
Abstract
This study examined rates of and contributing factors to self-determination among young adults with autism spectrum disorder. Caregivers of young adults with autism spectrum disorder, 16–25 years, from five Autism Treatment Network sites completed surveys about their young adults’ transition experiences including the American Institutes for Research Self-Determination measure. Data were analyzed using univariate and multivariate analysis. Caregivers (n = 479) reported their young adults with autism spectrum disorder as having moderate overall self-determination (x = 38; standard deviation = 9.04) with low capacity (x = 15.3; standard deviation = 5.67) and high opportunities at home (x = 23.1; standard deviation = 4.59). Young adults with autism spectrum disorder with intellectual disability or severe autism spectrum disorder symptomology experience significant disparities in overall self-determination compared to those without intellectual disability and less frequent symptom expression and severity. Barring severity indicators, there were few significant predictors of self-determination. Findings show a breakdown in self-determination skill-building. Young adults with autism spectrum disorder with intellectual disability or severe symptomology experienced significant disparities in self-determination. These findings show that current promotion of self-determination is not meeting the needs of young adults with autism spectrum disorder. Future interventions must identify what supports young adults with autism spectrum disorder need to capitalize on these opportunities to be independent and exert autonomy in their daily lives.
Adolescence and young adulthood are times for exploration and discovery (LeCroy & Ashford, 2013). The transition into adulthood is a pivotal phase during which individuals establish their own knowledge base, behaviors, experiences, and attitudes (Carter, Owens, Trainor, Sun, & Swedeen, 2009). During this time, caregivers often encourage autonomous behavior allowing adolescents and young adults to experiment with various activities in order to find their place in the world.
Through this experimentation, adolescents and young adults with varying disabilities develop the self-determination skills such as choice and decision-making, goal setting, problem-solving, self-monitoring, self-regulation, self-advocacy, and self-awareness (Carter et al., 2009; Shogren et al., 2008). Self-determination theory emphasizes the importance of providing individuals with opportunities to be in control of their own fate, enabling the person to fully participate in their own lives and community, and providing supports when needed. A large body of research has been conducted around the examination and promotion of self-determination skills in people with significant disabilities (Wehmeyer, 1998). Self-determination learning theory is a foundational theory in the field and the framework that guided the development of the American Institutes for Research (AIR) Self-Determination measure (Shogren et al., 2008; Wolman, Campeau, Dubois, Mithaug, & Stolarski, 1994). Within this theory, self-determination depends on a person’s capacity to be self-determined and the opportunities the person is given to exert control over their environment (Wolman et al., 1994). Similar to the social-ecological model, the development of self-determination requires a nexus of individual-level characteristics and interpersonal/social and environmental supports (Shogren, Villarreal, Dowsett, & Little, 2016; Walker et al., 2011; Wehmeyer, Abery, Mithaug, & Stancliffe, 2003). Providing education and supports for the development of a young adult’s capacity and age-appropriate challenge and opportunities is essential for the development of self-determination in all young adults.
Supporting the development of self-determination skills in young adults with special health care needs is of great importance. Structured school and community-related interventions have been shown to be successful in increasing self-determination and improving long-term outcomes for young adults with a variety of disabilities (Carter et al., 2009; Paradiz, Kelso, Nelson, & Earl, 2018). In particular, for young adults with disabilities, including physical, developmental, and intellectual, higher rates of self-determination are associated with better employment, independent living, and financial outcomes (Paradiz et al., 2018; Shogren, Wehmeyer, Palmer, Rifenbark, & Little, 2015; Wehmeyer & Palmer, 2003). The association between self-determination and important academic achievement and positive social and behavioral outcomes remains constant, regardless of the severity level or intellectual disability (Carter et al., 2009).
However, the process of developing self-determination is often hindered when an individual has a diagnosis of autism spectrum disorder (ASD) as the key characteristics of this disorder may fundamentally undermine self-determination efforts (Chou, Wehmeyer, Palmer, & Lee, 2017a). Difficulties with executive function and adaptive behavior are very common in ASD. Many young adults with autism spectrum disorder (YA-ASD) struggle with key components of self-determination, like self-monitoring, self-regulating, goal setting, and planning due to these deficits in executive dysfunction and adaptive abilities (Meltzer, 2018). Similarly, many YA-ASD prefer strict routines and feel discomfort in unfamiliar situations. These preferences often result in significant reliance on caregivers to plan activities, and set and maintain schedules. This reliance on caregivers limits YA-ASD’s choice-making behaviors and opportunities to control their own environment, thus limiting the development of self-determination skills within these individuals. As a result, YA-ASD have the lowest rates of self-determination and independence of all young adults, including those with learning and/or intellectual disabilities (Chou et al., 2017a). This continued dependence on caregivers and often governmental aid, which is estimated to cost US$196 billion annually in the US, results in lower quality of life across the lifespan (Buescher, Cidav, Knapp, & Mandell, 2014; Leigh & Du, 2015).
In order to minimize these burdens on individuals, families, and society, we must understand the factors that predict self-determination and use this information to develop interventions to promote self-determination among YA-ASD. A meta-analysis of people with intellectual disability and/or other conditions identified several predictors of self-determination including disability group and severity, gender, and race/ethnicity (Mumbardó-Adam et al., 2017a). Unfortunately, there is a dearth of literature focused on self-determination in YA-ASD (Carter et al., 2009; Chou et al., 2017a; Chou, Wehmeyer, Shogren, Palmer, & Lee, 2017b; Wehmeyer, Shogren, Zager, Smith, & Simpson, 2010). Several studies examining self-determination in people with ASD and/or intellectual disability found variations in self-determination that were predicted by intellectual disability, educational setting, disability severity, and age (Carter et al., 2013a, 2013b; Mumbardó-Adam, Shogren, Guàrdia-olmos, & Giné, 2017b). The vast majority of these studies include only a subsample of children or adolescents with autism, leaving a large gap in our understanding of how to best assist YA-ASD in building self-determination skills.
Guided by the self-determination learning theory, this study aims to improve this understanding by examining caregiver’s assessment of their YA-ASD’s self-determination utilizing the AIR Self-Determination measure. Specifically, this study examines the association between YA-ASD demographic, disability severity, caregiver- and family-related variables, and caregiver-reported YA-ASD self-determination (Carter, Lane, Pierson, & Glaeser, 2006; Chou et al., 2017b). Based on previous literature on youth with special health care needs and YA-ASD, we hypothesize that caregivers will report that YA-ASD will have relatively low levels of self-determination and that these levels will be associated with age, level of education, intellectual disability, and caregiver factors such as age and education level.
It is important to note that caregiver reports were used within this study—in contrast to both caregiver and YA-ASD reporters. The current study was unable to include YA-ASD self-report due to the limited resources available and as some YA-ASD did not have the intellectual or communication ability to complete the survey. Caregiver’s perceptions of the YA-ASD self-determination are useful in understanding what self-determination skills are being taught and promoted as well as the their perception of the YA-ASD self-determination skills. This study cannot provide information on the young adult’s perspectives of their self-determination skills, experiences, and expectations.
Methods
Participants
Eligible participants were restricted to the primary caregiver of a YA-ASD between the ages of 16 and 25 years. Diagnosis of ASD and age were verified through clinical records. Data collection sites were located across the country. Specifically, five Autism Treatment Network (ATN) sites, located in Ohio, Tennessee, Texas, Pennsylvania, and Missouri, were utilized to recruit eligible participants, distribute survey instruments and reminders, and provide compensation for participation. Specific ATN sites were included to ensure representation of minority populations, rural and urban communities, and communities with varying health care access issues. ATN sites utilized their network and clinic databases to identify eligible participants. ATN sites follow protocols, including conducting an Autism Diagnostic Observation Schedule (ADOS) on participants in the registry, for the diagnosis of ASD. Caregivers of all patients who meet the eligibility criteria (age and ASD diagnosis) were invited to participate in the study. Eligible participants were contacted by email and/or mail and during their young adult’s clinical appointments depending on site logistics. Postings about the study were also placed on the sites’ websites and Facebook/Twitter pages. Participants were given time to ask questions and provided a waiver of consent that further detailed the study prior to completing the survey.
Participant demographics
Demographic and condition-specific characteristics for YA-ASD and their caregivers (n = 479) are presented in Table 1. In additional, 30 caregivers started the survey but did not complete the self-determination measure and thus were excluded from the analysis. No significant differences were observed between those included and excluded due to survey completeness.
Demographic characteristics for adolescents and caregivers (N = 479).
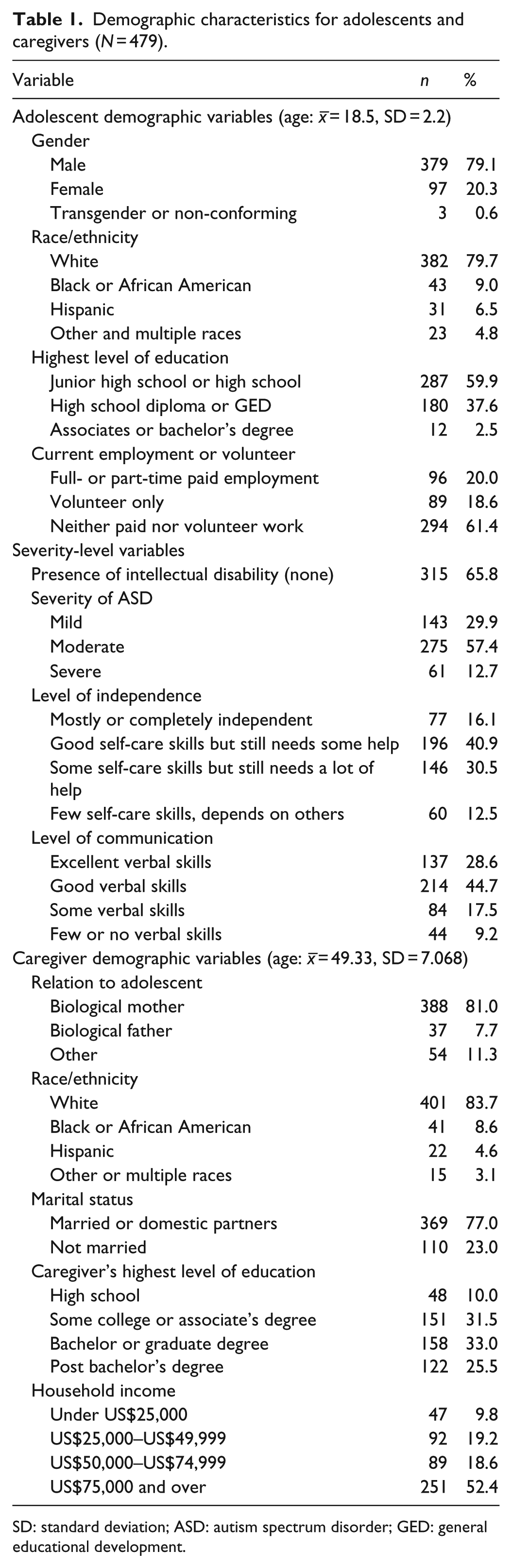
SD: standard deviation; ASD: autism spectrum disorder; GED: general educational development.
YA-ASD ranged in age from 16 to 25 years (M = 18.5; standard deviation (SD) = 2.2), while caregivers had a mean age of 49.33 years (SD = 7.068). The majority of YA-ASD were reported to have moderate ASD symptoms (57.4%). A total of 34% of YA-ASD also had an intellectual disability. Approximately 20% of YA-ASD had paid employment and 18.6% volunteered. The vast majority of caregivers were the young adult’s mother (81%). Caregivers were more likely to be married (77%) and had a household income of US$75,000 or more (52.4%).
Materials
Self-determination survey
Caregivers evaluated their young adult’s self-determination capacity and opportunity using two components of the AIR Self-Determination measure: “Things My Child Does” and “What Happens at Home,” respectively (Wolman et al., 1994). Each young adult’s capacity for self-determination was examined through six questions related to the caregiver’s perception of his or her ability, knowledge, and perception (Wolman et al., 1994). The opportunity component includes six questions related to the young adult’s opportunity/encouragement to demonstrate self-determination skills at home. The third component of the AIR Self-Determination measure, opportunity at school, was not included in this study as many of the young adults eligible for this study were no longer attending school. A Likert-type scale, ranging from never (one) to always (five), was used for each question. Previous studies have demonstrated adequate reliability and validity for the parent version of the AIR Self-Determination measure (Biggs & Carter, 2016; Carter et al., 2013b; Carter et al., 2009; Chou et al., 2017b).
Demographic survey
Variables previously associated with self-determination in young adults with autism and/or intellectual disabilities were included in the analysis (Carter et al., 2013a, 2013b). Individual young adult demographic explanatory variables included age, gender, race/ethnicity, level of education, and employment/volunteer status (Table 1). Caregiver and family factors included caregivers’ educational level, marital status, and household income (Table 1).
Severity-level variables
Severity measures used in this study were adapted from the National Survey of Children with Special Health Care Needs and the National Survey of Children’s Health. These severity measures included current ASD diagnosis, severity of ASD symptoms, presence of an intellectual disability, child’s limited ability to do things other children do, amount of time child was affected by condition in the past 12 months, communication limitation, and presence of intellectual disability (Table 1). All severity indicators were reported by the caregiver.
Procedures
The focus of the full survey was to validate a new health care transition measure, Health-Related Independence. The AIR Self-Determination measure and additional measures related to health, health care access, and transition support and individual caregiver-, and family-level variables were included in the study to assist in the validation of the Health-Related Independence measure. Participants completed the survey in 20–40 min, with most participants using REDCap to complete the survey online (Harris et al., 2009). A small number of caregivers completed the survey in paper format. Participants received a US$20 gift card for completing the survey.
Data analysis
Descriptive statistics were calculated to identify the characteristics of the sample and summarize the caregivers’ rating of the young adults’ self-determination scores (Table 2). Univariate statistics were then used to examine rates of self-determination and individual associations between self-determination and YA-ASDs’ demographics, ASD severity level, individual caregiver-, and family-level variables. Variables were entered into the hierarchical regression model in three blocks: (a) YA-ASD demographics, (b) young adult’s disability severity, and (c) caregiver and family characteristics. In the analysis, crude odds ratios (ORs) and 95% confidence intervals (CIs) were estimated to examine associations between explanatory variables and self-determination. SPSS 23 Complex Samples (SPSS Inc, 2013) were used for all analysis and weight estimates.
Caregiver’s report of YA-ASD self-determination scale questions.
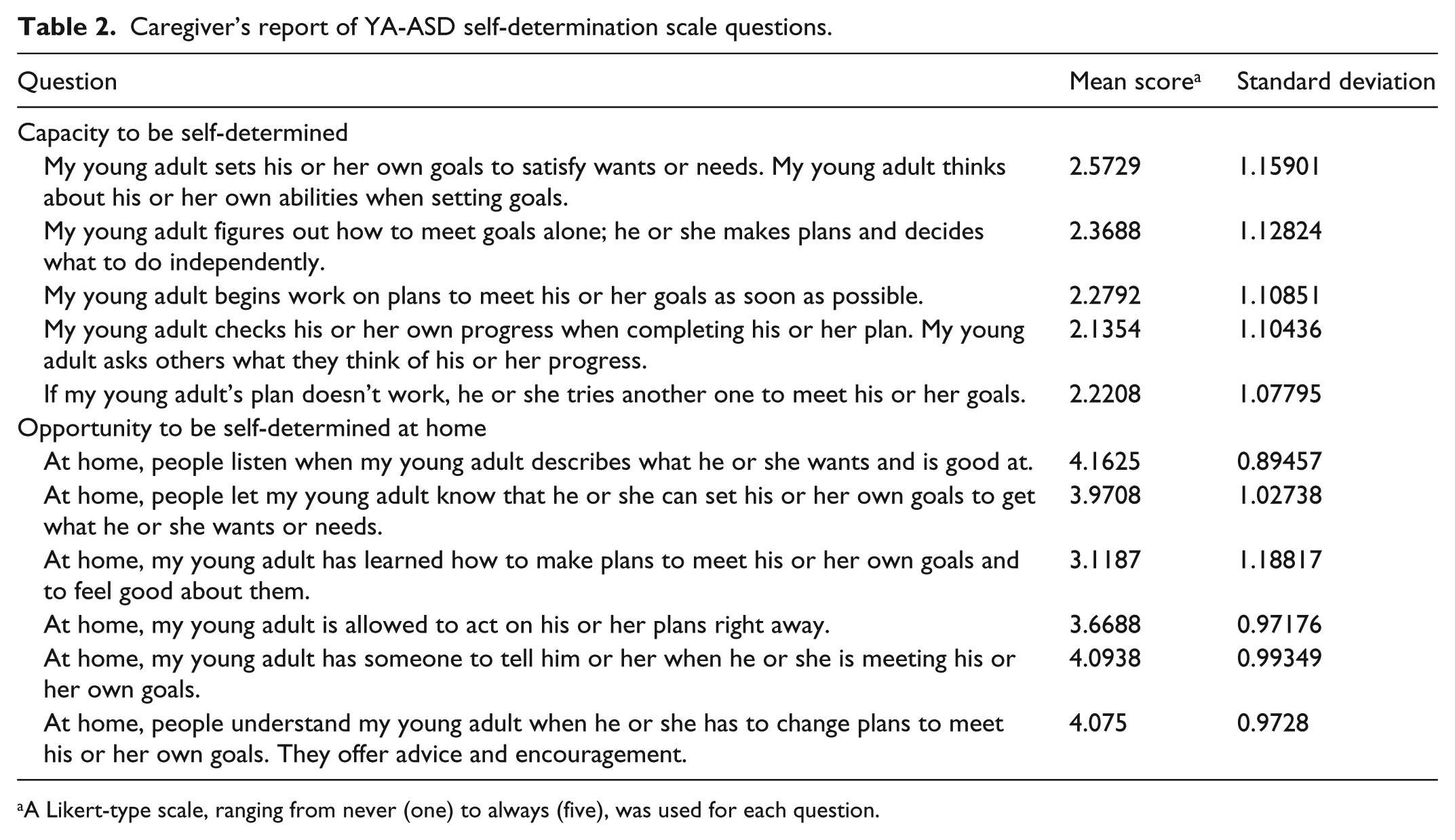
A Likert-type scale, ranging from never (one) to always (five), was used for each question.
Results
Level of self-determination
Caregiver reports of the YA-ASD’s AIR Self-Determination component scores, capacity and opportunity, ranged from 6–30 (the scale minimum and maximum). While their range was similar, the means within the two scales were diverse, as young adults’ capacity had a much lower mean (x = 15.3; SD = 5.67) than young adults’ opportunities at home (x = 23.1; SD = 4.59). Transforming the scores in percentiles of Level of Self-Determination, as outlined in the AIR Self-Determination Scale User Guide (Wolman et al., 1994), caregivers reported that 80% of young adults received opportunities at home, while only 51% of young adults had the capacity to be self-determined. The individual questions on the capacity and opportunity subscales build in complexity from “knowing what one needs/likes/is good at” to “the child’s ability to adjust their plan to meet their goal” for capacity and “listen when child talks about what (s)he wants/is good at” to “the families’ ability to offer advice and encouragements for these adjustments” for opportunity. Within the capacity subscale, all items, regardless of complexity, were rated at or below the predictive average of 2.5 on a 5-point scale. Adversely, four of the six opportunity items are rated 4 or higher on the 5-point scale with little change, regardless of the complexity of the questions (Table 2).
Caregivers reported a wide range of overall self-determination scores for their YA-ASD. The reported range in self-determination mirrored the lowest and highest score ranges within the scale with four YA-ASD with low scores of 12–13 points and five YA-ASD with high scores of 59–60 points. The average level of overall self-determination for the sample was 38 (SD = 9.04) points indicating moderate self-determination or 68% of the possible points within the scale.
Univariate analysis of self-determination
Correlation matrices of overall self-determination, capacity, and opportunity were examined for all YA-ASD demographics, disability severity, and caregiver and family demographic variables. The overall self-determination score was significantly correlated with several YA-ASD demographic variables, including gender, education level, and paid or volunteer work. Overall self-determination was significantly correlated with diagnosis and each of the YA-ASD severity measures. None of the caregiver demographic variables were significantly correlated. Similarly, capacity was significantly correlated with YA-ASD gender, education level, paid or volunteer work, all severity measures, and no caregiver and family variables. Opportunity was significantly correlated with one YA-ASD demographic variable (paid or volunteer work), all severity measures, and no caregiver and family variables.
Regression
The step-wise regression analysis showed similar patterns of significance between disability severity indicators and all caregiver-reported self-determination components (Table 3). When examining overall self-determination, both YA-ASD demographic and ASD severity blocks were significant and accounted for 41.6% of the variance in overall self-determination. Block 2 accounted for the majority of this with an F-change of 41.3. YA-ASD demographic and severity blocks added a significant amount of variance, while caregiver demographics, added in the third block, did not add a significant amount of variance. Specifically, YA-ASD’s age, gender, highest level of education, and paid or volunteer work were significantly associated with overall self-determination within the first block, while all variables examining level of severity, except diagnosis, contributed significantly within the second block. When severity measures were entered in the second block, all demographic variables became non-significant. We included caregiver and family variables within the analysis based on its theoretical and historical contributions, but similar to the bivariate analysis, none of the variables significantly contributed to the model.
Regression results for each component of caregiver-reported self-determination.
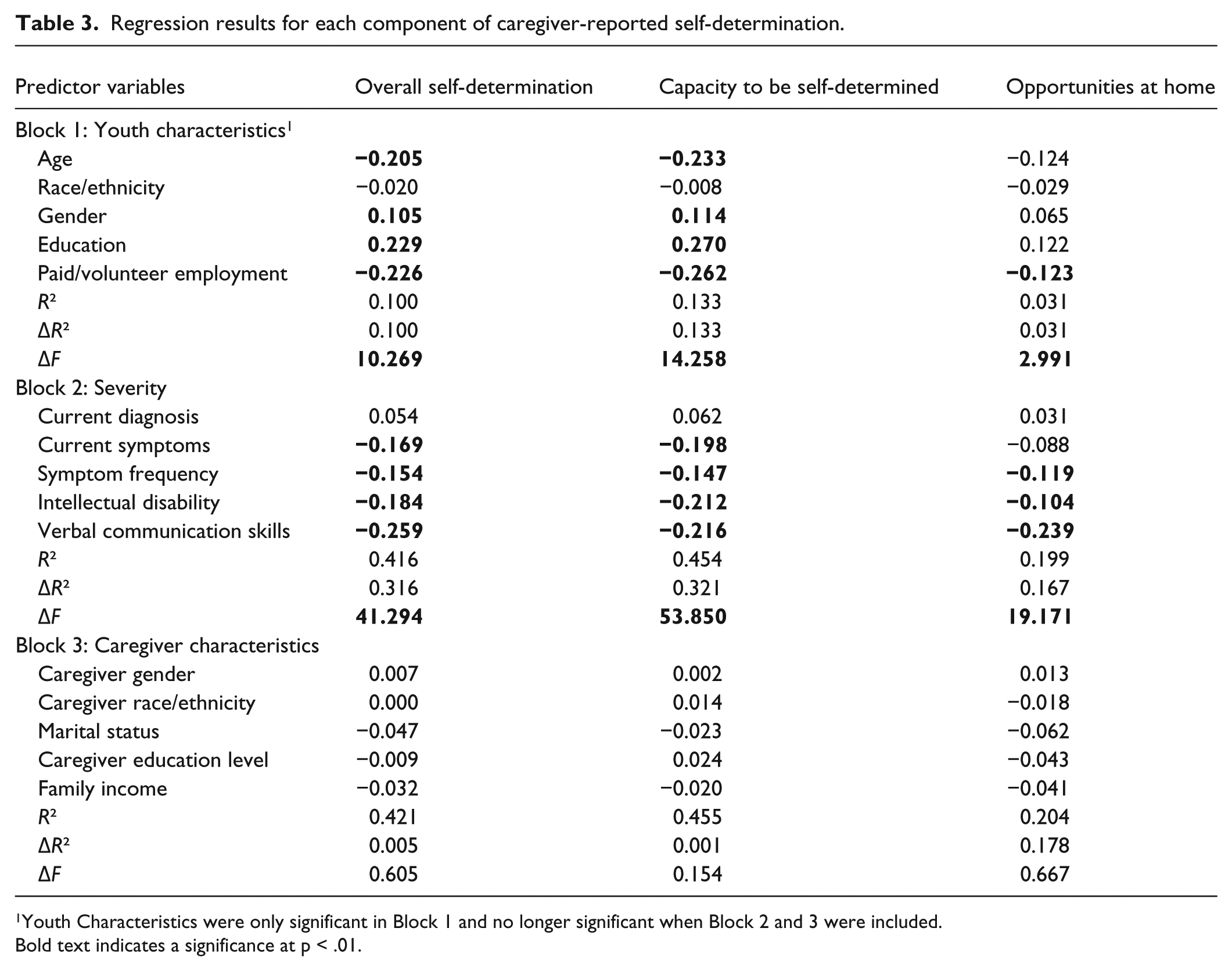
Youth Characteristics were only significant in Block 1 and no longer significant when Block 2 and 3 were included.
Bold text indicates a significance at p < .01.
Within our second analysis, block 1 (YA-ASD demographics) and block 2 (YA-ASD symptom severity) were significantly associated with young adults’ capacity to be self-determined. Conversely, block 3 made an insignificant contribution to the model. The full model accounted for 45.6% of the variance in capacity, with block 2 contributing 32% of total variance. YA-ASD’s demographic variables (i.e., age, gender, level of education, and paid or volunteer work) were significantly associated with self-determination capacity within the first block. Once again, multiple severity measures including intellectual disability, severity of symptoms, frequency of symptoms, and level of communication were significantly associated with capacity. When block 2 (severity measures) was entered, all block 1 (YA-ASD demographics) variables were non-significant, except YA-ASD education.
The last analysis examined the young adult’s opportunity to be self-determined. The full model accounted for 20.8% of the variance. Block 1 was significant accounting for 3% of the variance in opportunity as well as block 2, which accounted for 16.8% of the variance. Within block 1, YA-ASD’s age, education, and paid or volunteer work were significant predictors of opportunity, but each became non-significant when block 2 was entered. Intellectual disability, frequency of symptoms, and communication level were the only significant variables in block 2. Block 3 contributed little to the model, with no variables showing significant contribution. When block 3 was entered, intellectual disability became non-significant. Taken together, these findings underscore the importance perceived severity has on all aspects of self-determination.
Discussion
This is the first known study to examine multiple components of self-determination in an older adolescent and YA-ASD population. The findings of this study show that caregivers report that young adults have high levels of opportunity to practice self-determination skills at home but low levels of capacity for self-determination resulting in moderate levels of overall self-determination. In other words, caregivers report promoting and creating opportunities for self-determination while also reporting that the young adults have difficulty exercising self-determination skills. Furthermore, while many variables were associated with self-determination scores in bivariate analysis, few were shown to be significant predictors in multivariate regressions. The following sections will further examine the expected and unexpected findings in the context of the literature base where it exists.
Overall self-determination level
Within this study, caregivers rated their young adult’s self-determination as moderate. Unfortunately, few studies have examined self-determination in YA-ASD, and, to our knowledge, no study has included the two AIR Self-Determination components that we included, making study comparisons difficult (Biggs & Carter, 2016; Carter et al., 2013b; Carter et al., 2009; Chou et al., 2017b). This average does seem rather high for this sample, as nearly 70% had moderate to severe ASD symptoms and 34% had an intellectual disability. Previous studies on non-ASD and ASD populations have identified condition severity and opportunity limits to be significant predictors of self-determination (Carter et al., 2009; Nota, Ferrari, Soresi, & Wehmeyer, 2007; Wehmeyer et al., 2003; Wehmeyer & Bolding, 2001). As described below, the moderate self-determination score observed in this study may reflect the caregiver’s strong belief that they are providing opportunities for self-determination rather than the YA-ASD’s self-determination skills or the combination of both opportunity and capacity.
Self-determination opportunity and capacity
Caregivers rated opportunity for self-determination quite high at 80% of the possible points on the scale. As shown in Table 2, individual items scores were high with over half of the items receiving 4-points on a 5-point scale. Carter and colleagues (2009) found both caregiver and teachers reported that youth and young adults with severe intellectual or developmental disability received high levels of opportunities, as defined by the AIR measure, to engage in self-determination behavior at home.
As described previously, capacity to be self-determined was much lower than reports of opportunities to be self-determined with the average capacity of 15 points. These capacity scores are similar to those observed by Carter and colleagues (2013a, 2013b). Previous studies have shown higher scores on the first items within the capacity scale with lower scores on more complex items (Carter et al., 2013a). Conversely, caregivers within this study rated their young adults’ self-determination level low across all individual items, regardless of the difficulty or complexity of the skill examined in the question (Table 2).
High opportunity and low capacity
Within this study, caregiver-reported opportunities for self-determination scores consistently outpace the young adults’ capacity (i.e., the youths’ ability to utilize these opportunities) scores. The large difference between opportunity and capacity scores was surprising as the skills or activities that the caregivers reported fostering and encouraging within the opportunity scale were the same skills the young adults seem to be unable to perform within the capacity scale. This suggests that although many YA-ASD were not able to complete activities such as “offer advice and encouragement (to YA-ASD about) . . . changing plans to meet his or her own goal,” the pattern of rating young adults’ opportunities at home high within each item, regardless of complexity, while also rating the young adults’ capacity as low for each item, is difficult to understand and interpret. It is possible that caregivers are reporting what opportunities they believe should be happening in the home rather than the actual situation. It is also possible that the operationalization of the opportunity questions within the AIR Self-Determination measure does not match the opportunities YA-ASD need to be self-determined. Similarly, the unique symptoms associated with ASD might influence how the person behaves in a self-determined manner. In such cases, the YA-ASD’s self-determined skills would be underreported within the AIR and other self-determination measures. Future work should examine specific ASD support needs and observations and self-reports of self-determination behaviors in YA-ASD.
Two studies to date, utilizing multiple reporter data in measuring self-determination, found that caregiver and teacher reports were relatively consistent with each other—high opportunity with lower capacity, but diverged from young adult reports—low opportunity with relatively high capacity (Carter et al., 2006; Carter et al., 2009). Similarly, a study of young adults with intellectual disability in Spain indicated that the young adults’ rated opportunity at home was low in general and compared to opportunities at school (Mumbardó-Adam et al., 2017b).
Although the AIR Self-Determination measure has been validated in numerous studies, further research is needed to examine the influence that the type of rater has on the subscale and overall self-determination scores. The culmination of research suggests that each rater (i.e., caregivers, teachers, and young adults) comes with their own biases, and rating differs accordingly (Carter et al., 2013b; Carter et al., 2006; Carter et al., 2009). Studies utilizing only one outside rater and no self-report data, as the current study does, should be cognizant that they are likely only presenting one perspective on this complex and multifaceted issue. The use of multi-respondent assessments would assist in better understanding of self-determination and identifying whether reporting differences between caregivers and YA-ASD exist. Furthermore, the use of an outside observer or precise skill-based measure is needed to expand our understanding of self-determination, how it is developed, and how it affects future outcomes.
Regression
Within the regression analysis, no demographic variables were consistent predictors, whereas several severity indicators were shown to be strong predictors across components: symptom severity, frequency of symptoms, communication level, and presences of intellectual disability (Table 3). Previous research on ASD and non-ASD populations has similarly shown the significant impact of severity of condition and intellectual disability on self-determination (Carter et al., 2013a, 2013b; Carter et al., 2009; Chou, Palmer, Wehmeyer, & Skorupski, 2017c; Mumbardó-Adam et al., 2017b). A meta-analysis of this issue identified a consistent association between ASD diagnosis and lower self-determination scores compared to other diagnosis even after controlling for intellectual disability and other individual and environmental factors (Mumbardó-Adam et al., 2017a). Although the current study has no comparison group, we observed similar associations with complexity and severity of ASD symptom indicators and lower levels of overall self-determination and domain scores, after controlling for the presence of an intellectual disability.
The overwhelming significance of severity-level variables in predicting self-determination could be due to young adults’ difficulty learning and executing tasks across multiple domains and/or caregivers’ tendency to conflate the level of disability with the ability to be self-determined (Carter et al., 2013b). In theory, a person’s disability level and cognitive ability should affect the level of support a person needs to be self-determined, but it should not control their ability to be self-determined. The association between YA-ASD condition severity and caregiver’s report of self-determination capacity, shown in this study and other studies, calls into question whether YA-ASD are receiving the support and opportunity from caregivers that is needed to achieve self-determination (Dieleman et al., 2018). Furthermore, our findings underscore the importance of knowing how caregivers, YA-ASD, and others define self-determination, how YA-ASD exhibit self-determination skills, and what opportunities they need to support increased self-determination. Future research must evaluate the level of self-determination, opportunity to be self-determined, and intervening variables through objective qualitative and quantitative lens to shed more light on self-determination capacity and promotion within the ASD community.
While individual and caregiver characteristics are often significant in models examining service delivery, quality of care, and unmet needs, these variables seemed to have little effect on self-determination (Cheak-Zamora & Farmer, 2015 ; Magana, Parish, Rose, Timberlake, & Swaine, 2012; Vohra, Madhavan, Sambamoorthi, & St Peter, 2014). The study findings were counter to our hypothesis that age, level of education, and caregiver education would be associated with the level of self-determination. Previous studies have observed significant effects for gender, race/ethnicity, age, and household’s federal poverty level, but these factors were not consistent predictors across studies (Carter et al., 2013a, 2013b; Mumbardó-Adam et al., 2017a; Mumbardó-Adam et al., 2017b). It is likely that YA-ASD and caregiver demographic characteristics play a role in the support for and development of self-determination, but the influence of condition severity and intellectual disability overpowers this effect. In addition, the lack of variance in opportunity scores may affect our ability to identify differences between groups within the opportunity domain and the cumulative overall self-determination score.
Future research and intervention implications
Self-determination skills improve young adults’ level of autonomy, independence, and quality of life (Biggs & Carter, 2016). In light of our results, it is clear that YA-ASD have limited self-determination capacity; there is a need for tailored interventions that focus on self-determination and independence for YA-ASD. Furthermore, the concepts covered in the AIR Self-Determination measure (i.e., understanding self, ability to set goals and make plans, and ability to evaluate efforts) are essential skills needed for self-determination and should be included in all transition programs.
Future interventions should incorporate the specific factors that have been shown to foster YA-ASD self-determination skills (Carter et al., 2013b; Lee, Simpson, & Shogren, 2007; Wood, Fowler, Uphold, & Test, 2005). Social skills, positive self-talk, community engagement, family cohesion, options/opportunities, and self-advocacy skills have been tied to the development of self-determination (Carter et al., 2013b; Nadig, Flanagan, White, & Bhatnagar, 2018; Oswald et al., 2018). Likewise, interventions should target the factors, such as poor communication skills and disability severity, that seem to deter young adults’ self-determination. Fortunately, unlike demographic characteristics, severity-level factors can be improved with consistent and age-appropriate interventions (Carter et al., 2009; Chou et al., 2017a; Zalewska, Migliore, & Butterworth, 2016).
Successful self-determination models in YA-ASD and youth with other special health care needs have included education and skill-building around goal setting, decision-making, and self-regulation while incorporating real-work application of these skills (e.g., assisting young adults in actively participating in their independent education plan (IEP), engaging in community activities, and/or working with others) (Nadig et al., 2018; Palmer, Wehmeyer, Shogren, Williams-Diehm, & Soukup, 2012). The Acquiring Career, Coping, Executive control, Social Skills (ACCESS) program is one example of a successful program for young adults and adults with ASD which improves self-determination and independent functioning within a group intervention setting (Oswald et al., 2018). Another program, Spectrum Pathways, builds self-determination in YA-ASD through goal setting and coaching (McDonald et al., 2018). The young adults work with program facilitators to set goals in areas ranging from education to employment to social relationships and receive weekly coaching sessions to work on attaining these goals.
The AIR Self-Determination measure has been used in a number of ways in previous studies. In fact, the majority of studies using the AIR Self-Determination measure selected certain portions of the measure that best fit their research need (Carter et al., 2013a, 2013b; Carter et al., 2009). Within this study, we excluded the “what happens at school” portion of the measure as many of the YA-ASD within the study were no longer attending school. This repeated technique of using part of the scale calls into question the validity of the scale, begging the question “Is the scale valid when it is broken down into its subscale components?” In addition, Shogren et al. (2008) found that the AIR Self-Determination measure measures a different aspect of self-determination than the Arc self-determination scale. Future research should examine the validity of the AIR Self-Determination measure and the individual components as well as other measures within the YA-ASD and ASD population.
Limitations
The current study has several limitations. First, the cross-sectional methodology of this survey does not permit examination of a causal relationship between self-determination and demographic, severity, or caregiver- and family-level factors. Second, caregiver reports were used and are subjective in nature. It is possible that caregivers had difficulty recalling or are overreporting specific activities within the self-determination measure or other variables of interest. Furthermore, the young adults’ self-reports were not included in the study; thus, we are unable to provide their perspective. The research team focused on caregivers in an effort to obtain data on YA-ASD within and without significant communication limitations. While this decision added in broadening our sample and increasing the sample size, the lack of YA-ASD perspectives is a significant limitation. Future studies should, at minimum, include a subsample of YA-ASD as self-reporters of self-determination skills and needs.
The current study does not include the opportunities at school component within the AIR measure. Information about opportunities at school may have contributed important information about another component of self-determination for those currently in school. In addition, this information may have improved our understanding of the discrepancy between caregiver’s report of YA-ASD’s capacity and opportunities at home. Finally, we attempted to include a diverse and nationally representative sample but had limitations on the ethnic and racial diversity of caregivers participating in the study. This weakness may limit our ability to find significant differences in these areas. Future research is needed to adequately sample a more racially and ethnically diverse population. Despite these limitations, this study makes a unique contribution by examining multiple components of self-determination in an older adolescent and young adult ASD population with data from a national sample.
Conclusion
This study aimed at increasing our understanding of the level of self-determination and contributing factors within a large sample of older adolescents and young adults with ASD. While advocacy and educational organizations call for increased focus on independence, we have identified important disparities in access to self-determination skill-building for YA-ASD. The findings of this study show that caregivers report high levels of opportunity for young adults to practice self-determination skills at home but low levels of the young adults’ capacity for self-determination. This study also demonstrates that YA-ASD with intellectual disability or severe ASD symptomology experience significant disparities in overall self-determination. In most cases, disability severity indicators decreased the odds of having moderate self-determination by 15%–26%.
These findings indicate a breakdown in self-determination skill-building within the education setting and/or at home which prevents the young adult from utilizing self-determination skills. Self-determination interventions should be initiated when the youth are approximately 12–13 years of age to capitalize on the built-in support system, peer modeling, and provide the youth with opportunities to utilize these skills in safe and achievable ways as they move into adulthood. Such interventions must encourage YA-ASD to capitalize on these opportunities while providing the young adults with the space and time needed to implement this new autonomy in their own way. Educators, caregivers, and advocacy groups should strive to incorporate stronger collaboration and coordination of self-determination and independent skill-building across home, school, and community settings for all youth and young adults, particularly those with increased symptom severity. Furthermore, education policy and funding streams must be established to support teachers and community groups in providing additional support to this growing, vulnerable population.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Due to the electronic nature and absence of identifiable information collected in this survey, all individual participants were provided information about the study and a waiver of consent in the study.
Statement of the welfare of animals
This article does not contain any studies on animals performed by any of the authors.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.C.C.-Z. received the grant from the Department of Defense, Assistant Secretary of Defense for Health Affairs, that allowed this project to be conducted. A.M.-B. and B.A.M. were collaborators on this grant and received partial funding for their time working on the grant. A.C. received pay as part of this project and no additional financial or non-financial gain.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Assistant Secretary of Defense for Health Affairs, through the Autism Research Program, Idea Development Award under Award No. W81XWH-14-1-0604. The US Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick MD 21702-5014 is the awarding and administering acquisition office. Opinions, interpretations, conclusions, and recommendations are those of the author and are not necessarily endorsed by the Department of Defense.