
Abstract
Adolescents with autism spectrum disorder frequently experience social communication difficulties, executive functioning deficits, and anxiety and depressive symptoms, which are similar to the symptoms and correlates of sluggish cognitive tempo. Although sluggish cognitive tempo is related to, but distinct from, the inattentive and hyperactive-impulsive symptoms of attention-deficit/hyperactivity disorder that commonly co-occur with autism spectrum disorder, few studies have examined sluggish cognitive tempo in autism spectrum disorder. We examined whether sluggish cognitive tempo and attention-deficit/hyperactivity disorder were differentially associated with autism symptomatology, daily life executive functioning, and internalizing and externalizing symptoms in 51 adolescents (ages 13–18 years) with autism spectrum disorder without intellectual disability. Regression analyses controlling for age and IQ showed that sluggish cognitive tempo symptoms, but not attention-deficit/hyperactivity disorder symptoms, were associated with increased autism symptomatology and internalizing symptoms. Attention-deficit/hyperactivity disorder symptoms, but not sluggish cognitive tempo symptoms, were associated with increased externalizing behaviors and behavior regulation deficits. Both sluggish cognitive tempo and attention-deficit/hyperactivity disorder were independently associated with increased metacognitive deficits. This study provides preliminary evidence that sluggish cognitive tempo symptoms are elevated in autism spectrum disorder and associated with key clinical correlates, with implications for the assessment and treatment in adolescents with autism spectrum disorder.
Keywords
Introduction
It is well established that children and adolescents with autism spectrum disorder (ASD) have significant social skill deficits including building and maintaining friendships, understanding the perspectives of others, picking up on social cues, and engaging in conversations with others (American Psychiatric Association, 2013; Volkmar et al., 2014). Executive functioning (EF) skills such as initiating tasks, sustaining attention, thinking flexibly, planning and organizing, prioritizing tasks, shifting to different thoughts and actions, and solving problems are also estimated to be impaired in 35%–70% of individuals with ASD (Blijd-Hoogewys et al., 2014; Rosenthal et al., 2013). Furthermore, EF deficits appear to increase from childhood to adolescence and have been linked to poor adult outcomes (Hume et al., 2009; Kenworthy et al., 2009; Pugliese et al., 2016). Anxiety and depression also occur at much higher rates in adolescents with ASD than in the general population, with estimates of 30%–35% having clinically significantly internalizing symptoms based on parent report (Strang et al., 2012). Interestingly, the functional impairments observed in individuals with ASD without intellectual disability (i.e. IQ ⩾ 70) are quite consistent with impairments related to sluggish cognitive tempo (SCT) symptoms (i.e. poor social skills, daily life executive dysfunction, anxiety and depression).
SCT, a commonly co-occurring yet distinct correlate of attention-deficit/hyperactivity disorder (ADHD), is characterized by behaviors such as excessive daydreaming, mental confusion, staring blankly, being lost in thoughts, slow thinking and responding, and losing one’s train of thought (Becker et al., 2016b). Although 27%–39% of children and adolescents with ADHD also demonstrate elevated SCT symptoms (Barkley, 2013; Servera et al., 2018), SCT is distinct from ADHD. In fact, the separability of SCT from ADHD has been documented in 20 studies, and there is clear evidence for the internal validity, and compelling evidence for the external validity, of SCT as a distinct construct (Becker et al., 2016b). Critically, as noted above, SCT symptoms are associated with significant impairments in multiple domains. Specifically, SCT symptoms are associated with impaired social functioning, particularly difficulty detecting social cues, low social engagement, and withdrawal/isolation (Becker et al., 2017; Marshall et al., 2014; Mikami et al., 2007). There is also emerging evidence that SCT symptoms are associated with real-world EF deficits, particularly in metacognitive domains that include self-motivation, time management, organization, and working memory (Araujo Jiménez et al., 2015; Barkley, 2013; Becker and Langberg, 2014). Furthermore, SCT symptoms are more clearly associated with internalizing symptoms (e.g. depression, anxiety) than with externalizing symptoms (e.g. rule breaking behaviors) (Barkley, 2013; Becker et al., 2016b).
Examining SCT in ASD is warranted for a few reasons. First, SCT symptoms are often characteristic of individuals with ASD (e.g. “seems to be in a world of his or her own,” “gets lost in his or her own thoughts”) (Reinvall et al., 2017). In fact, in a sample of children and adolescents with ASD without intellectual disability, SCT symptoms were positively associated with core ASD symptoms (i.e. Reciprocal Social Interaction and Language/Communication domains assessed using the Autism Diagnostic Interview Revised) (Reinvall et al., 2017). Second, Barkley (2013) found that among children with elevated SCT symptoms (with or without ADHD), 28.3% had a parent-reported ASD diagnosis. In contrast, among children with elevated ADHD (with or without SCT), 24.9% had a parent-reported ASD diagnosis. Thus, the rates of ASD were somewhat (though not significantly) higher in children with SCT than in children with ADHD. Third, adolescents with ASD frequently experience co-occurring ADHD symptoms, with approximately 30%–70% of individuals with ASD also meeting criteria for an ADHD diagnosis (Gadow et al., 2006; Goldstein and Schwebach, 2004; Lee and Ousley, 2006). As SCT predicts poorer outcomes in children with ADHD (Becker et al., 2016b), as well as poorer methylphenidate response (Froehlich et al., 2018), it is important to investigate the clinical correlates of SCT in individuals with ASD to determine whether individuals with ASD and high SCT symptomatology show more impairment, which could then lead to more effective, targeted treatment planning efforts.
Only one study to date has investigated SCT in children and adolescents with ASD without intellectual disability. This study investigated SCT in 55 children and adolescents (aged 5–15 years) with ASD without intellectual disability (Reinvall et al., 2017). Two items on the Five to Fifteen Questionnaire (“often in own world or daydreaming” and “seems slow, inert or lacking energy”) were rated by parents on a three-point Likert-type scale (0 = does not apply, 1 = applies sometimes or to some extent, 2 = definitely applies). Scores on these two items were summed and used to define SCT status; the sample was divided into high (score of 3 or 4), medium (score of 2), and low (score of 0 or 1) SCT groups to examine the relationship with parent-reported social skills and internalizing and externalizing diagnoses (Reinvall et al., 2017). Consistent with the literature, higher SCT symptoms were related to increased social difficulties and increased rates of internalizing disorders (e.g. generalized anxiety disorder, obsessive compulsive disorder, and major depression diagnoses) in children with ASD. Importantly, these associations were maintained even when controlling for ADHD symptoms and age. There was no significant relationship between SCT symptoms and externalizing disorders (Reinvall et al., 2017). Given that only one study has investigated the clinical correlates of SCT in ASD, additional research is warranted to increase our understanding of the relationship between both SCT and ADHD symptoms in ASD.
The current study seeks to further examine SCT in individuals with ASD. Specifically, using a sample of well-phenotyped, adolescents with ASD without intellectual disability, we examined whether SCT symptoms and ADHD symptoms were differentially associated with ASD symptom severity, internalizing symptoms, and externalizing symptoms. We build upon extant literature by also examining the association of SCT and real-world ratings of EF. The Behavior Rating Inventory of Executive Function (BRIEF) is thought to provide a picture of an individual’s idiographic cognitive functioning (McCandless and O’Laughlin, 2007) and may be more likely to predict real-life impairments than cognitive tests (Barkley and Fischer, 2011). Daily life EFs include behaviors related to time management, organization and problem solving, self-discipline, motivation, and activation (Barkley and Fischer, 2011). Importantly, individuals with ASD evidence impairments in daily life EFs (Rosenthal et al., 2013), and daily life EF ratings have also been associated with SCT (Barkley, 2013; Becker and Langberg, 2014; Capdevila-Brophy et al., 2014; Jiménez et al., 2015). We hypothesized that (a) both SCT and ADHD symptoms would be associated with increased ASD symptom severity, (b) SCT symptoms would be uniquely associated with internalizing symptoms whereas ADHD symptoms would be uniquely associated with externalizing symptoms, and (c) both SCT and ADHD symptoms would be uniquely associated with poorer metacognitive EF whereas only ADHD symptoms would be uniquely associated with poorer behavior regulation EF.
Methods
Participants
Families with adolescents ages 13–18 years were recruited for an ongoing study through the standard clinical flow at an outpatient clinic specializing in re-evaluation of ASD. Participants who contributed data for the current analyses were 51 adolescents with ASD without intellectual disability (i.e. IQ ⩾ 70). No specific inclusion or exclusion criteria were utilized. The sample was comprised primarily of White (86.2%), male (90.2%) adolescents (16.28 ± 1.32 years) with average IQ (98.41 ± 16.45). Additional sample characteristics are provided in Table 1.
Participant demographics (N = 51).
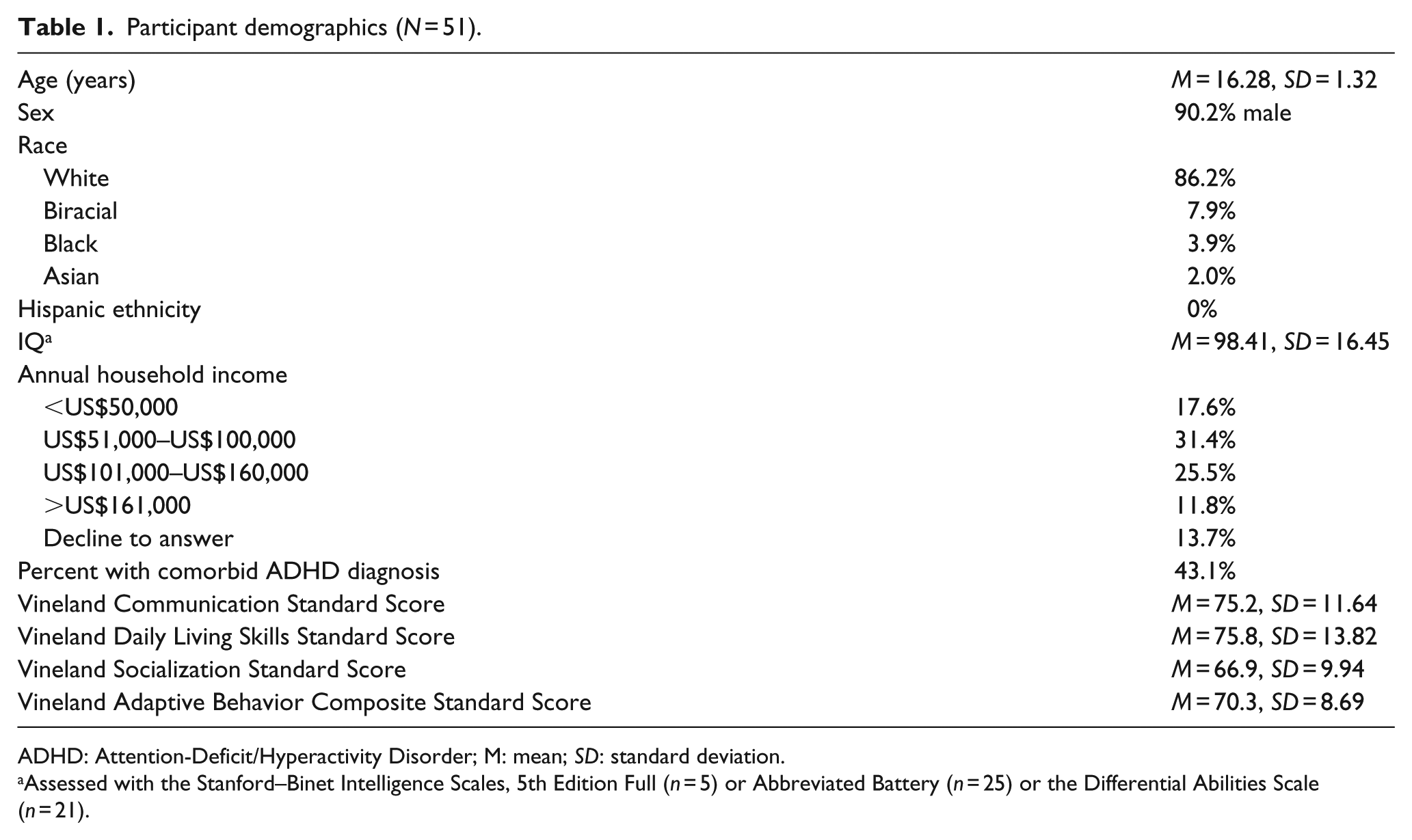
ADHD: Attention-Deficit/Hyperactivity Disorder; M: mean; SD: standard deviation.
Assessed with the Stanford–Binet Intelligence Scales, 5th Edition Full (n = 5) or Abbreviated Battery (n = 25) or the Differential Abilities Scale (n = 21).
Procedures
As part of the standard battery of clinical assessments, adolescents were administered Module 4 of the Autism Diagnostic Observation Schedule, 2nd Edition (ADOS-2) (Lord et al., 2012) by a research reliable assessor (first author) and an IQ assessment (e.g. Stanford–Binet Intelligence Scales, 5th Edition (Roid, 2003)). Concurrently, the parent completed ratings including the Vineland Adaptive Behavior Scales (VABS) (Sparrow et al., 2005, 2016) and the measures described below. All procedures were in accordance with Institutional Review Board standards and informed consent/assent was obtained.
Measures
Child Behavior Checklist
The Child Behavior Checklist (CBCL; Achenbach, 1991) is a widely used reliable and valid measure of child behavior and psychopathology. In the present study, the broadband internalizing and externalizing scales were used in addition to the specific DSM-oriented attention-deficit/hyperactivity problems (i.e. ADHD symptoms) and SCT scales. The SCT scale is composed of four items (“confused or seems to be in a fog,” “daydreams or gets lost in his or her thoughts,” “stares blankly,” “underactive, slow moving, or lacks energy”), has been frequently used in previous studies of SCT (Garner et al., 2017), and demonstrates adequate internal consistency (Becker et al., 2016b). Higher T-scores on the SCT scale reflect more SCT symptomatology.
BRIEF
Parents completed the BRIEF (Gioia et al., 2000), a validated assessment of everyday skills measuring EF, including inhibition, shifting attention, emotional control, initiating tasks, problem solving, working memory, and monitoring activities. For the current study, the Behavior Regulation Index (ability to maintain appropriate regulatory control of one’s own behavior and emotional responses) and Metacognition Index (ability to initiate, plan, organize, self-monitor, and sustain working memory) T-scores were utilized. Higher scores indicate poorer functioning.
Social Communication Questionnaire
The Social Communication Questionnaire (SCQ) Lifetime Form (Rutter et al., 2003) is a parent-report questionnaire tapping historical and current symptoms of ASD. This 40-item, yes/no checklist was empirically derived from the Autism Diagnostic Interview—Revised (Lord et al., 1994) and has been demonstrated to be an effective parent report tool of autism symptoms. We used the SCQ total score as an index of ASD symptomatology. Higher scores indicate more behaviors characteristic of ASD.
Statistical analyses
Missing data varied with 9.8% of the sample missing the SCQ and 15.7% missing the BRIEF Behavior Regulation and Metacognition Index T-scores. Tests of patterns of missingness suggested data were missing completely at random (Little’s MCAR test: χ2 = 26.25, df = 21, p = .197). Comparison of participants with and without complete data indicated that the groups did not significantly differ on age, IQ, sex, race, income, ASD symptomatology, or VABS composite. Analyses were run with all available data; no imputation or substitution methods were implemented for missing data.
For primary analyses, we first examined whether rates of elevated SCT (i.e. T-score ⩾70 on CBCL SCT subscale) were higher than rates of elevated ADHD (i.e. T-score ⩾70 on CBCL ADHD subscale) using a chi-square analysis, and we also used paired samples t-tests to compare continuous SCT and ADHD symptom severity scores. We then examined bivariate correlations (two-tailed) among study variables. A correlation of .10 is considered a small effect, .30 is considered a medium effect, and .50 is considered a large effect (Cohen, 1988). Finally, regression analyses were conducted to examine the independent associations of SCT and ADHD symptoms in relation to autism symptomatology, co-occurring internalizing and externalizing behaviors, and daily life EF, above and beyond IQ and age. Specifically, IQ and age were entered on Step 1, followed by SCT and ADHD symptoms on Step 2.
Results
Prevalence of elevated SCT and ADHD symptoms in adolescents with ASD
37.3% of participants (n = 19) had a T-score ⩾70 on the SCT subscale compared to 15.7% of participants (n = 8) with a T-score ⩾70 on the ADHD subscale (five participants had clinical elevations on both the SCT and ADHD subscales). However, despite twice as many participants being classified as having elevated SCT compared to elevated ADHD, this difference was not statistically significant (χ2(1) = 2.587, p = .108). Paired samples t-tests using continuous SCT and ADHD symptoms scores indicated that participants did have significantly higher SCT T-scores than ADHD T-scores (t = 3.93, p < .001; see Table 2 for means and standard deviations).
Intercorrelations and descriptive statistics of study variables.
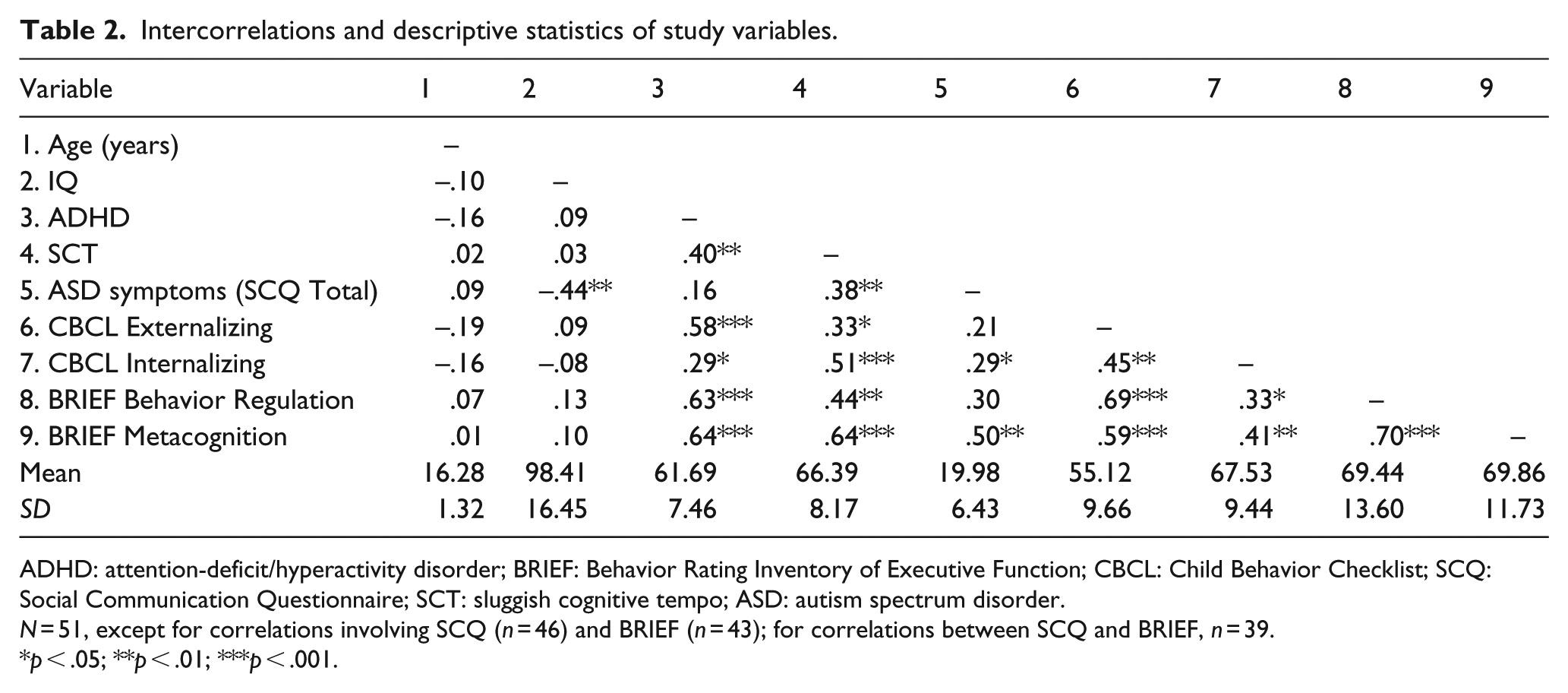
ADHD: attention-deficit/hyperactivity disorder; BRIEF: Behavior Rating Inventory of Executive Function; CBCL: Child Behavior Checklist; SCQ: Social Communication Questionnaire; SCT: sluggish cognitive tempo; ASD: autism spectrum disorder.
N = 51, except for correlations involving SCQ (n = 46) and BRIEF (n = 43); for correlations between SCQ and BRIEF, n = 39.
p < .05; **p < .01; ***p < .001.
Correlation analyses
Intercorrelations and descriptive statistics of study variables are presented in Table 2. SCT symptoms, but not ADHD symptoms, were significantly correlated with autism symptomatology (higher SCQ total score). SCT symptoms were strongly correlated with increased internalizing symptoms and moderately correlated with externalizing behaviors; in contrast, ADHD symptoms were strongly correlated with externalizing behaviors and moderately correlated with internalizing symptoms. Both SCT and ADHD symptoms were strongly correlated with higher BRIEF Metacognition scores; SCT symptoms were moderately correlated and ADHD symptoms were strongly correlated with higher BRIEF Behavior Regulation scores.
Regression analysis examining ASD symptomatology
Above and beyond IQ and age, ADHD symptoms were unassociated with the SCQ total score (β = .07, p = .608) whereas SCT symptoms remained significantly associated with higher SCQ total score (β = .34, p = .018; see Table 3 for full results).
Multiple regression analysis examining SCT and ADHD symptoms in relation to ASD symptom severity.
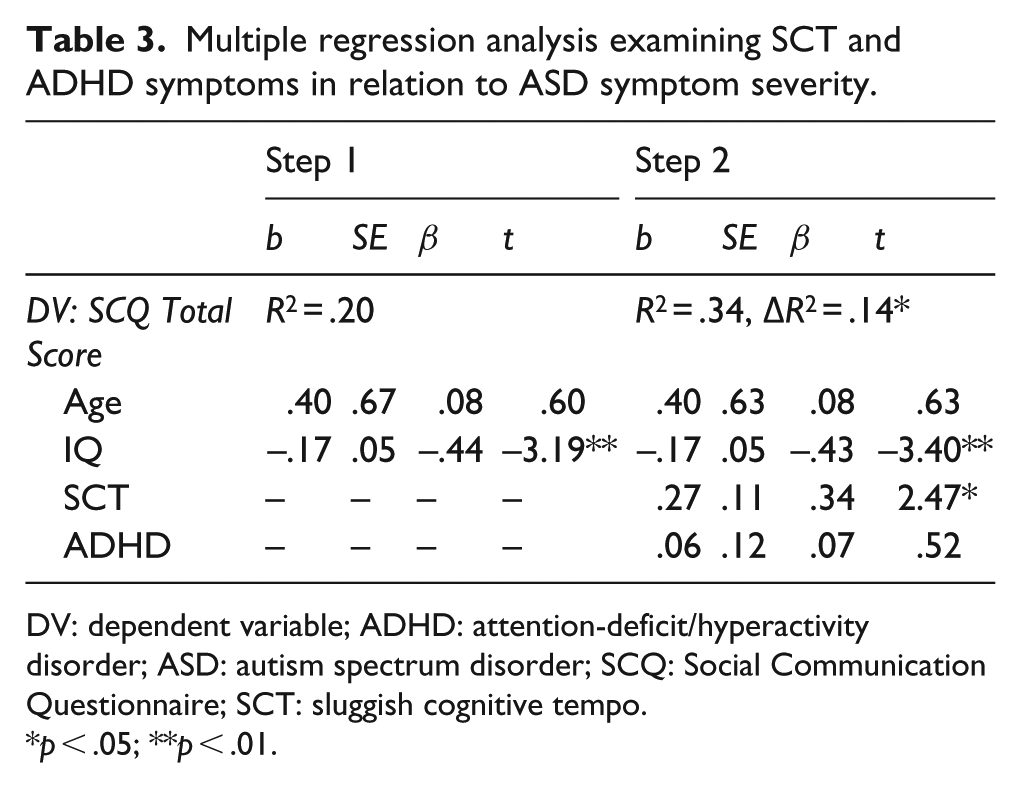
DV: dependent variable; ADHD: attention-deficit/hyperactivity disorder; ASD: autism spectrum disorder; SCQ: Social Communication Questionnaire; SCT: sluggish cognitive tempo.
p < .05; **p < .01.
Regression analyses examining externalizing and internalizing problems
When SCT and ADHD symptoms were entered simultaneously in the model, above and beyond age and IQ, ADHD symptoms remained significantly associated with more externalizing behaviors (β = .51, p < .001) whereas SCT symptoms were no longer associated with externalizing behaviors (β = .13, p = .325). Conversely, ADHD symptoms were no longer associated with internalizing symptoms (β = .08, p = .552) whereas SCT symptoms remained significantly associated with more internalizing symptoms (β = .48, p < .001; see Table 4).
Multiple regression analysis examining SCT and ADHD symptoms in relation to externalizing and internalizing problems.
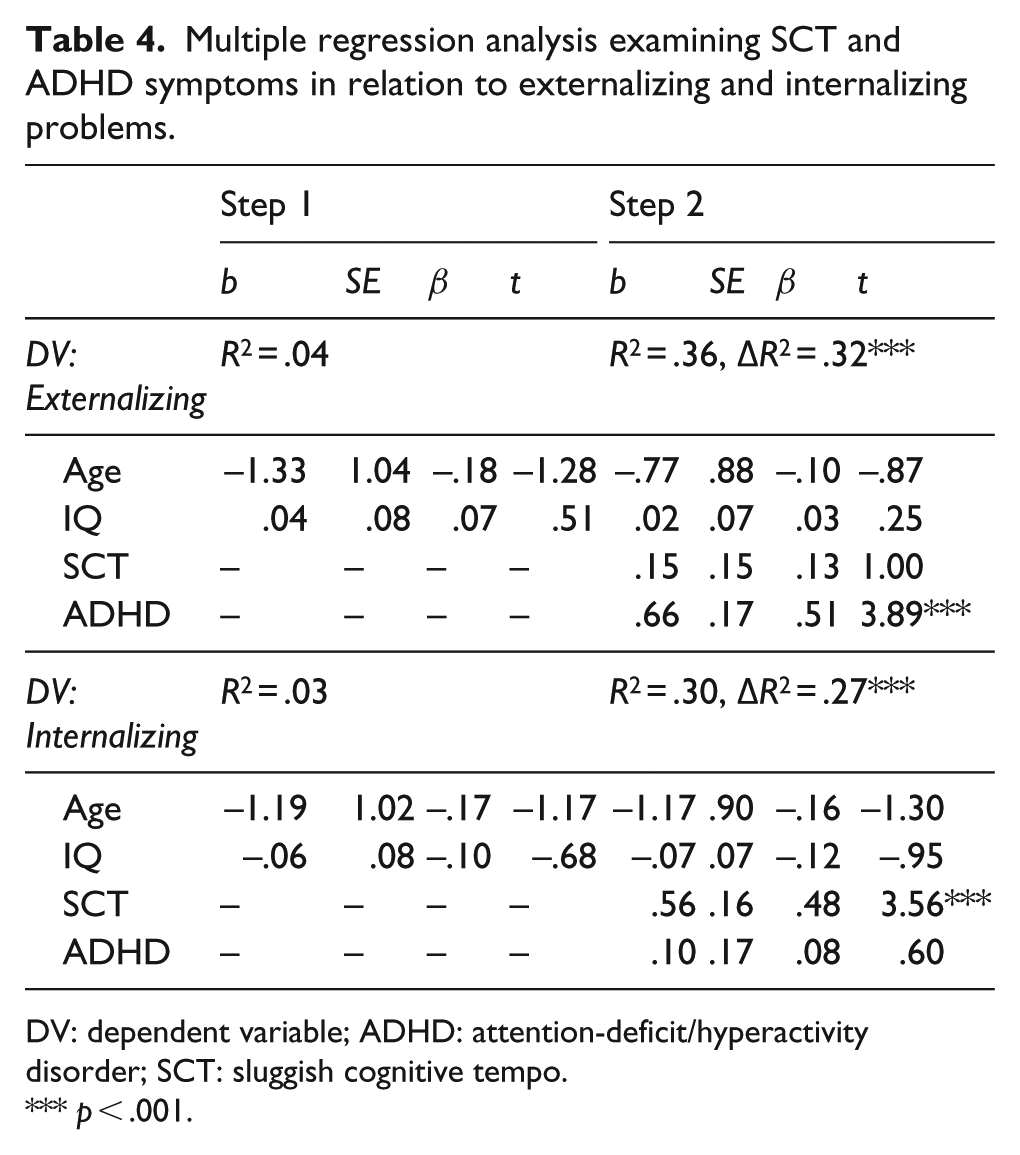
DV: dependent variable; ADHD: attention-deficit/hyperactivity disorder; SCT: sluggish cognitive tempo.
p < .001.
Regression analyses examining daily life EF
When SCT and ADHD symptoms were entered simultaneously in the model, above and beyond age and IQ, ADHD symptoms remained significantly associated with greater behavior regulation EF deficits (β = .58, p < .001) whereas SCT symptoms were no longer associated with behavior regulation deficits (β = .18, p = .188). Both ADHD symptoms and SCT symptoms remained significantly associated with greater metacognition EF deficits (βs = .47 and .43, respectively, both ps < .001; see Table 5).
Multiple regression analysis examining SCT and ADHD symptoms in behavior regulation and metacognition daily life executive functioning.
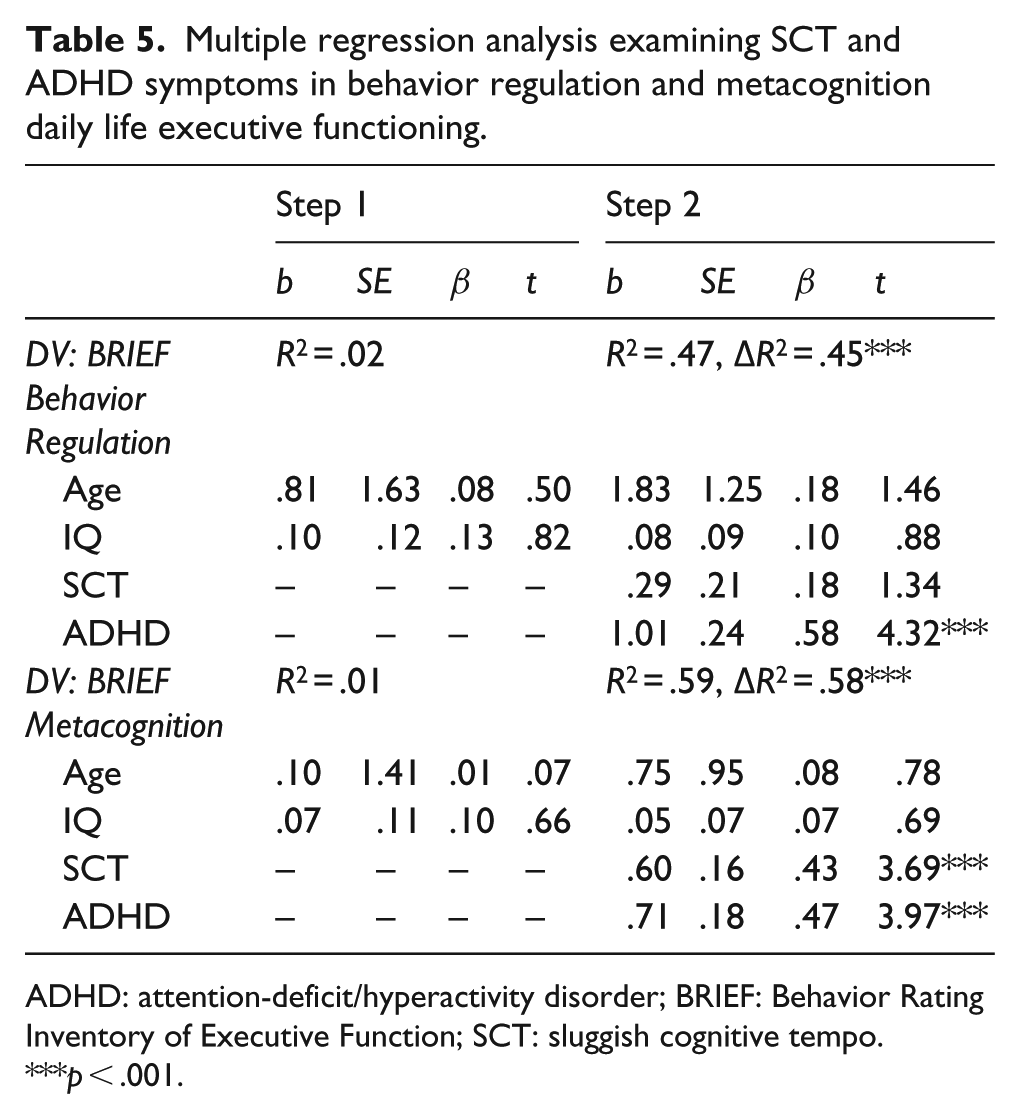
ADHD: attention-deficit/hyperactivity disorder; BRIEF: Behavior Rating Inventory of Executive Function; SCT: sluggish cognitive tempo.
p < .001.
Supplemental analyses controlling for ASD severity
Regression analyses examining SCT and ADHD symptoms in relation to CBCL externalizing/internalizing problems and BRIEF behavior regulation/metacognition were re-run with SCQ total score added as a covariate (n = 46 for the CBCL analyses and n = 43 for the BRIEF analyses). Results were unchanged, indicating that our primary findings were not confounded by autism symptomatology (see Supplemental Tables 1 and 2 for results of analyses also including the SCQ in the models).
Discussion
Our study makes a significant contribution to the literature in examining the correlates of SCT in an ASD population, particularly given the phenotypic similarities between youth with ADHD and youth with ASD (e.g. social communication deficits, EF deficits). In adolescents with ASD without intellectual disability, we found that (1) rates of clinically elevated SCT symptoms were twice as high, albeit non-significantly, than rates of clinically elevated ADHD symptoms, (2) SCT but not ADHD symptoms were associated with increased ASD symptomatology, and (3) SCT and ADHD symptoms were differentially related to other co-occurring mental health dimensions and daily life EF difficulties.
Consistent with a number of previous studies in ADHD-defined and community-based samples (Becker et al., 2016b), we found SCT and ADHD symptoms to part ways in their unique relations with internalizing and externalizing symptoms. Whereas ADHD symptoms (but not SCT symptoms) were associated with increased externalizing behaviors, SCT symptoms (but not ADHD symptoms) were associated with increased internalizing symptoms. This double dissociation has been found in other studies examining SCT and ADHD (Becker et al., 2016b), and we directly replicate this finding for the first time in adolescents with ASD without intellectual disability.
In addition, both ADHD and SCT symptoms were associated with metacognitive difficulties as rated on the BRIEF for adolescents with ASD. The metacognition index is a composite score composed of the initiate, working memory, plan/organize, organization of materials, and monitor subscales—all domains in which youth with ASD have documented problems. It is not surprising that SCT, characterized by daydreaming, mental fogginess, hypoactivity, sluggishness, and inconsistent alertness, is also associated with problems in these domains, and our findings are consistent with previous research in children with ADHD (Araujo Jiménez et al., 2015; Becker and Langberg, 2014). However, it appears ADHD symptoms are more strongly associated with metacognitive deficits in community-based samples (Barkley, 2013). Also as expected, SCT was not associated with challenges in inhibiting impulsive responses, adjusting to changes in routine/task demands, and emotional control (BRIEF behavioral regulation index) which we would expect to be more characteristic of ADHD symptoms than SCT symptoms (Araujo Jiménez et al., 2015; Barkley, 2013; Becker and Langberg, 2014). It should be noted, however, that there is some evidence that SCT is associated with poorer emotion regulation specifically (e.g. Araujo Jiménez et al., 2015; Becker et al., 2015). Studies with larger samples that can examine more nuanced aspects of EF—including both ratings and neuropsychological task performance—are warranted in youth with ASD without intellectual disability.
The positive association between SCT and ASD symptomatology is another important finding from this study, and we found this association to be robust even when controlling for age, IQ, and ADHD symptoms. Whether SCT is best conceptualized as a distinct psychiatric disorder (Barkley, 2014) or a transdiagnostic construct (Becker et al., 2016b) remains unclear. In order to examine these possibilities, it is critical to extend SCT research beyond the domain of ADHD and investigate whether SCT predicts functional outcomes across a range of clinical populations (Becker et al., 2016b). Few studies have tackled this question, although extant studies with learning-disordered (Garner et al., 2010), sleep-disordered (Becker et al., 2016a), and psychiatrically hospitalized (Becker et al., 2014) children, as well as children with prenatal alcohol exposure (Graham et al., 2013) and leukemia (Reeves et al., 2007), suggest that SCT is related to functional outcomes across a wide range of clinical populations. We replicate recent findings demonstrating SCT to be related to poorer functioning in adolescents with ASD without intellectual disability (Reinvall et al., 2017). Of course, ADHD is conceptualized as a distinct psychiatric disorder and also frequently co-occurs with and predicts impairment in ASD and many other psychiatric and medical conditions. More research is needed to determine whether SCT has validity as its own psychiatric disorder or is a construct of transdiagnostic importance, but it is increasingly clear that SCT symptoms are associated with poorer functional outcomes across sample types.
Considered together, our findings largely parallel findings showing SCT to significantly predict specific impairment domains in youth with ASD without intellectual disability (Reinvall et al., 2017). Thus, SCT may be clinically meaningful and important to assess regardless of how SCT is ultimately conceptualized. Assessing for SCT when diagnosing ASD may inform diagnostic and case conceptualization and may furthermore inform intervention. For example, an adolescent with ASD who often daydreams and needs 5–10 s to process and respond to a question or comment from an adult or peer, may benefit from being taught to verbally (e.g. “Give me a second”), or nonverbally (e.g. holding a finger up to indicate that they need a few seconds) inform others of their intention to respond. As another example, a teen who easily loses their train of thought can be taught to implement strategies to remind them to stay on task or complete a task. Clinically, we often teach adolescents to use timers or reminders on their phone or smartwatch for daily living skills tasks such as switching the laundry from the washing machine to the dryer or taking food out of the oven. Further, SCT may prevent adolescents and young adults with ASD from being successful in the classroom (e.g. difficulties maintaining the focus needed to take notes) or workplace (e.g. completing tasks in a slow or inefficient manner), and they would likely benefit from supports and compensatory strategies (e.g. audio recording classroom notes, obtaining a copy of a classmate’s notes, using checklists to complete tasks quickly and efficiently, taking short breaks to increase productivity) to increase their performance. Finally, SCT symptoms may be important for informing treatment decisions for children with ADHD (e.g. Froehlich et al., 2018), and SCT may likewise inform the heterogeneity and clinical care of youth with ASD (Reinvall et al., 2017). For example, recent research highlights elevated suicidal behaviors in youth with ASD (Mayes et al., 2013), and SCT may be a distinct predictor of suicidal risk (Becker et al., 2016c) and thus, a potentially important domain to assess when determining which youth with ASD are most at-risk. Although our findings cannot directly speak to the importance of SCT in the treatment of youth with ASD, our findings align with other studies in underscoring the importance of additional research in this area.
Our findings should be interpreted in light of study limitations. First, because our data were not derived from a formal research study, there was no information available on a variety of constructs (e.g. social withdrawal, academic performance, sleep problems), all of which have been shown to be correlates of SCT (Becker et al., 2016b). In addition, the SCT measure used included only a few items and does not capture the full picture of SCT symptomatology. Also, data were restricted to parental ratings; since it is unclear if SCT operates differently in home and school contexts (Burns et al., 2017; Watabe et al., 2014), collecting teacher ratings will be important in future studies. The sample size was relatively small and cross-sectional in nature precluding causal inferences. Thus, larger, longitudinal studies are warranted. Finally, we utilized the BRIEF to provide ratings of real-world EF, and we acknowledge some content overlap between ADHD symptoms and daily life EF items. To eliminate concerns regarding any overlap, and to more fully understand SCT in relation to EF among youth with ASD, it will be important for future research to use objective neuropsychological tasks. This is especially importance since there is generally low concordance between those sorts of tasks and BRIEF ratings (Donders, 2002). In fact, some have argued that performance-based measures and rating measures of EF assess different underlying mental constructs with former providing information regarding efficiency of processing, and the latter capturing success in rational goal pursuit (Toplak et al., 2013). In particular, it will be important for future studies to examine whether SCT symptoms are associated with performance-based measures of processing speed, including both motoric (e.g. Haigh et al., 2018; Mayes and Calhoun, 2007; Oliveras-Rentas et al., 2012) and inspection time (e.g. Barbeau et al., 2013; Kenworthy et al., 2013; Scheuffgen et al., 2000; Wallace et al., 2009) measures that may be differentially implicated in ASD.
Despite these limitations, our study used a well-characterized sample of clinically-referred adolescents with ASD without intellectual disability and found SCT to be independently related to ASD and internalizing symptomatology as well as metacognitive EF deficits. In addition, SCT symptoms are clearly elevated in non-ADHD clinical samples and, if our findings are replicated in future research, may be important to advance our understanding of ASD heterogeneity and intervention efforts.
Supplemental Material
AUT811329_Lay_Abstract – Supplemental material for Clinical correlates of sluggish cognitive tempo in adolescents with autism spectrum disorder
Supplemental material, AUT811329_Lay_Abstract for Clinical correlates of sluggish cognitive tempo in adolescents with autism spectrum disorder by Amie Duncan, Leanne Tamm, Allison M Birnschein and Stephen P Becker in Autism
Supplemental Material
AUT811329_Supplemental_material – Supplemental material for Clinical correlates of sluggish cognitive tempo in adolescents with autism spectrum disorder
Supplemental material, AUT811329_Supplemental_material for Clinical correlates of sluggish cognitive tempo in adolescents with autism spectrum disorder by Amie Duncan, Leanne Tamm, Allison M Birnschein and Stephen P Becker in Autism
Footnotes
Funding
Amie Duncan’s research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1 TR001425. Stephen Becker is supported by award number K23MH108603 from the National Institute of Mental Health (NIMH). Leanne Tamm and Amie Duncan are co-Principal Investigators on award R21HD090334-01A1 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). The content is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. National Institutes of Health (NIH).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.