
Abstract
Resilience is an increasingly popular concept in literature as a protective factor against mental ill-health. While elevated rates of anxiety and mood disorders occur in adults on the autism spectrum, there is a gap in literature investigating the application of resilience to this population. This brief report examined the factor structure and psychometric properties of the 10-item Connor–Davidson Resilience Scale in a sample of 95 autistic adults (Mage = 44). Our findings provide evidence for a unidimensional structure and robust psychometric properties of the scale in an autistic population, in line with factorial studies involving the general population.
Lay Abstract
Adults on the autism spectrum experience high rates of anxiety and depression, and may be particularly vulnerable to difficult and traumatic life experiences, which may contribute to the development and maintenance of these conditions. Resilience is an increasingly popular concept in research, which describes the ability to ‘bounce back’ following difficult emotional experiences, and the flexibility to adapt to stressful and demanding situations. The Connor–Davidson Resilience Scale has been used predominantly in studies involving non-autistic adults to measure resilience. While resilience is a potentially important concept for autistic adults, the suitability of the 10-item version of the Connor–Davidson Resilience Scale for use with adults on the spectrum has not yet been studied. In this short report, we investigate whether the Connor–Davidson Resilience Scale 10 is a valid measure to use with this population, and its relationship with other measures of mental well- or ill-being. Participants were 95 autistic adults with a mean age of 44 (63% female) who completed measures of resilience, autism symptoms, depression, anxiety and mental wellbeing. Overall, the findings indicate that the Connor–Davidson Resilience Scale 10 may be reliably used with autistic adults to measure trait resilience, which is associated with positive wellbeing and may serve as a protective factor from negative mental wellbeing. Future studies may use the Connor–Davidson Resilience Scale 10 to investigate resilience as a protective factor from negative mental health outcomes in response to traumatic and adverse emotional events for which autistic individuals may be particularly susceptible.
Introduction
It is consistently reported that adults on the autism spectrum experience a range of psychiatric comorbidities at rates significantly higher than the general population. Lifetime rates for diagnosed psychiatric conditions are reported to be between 54% and 79%, with anxiety and mood disorders being the most common (Croen et al., 2015; Lever & Geurts, 2016; Uljarević et al., 2019). However, the factors implicated in this over-representation of co-occurring psychiatric symptoms are under-researched. Given their high prevalence, persistence into adulthood and significant impact on functioning and quality of life (Robertson, 2010), understanding the risk and protective factors involved in poor mental health outcomes are key to the development of effective support programmes for this population.
An emerging area of research examining protective factors for mental health in adults from the general population has focused on the construct of resilience. The term has been used to describe the ability to recover or ‘bounce back’ following difficult emotional experiences, as well as the flexibility to adapt to stressful and demanding situations (Connor & Davidson, 2003). Findings across a range of normative and clinical populations suggest the importance of resilience in mental health and wellbeing outcomes, particularly for those who experience elevated levels of psychiatric symptoms. In a meta-analysis of resilience and mental health, Hu and colleagues reported negative correlations between resilience and indicators of mental ill-health, and conversely positive correlations with indicators of mental wellbeing for their 60 eligible studies (N = 68,720), with medium effect size (Hu et al., 2015). In this analysis, indicators of mental wellbeing included life satisfaction and positive affect, while indicators of mental ill-health included depression, anxiety and negative affect.
There is both qualitative and quantitative evidence to suggest that individuals on the spectrum are particularly vulnerable to difficult and traumatic experiences, such as bullying (Weiss et al., 2015), life-threatening injury or illness and parental divorce (Taylor & Gotham, 2016). It is possible that such adverse experiences contribute to the development and maintenance of these psychiatric comorbidities. However, despite this and noted evidence suggesting a crucial role of resilience in non autism spectrum disorder (ASD) sample, its role in ASD remains largely unexplored.
The Connor–Davidson Resilience Scale (CD-RISC) is the most frequently used instrument to measure resilience. The original, 25-item scale was designed to capture 17 characteristics of resilient people, such as ‘tolerance of negative affect’, ‘recognition of limits to control’ and ‘optimism’ (Connor & Davidson, 2003). A 10-item version of the scale (CD-RISC 10) was subsequently developed with the aim of developing a unidimensional measure of construct resilience (Campbell-Sills & Stein, 2007). The CD-RISC 10 has been translated to numerous languages and studied in a range of populations including survivors of traumatic experiences (Wang et al., 2010) and adults with long-term physical disabilities (Battalio et al., 2017). Aligned with the purpose of its original development, studies examining the factor structure of the CD-RISC 10 have consistently replicated a unifactorial structure and demonstrated strong psychometric properties (e.g. Madewell et al., 2016; Wang et al., 2010).
Despite the potential importance of resilience for the mental health of adults on the spectrum, no measures to date have been validated for this population. Therefore, the primary focus of this article is to investigate the psychometric robustness of the CD-RISC 10 in a sample of autistic adults over the age of 25. In addition, we investigate the relationship between CD-RISC 10 scores and various measures of mental ill- and well-being, to confirm the role of resilience in this population, providing insight for the future development of targeted and effective supports and interventions for their high rates of psychiatric comorbidities.
Method
Participants
Participants were 95 autistic adults who participated in the second wave of the Australian Longitudinal Study of Adults with Autism (ALSAA; Arnold et al., 2019), a nationwide longitudinal survey study funded by the Cooperative Research Centre for Living with Autism (Autism CRC). Recruitment occurred via mail and email dissemination of study advertisements to autism-specific organisations, disability employment services, autism self-advocacy groups, higher education institutions and online communities. All participants were aged 25 years or older and self-reported that they had received a clinical diagnosis of an ASD. Participants were required to report their specific diagnosis (e.g. ‘autism spectrum disorder’), year of diagnosis and details of the professional who provided the diagnosis. In addition, in order to be included in the analysis, participants had to meet the Autism Quotient-Short (AQ-Short; Hoekstra et al., 2011) cut off score of >65 that has been shown in previous research to provide optimal balance between sensitivity (0.97) and specificity (0.82). Of the original sample (N = 103), eight were dropped for missing data on the CD-RISC. Of the included sample (N = 95), two participants had missing data on the Warwick–Edinburgh Mental Well-Being Scale (WEMWBS), and two other participants missing data on the Patient Health Questionnaire-9 (PHQ-9).
Measures
Information regarding date of birth, assigned sex at birth and presence of comorbid intellectual disability was collected from survey respondents.
The CD-RISC 10 (Campbell-Sills & Stein, 2007) is a brief version of the CD-RISC 25 (Connor & Davidson, 2003), developed on the basis of factor analysis to produce a unidimensional measure of trait resilience. The items chosen for this version came from the ‘hardiness’ and ‘persistence’ factors of the original scale and have displayed good psychometric properties with a consistent unifactorial structure across studies. Participants rate 10 items on a 5-point Likert-type scale from 0 ‘Not true at all’ to 4 ‘True nearly all the time’ (score range 0–40) with higher scores reflecting greater resilience.
The American Psychiatric Association’s severity measure for generalised anxiety disorder (GAD; Craske et al., 2013) provides a dimensional assessment of GADs as defined in the fifth revision of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association, 2013). It consists of 10 items rated on a 5-point Likert-type scale from 1 ‘Never’ to 5 ‘All of the time’ (score range 10–50).
The PHQ-9 (Kroenke et al., 2001) is a nine-item screening measure of depression as described in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). It uses a 4-point scale ranging from 1 ‘Not at all’ to 4 ‘Nearly every day’ (score range 9–36), with higher scores indicating more severe depression. It has been validated in an autism sample.
The WEMWBS (Tennant et al., 2007) consists of 14 positively worded items measuring different aspects of positive mental health. Responses are scored on a 5-point Likert-type scale ranging from 1 ‘None of the time’ to 5 ‘All of the time’ (score range 14–70), with higher scores indicating greater mental wellbeing.
CD-RISC factor structure, reliability, and validity
The CD-RISC was examined for latent components using the Exploratory Structural Equation Modelling framework (ESEM; Asparouhov & Muthén, 2009). Similar to confirmatory factor analysis (CFA), ESEM provides a comprehensive set of indices that can be used to assess the fit of the model, unlike CFA, which only allows items to load onto the hypothesised factor while setting the loading to zero onto other factors, an assumption suggested as unrealistic when applied to behavioural, psychological and psychiatric data (Marsh et al., 2014). Although ESEM has the noted advantages over the CFA approach where two or more latent factors are present, for unidimensional factor solutions these two latent variable approaches perform identically (given that all items load onto only one factor). ESEM was conducted with MPLUS 8.0 (Muthén & Muthén, 1998–2011) using the maximum likelihood estimator which is robust to non-normal data distribution and specifying the geomin rotation. The comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), the standardised root mean square residual (SRMR) and the chi-square test were used to evaluate model fit. For the CFI and TLI, values >0.90 or >0.95 indicate adequate and excellent fit, respectively. For the RMSEA and SRMR, values of <0.08 or <0.06 indicate adequate and excellent fit, respectively (Hu & Bentler, 1999). The 90% confidence interval for the RMSEA was used to test significance with a threshold of <0.08, with the close fit-test significance level set at a p-value of >0.05 (Kline, 1998).
The reliability of the scale was evaluated via both the composite reliability index (CRI; Bagozzi & Yi, 2012) and Cronbach’s alpha reliability coefficient. CRI is an indicator of the shared variance among the observed variables that serve as indicator of a latent construct and it provides a more reliable index of scale reliability than Cronbach’s alpha when measurement errors are either correlated or uncorrelated (Bagozzi & Yi, 2012). Values above 0.60 are considered as adequate. Validity of the CD-RISC scale was examined by first exploring its relationship with autism symptom severity (indexed by total Autism Quotient (AQ) score), then its relationship with negative (indexed by the GAD and PHQ-9) and positive (indexed by the WEMWBS) aspects of well-being. Correlations with age and gender were also explored. Past studies tend to suggest lower CD-RISC scores for students and young adults compared with adults from general population samples, and inconclusive past evidence regarding gender (Connor & Davidson, 2003; Davidson & Connor, 2017).
Results
In the present sample, 63% were female with a mean age of 44 years (SD = 12.3), mean CD-RISC score of 20.4 (SD = 8.0) and a mean AQ score of 90 (SD = 9.6; range = 69–112). The majority of the sample was diagnosed with Asperger’s Syndrome (59%) or autism spectrum condition/disorder (32%) with one participant (1%) reporting comorbid intellectual disability.
A single factor solution model provided excellent fit to the data (chi-square test = 41.64, p = 0.20; CFI = 0.986, TLI = 0.982; RMSEA = 0.045, close fit test p = 0.54; SRMR = 0.038). All items showed good to excellent loadings ranging from 0.53 to 0.83. Factor loadings, item-factor correlations and item frequency are presented in Table 1.
Factor loading, item-scale correlations and item endorsement.
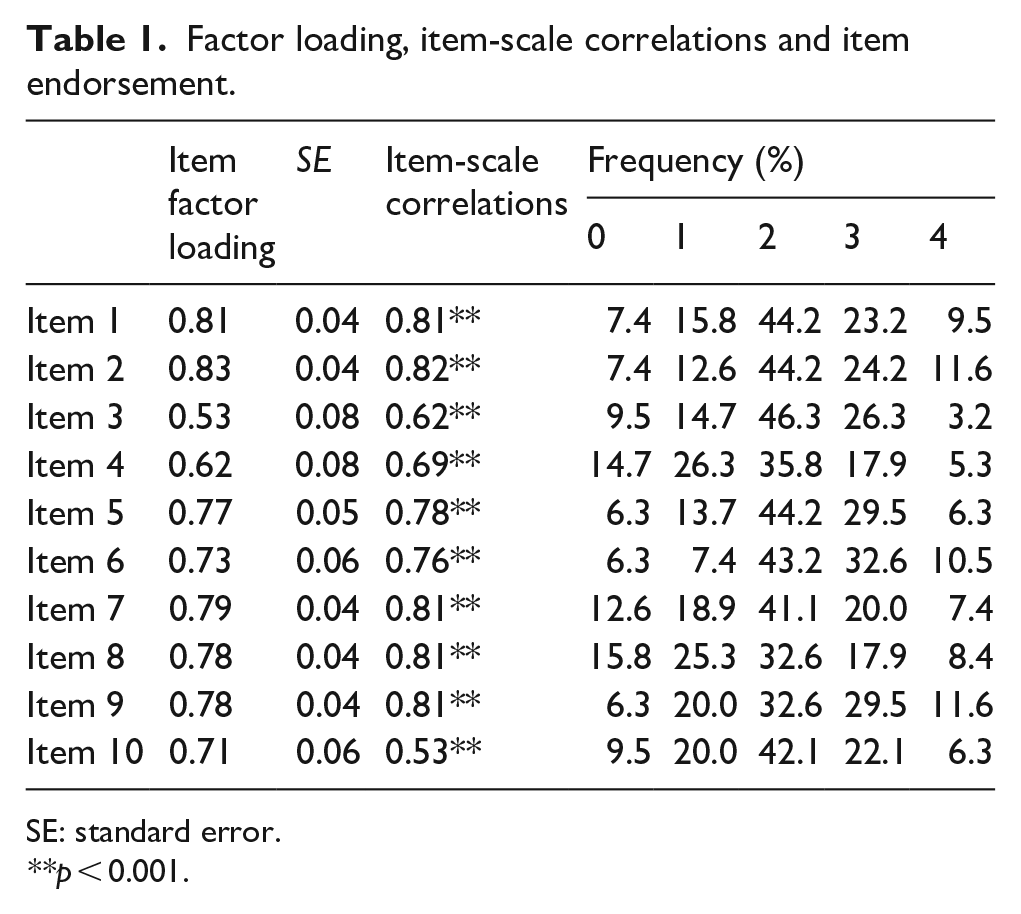
SE: standard error.
p < 0.001.
The reliability of the derived factors was in the good to excellent range as indicated by a CRI of 0.90 and Cronbach’s alpha of 0.92, with a mean item-scale correlation of 0.74 (SD = 0.09). Correlations between the study measures are presented in Table 2.
Pearson’s correlations between study measures with 95% confidence intervals.
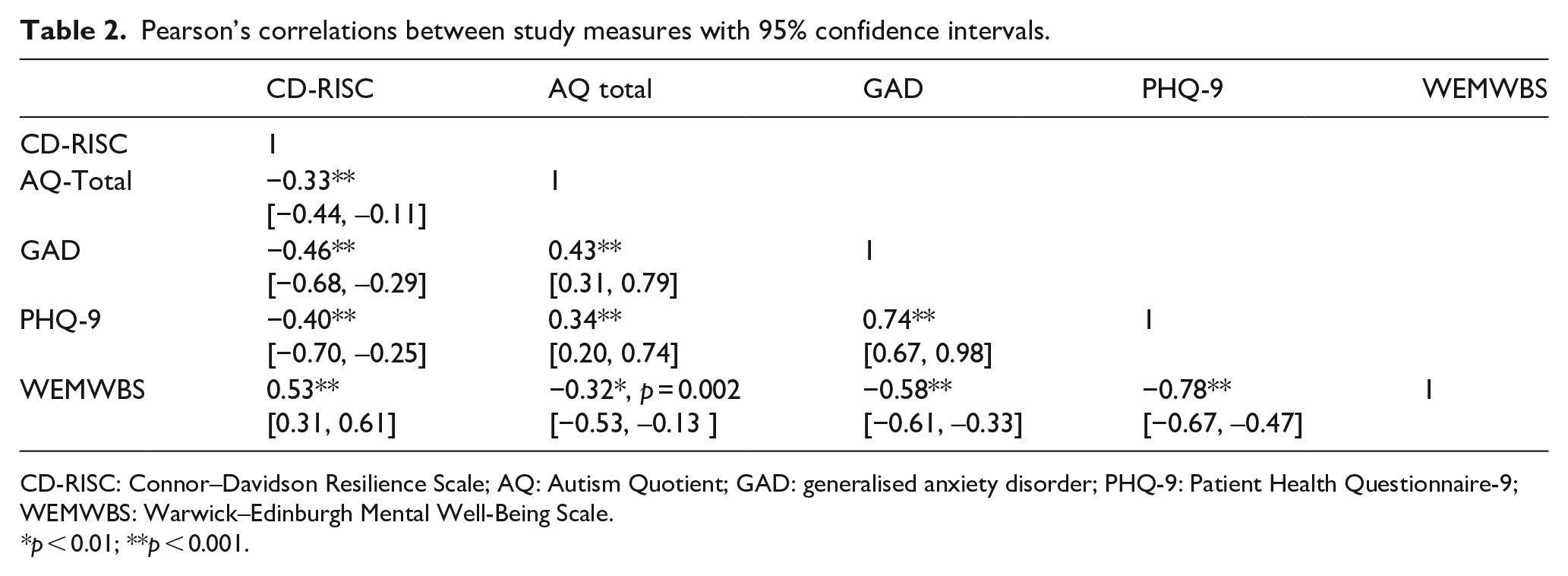
CD-RISC: Connor–Davidson Resilience Scale; AQ: Autism Quotient; GAD: generalised anxiety disorder; PHQ-9: Patient Health Questionnaire-9; WEMWBS: Warwick–Edinburgh Mental Well-Being Scale.
p < 0.01; **p < 0.001.
Neither age nor sex was associated with the CD-RISC scores. Significant negative associations were found between the CD-RISC and the GAD (r = –0.46, p < 0.001), PHQ-9 (r = –0.40, p < 0.001) and AQ (r = –0.33, p < 0.001), while positive associations existed between the scale and WEMWBS (r = 0.53, p < 0.001). The AQ total score was associated with the GAD (r = 0.43, p < 0.001), PHQ-9 (r = 0.34, p < 0.001), and WEMWBS (r = –0.32, p = 0.002). Fisher’s r-to-z transformation was used to formally test whether the strength of the correlations differed between males and females. None of the comparisons were statistically significant (CD-RISC – AQ-total correlation: p = 0.68; CD-RISC – GAD: p = 0.49; CD-RISC – PHQ-9: p = 0.94; CD-RISC – WEMWBS: p = 0.27).
Discussion
The aim of this investigation was to explore the psychometric properties of the CD-RISC 10 in a sample of autistic adults. Our findings provide evidence for a unidimensional structure and robust psychometric properties of the scale in an autistic population, in line with factorial studies of this scale in non-ASD samples. High item-total scale relationships provided additional evidence for the construct validity and unidimensional measure of trait resilience in autistic adults. The scale also displayed convergent and divergent validity, demonstrated by the distinct pattern of relationships with positive and negative aspects of mental wellbeing.
Overall, these findings indicate that the scale may be reliably used with autistic adults to measure trait resilience; a single factor indicating one’s ability to cope with stress (Connor & Davidson, 2003) which is associated with positive wellbeing and may serve as a protective factor from negative mental wellbeing. Future studies may use the CD-RISC 10 to model the role of resilience as a protective factor from negative mental health outcomes in response to traumatic and adverse emotional events for which autistic individuals may be particularly susceptible. Comparisons may be drawn between the presentation and effects of resilience for those on the spectrum and those not on the spectrum, in order to develop the most accurate understanding for this population. Models should also consider autism-related factors that are known to affect mental health outcomes, such as intolerance of uncertainty, sensory processing differences, emotion regulation and certain aspects of temperament, including both reactivity and regulation components (Cai et al., 2018).
The findings also have important implications for the development of clinical interventions for depression, anxiety and other effects of traumatic or stressful experiences. The reported relationships between resilience and positive and negative aspects of wellbeing are aligned with the intention of the authors of the CD-RISC, who envisaged resilience to be an important target for the ‘. . . treatment of anxiety, depression and stress reactions’ (Connor & Davidson, 2003).
Given their particular vulnerability to stressful and negative life events, it will also be important to understand the relationship between the CD-RISC 10 and measures that explore strategies to manage stressful events and the negative emotions that result, such as the Brief COPE (Carver, 1997). It will be important for future studies to compare the predictive validity and explanatory power of the CD-RISC against alternative measures of resilience that exist with a slightly differing conceptual focus.
The generalisability of these findings are limited by the self-report design of the study which did not collect clinically validated diagnoses for the autism sample. While not clinically validated, participants were required to explicitly indicate that they had received a formal diagnosis, report which year the diagnosis occurred, by which medical professional (profession and name) and which diagnostic label they were given. We believe the explicit nature and specificity of these questions, together with the voluntary (non-reimbursed) and extensive (up to 3 h to complete) nature of the survey, minimise the risk of fraudulent or inappropriate responding by those without a diagnosis. This method has been argued as suitable for research that may be generalisable to adults who identify as autistic (Bal & Lounds Taylor, 2019). This is particularly relevant for the ‘hidden population’ (Lai & Baron-Cohen, 2015) of middle-aged and older autistic adults for whom significant barriers to obtaining a diagnosis exist. In such cases, rigour can be raised by the inclusion of an autism measure (Bal & Lounds Taylor, 2019) as was done in this study via use of the AQ-short. This approach was deemed appropriate by the autistic advisors.
This was a predominantly female sample, a common self-selection bias that occurs in online survey studies involving both autistic and non-autistic adults (e.g. Nicolaidis et al., 2013). While no correlation was observed between CD-RISC 10 scores and sex, it may be useful to replicate the findings in a larger scale study enabling the investigation of structural invariance across sexes. Overall, the findings indicate support for the use of the CD-RISC 10 as a measure of trait resilience in autistic adults.
Footnotes
Acknowledgements
We are grateful for the contribution and participation of all adults on the autism spectrum and their carers involved in the ALSAA study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Cooperative Research Centre for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centres Programme.