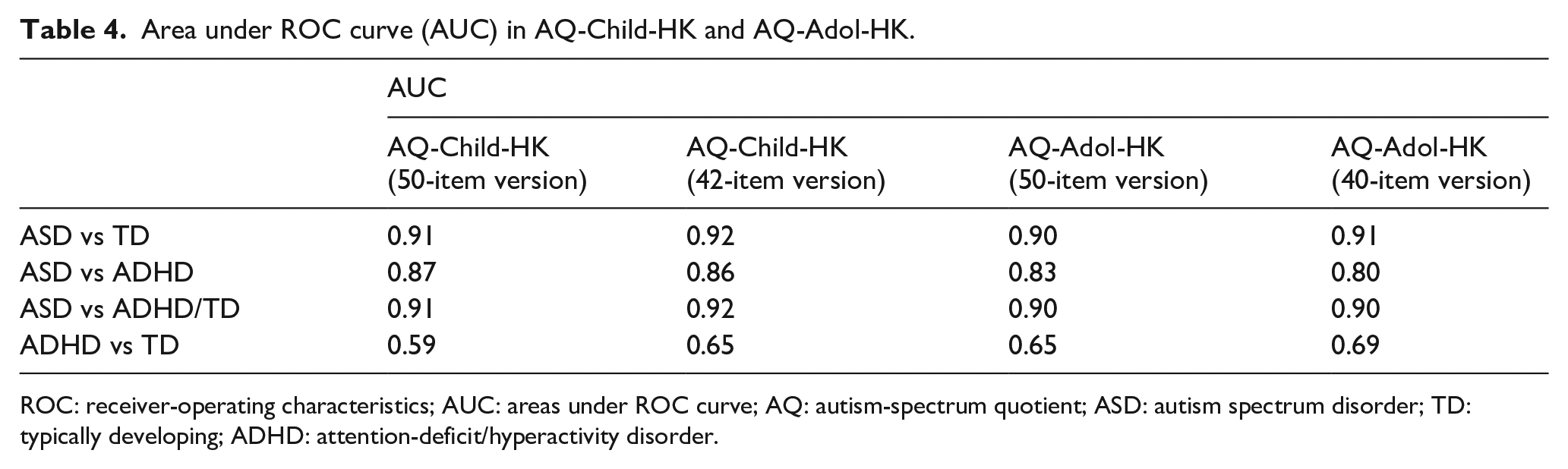
ROC: receiver-operating characteristics; AUC: areas under ROC curve; AQ: autism-spectrum quotient; ASD: autism spectrum disorder; TD: typically developing; ADHD: attention-deficit/hyperactivity disorder.
The AQ-Child-HK and AQ-Adol-HK showed that their total scores were competent in differentiating between the ASD and TD groups, given large AUCs of 0.91 and 0.90 respectively. In terms of differentiating ASD from ADHD, the AUCs attained were also sizable, 0.87 and 0.83, respectively for both the AQ-Child-HK and AQ-Adol-HK. However, when comparing between the ADHD and TD groups, their score differences on the AQ-Child-HK and AQ-Adol-HK, as reported above, were relatively modest; thus, the AUCs attained were small, 0.59 and 0.65, respectively, indicating that the two AQ questionnaires were ineffective in distinguishing the two groups.
The simple rule of using the highest summation of sensitivity and specificity figures was adopted to determine the optimal cutoff scores to differentiate between the ASD and TD groups. This rule yielded a similar score of 76 for both the AQ-Child-HK (sensitivity: 81%; specificity: 91%) and AQ-Adol-HK (sensitivity: 79.5%, specificity: 87.1%).
As the ADHD and TD groups could not be differentiated from each other on the AQ-Child-HK and AQ-Adol-HK, they were combined to form a single, non-ASD group to be contrasted with the ASD group. ROC curve analysis showed that large AUCs achieved on both the AQ measures, respectively, 0.91 and 0.90. The optimal cutoff score was found to be 76 again for both the AQ-Child-HK and AQ-Adol-HK with respective sensitivity of 81%/79.5% and specificity of 90%/86.2%.
Item analysis and shortened versions
On the AQ-Child-HK, items 9, 13, 24, 25, 29, 30, 43 and 49 were found to be unable to discriminate between the ASD and TD groups significantly (p > .05) (given space limitation, detailed figures available upon request). Among them, item 29, 30 and 49 had already been inappropriate for young children in the original AQ-Child’s study (Auyeung et al., 2008). Thus, a shortened 42-item AQ-Child-HK could be created by removing the above eight items.
On the AQ-Adol-HK, items 3, 9, 13, 19, 24, 25, 29, 30, 43 and 49 were also found to be unable to significantly discriminate the ASD and TD groups (p > .05) (given space limitation, detailed figures available upon request). Thus, a shortened 40-item AQ-Adol-HK could be created by removing the above 10 items.
All the above analysis was repeated with the two shortened versions. Results were largely similar to those of the original longer versions such as lack of significant age, gender and SES effects, as well as comparable internal consistency, test–retest reliability, factor structure, and AUCs. Particularly, Table 4 lists the AUCs between the shortened and original versions, indicating similar capability in differentiating across the ASD, ADHD and TD groups (given space limitation, detailed figures of other analysis available upon request).
Discussion
AQ and demographics
Age, gender and SES are not associated with the total score of both the AQ-Child-HK and AQ-Adol-HK. This is consistent with the findings reported in other language versions of the AQ (e.g. Auyeung et al., 2008; Baron-Cohen et al., 2006; Wakabayashi et al., 2007), suggesting that the assessment of autistic traits by the AQ is not moderated by common sociodemographic variables. This is encouraging, since these two screening tools can thus be equally applicable to the children/adolescents of different age, gender and SES.
Psychometric properties of the AQ
In terms of reliability, the internal consistency for the total score is high for both the AQ-Child-HK (α = 0.80) and AQ-Adol-HK (α = 0.82), while their test–retest reliability is equally satisfactory (ICC = 0.80 and 0.93, respectively). These high figures are consistent with findings on the AQ-Child and AQ-Adol in the United Kingdom and other countries (Auyeung et al., 2008; Baron-Cohen et al., 2006; Sonié et al., 2013; Wakabayashi et al., 2007).
The total score of the AQ-Child-HK and AQ-Adol-HK differentiates the ASD and TD groups with large effect sizes (d = 2.88 and 1.81, respectively). These expectedly lead to correspondingly large AUCs, 0.91 and 0.90, respectively, underlining the high discriminative power of the two AQ questionnaires in identifying children/adolescents with ASD from their TD peers. The optimal cutoff point is 76 for both questionnaires with satisfactory sensitivity and specificity (79.5% to 91%). These figures are largely within the range to existing findings on these two questionnaires, ranging from 72.7% to 100% (Auyeung et al., 2008; Baron-Cohen et al., 2006; Wakabayashi et al., 2007).
CFA is unable to confirm the factorial validity of a five-factor model or the five subscales of the AQ. Alternatively, EFA of both the AQ-Child-HK and AQ-Adol-HK is able to identify the same three comparable factors of the original AQ, namely, Social Skills, Attention to Detail, and Communication. These convergent findings seem to collaborate well with those of previous studies in various languages (Austin, 2005; Auyeung et al., 2008; Hoekstra et al., 2008; Hurst et al., 2007; Kloosterman et al., 2011; Stewart & Austin, 2009). The three factors/subscales that this study identifies have been the most frequently replicated. Thus, besides the total score, more confidence can be given to subscale scores on Social Skills, Attention to Detail, and Communication. Furthermore, these three factors/subscales may constitute the core features of ASD across cultures.
Item analysis of the AQ-Child-HK and AQ-Adol-HK shows that a largely overlapping set of items (9,13,24,25,29,30,43 and 49), with the exception of two (3 and 19), that are less discriminative in the Hong Kong context. This finding of overlapping items suggests that these identified items may not be just sample or age specific. On closer examination, some of these items tap into preferences in social/leisure activities, for example, item 13 ‘rather go to a library than a birthday party’, item 24 ‘rather go to the cinema than a museum’ and item 43 ‘likes to plan any activities s/he participates in carefully’. Parents in Hong Kong tend to control their children’s schedules/activities tightly, given the very competitive local educational environment. Little choice and time are available for children/adolescents to plan and initiate their own preferred social/leisure activities.
Preference in numbers and dates is not uncommon among children/adolescents with ASD in Hong Kong. Yet, the under- or over-endorsement of Hong Kong parents on some items, for example, item 9 ‘fascinated by dates’, item 29 ‘not very good at remembering phone numbers’, and item 49 ‘not very good at remembering people’s date of birth’, may once again be related to the local competitive schooling. Local parents usually push their children hard to develop good rote memory for achieving high marks in examinations. They will not be satisfied with some even better-than-average performance from their children with ASD.
Yet, analysis of the shortened versions of the AQ-Child-HK and AQ-Adol-HK reports similar findings as those of the original versions. Importantly, the AUCs between them are almost identical in identifying children/adolescents with ASD from their TD peers (AQ-Child-HK: 0.92 vs 0.91; AQ-Adol-HK: 0.91 vs 0.90). In other words, the presence of less-discriminative items does not seem to hurt the original versions. Or, the locally shortened versions do not apparently improve their discriminative capability. Though there may be local explanations for some of the items to be less discriminative, it plays safe to recommend the continual use of the equally discriminative original versions in Hong Kong, until future study consistently identifies the same set of non-discriminative items. For the time being, the lack of differences in discriminative power between the original and locally shortened versions suggests the cross-cultural applicability of the two AQ questionnaires in screening ASD in children/adolescents, as well as the cross-cultural validity of some of the core ASD traits that these questionnaires encompass.
Screening specificity of the AQ
The second aim of this study is to examine the screening specificity of the AQ-Child-HK and AQ-Adol-HK to differentiate between ASD and ADHD. Many existing psychometric studies on assessment tools, including those of the AQ, mainly use one single comparison group, mostly a TD sample. Unfortunately, this methodological design can only prove that a measure can identify cases from non-cases; it does not attest to whether a measure is specific to a particular disorder such as ASD. It is only when a psychiatric comparison group, on top of the TD group, is added, then it is methodologically sound to demonstrate whether the measure in question is able to differentiate different psychiatric disorders and can thus start to claim to be specific to one targeted disorder. This study, given the additional comparison group of children/adolescents with ADHD, represents a methodological improvement to begin testing whether the AQ is indeed a measure of ASD only and not of other child and adolescent disorders. So far, there is only one study examining this issue with the AQ-Adult (Sizoo et al., 2009). As for the AQ-Child and AQ-Adol, there is no such report in the literature. Our results show that the ASD group’s AQ scores are significantly higher than those of the ADHD group with large effect sizes and AUCs (AQ-Child-HK: Cohen’s d = 1.54, AUCs = 0.87; AQ-Adol-HK: Cohen’s d = 1.33, AUC = 0.83). These results compare favourably with the effect size (d = 1.12) reported on the previous AQ-Adult study contrasting these two disorders (Sizoo et al., 2009).
On the contrary, though the ADHD group’s AQ-Child-HK and AQ-Adol-HK scores are statistically higher than those of the TD group, they only achieve small-to-moderate effect sizes (d = 0.18–0.55). Closer inspection reveals that the ADHD group tends to score higher than the TD group in items on Communication and Attention Switching subscales, for example, item 4 ‘frequently gets so strongly absorbed in one thing that s/he loses sight of other things’ and item 7 ‘has difficulty understanding rules for polite behaviour’, which are likely to be associated with the inattentive and impulsive features of ADHD. These findings echo the clinical observation of overlapping behavioural symptomatology between ASD and ADHD (Antshel & Russo, 2019). Nevertheless, the AUC analysis suggests that both the AQ-Child-HK and AQ-Adol-HK are unable to distinguish between the ADHD and TD groups effectively (AUCs = 0.59–0.65). The AQ-Child-HK and AQ-Adol-HK are thus not measures of ADHD or general psychopathology. Their ability to differentiate between ASD and ADHD/TD groups, but not between the latter two, supports the screening specificity of the AQ in identifying ASD, as it is originally designed to be, despite the claimed shared symptomatology of ADHD and ASD in social difficulties.
For practical use in screening ASD, an optimal cutoff score in differentiating the three groups of this study, that is, the ASD, ADHD and TD groups, is identified with the latter two groups combined. A similar cutoff score of 76 is yielded for both the AQ-Child-HK and AQ-Adol-HK, as in the case of differentiating between the ASD and TD groups. This is not unexpected, given TD children/adolescents constituting the majority in the combined ADHD/TD group. Nonetheless, a single cutoff score for screening the ASD group from the TD group and from the ADHD and TD groups combined is welcome for the practical purpose because separate cutoff scores will be cumbersome.
It should be noted in Table 4 that the majority of the AUCs between the original and locally shortened versions of the AQ-Child-HK and AQ-Adol-HK in discriminating the ASD group from the ADHD and TD/ADHD groups, as well as the ADHD group from the TD group are close to be almost identical. These back our earlier recommendation for the continual use of the original versions in Hong Kong.
Limitations
This study has several limitations. First, only one psychiatric comparison group of ADHD is chosen to be included in this study because of suspected phenotypic overlaps between it and ASD, for example, social difficulties (Gardner & Gerdes, 2015; Ros & Graziano, 2018). The screening specificity of the AQ on ASD cannot be further confirmed without involving more child and adolescent psychiatric disorders as control. Second, the clinical diagnosis of the two clinical groups is not reconfirmed by a standardized diagnostic instrument. Nonetheless, the ASD and ADHD participants are all under active follow-up at a child psychiatric clinic. Their attending clinicians reaffirm their clinical diagnosis before referring them for participation in this study. This updated re-affirmation of the clinical diagnosis of ASD or ADHD gives confidence to their validity. Third, while the sample size of the TD group can be considered as large with about 2000, the combined sample size of the two clinical groups is relatively small, totaling only 335. Finally, there is no involvement of an adolescent ADHD group in the examination of test–retest reliability for the AQ-Adol-HK.
Conclusion
Both the AQ-Child-HK and AQ-Adol-HK demonstrate satisfactory psychometric properties in screening ASD, comparable to those of other language versions of the AQ across cultures. In this study, they additionally prove their screening specificity by differentiating ASD from another common child psychiatric disorder, ADHD, which shares potential phenotypic overlap with ASD in social difficulties. The two AQ questionnaires cannot differentiate between the ADHD and TD groups, and thus do not misclassify ADHD as ASD. These findings support that the AQ-Child-HK and AQ-Adol-HK are not general measures of child and adolescent psychopathology but can claim to be more specific measures of ASD, given their success in identifying the ASD group from the ADHD/TD groups, while failing to differentiate the latter two.