
Abstract
Little is known about the alliance between therapists and children with autism spectrum disorder who are receiving psychological therapies in outpatient treatment settings. This study examined the therapeutic alliance in children with autism spectrum disorder and clinical anxiety, who were receiving cognitive behavioral therapy in a randomized, controlled trial. The Therapeutic Alliance Scale for Children was administered to a sample of children and youth with autism spectrum disorder and anxiety (N = 64; aged 7–14) as well as to their parents and therapists. A comparison sample of typically developing youth with clinical anxiety (N = 36; aged 5–12) was included. The child-therapist alliance was more positive among typically developing children than among children with autism spectrum disorder; correspondingly, the parent-therapist alliance was also more positive among parents of typically developing children. Therapist reports of positive child-therapist alliance predicted post-treatment reductions in anxiety among children with autism spectrum disorder, although child reports of this alliance did not. Parent reports of positive parent-therapist alliance also predicted post-treatment reductions in the child’s anxiety in the group with autism spectrum disorder. A strong therapeutic alliance appears to be associated with better treatment outcomes in children with autism spectrum disorder receiving cognitive behavioral therapy, although a thoughtful and diagnostically sensitive approach is advisable to promote a positive alliance with children with autism spectrum disorder.
Autism spectrum disorders (ASDs) are lifelong neurodevelopmental conditions characterized by deficits in social communication and repetitive behaviors (American Psychiatric Association, 2013). However, several decades of research have produced numerous interventions that are capable of remediating core and comorbid symptoms (i.e. evidence-based interventions (EBIs)). While these advances have led to a significantly improved long-term prognosis for individuals with ASD, it remains unclear why certain interventions are efficacious.
The field has become increasingly concerned with translating EBIs from university settings to school and community settings in which more children will be able to access them (Kasari & Smith, 2013). In order to facilitate successful dissemination of EBIs, it is important to identify intervention characteristics—specific and nonspecific—associated with successful treatment outcomes in EBI implementation (Kasari & Smith, 2013; Wood, McLeod, Klebanoff, & Brookman-Frazee, 2015). Specific factors such as particular behavioral practices (e.g. extinction) have been studied in numerous trials for children with ASD. However, studies examining the effect of nonspecific factors such as the role of the therapeutic alliance in EBIs for ASD are sparse.
The therapeutic alliance, defined as the emotional and collaborative elements of the relationship between client and therapist, has long been viewed as an influential factor in many types of psychotherapy (e.g. McLeod, 2011). The therapeutic alliance encompasses several related components, such as engagement, therapists’ warmth, and the bond between client and therapist (Shirk & Karver, 2003). While the literature on relational variables in psychotherapy typically defines the therapeutic relationship as the extent to which the client and therapist like or feel close with one another, the therapeutic alliance has come to refer to a broader set of relational variables. The therapeutic alliance includes not only the therapeutic relationship, but also factors such as agreement on therapeutic goals and tasks related to the pursuit of therapeutic goals (Luborsky, 1994).
The origin of the study of the therapeutic alliance can be traced back to psychoanalytic conceptions of transference and countertransference (Freud, 1912). Conceptualizations of the therapeutic bond continued to evolve and first underwent empirical testing in Orlinsky and Howard’s (1975) examination of the relationship between therapist credibility and client engagement with treatment outcome. Orlinsky and Howard (1975) formulated a definition of alliance encompassing working alliance (client and therapist investment in therapy), empathic resonance, and mutual affirmation. Bordin (1979) went on to develop the modern conceptualization of the alliance, which also consists of three dimensions: (1) the bond or affective aspects of the relationship, (2) the therapists’ ability to engage the client in therapeutic tasks, and (3) agreement between client and therapist about the goals of therapy. When all components of the alliance are present, clients are more engaged in the therapeutic process (Chiu, McLeod, Har, & Wood, 2009).
Several meta-analyses have found that the therapeutic alliance consistently predicts outcomes across various types of treatments and measurements in both adult and child psychotherapy (e.g. Horvath & Bedi, 2002; McLeod, 2011). Effect sizes found in adult psychotherapy have been moderate (r = 0.27; Horvath, Del Re, Flückiger, & Symonds, 2011). Smaller effects have been found in child psychotherapy (r = 0.14–0.22; McLeod, 2011; Shirk & Karver, 2003). However, this may be due to factors such as methodological flaws, inconsistent measurement of alliance, and the existence of multiple, important moderators of the alliance-outcome association (McLeod, 2011). While there is less research on the alliance in child psychotherapy, a comprehensive meta-analysis has revealed that child- and parent-therapist alliances were similarly related to outcomes and that the strength of the relationship varied across type of treatment (i.e. individual versus family based), child characteristics, and method of assessment (McLeod, 2011). For example, the alliance-outcome association was found to be stronger for children versus adolescents (ES = 0.20), treatment seeking families (ES = 0.27), and youth with externalizing (ES = 0.20) or a mixture of presenting problems (ES = 0.24) (McLeod, 2011).
In this study, we examined the effects of the alliance in an evidence-based psychotherapy treatment for families of youth with ASD, personalized cognitive behavioral therapy (P-CBT). In the past decade, researchers have begun to explore the use of cognitive-behavioral psychotherapy approaches with children with ASD. CBT approaches have continued to gain ground, demonstrating promise for treating both core symptoms as well as frequently occurring comorbidities (e.g. Danial & Wood, 2013). In particular, P-CBT for youth with ASD and comorbid anxiety, which combines traditional CBT techniques, adaptations for youth with ASD, and parent and teacher involvement, has met the criteria as a probably efficacious treatment (Danial & Wood, 2013). P-CBT is a variant of modular CBT (cf. Chorpita & Weisz, 2009). The specific session content/modules chosen for a specific child, and the number of times a session type/module is repeated, varies from child to child in this variant of CBT because it is personalized to the child’s presenting symptoms and clinical response during CBT (Sze & Wood, 2007, 2008). This variant of CBT differs from other CBT programs for youth (with or without ASD) which progress in a linear, preset manner. One form of modular CBT has been found to be more effective than linear CBT in a large-scale clinical trial with typically developing (TD) youth (Weisz et al., 2012), possibly because it can be personalized to clinical need and youth response.
A recent meta-analysis found the effect of the alliance in CBT to be equivalent to the effect found in other types of treatments (Flückiger, Del Re, Wampold, Symonds, & Horvath, 2012). Therapeutic alliance may be particularly important in child CBT because youth participants are often not self-selecting, so alliance is needed to engage them in therapy (Marker, Comer, Abramova, & Kendall, 2013). Furthermore, because CBT requires active participation on the part of youth, engagement is critical and a trusting relationship between youth and therapist may be key to facilitating exposure tasks, an important and challenging aspect of CBT (Chiu et al., 2009).
As yet, very little is known about the role of therapeutic alliance in interventions for school-aged youth with ASD. To date, there have been a few empirical studies on therapeutic alliance in interventions for youth with ASD and all have focused exclusively on parent-therapist alliance. In a study on the impact of working alliance between parents and therapists on consultation and treatment in an early intensive behavioral intervention for children with autism, Myers (2008) found that higher parent-reported ratings of alliance were associated with increased parent and child progress. Another study on alliance between mothers of toddlers with autism and behavioral intervention providers revealed that maternal reports of stronger alliances with therapists were associated with lower levels of distress and higher levels of wellbeing (Davis, 2008).
All that is currently known about child-therapist alliance in interventions for school-aged youth with ASD originates from qualitative case studies. Although it is difficult to draw firm conclusions from case studies on therapy with youth with ASD, several key themes have emerged. The first is that forming an alliance with children and adolescents with ASD is possible, but can challenge therapists’ assumptions and expertise (Benda, 2002; Pope, 1993; Ramsay et al., 2005). Other themes are that alliance is important in psychotherapy with individuals with ASD, because it serves as a model for relationships with others (Pope, 1993), provides a “laboratory” to learn and practice social skills and receive feedback (Ramsay et al., 2005), and helps clients with ASD to improve their overall functioning by providing them with a better understanding of themselves and others (Ramsay et al., 2005). Taken together, the extant literature on child and parent-therapist alliance suggests that therapeutic alliance may be an important factor in interventions for youth with ASD, but more research is necessary in order to address this question.
Although there is not a great deal of research on the therapeutic alliance in ASD, there is some research on therapeutic alliance in clinical populations similar to ASD that has possible implications for this study. The strength of the alliance has been shown to be associated with CBT outcomes for children with disorders that are commonly comorbid for youth with ASD, such as oppositional defiant disorder (ODD), conduct disorder (CD) (Gerstein et al., 2011; Kazdin & Durbin, 2012), and anxiety disorders (Chiu et al., 2009; McLeod, 2011). While research on alliance is also sparse in these areas, it provides support for the predicted association between alliance and outcome in CBT for youth with ASD and clinical anxiety in this study.
This study
In order to assess the nature and function of the therapeutic alliance in P-CBT for youth with ASD, we compared a sample of youth with ASD and an anxiety disorder receiving P-CBT to a sample of TD youth with an anxiety disorder receiving a comparable P-CBT program. The goals of the study were threefold. First, we explored the possible differences in therapeutic alliance in children with ASD and TD children. Related subgoals involved examining the internal consistency of self-report of alliance in ASD youth and the concordance of child-report and therapist-report of alliance among ASD youth. Second, we explored whether or not therapeutic alliance predicts treatment outcomes for youth with ASD, as it does for TD youth. A subgoal here was to examine whether or not parent-therapist alliance is more important for youth with ASD than it is for TD youth in predicting outcomes. Third, we explored developmental differences in the alliance-outcome linkage in youth with ASD. Our hypotheses were as follows:
The therapeutic alliance will be weaker for children with ASD and clinical anxiety than for TD children with clinical anxiety.
A positive therapeutic alliance will predict greater reductions in anxiety severity for children with ASD and anxiety, with the parent-therapist alliance emerging as a stronger predictor than the child-therapist alliance.
Methods
Participants
The sample included 100 children aged 5–15 years and their primary parents (i.e. the parent primarily responsible for the child who volunteered to attend weekly therapy sessions) residing in an urban area of the western United States. In all, 36 of the children were TD with an anxiety disorder and 64 children had both ASD and an anxiety disorder. The sample consisted of participants from four randomized controlled trials (RCTs) of P-CBT for child anxiety who completed therapeutic alliance measures (Chiu et al., 2013; Fujii et al., 2012; Wood et al., 2009; Wood et al., 2015). One of the RCTs included TD children with anxiety and the other three included children with ASD and co-occurring anxiety (see Table 1 for details about each RCT-based subsample). In the RCT including TD children with anxiety (Chiu et al., 2013), children aged 5–12 years old were randomly assigned to P-CBT (the Building Confidence Program; (Wood, McLeod, Hiruma, & Phan, 2008; Wood, Piacentini, Southam-gerow, Chu, & Sigman, 2006) or a waitlist condition followed by receiving P-CBT. TD children were referred by school psychologists and teachers, who received a letter about the study. In the three RCTs for children with ASD and anxiety (Fujii et al., 2012; Wood et al.,2009, 2015, 2015), children received P-CBT based on the Building Confidence Program with adaptations for youth with ASD, such as a social coaching module. In all three RCTs for children with ASD and clinical anxiety, children aged 7–15 were randomly assigned to either immediate treatment ((IT)P-CBT) or a waitlist control group, which was followed by receiving P-CBT. Children were referred by a medical center-based autism clinic, regional centers, school staff, and parent support groups. In the ASD plus anxiety group, the average age was 10.8 years old. In the TD plus anxiety group, the average age was 8.4 years old (see Table 2 for full sample description).
Details of four RCTs used for the combined sample in this study.
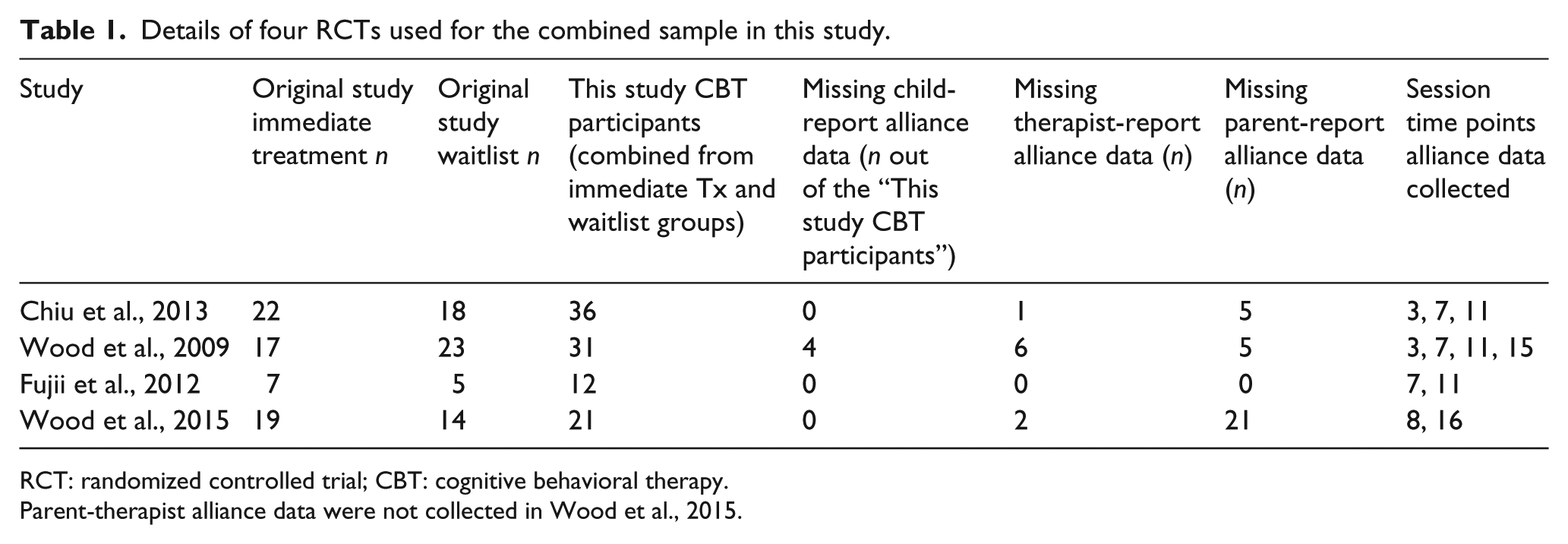
RCT: randomized controlled trial; CBT: cognitive behavioral therapy.
Parent-therapist alliance data were not collected in Wood et al., 2015.
Participant demographics.
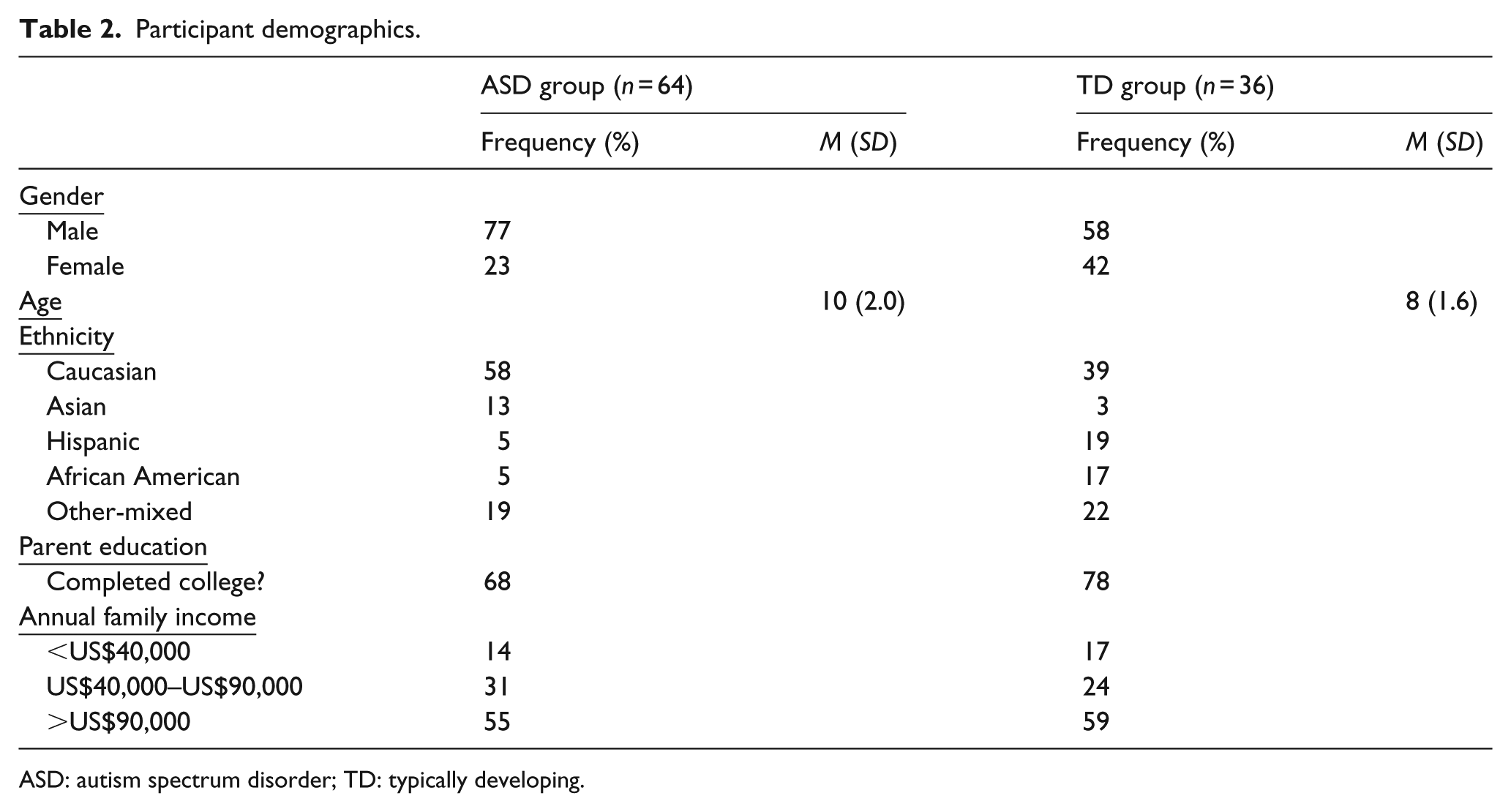
ASD: autism spectrum disorder; TD: typically developing.
In each of the four RCTs that we drew from for the combined sample in this study, approximately half of the participants were randomized to immediate P-CBT, and the other half to a 3-month waitlist (or, in the case of Fujii et al., 2012, to treatment-as-usual (TAU)). Following the waitlist/TAU period, families received the same P-CBT treatment as those randomized to IT. Most waitlist families provided therapeutic alliance ratings once they began P-CBT and also provided post-treatment outcome data following P-CBT. Hence, for this study, the IT and waitlist/TAU groups were combined for all analyses; all families with therapeutic alliance measures pertaining to P-CBT were included in analyses regardless of randomization status. Table 1 provides the published sample sizes for the IT and waitlist/TAU groups for each original study, as well as the combined sample sizes of the two groups that were included in this study analyses (i.e. those with alliance data). Note that the Wood et al., (2015) study was a three-site study and that only data from the present authors’ study site was utilized in these analyses. Also noted in Table 1 are the session time points at which the therapeutic alliance was measured and the amount of missing alliance data for each of the three informants (note that parent-therapist alliance data were not collected in Wood et al., 2015). The therapeutic alliance data from the four RCTs have not been analyzed or published previously.
In order to be included in the RCT for TD children with anxiety disorders, participants had to (1) meet the research criteria for either separation anxiety disorder (SAD), social phobia, generalized anxiety disorder, or obsessive compulsive disorder (OCD) and (2) maintain a stable dosage of psychiatric medication, if on medication at the baseline assessment (i.e. if on medication, waited at least 1 month at a stable dose before completing the baseline assessment). In order to be included in the RCTs for children with ASD and anxiety, participants had to meet the above criteria while also meeting research criteria for a diagnosis of ASD on the ADOS and ADI-R (see below). Families of children with ASD were excluded if the child had an IQ score of less than 70. All participants in this study also met the following inclusion criteria: (1) availability of measures of Therapeutic Alliance Scale for Children Revised (TAS-C/P; Shirk & Saiz, 1992) completed by the child, parent, or therapist during sessions 3, 7, 8, 11, 15, or 16 (see Table 1), (2) no missing diagnostic measures, and (3) family participated in P-CBT treatment, either immediately post-randomization or following a waitlist/TAU. All four RCTs have been approved by a university institutional review board. Children gave verbal or written assent and parents gave written informed consent to participate. Families were provided with a small honorarium for their participation in pre- and post-treatment assessments.
Measures
ASD diagnosis
The Autism Diagnostic Interview-Revised (ADI-R; Lord, Rutter, & Le Couteur, 1994) is a reliable and valid diagnostic assessment of ASDs for individuals with a mental age of 2 years and above. It is a 93-item parent-reported standardized interview, which includes assessment of communication, social, and repetitive behavior domains.
The Autism Diagnostic Observation Schedule (ADOS)—Module 3 (Lord, Rutter, DiLavore, & Risi, 2000) is a semi-structured observational assessment with excellent psychometric properties (Lord et al., 2000). It is administered to youth by trained independent evaluators (IEs) to allow for observation of social interaction, stereotyped behaviors, and atypical language use. In this study, module 3 of the ADOS was used, which is designed for children and adolescents who are verbally fluent.
Therapeutic alliance
The Therapeutic Alliance Scale for Children-Revised (TAS-C/P; Shirk & Saiz, 1992) is a 12-item four-point Likert-type scale measure administered to child, parent, and/or therapist. It assesses agreement between the therapist and the youth or parent regarding the tasks and goals of therapy (Task Scale; 6 items; “The child engaged with you in learning new ways of handling or coping with feelings”) and youth and parent affect toward the therapist (Bond Scale; 6 items; “I liked spending time with my therapist”) with 1 meaning not at all and 4 meaning very much. A total TAS-C/P score is calculated based on a composite of all 12 items and can range from 12 to 48, with higher scores indicating stronger therapeutic alliance. Children and therapists rated the child-therapist alliance, while parents rated the parent-therapist alliance. The TAS-P has demonstrated adequate internal consistency (α = 0.81), test–retest reliability (r = 0.82), temporal stability, convergent validity with therapist-reported alliance (r = 0.67), divergent validity with child-therapist alliance (intraclass correlation (ICC) = 0.40), and predictive validity (Accurso, Hawley, & Garland, 2013; Hawley & Weisz, 2005; Shirk & Saiz, 1992). The TAS-C has also shown adequate internal consistency (α = 0.88), test–retest reliability (r = 0.79), temporal stability, convergent validity with observational measures of alliance (r = 0.52), divergent validity with parent-therapist alliance (ICC = 0.40), and predictive validity (Accurso et al., 2013; Fjermestad et al., 2012; Hawley & Weisz, 2005; Kazdin, Marciano, & Whitley, 2005). However, the psychometric properties of the TAS-C have yet to be established in ASD samples.
Anxiety severity
The Anxiety Disorders Interview Schedule: Child and Parent Versions (ADIS-C/P; Silverman & Albano, 1996) is a semi-structured interview assessing the presence and severity of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) anxiety disorders and associated comorbid disorders. The ADIS-C/P is administered by trained IEs to both the child and the parent. The IEs make composite diagnoses and severity ratings based on the youth and parent interviews. A Clinician’s Severity Rating (CSR) score, ranging from 0 to 8 (with a higher score indicating greater anxiety), is generated for each anxiety disorder (e.g. SAD). A CSR score of 4 or greater qualifies as clinically significant. In this study, the participant’s highest CSR score was used as a measure of anxiety severity. The ADIS-C/P has sound psychometric properties in TD samples (Wood, Piacentini, Bergman, McCracken, & Barrios, 2002). There is also preliminary evidence suggesting favorable psychometric properties in ASD samples (Renno & Wood, 2013; Wood et al., 2009).
The Multidimensional Anxiety Scale for Children-Parent Report (MASC-P, March, Parker, Sullivan, Stallings, & Conners, 1997) is a 39-item parent-report Likert-type-scale measure of youth anxiety severity administered to the parent. It consists of four subscales assessing physical symptoms, social anxiety, harm/avoidance, and separation/panic. Preliminary evidence suggests favorable psychometric properties in ASD samples for parent report (α = 0.88; Bellini, 2004). There is also evidence of treatment sensitivity of the MASC-P in ASD populations (Wood et al., 2009). In this study, the total MASC-P scores were used as a measure of anxiety severity.
Procedure
Initial contact and baseline assessment
In each RCT, research staff made initial contact with families, conducting phone screens with parents to determine the child’s age, symptoms of anxiety, IQ, and, in the three ASD/anxiety RCTs, prior ASD diagnosis. The families who appeared to meet the eligibility criteria based on the phone screen were scheduled for an intake assessment. During the assessment, families completed consent and assent forms, diagnostic interviews, and self-report measures. Trained doctoral students and clinical psychologists blind to treatment condition administered the ADIS-P, MASC-P, and in the case of the ASD RCTs, the ADOS and ADI-R at the intake assessment.
Randomization and post-treatment assessment
Across RCTs, families that met the inclusion/exclusion criteria based on the intake assessment were randomized to either an IT or a waitlist/TAU condition by research staff using a computer randomization program. Post-treatment assessments, consisting of re-administering all anxiety measures, were completed within the last week of P-CBT.
Intervention phase: TD children with anxiety
TD children with anxiety and their primary parents received 12–16 therapy sessions lasting 60–80 min. Therapists followed the Building Confidence treatment manual for P-CBT (Wood et al., 2008). The therapists were nine clinical psychology doctoral students and one clinical psychologist. Training consisted of reading the treatment manual, participating in a workshop, conducting a supervised training case, and attending weekly group supervision meetings. The treatment consisted of three primary components: (1) training the child in skills such as relaxation strategies, emotion recognition, and cognitive reframing of feared situations, (2) training the parents in skills such as utilization of a reward system and communication techniques, and (3) graded exposure to feared situations paired with rewards.
Intervention phase: children with ASD and anxiety
Children with ASD and anxiety and their primary parents received 16 sessions of treatment lasting 90 min (30 min with the child and 60 min with the parent; note that 7 families in Fujii et al., 2012 received 32 sessions of treatment). Therapists followed a version of the Building Confidence treatment manual for P-CBT adapted for children with ASD and co-occurring anxiety. The therapists’ previous experience was variable, as there were two doctoral-level psychologists and 11 doctoral students in clinical or educational psychology. Training consisted of reading the treatment manual, 8 h of initial training, listening to recordings of treatment sessions conducted by a model therapist, and attending weekly group supervision meetings. The intervention components were similar to those used in the P-CBT intervention for TD children with anxiety, with added components addressing social skills and circumscribed interests and repetitive behaviors. The initial training, manual, and supervision all addressed clinical skills for successfully engaging with youth with ASD.
TAS-C/P collection
TAS-C/P measures were collected at least twice in each RCT, during sessions 3, 7, 8, 11, 15, or 16 (see Table 1). Parents completed the TAS-C/P in a private room separated from both the child and the therapist. Children completed the TAS-C/P in a private room with an undergraduate research assistant present to answer questions and provide clarification of items, if necessary. Undergraduate research assistants read the TAS-C items aloud to the children during completion of the questionnaire and told them to ask for clarification of items, if necessary. Children completed the TAS-C in a private room separated from the parent and therapist. Children were told that their answers would remain confidential and were encouraged to answer honestly.
Results
Descriptive statistics and convergent validity
Mean Pearson correlations among child TAS-C, therapist TAS-C, and parent TAS-P scores averaged across all available time points were examined for the ASD and TD groups. A moderate-to-large significant correlation was found between average child and therapist TAS-C scores for the ASD group (r = 0.47, p < 0.000). Interestingly, although they were rating different relationships (child-therapist and parent-therapist), the average therapist TAS-C and parent TAS-P were also significantly correlated for the ASD group (r = 0.44, p = 0.007). For the TD group, the correlations between child and therapist TAS-C (r = 0.20, p = 0.23) as well as therapist TAS-C and parent TAS-P (r = 0.19, p = 0.28) were not statistically significant. Notably, there was agreement among children and therapists on the child-therapist alliance in the ASD sample.
Paired t-tests were conducted to compare the means of child TAS-C and therapist TAS-C. The ASD group mean for child TAS-C (M = 33.54, SD = 6.39) was not significantly different from that of therapist TAS-C (M = 33.47, SD = 6.50) (t(55) = −0.09, p = 0.93). The TD group mean for child TAS-C (M = 36.91, SD = 6.65) was also not significantly different from the mean of therapist TAS-C (M = 37.60, SD = 7.20) (t(34) = −0.46, p = 0.65). Children with ASD as well as TD youth did not evidence statistically significant differences from their therapists in how they rated the quality of the child-therapist alliance.
Psychometric properties of the TAS-C/P
Cronbach’s alpha coefficients of the TD and ASD groups’ child-report measures of therapeutic alliance were calculated to assess the internal consistency. Prior research has shown that youth with ASD often experience challenges in self-reporting accurately (Barnhill et al., 2000; Nicpon, Doobay, & Assouline, 2010); therefore, we explored whether youth with ASD were able to self-report on the alliance with consistency. The reliability of the TAS-C has been previously established in TD children aged 7–12 years. While three 5-year-olds and two 6-year-olds were included in the analyses, they were present only in the TD group. In order to determine whether or not children below 7 should be excluded from the analyses, an internal consistency analysis of only the 5 and 6-year-olds’ TAS-C responses was conducted. The internal consistency of the TD 5 and 6-year-olds responses (α = 0.85) was highly consistent with that of the TD group as a whole (α = 0.84); therefore, they were included in subsequent internal consistency analyses.
For the ASD group, internal consistency of child-report TAS-C scores (α = 0.89) was higher than the level typically deemed acceptable (α
In order to determine the internal consistency of the TAS-C for children below 10 years old with ASD, we conducted separate internal consistency analyses for children 7–10 years old and 10–14 years old with ASD. Internal consistency of the 7–9-year-old group (α = 0.83) was lower than that of the 10–14-year-old group (α = 0.92), but was still in the acceptable range.
In TD populations, it has been unclear whether or not the Task and Bond elements of the alliance are independent or interdependent (Bordin, 1979; McLeod & Weisz, 2005; Shirk & Saiz, 1992). We examined both the internal consistency of the Bond and Task subscales for ASD child TAS-C as well as the correlation between the two subscales in order to examine their interdependence. The internal consistency of the Task subscale of the child TAS-C in the ASD group (α = 0.73) was somewhat lower than that of the Bond subscale (α = 0.87), but was still acceptable. The Pearson’s correlation between the Bond and Task subscale was high for the ASD group child TAS-C (r = 0.81, p < 0.001).
Hypothesis 1: Group differences in alliance
It was hypothesized that the therapeutic alliance would be weaker for children with ASD and anxiety than for TD children with anxiety. TAS-C/P total scores were averaged across all available time points for each participant to increase the statistical power and achieve efficient data reduction. We used a one-way analysis of variance (ANOVA) to examine the effect of group on the TAS-C/P scores.
Child-therapist alliance
In the ANOVA model including child TAS-C as the dependent variable, group TD versus ASD was statistically significant (see Table 3). In the model including therapist TAS-C/P as the dependent variable, group TD versus ASD was also statistically significant (see Table 3). Therefore, there was a significant difference between the two groups in therapist-rated and child-rated alliance scores. Therapist and child ratings of alliance in the ASD group were significantly lower than those in the TD group.
Differences in alliance scores between typically developing and ASD groups.
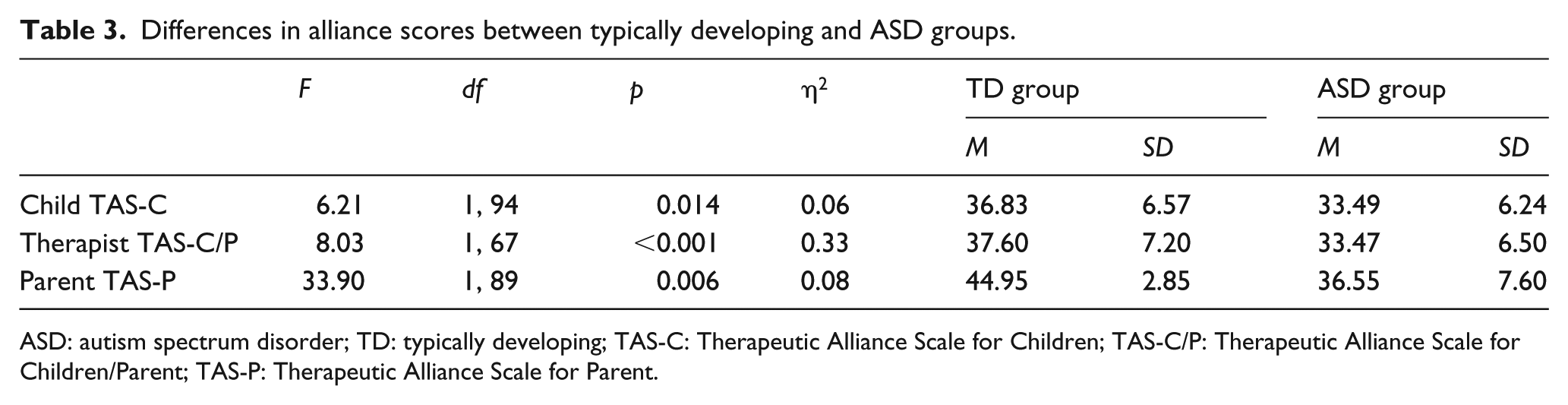
ASD: autism spectrum disorder; TD: typically developing; TAS-C: Therapeutic Alliance Scale for Children; TAS-C/P: Therapeutic Alliance Scale for Children/Parent; TAS-P: Therapeutic Alliance Scale for Parent.
Parent-therapist alliance
In the ANOVA model including parent TAS-P as the dependent variable, group (TD versus ASD) was statistically significant (see Table 3). Therefore, there was a significant difference between the two groups in parent-rated alliance scores. Parent ratings of alliance in the ASD group were significantly lower than those in the TD group.
Hypothesis 2: Alliance-outcome associations
It was hypothesized that a more positive therapeutic alliance would predict greater reductions in anxiety severity for children with ASD and anxiety. Numerous studies have already established the link between alliance and outcome in psychotherapy for TD children; therefore, we focused the alliance-outcome analyses on the ASD group. A set of six regression analyses was conducted for the ASD group to examine whether child-report TAS-C, therapist-report TAS-C, and parent-report TAS-P were significant predictors of anxiety severity (as measured by MASC-P total scores and ADIS-P CSR) at the end of treatment for the ASD group. TAS-C/P total scores were averaged across all available time points for each participant and were included as predictors in these regressions. Post-treatment MASC-P total score or ADIS-C/P highest CSR score was entered as the dependent variable and pretreatment MASC-P total score or ADIS-C/P highest CSR score as well as either average child-report TAS-C total score, therapist-report TAS-C total score, or parent-report TAS-P total score were entered as the predictor variables.
Child-therapist alliance
We found that the average therapist-report TAS-C significantly predicted post-treatment MASC-P scores (β = 0.26, p = 0.03) for the ASD group. In this model, pretreatment MASC-P scores and therapist-report TAS-C explained 37% of the variance in post-treatment MASC-P scores in the ASD group (R2 = 0.37, F(2,43) = 12.93, p < 0.001). Average child-report TAS-C was not a significant predictor of post-treatment MASC-P scores.
Average therapist-report TAS-C was a significant predictor of post-treatment ADIS-C/P highest CSR scores (β = 0.28, p = 0.04). Pretreatment ADIS-C/P highest CSR scores and therapist-report TAS-C explained 13% of the variance in post-treatment ADIS-C/P highest CSR scores (R2 = 0.13, F(2,45) = 3.35, p = 0.04). Average child-report TAS-C was not a significant predictor of post-treatment ADIS-C/P highest CSR scores.
Parent-therapist alliance
Parent-report TAS-P was a significant predictor of post-treatment ADIS-C/P highest CSR scores (β = 0.33, p = 0.05). Pretreatment ADIS-C/P highest CSR scores and parent-report TAS-P explained 19% of the variance in post-treatment ADIS-C/P highest CSR scores (R2 = 0.19, F(2,30) = 3.52, p = 0.04). Higher ratings of both parent-therapist alliance predicted decreased anxiety scores on the ADIS-C/P at post-treatment
Exploratory bond and task analyses
We conducted an exploratory series of follow-up regression analyses using the TAS-C/P Bond and Task subscale averages as predictors of post-treatment MASC-P and ADIS-C/P highest CSR scores. The therapist TAS-C Bond scale was the only significant predictor of post-treatment MASC-P scores (β = 0.27, p = 0.03). Similarly, the therapist TAS-C Bond subscale was a significant predictor of post-treatment ADIS-C/P highest CSR scores (β = 0.31, p = 0.03). Higher scores on the therapist-reported Bond scale of the TAS-C predicted decreased anxiety scores on both the MASC-P and ADIS-C/P, while the Task subscale did not.
Age and alliance outcome associations
Child-therapist alliance
Exploratory multiple regression analyses were conducted in order to examine the potential moderating effects of age on the association between TAS-C/P and post-treatment MASC-P and ADIS-C/P scores. The post-treatment MASC-P total score or ADIS-C/P highest CSR score was entered as the dependent variable and baseline MASC-P total score or ADIS-C/P highest CSR score, average TAS-C/P total score, age, and the interaction between age and average TAS-C/P total were entered as the independent variables. Age and the interactions between age and average child and therapist TAS-C were not significant predictors of MASC-P or ADIS-C/P highest CSR scores.
Parent-therapist alliance
In the model including pre- and post-ADIS-C/P CSR, age, parent TAS-P, and parent TAS-P × age interaction, the parent TAS-P × age interaction was significant (β = −5.41, p = 0.04). When disaggregating the simple slopes of this analysis, parent TAS-P had a stronger effect on post-treatment ADIS-C/P highest CSR scores for children aged 10 years and older (β = 0.60, p = 0.01) than for younger children (β = 0.02, p = 0.93). This suggests that a positive parent-therapist alliance had a stronger relationship with post-treatment reductions in anxiety on the ADIS-C/P for older children with ASD than for younger children with ASD.
Discussion
The therapeutic alliance can be measured with consistency in children with ASD and it appears to be associated with anxiety treatment outcomes in this population, although this effect appears to be limited to therapist and parent report of the alliance. Internal consistency and child-therapist agreement on ratings of the alliance were adequate in our sample of children with ASD. Of note, children with ASD had lower ratings of child-therapist alliance than TD youth according to both children and their therapists. A similar finding emerged for the parent-therapist alliance (lower for the ASD group than the TD group). Our findings linking therapeutic alliance with post-treatment anxiety reduction converge with studies of alliance in TD populations, demonstrating a consistent link between the alliance and treatment outcome (McLeod, 2011; Shirk & Karver, 2003). As the first empirical study of child-therapist alliance in psychotherapy for youth with ASD, the results of this study provide an initial indication that alliance may be an important component of EBIs for ASD and an area warranting further inquiry.
Notably, youth with ASD were able to reliably report on the alliance with their therapists. Internal consistency of the child-report TAS-C exceeded the acceptable level for both younger (aged 7–9) and older (aged 10–14) children with ASD. Although previous studies have found that children with ASD can be unreliable reporters in psychosocial domains (Nicpon et al., 2010), this study suggests that youth with ASD may be capable reporters of the therapeutic alliance and provides support for the use of the TAS-C with this population. The possible utility of the TAS-C for youth with ASD paves the way for further research on the therapeutic process for youth with ASD, given that the TAS-C is a widely used and well-established measure in child psychotherapy research.
Group differences
Our hypothesis that the average strength of the child-therapist and parent-therapist alliance would be significantly higher for the TD group than the ASD group was supported. One of the defining features of ASD is difficulty in forming social relationships. The child-therapist alliance is a social relationship and youth with ASD may have greater difficulty than TD children in forming such a relationship. By the same token, perhaps the relative difficulties therapists experienced in forming bonds with children with ASD spilled over to the parent-therapist alliance in some ways (i.e. through parental identification with their child or frustration with the tensions exhibited between the child and therapist). Importantly, however, the alliance with a therapist is a bidirectional relationship over which a professional and dedicated therapist has considerable influence. Finding ways to foster a positive alliance in psychotherapy with children with ASD should be viewed as a goal of future clinical research and practice. A mediocre or adverse alliance is not inevitable in psychotherapy with children with ASD, and, as analyses related to our second main hypothesis demonstrate (discussed immediately below), the effort needed to positively engage children in ASD in therapy likely has important therapeutic benefits.
Child-therapist alliance
In our primary analyses of our second hypothesis, therapist reports of the child-therapist alliance were a significant predictor of both post-treatment MASC-P and ADIS-C/P scores. This finding underscores the importance of positively engaging youth with ASD in therapy. Because some youth with ASD may at times appear less intrinsically motivated for behavioral/emotional changes, a strong child-therapist alliance could be key to facilitating treatment engagement. It is possible that while some youth with ASD may not be engaged around the concept of symptom amelioration, they may be either motivated by a desire to work with a therapist they like or by building up trust in the viewpoint and concerns of a therapist with whom they have developed a warm relationship. Our finding that the therapist-report Bond subscale of the TAS-C was more predictive of treatment outcome than the Task subscale may support this notion. It also suggests that although technique is often emphasized over alliance in CBT (e.g. Castonguay, Constantino, McAleavey, & Goldfried, 2010) and in other prominent EBIs for ASD, such as applications of applied behavior analysis (Reichow, 2012), the affective bond may be an important component in CBT for youth with ASD. Further research is needed in order to understand the potentially unique mechanisms underlying the alliance-outcome association in therapy for youth with ASD.
Our findings also demonstrated that ratings of alliance from youth with ASD converge significantly with those of their therapists. This finding is consistent with other studies demonstrating moderate correlations between child and therapist ratings of alliance in therapy for similar populations, for example, children with internalizing and externalizing disorders (e.g. Kazdin, Whitley, & Marciano, 2006; Kendall et al., 2009). Although children’s ratings of the alliance did not significantly predict the treatment outcome in this study, their ratings should not be summarily discounted in future studies, given the apparent reliability and validity of their TAS-C scores in our psychometric analyses.
Parent-therapist alliance
Parent-therapist alliance, as rated by parents, had a comparable linkage with post-treatment ADIS-C/P CSR scores in comparison with the therapist-reported child-therapist alliance. These findings suggest that while parent-therapist alliance may play an important role in therapy for youth with ASD, the child-therapist alliance may have an equivalent, if somewhat independent, impact (i.e. it may be possible for a therapist to develop a positive alliance with one family member, such as a parent, but not another, such as a child). Previous studies have found that parent and child alliance are similarly related to treatment outcome (McLeod, 2011).
Interestingly, we found some indication that parent-therapist alliance had a stronger relationship with treatment outcome for older than younger children with ASD. It is possible that given the challenges faced by parents of pre-adolescents and early adolescents (e.g. with effective discipline, a child’s larger physical stature, and desire for autonomy) the relationship between parent and therapist takes on a heightened level of importance. Further study of the nature of alliance formation for youth with ASD of various ages could aid in adapting interventions for differing developmental levels.
Limitations
The generalizability of this study is limited by its highly educated sample of families from a major metropolitan area. Future research in more diverse communities would be desirable. Previous studies have found that ethnic matching between client and therapist may have an impact on alliance formation (e.g. Cabral & Smith, 2011), but this has yet to be studied in psychotherapy for youth with ASD. Given that the TAS-C/P was administered at several time points for each participant, a multilevel analysis would have been an alternative tool for the treatment of the repeated measures data in this study. However, power concerns precluded a multilevel analysis given our sample size. In addition, the ASD sample in this study consists of youth with high-functioning autism. Studies of alliance in samples of minimally verbal youth or youth with different cognitive abilities will be needed to determine if alliance functions similarly in various subpopulations of youth with ASD.
An aspect of this study that provides an important context for the findings is that most of the therapists were graduate students in clinical or educational psychology. Although all therapists were given clinical supervision per study protocol, it is possible that relative inexperience in clinical work may have led to somewhat different results in comparison with the alliance that might have been formed with licensed and more experienced therapists. For example, perhaps some graduate student therapists lacked the flexibility to form a positive alliance with some of the children with developmental challenges. On the other hand, it is equally possible that relative youth and inexperience may have been an asset in forming an alliance through factors such as therapist motivation; the child therapy literature has yielded inconsistent and often nonsignificant findings on whether therapist experience impacts the alliance (Accurso & Garland, 2015).
Conclusion and future directions
This study serves as a first step in understanding the therapeutic process for youth with ASD. Future studies utilizing larger sample sizes and various measures of outcome and alliance should be conducted to further explore the predictive power of the therapeutic alliance in psychotherapy for youth with ASD. Given that different measurement sources of alliance have been found to have differing relationships with outcomes in therapy for TD children (McLeod, 2011), utilizing observational measures of alliance may be warranted (e.g. McLeod, 2005).
In addition to further exploring the role of alliance in P-CBT for youth with ASD, it will be important to examine the role of alliance in other commonly used EBIs for youth with ASD, such as discrete trial training and pivotal response treatment. It may be that the formation of a strong alliance is critical in some forms of therapy for youth with ASD and less important in others. Studying the relative importance of the alliance in various EBIs for ASD may provide information that can help improve training for clinicians and deepen understanding of the underlying mechanisms of EBIs. In order to maximize the effectiveness and efficiency of EBIs for ASD, it may be helpful to determine whether or not devoting substantial intervention time to alliance formation is a worthwhile investment. Examining therapist characteristics and alliance-building behaviors that impact alliance formation is also warranted. This research could ultimately assist in the formation of training materials for therapists working with youth with ASD.
The results of this study suggest that the therapeutic alliance may play an important role in psychotherapy for school-aged youth with ASD. A more thorough understanding of the therapeutic relationship in interventions for youth with ASD may be helpful in therapist training as well as in future intervention development. Considering the therapeutic alliance as a possible core component of EBIs for ASD could support much needed efforts to bring high-quality ASD interventions to the community.
Supplemental Material
AUT841197_Lay_Abstract – Supplemental material for The therapeutic alliance in cognitive-behavioral therapy for school-aged children with autism and clinical anxiety
Supplemental material, AUT841197_Lay_Abstract for The therapeutic alliance in cognitive-behavioral therapy for school-aged children with autism and clinical anxiety by Sami M Klebanoff, Kashia A Rosenau and Jeffrey J Wood in Autism
Footnotes
Declaration of conflicting interests
S.M.K., K.A.R., and J.J.W. declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the University of California Los Angeles Institutional Review Board and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
Funding for this study was provided by the National Institute of Child Health and Human Development (Grant No. HD65270-01), the National Institute of Mental Health (Grant No. MH075806), a UCLA Faculty Grant, and a grant from Autism Speaks.
Informed consent
Informed consent was obtained from all the individual participants included in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.