
Abstract
People with Autism Spectrum Disorder show an increased risk of experiencing potentially traumatic events, particularly social victimization. However, Autism Spectrum Disorder and Post-Traumatic Stress Disorder co-occurrence was hardly studied. We examined exposure to potentially traumatic life events and PTSD symptoms in adults with Autism Spectrum Disorder vs typical adults. Twenty-five adults with Autism Spectrum Disorder and 25 typical adults were comparable on age and gender. Participants self-reported on potentially traumatic life events of social and non-social nature, and on PTSD symptoms related to their most distressing event. Results showed higher rates of probable-Post-Traumatic Stress Disorder in the Autism Spectrum Disorder group (32%) compared with the typical adults group (4%). Individuals with Autism Spectrum Disorder reported more PTSD symptoms, particularly re-experiencing and hyper-arousal, compared with typical adults, although the latter was elevated only in females with Autism Spectrum Disorder. Participants with Autism Spectrum Disorder, especially females, reported more negative life events, particularly social events, than typical adults. Sixty percent of Autism Spectrum Disorder participants, but only 20% of typical adults, chose a social event as their most distressing event. Individuals with Autism Spectrum Disorder and probable-Post-Traumatic Stress Disorder co-occurrence presented poorer social skills compared with those with Autism Spectrum Disorder alone. Results indicate increased vulnerability of individuals with Autism Spectrum Disorder to trauma and Post-Traumatic Stress Disorder, especially due to social stressors. Females with Autism Spectrum Disorder may be particularly vulnerable to Post-Traumatic Stress Disorder.
Lay Abstract
People with Autism Spectrum Disorder show an increased risk of experiencing traumatic events, particularly social victimization. However, Autism Spectrum Disorder and Post-Traumatic Stress Disorder co-occurrence was hardly studied. We examined exposure to traumatic life events and Post-Traumatic Stress Disorder symptoms in adults with Autism Spectrum Disorder vs typical adults. Two groups took part in this study: Twenty-five adults with Autism Spectrum Disorder and 25 typical adults of similar age and male to female ratio. Participants completed questionnaires on potentially traumatic life events of social and non-social nature, as well as on Post-Traumatic Stress Disorder symptoms related to their most distressing event. Participants also filled out an autism traits questionnaire. Results showed a higher Post-Traumatic Stress Disorder rate in the Autism Spectrum Disorder group (32%) compared with the typical group (4%). Individuals with Autism Spectrum Disorder reported more Post-Traumatic Stress Disorder symptoms, particularly re-experiencing and increased physiological arousal, compared with typical adults, although the latter was elevated only in females with Autism Spectrum Disorder. Participants with Autism Spectrum Disorder, especially females, reported more negative life events, particularly social events, than typical adults. Sixty percent of Autism Spectrum Disorder participants, but only 20% of typical participants, chose a social event as their most distressing event. Individuals with Autism Spectrum Disorder who were also suspected as having Post-Traumatic Stress Disorder (based on their questionnaires) presented poorer social skills compared with those with Autism Spectrum Disorder alone. Results indicate that individuals with Autism Spectrum Disorder are more susceptible to trauma and Post-Traumatic Stress Disorder, particularly due to social stressors. Females with Autism Spectrum Disorder may be especially vulnerable to Post-Traumatic Stress Disorder.
Keywords
Introduction
Autism Spectrum Disorder is a neurodevelopmental condition, characterized by social communication deficits, and restricted, repetitive, behavior patterns (American Psychiatric Association [APA], 2013). It is well documented that individuals with Autism Spectrum Disorder (ASD) experience high rates of psychiatric co-occurrence, with other conditions—attention-deficit/hyperactivity disorder (ADHD), anxiety, and depression being the most commonly diagnosed (Joshi et al., 2012). Recently it has been suggested that individuals with ASD are at an increased risk of experiencing potentially traumatic events and being significantly affected by them (Haruvi-Lamdan et al., 2018; Kerns et al., 2015). The current study examined the association between ASD and symptoms of Post-Traumatic Stress Disorder (PTSD).
PTSD is the most common chronic stress disorder resulting from exposure to traumatic events. According to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), post-traumatic symptoms fall into four main clusters: Re-experiencing symptoms (e.g. recurrent distressing memories or dreams, flashbacks); Cognitive and behavioral avoidance of traumatic reminders; Negative alterations in cognition and mood (e.g. inability to experience positive emotions, negative beliefs, or expectations); and Alterations in hyper-arousal (e.g. startle responses, irritable behavior and anger, sleep disturbances). More than 80% of individuals with PTSD have one or more co-occurring conditions, most commonly depression, anxiety, and substance abuse disorders (Van Minnen et al., 2015). PTSD severity has been shown to worsen by high co-occurrence with other psychiatric conditions (e.g. Kessler, 2000). While the vast majority of the population is exposed to a potentially traumatic event at some point in life, only a small percentage (5.6% lifetime prevalence; Koenen et al., 2017) will develop PTSD. Various studies have attempted to identify different factors related to risk and maintenance of PTSD (e.g. Marx & Gutner, 2015).
However, a surprisingly small number of studies have examined the susceptibility to PTSD in individuals with neurodevelopmental conditions. Studies suggest that youth with intellectual and developmental disabilities are 1.5 to over 3 times more likely to be maltreated (Hibbard & Desch, 2007; Reiter et al., 2007) or to be exposed to trauma in general (Martorell & Tsakanikos, 2008), compared with their typically developing peers. A few studies have shown that individuals with ASD are exposed and strongly affected by traumatic events, especially abuse (e.g. Cook et al., 1993; Mandell et al., 2005; Taylor & Gotham, 2016). However, these were either case studies or uncontrolled studies. Furthermore, most of these studies focused on children and relied on parental report. Finally, the ASD samples were highly heterogeneous in terms of intellectual abilities, and, most importantly, PTSD symptoms (PTSS) were rarely measured as the outcome of exposure to traumatic events. To the best of our knowledge, only one study focused on PTSD and ASD, which examined it among children following various traumatic events, such as accidents, natural disasters, violence, and abuse (Mehtar & Mukaddes, 2011). This study reported a PTSD prevalence of 17.4% in children with ASD. Four studies examined PTSD rates as part of a general examination of psychiatric conditions co-occurring with ASD; two examined it among children and adolescents and found a PTSD prevalence of 1.7% (Reinvall et al., 2016) and 0% (de Bruin et al., 2007). Three studies examined psychiatric symptomatology among adults with ASD and found PTSD rates of 7% (Strunz et al., 2014), 1.6% (Hofvander et al., 2009), and 0% (Taylor & Gotham, 2016). Four studies measured PTSS as part of research on anxiety disorder treatment among children and adolescents and found PTSD rates of 2.5% (Wood et al., 2009), 3.3% (White et al., 2013), 3.1% (McConachie et al., 2014), and 3% (Wood et al., 2015). Another study by Storch and colleagues (2013) reported a PTSD rate of 3% in an ASD sample, and PTSD was associated with suicidal thoughts and behaviors. Finally, Hollocks and colleagues (2016) focused on cognitive and biological correlates of anxiety in ASD and reported no co-occurrence with PTSD. It is therefore hard to draw clear conclusions from those different findings. In addition, Kildahl and colleagues (2019) reviewed studies that examined post-traumatic symptoms in individuals with ASD and intellectual impairments. Their findings highlight the gaps in the literature regarding the identification of PTSD in individuals with ASD. The majority of reviewed studies did not include a standard measurement of PTSS and studies varied in sample characteristics, methodology, and types of traumatic events. Finally, a growing body of evidence suggests that, compared with those with low levels of autistic traits (AT), individuals with higher levels of AT in the general population are more exposed to potentially traumatic events (Dell’Osso et al., 2018; Kunihira et al., 2006), and suffer from higher levels of PTSS following them (Haruvi-Lamdan et al., 2019; Roberts et al., 2015).
Interestingly, PTSD and ASD show an opposite directionality of gender-related vulnerability. PTSD is common approximately twice as more in females as in males due to various risk factors (e.g. traumatic exposure, genetic and biological vulnerability). Males and females with PTSD were also found to differ in terms of symptom cluster manifestation (Farhood et al., 2018; Yehuda et al., 2015). ASD, on the other hand, is more common in males than in females, with a male to female ratio varying from 3:1 (Loomes et al., 2017) to 16:1 (Ferri et al., 2018). Previous studies suggested gender differences in core ASD symptoms and raised the possibility of different male and female phenotypes (Hull et al., 2017; Lai et al., 2015). In both research fields, studies attempt to shed further light on gender differences and vulnerability. To the best of our knowledge, the levels of PTSS among individuals with ASD have not been explored in relation to gender.
The definition of a traumatic event has changed throughout the years, since the introduction of PTSD in Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III; APA, 1980). Although there is still an ongoing debate regarding this definition (Larsen & Berenbaum, 2017), DSM-5 defines a traumatic event as one which involves a direct or indirect exposure to actual or threatened death, serious injury, or sexual violence (APA, 2013). This debate is highly relevant when examining the unique experiences of individuals with neurodevelopmental conditions. A review that examined trauma and PTSD among adults with intellectual impairments discussed the difficulty to differentiate between stressful life events and traumatic events, and argued for broadening the examination of different types of events and experiences that may potentially be perceived as traumatic (Martorell & Tsakanikos, 2008). Another review, by Kerns et al. (2015), indicated that individuals with ASD may experience a variety of stressful situations (e.g. intense sensory stimuli, changes in routine, medical ordeals) as traumatic. Various characteristics of sensation, perception, social awareness, and cognition, which are unique to individuals with ASD, may determine which events would be experienced by them as traumatic. A recent article discussed this issue and focused on traumatic subjective perception of three groups of patients who are at risk to developing PTSD, one being ASD (Brewin et al., 2019). The authors argued that these groups’ PTSS are often overlooked and suggested adding an “altered perception” subtype to PTSD criteria in the future. Specifically, it is possible that social stressors are a significant source of vulnerability for individuals with ASD (Haruvi-Lamdan et al., 2018; Hoover, 2015). Several studies suggest that social demands are more often appraised as stressful by individuals with ASD compared with typical individuals (Gillott & Standen, 2007; Jansen et al., 2003). Individuals with ASD experience greater social isolation and distress compared with their typical peers (Tani et al., 2012). Therefore, it is reasonable to assume that some social interactions are experienced as particularly stressful, and even traumatic, among this population. Furthermore, children and adults with ASD are more often verbally, physically, and socially bullied, relative to the general population (Bitsika & Sharpley, 2014; Falla & Ortega-Ruiz, 2019; Schroeder et al., 2014). Studies have shown that children with ASD are bullied more often than peers with other disabilities (Sreckovic et al., 2014; Zeedyk et al., 2014). However, PTSS were not measured in any of these studies (Hoover, 2015), although previous studies among the general population suggested bullying is a potential precursor of PTSD (Idsoe et al., 2012; Nielsen et al., 2015).
The main aim of this study was to examine PTSS among adults with ASD and typical adults (TA), following various potentially traumatic life events, including a wide range of negative social events (such as bullying and social exclusion), as well as events more commonly studied in relation to PTSD (such as exposure to war or terror, serious accidents or injury). We aim to shed light on the level of PTSS in adults with ASD, and to examine the moderating role of gender. Moreover, we aim to understand which types of events are perceived as traumatic for adults with ASD, and specifically whether negative social events are more commonly associated with PTSS in this group. Finally, we aimed to assess whether the existence of an ASD and probable PTSD co-occurrence exacerbates the clinical picture of ASD.
Methods
Participants
Fifty adults, aged 18–35 (M = 22.82, SD = 3.57), participated in the study: 25 with a formal diagnosis of ASD and 25 TA. The groups were comparable on age and gender (10 females in each group). Participants of both groups were invited to take part in a life events study, using advertisements placed in Internet forums and social networks. Participants with ASD were also recruited through non-governmental organizations, which operate community programs for adults with ASD in Israel. Inclusion criteria for both groups were age of 18 and above, and Hebrew as a native tongue. Typical participants were screened-out for ASD using the Autism-Spectrum Quotient (AQ; Baron-Cohen et al., 2001), and all scored below cutoff. Inclusion criteria for the ASD group was a formal diagnosis of ASD with no intellectual impairment, from a clinical psychologist or psychiatrist, and recognition of the diagnosis by the Israel Ministry of Welfare and the National Insurance service. Individuals with a self-reported diagnosis of psychosis were excluded from the study (n = 1). Among males, the median age in which they were diagnosed with ASD was 4.5 while among females the median age for diagnosis was 14. Only two participants (8%) with ASD had a legal guardian. The majority of participants were Jewish, single, and born in Israel.
No differences were found between the groups regarding self-reported socio-demographic characteristics or psychiatric co-occurring conditions. In the ASD group, 20% reported on co-occurring ADHD, 8% on depression and anxiety, and 4% on OCD. In the TA group, 12% reported a current diagnosis of ADHD, and 4% reported a diagnosis of depression and anxiety. An ASD-TA group difference in background variables was found only for education (χ2(1) = 13.60, p < 0.001), with more typical participants reporting academic education (n = 20, 80%), compared with participants with ASD (n = 7, 28%). Table 1 presents the sample’s characteristics and group differences on the study’s measures.
Sample characteristics and group differences.

ASD: Autism Spectrum Disorder; TA: typical adults; PTSD: Post-Traumatic Stress Disorder; PCL-5: PTSD Checklist for DSM-5; AQ: Autism-Spectrum Quotient.
p < 0.05, **p < 0.01, ***p < 0.001.
Procedure
Initially, a short telephone interview was conducted in order to assess compatibility to the study, as well as to provide information on the study, and to schedule a meeting. All participants and, when required, their legal guardians, provided written informed consent. All participants completed self-report questionnaires during a face to face meeting with a qualified member of the research team. Participants were compensated for their time. The study received an official ethical approval from Bar-Ilan University’s institutional review board (IRB), where the study was conducted.
Measures
Socio-demographic background
Participants were presented with a variety of background questions assessing socio-demographic factors, including date and place of birth, family status, socio-economic status, religiosity, and psychiatric diagnoses.
Traumatic life events
This measure includes a comprehensive list of potentially traumatic life events, divided into two parts: The first part was based on the Life Events Checklist for DSM-5 (LEC-5; Weathers, Blake, et al., 2013). It included events such as sexual assault, exposure to war or terror, a serious accident, and life-threatening illness or injury. These events are compatible with the traumatic event definition (Criterion A) in the DSM-5. Thus, we considered them as “PTSD criterion A events” (APA, 2013). The second part comprised a list of negative interpersonal situations that were based on a bullying questionnaire (Sourander et al., 2010). These included exposure to various forms of bullying and cyberbullying, including physical (e.g. hitting, pushing), verbal (e.g. name-calling, threats), or psychological (e.g. social exclusion, ostracism). In the current study, we considered them as “negative social events.” Participants were asked to record stressful events, which they have experienced during their lifetime. Next, they were asked to note which event caused them the most significant distress from the entire list.
PTSD Checklist for DSM-5 (PCL-5), Specific Version
The PCL-5 (Weathers, Litz, et al., 2013) is a self-report questionnaire measuring PTSS in the preceding month. Items correspond directly with the 20 symptoms of PTSD appearing in DSM-5 (APA, 2013). The PCL-5-S (specific) asks about symptoms in relation to an identified stressful experience. Participants were asked to complete it while referring to the event, which they marked as most distressing, from the potentially traumatic life events list described above. The self-report rating scale is 0–4 for each symptom (from “Not at all” to “Extremely”). The PCL-5 yields a total score, a score for each symptom cluster, and a probable PTSD diagnosis according to a cutoff score of 38, which is commonly used in trauma studies (Bovin et al., 2016). The PCL-5 has been shown to have very good psychometric properties (Blevins et al., 2015). In the current study, the instrument has shown excellent internal consistency (Cronbach’s alpha = 0.94).
The Autism-Spectrum Quotient (AQ)
The AQ (Baron-Cohen et al., 2001) has been used extensively as a self-report measure of AT, and as a screener for ASD. It comprises 50 items, grouped into five theory-driven clusters: social skill difficulties, communication difficulties, attention switching difficulties, attention to details, and limited imagination. Participants rate to what extent they agree or disagree with each statement on a 4-point Likert-type scale ranging from 1 (“definitely agree”) to 4 (“definitely disagree”). Using a binary scoring system (o or 1), scores range between 0 and 50, with a higher total score suggesting more AT. AQ scores have been shown to be stable cross-culturally (Hurst et al., 2007) and demonstrated good diagnostic validity (Baron-Cohen et al., 2001). In the current study, the AQ has shown very good internal consistency (Cronbach’s alpha = 0.89).
Results
Associations between ASD and PTSS
An examination of differences in probable PTSD rates revealed that the proportion of participants in the ASD group reporting a probable PTSD diagnosis according to the PCL cutoff score of 38 (n = 8, 32%) was 8 times higher than in the typical group (n = 1, 4%; Fisher’s exact test p < 0.05). Pearson correlations revealed that PCL total score (r = 0.58, p < 0.01), re-experiencing (r = 0.51, p < 0.01), negative alterations in mood and cognition (r = 0.51, p < 0.01), and hyper-arousal (r = 0.48, p < 0.05) symptoms significantly correlated with the social skills sub-scale of the AQ in the ASD group. In the typical group, PTSS were significantly correlated with both the AQ subscales of social skills and attention to details: the PCL total score (r = 0.40, p < 0.05), re-experiencing (r = 0.44, p < 0.05), and negative alterations in mood and cognition (r = 0.53, p < 0.01) symptoms were associated with social skills difficulties; The PCL total score (r = 0.49, p < 0.05), re-experiencing (r = 0.63, p < 0.01), and negative alterations in mood and cognition (r = 0.42, p < 0.01) were associated with the AQ’s attention to details subscale.
Next, a multivariate analysis of covariance (MANCOVA) was conducted, with group and gender as the independent variables, and PCL scores (total score and the four symptom cluster scores) as the dependent variables. Since the ASD and typical groups differed on education level, this variable was added to the analysis as a covariate. Table 2 presents descriptive PTSS scores by group and gender.
Means (SD) of PTSD symptom scores by group and gender.
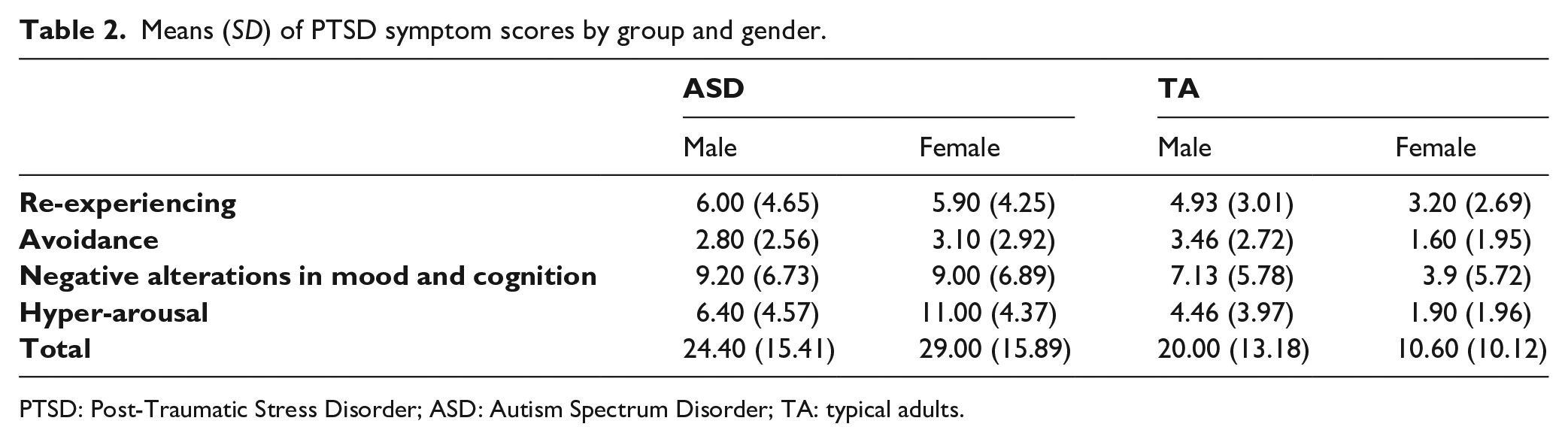
PTSD: Post-Traumatic Stress Disorder; ASD: Autism Spectrum Disorder; TA: typical adults.
The MANCOVA showed a significant main effect for group (F(4,42) = 6.24, p < 0.001, η2 = 0.37), and a significant group × gender interaction effect (F(4,42) = 2.82, p < 0.05, η2 = 0.21). Univariate analyses revealed that compared with typical participants, those with ASD reported a significantly higher PCL total score (F(1,45) = 7.56, p < 0.01, η2 = 0.14), as well as significantly higher levels of PTSS of re-experiencing (F(1,45) = 4.39, p < 0.05, η2 = 0.08) and hyper-arousal (F(1,45) = 20.27, p < 0.001, η2 = 0.31). A marginally significant difference was also found for negative alterations in mood and cognition, with higher scores reported among participants with ASD, compared with TA (F(1,45) = 3.63, p = 0.063, η2 = 0.075). Figure 1 presents group differences in PTSS.
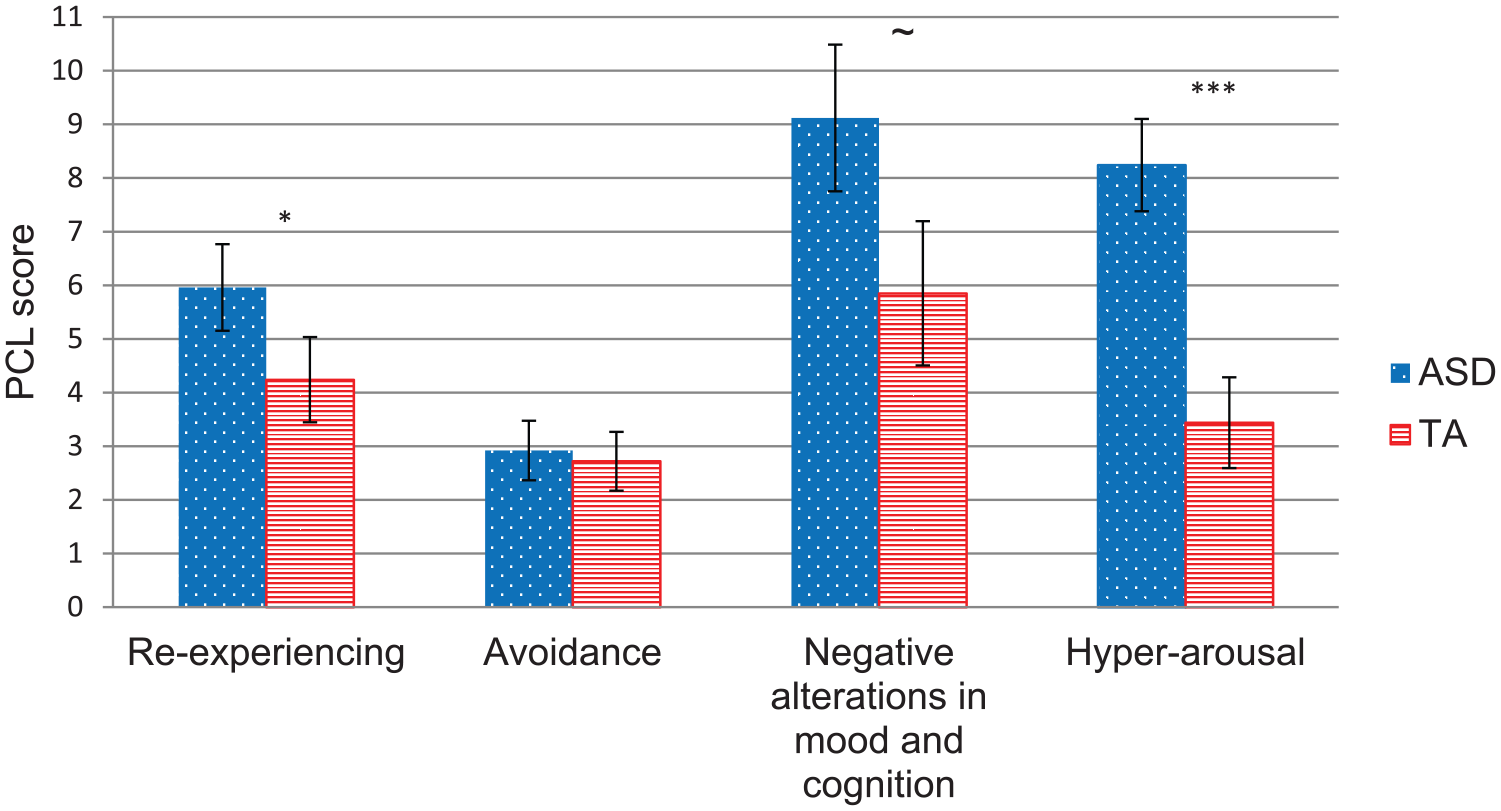
Groups differences in PTSD symptoms.
A univariate interaction analysis revealed that the source of the multivariate interaction effect was a significant interaction for hyper-arousal symptoms (F(1,45) = 9.65, p < 0.01, η2 = 0.18). A simple effects analysis showed that while the difference in hyper-arousal symptoms between females with ASD and TA females was significant, with the latter showing lower symptom levels (i-j = 9.27, SE = 1.90, p < 0.001), no difference was found between males with ASD and typical males (i-j = 2.02, SE = 1.49, p = 0.18). A marginally significant gender × group interaction was also found for PCL total score (F(1,45) = 3.14, p = 0.083, η2 = 0.065), again with females with ASD reporting higher symptom levels than typical females.
The severity of ASD symptoms as a function of co-occurrence with probable PTSD
Next, we set out to examine whether the existence/non-existence of the co-occurrence of ASD with probable PTSD is associated with greater ASD symptom severity. Thus, we conducted a MANOVA comparing between those with ASD alone (no co-occurring probable PTSD; n = 17) and those with ASD-prob.PTSD (ASD and probable PTSD; n = 8) co-occurrence on AQ scores. The analysis showed a significant main effect for ASD-prob.PTSD co-occurrence (F(5,19) = 3.31, p < 0.05, η2 = 0.46). Univariate analyses revealed that compared with those without a probable PTSD diagnosis (i.e. ASD only), those with ASD-prob.PTSD co-occurrence reported a significantly higher AQ score on the social skills subscale (F(1,23) = 9.98, p < 0.05, η2 = 0.303). Unfortunately, due to the very small number of participants with probable PTSD from the TA group (n = 1), we were unable to assess the same question regarding PTSS severity.
Exposure to potentially traumatic life events
As noted earlier, in this study we chose to examine a wide variety of potentially traumatic life events, including events clearly meeting the PTSD DSM-5 events criterion (criterion A; e.g. war, sexual assault, traffic accidents) and social stressors, such as bullying and ostracizing. A MANCOVA was conducted, with group and gender as the independent variables, and number of potentially traumatic life events (total count, number of negative social events and PTSD criterion A events) as the dependent variables. Due to the between-group difference in education, the latter was added as a covariate. The MANCOVA yielded main effects for group (F(2,44) = 14.64, p < 0.001, η2 = 0.40), gender (F(2,44) = 9.60, p < 0.001, η2 = 0.304), and the group × gender interaction (F(2,44) = 4.50, p < 0.05, η2 = 0.17). Univariate analyses revealed that the source of the multivariate group effect was a significant difference between the ASD and TA groups in both the total number of potentially traumatic events (F(1,45) = 11.06, p < 0.01, η2 = 0.20) and the number of negative social events (F(1,45) = 25.12, p < 0.001, η2 = 0.36), with participants with ASD reporting higher exposure compared with typical participants. No group difference was found for the number of PTSD criterion A events. Table 3 presents average numbers of potentially traumatic life events by group and gender.
Mean numbers (SD) of potentially traumatic life events by group and gender.
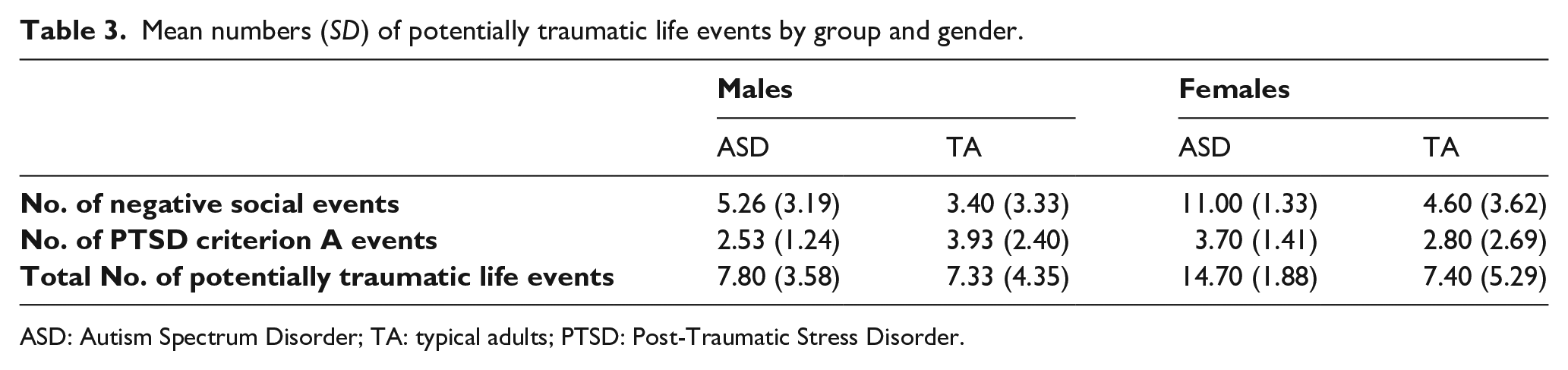
ASD: Autism Spectrum Disorder; TA: typical adults; PTSD: Post-Traumatic Stress Disorder.
In addition, significant gender differences were found regarding the total number of potentially traumatic events (F(1,45) = 9.40, p < 0.01, η2 = 0.17) and the number of negative social events (F(1,45) = 17.90, p < 0.001, η2 = 0.28), with females reporting higher exposure compared to males. Additionally, a significant group by gender interaction was found for the total number of potentially traumatic events (F(1,45) = 9.05, p < 0.01, η2 = 0.17). While the difference between females with ASD and typical females was significant (i-j = 7.70, SE = 1.91, p < 0.001), the difference between males with ASD and typical males was not (i-j = 0.66, SE = 1.49, p = 0.66). A significant interaction was also found regarding the number of negative social events (F(1,45) = 7.95, p < 0.01, η2 = 0.15). While the difference between females with ASD and typical females was significant (i-j = 7.21, SE = 1.43, p < 0.001), the difference between males with ASD and typical males was only marginally significant (i-j = 2.25, SE = 1.12, p = 0.051). Finally, a marginally significant interaction was found regarding the number of PTSD criterion A events (F(1,45) = 3.18, p = 0.08, η2 = 0.07). While the difference between females with ASD and typical females was not significant (i-j = 0.49, SE = 0.95, p = 0.61), the difference between males with ASD and typical males was significant (i-j = 1.60, SE = 0.74, p < 0.05). The effects of exposure to potentially traumatic life events are illustrated in Figures 2 and 3.
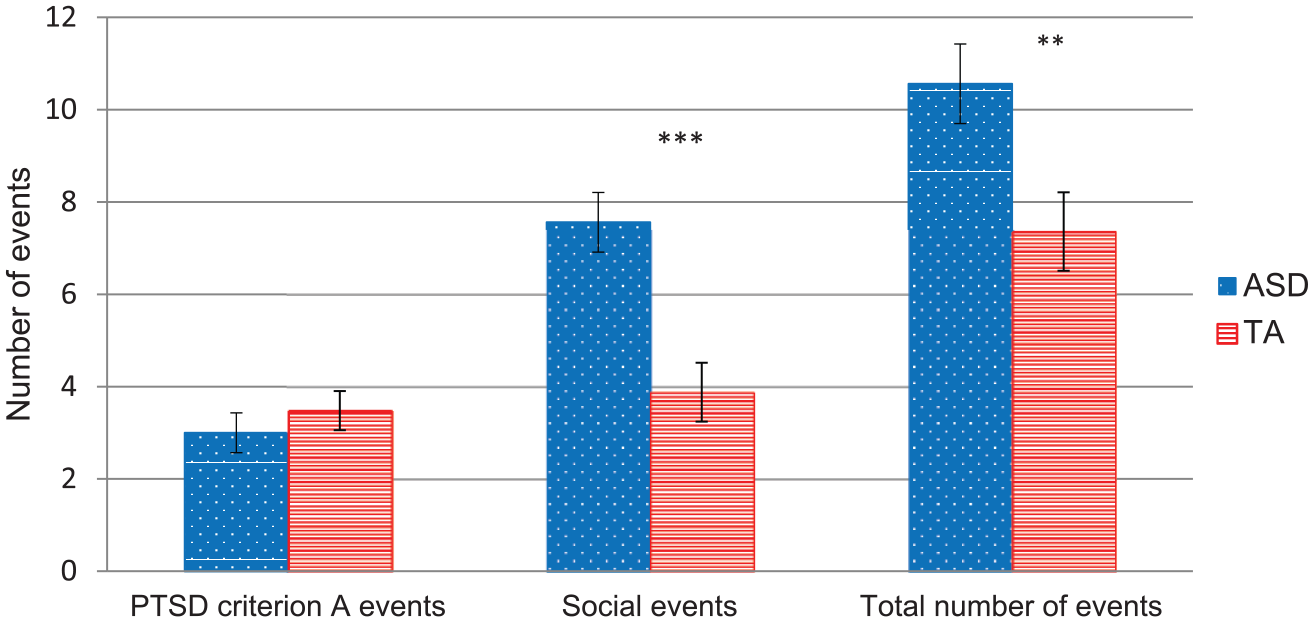
Group differences in exposure to potentially traumatic life events.

Group × gender interaction regarding exposure to negative social events.
Finally, we examined which types of events were associated with PTSS in the ASD and TA groups. Thus, Pearson correlations were calculated in order to examine the association between PTSS and potentially traumatic exposure. As can be seen in Table 4, a significant positive association between PTSS and number of negative social events was found in the ASD group, but not in the TA group. In contrast, a significant positive association was found between PTSS and PTSD criterion A events among the TA group, but not in the ASD group. Looking at the PCL symptom clusters, the ASD group showed significant positive associations only for hyper-arousal symptoms with negative social events, and with total number of negative life events. In the TA group, significant associations were found between all symptom clusters and PTSD criterion A events, but no correlation was found for negative social events in this group.
Pearson correlations between number of potentially traumatic events and PCL scores.
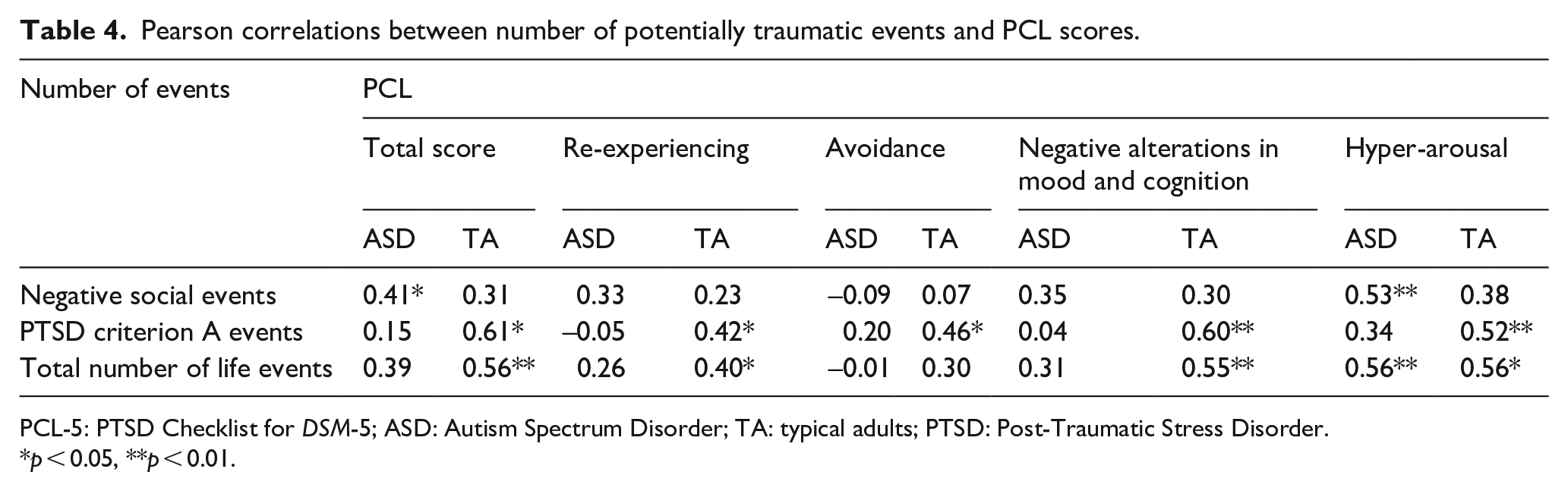
PCL-5: PTSD Checklist for DSM-5; ASD: Autism Spectrum Disorder; TA: typical adults; PTSD: Post-Traumatic Stress Disorder.
p < 0.05, **p < 0.01.
Finally, 60% (n = 15) of participants with ASD chose a negative social event as the event that caused them the most significant distress, compared with only 20% (n = 5) of typical participants (χ2(1) = 8.33, p < 0.01). The events most frequently chosen by ASD participants as the most distressing were shunning, followed by physical, and verbal violence. In the TA group, combat and exposure to terror were the events most commonly chosen as most distressing.
Discussion
This is one of very few studies to have examined PTSS levels in adults with ASD. So far, ASD-PTSD co-occurrence has received little empirical attention. Our analysis reveals the increased vulnerability of adults with ASD(with no intellectual impairment) to trauma and probable PTSD, and the role of gender as a moderator of the PTSS levels in adults with ASD. The results suggest that females with ASD are at a greater risk for exposure to potentially traumatic events and for manifestation of PTSS. Perhaps most importantly, our findings indicate that the social sphere in particular may be potentially traumatic for individuals with ASD, especially for females. In addition, we found that individuals with ASD and probable PTSD co-occurrence present a more severe clinical picture, compared with those endorsing ASD alone.
Our main finding revealed that individuals with ASD reported significantly higher levels of PTSS, compared with typical participants. Looking at the four PCL symptom clusters, individuals with ASD reported higher levels of re-experiencing and hyper-arousal symptoms, as well as marginally significant higher levels of negative alterations in mood and cognition. These findings are in line with a previous study, which examined the association of PTSS and AT in a typical adult sample, revealing that those with the highest level of AT reported higher levels of PTSS, particularly from the hyper-arousal cluster, compared with those with lower AT (Haruvi-Lamdan et al., 2019).
One explanation for ASD and probable PTSD co-occurrence shown here may be that ASD serves as a vulnerability factor for PTSD. Hirvikoski and Blomqvist (2015) found that adults with ASD reported significantly higher subjective stress and poorer ability to cope with stress in everyday life, compared with typical adults. One’s subjective perception of his or her ability to cope with a specific stressor is central in defining the level of experienced distress (Karasek & Theorell, 1990). Individuals with ASD often show executive functioning difficulties (Kenworthy et al., 2008), which may impede their choice of appropriate coping strategies. Another aspect related to ASD that may affect individuals’ subjective distress level following trauma is sensory hypersensitivity (e.g. Horder et al., 2014), a factor that has been associated with vulnerability to PTSD (Engel-Yeger et al., 2013). In addition, communication difficulties and impaired social skills may get in the way of reporting traumatic experiences and seeking help or treatment (Cook et al., 1993). It is also possible that individuals with ASD receive less social support, which is known as a major protective factor in the face of trauma (Wright et al., 2013). Importantly, ASD-PTSD co-occurrence could be attributed to potential shared vulnerability mechanisms for both disorders, including emotion regulation deficits, increased rumination, difficulties in autobiographical memory, and impaired social cognition (Haruvi-Lamdan et al., 2018). This possibility of shared mechanisms calls for future research.
Previous studies have shown mixed findings regarding the specific symptoms characterizing individuals with ASD following trauma. In their review article, Kildahl and colleagues (2019) have shown that on the majority of studies examining response to traumatic events among individuals with ASD and intellectual disability parents reported symptoms of hyper-arousal and negative alterations in mood and cognition following traumatic experiences. These symptoms were relatively more easily identified, as opposed to intrusive memories and re-experiencing symptoms, which cannot be fully captured using parental report. The few case studies that described re-experiencing symptoms involved individuals with intact verbal abilities. Therefore, they emphasized the importance of self-report measures that may capture the subjective experience and symptomatology among traumatized individuals with ASD. In addition, previous studies have shown that children with ASD who experienced frequent peer victimization reported increased arousal levels, including a stronger tendency for anxiety, anger, hyper-sensitivity, self-injury, stereotypic behavior, and hyperactivity (Bitsika & Sharpley, 2014; Cappadocia et al., 2012). Looking at the group differences in specific PTSS clusters, our results reveal the central role of hyper-arousal and re-experiencing symptoms. The hyper-arousal cluster includes several symptoms which may be considered “non-specific” to PTSD, including sleep impairments, difficulty concentrating, agitation, and anger. This non-specific nature may account for this cluster’s association with other disorders co-occurring with PTSD (Horesh et al., 2017). It is also possible that, at least in part, hyper-arousal is also related to underlying symptoms of anxiety, which have been found to be elevated among those with ASD (Zaboski & Storch, 2018). While we did not specifically assess anxiety in this study, this is a possible explanation. In addition, individuals with ASD have been shown to experience sensory hyper-sensitivity, which in turn may cause them to feel more agitated, hypervigilant, and generally aroused (Green & Ben-Sasson, 2010). As for re-experiencing, individuals with ASD were found to report high levels of rumination and intrusive thoughts (Carne et al., 2013; Gotham et al., 2014). This tendency to “rehash” mental and emotional content is at the core of the re-experiencing cluster, and characterizes post-traumatic intrusions (e.g. constant reminders of the trauma, flashbacks). Future qualitative inquiries may examine whether the symptom clusters highlighted in our study fully capture the nature of the post-traumatic experience in adults with ASD. Notably, there is also the possibility of the increased hyper-arousal symptoms resulting from an overlap between ASD symptoms and PTSS, that is, that some similarities between symptoms that are characteristic of both conditions may inflate the level of PTSS reported by individuals with ASD. However, symptom overlap is unlikely to explain the elevated re-experiencing PTSS found in the current study.
In our sample, females with ASD reported marginally significant higher levels of PTSS in general, and significantly higher levels of hyper-arousal symptoms, compared with typical females. This difference was not found among males. A possible explanation for this finding may be that the gender difference in PTSD rates in the general population becomes even more profound among individuals with ASD. As noted, in the general population females face a lifetime risk for PTSD that is twice as high as males (Yehuda et al., 2015). Although gender differences in PTSS among individuals with ASD were hardly ever studied before, one study did show that females who experienced victimization and/or bullying reported more symptoms of anxiety compared with males (Bouman et al., 2012). Our findings regarding PTSS gender differences are particularly concerning considering the high prevalence of suicidal thoughts and behaviors among individuals with ASD (Kirby et al., 2019), as well as among women belonging to traumatized or abused minorities in society (Basile et al., 2016). In fact, women with ASD were found to face a particularly high risk of dying by suicide (Hirvikoski et al., 2016). Thus, traumatized women with ASD may represent a particularly high-risk group, which possibly requires special attention and treatment. Clearly, more studies are needed in order to elucidate PTSD gender differences among individuals with ASD. We believe such an examination is of particular importance in this era of personalized medicine.
Increased risk for traumatic exposure among individuals with ASD may also serve as a vulnerability factor for PTSD (Haruvi-Lamdan et al., 2018). Indeed, our findings indicate that individuals with ASD were significantly more exposed to potentially traumatic life events compared with typical adults. In particular, participants with ASD were more exposed to negative social events (e.g. bullying, ostracism), while regarding PTSD criterion A events there was no group difference. Moreover, in our sample, lifetime exposure to negative social events was related to PTSS in the ASD group, but not in the TA group. In contrast, lifetime exposure to criterion A events was related to PTSS among the TA group, but not the ASD group. In addition, our results revealed that individuals with ASD showed a higher tendency to choose negative social events as their most distressing experience, compared with typical adults. This emphasizes the centrality of social stressors for individuals with ASD, compared with events that are more commonly studied in trauma research. In this study, we included a wide range of negative interpersonal experiences, from bullying, verbal insults, humiliations, and social exclusion, to physical violence. These situations appear to be perceived as more traumatic for individuals with ASD than for their typical peers. The PTSD cognitive model by Ehlers and Clark (2000) emphasizes the importance of the victim’s subjective perception on the development and persistence of PTSD. The social communication difficulties experienced by individuals with ASD may affect the interpretations and meaning they assign to different situations. It is possible that they encounter a social environment that is less accepting, and potentially more aggressive toward them (White et al., 2016). Moreover, at least for some individuals with ASD, being aware of the difference between themselves and their typical peers, as well as the way they are viewed by the latter, may be a source of significant stress. The fact that individuals may be differentially vulnerable to certain types of events is of key importance when attempting to understand the huge variability in PTSD manifestation (Galatzer-Levy & Bryant, 2013). For those with ASD, negative events occurring within the social realm seem to exert a unique influence in terms of PTSS.
Importantly, our findings may indicate that for individuals with ASD, negative social events exert a cumulative effect, as they are often experienced in a chronic, continuous fashion. Spence and colleagues (2019) suggested that for many individuals the traumatic event occurs within the context of other negative experiences, and that one’s emotional distress should be understood in light of this broader set of events. This claim seems particularly relevant when it comes to ASD, as traumatic social events often occur as part of ongoing, stress-inducing, interpersonal difficulties. For example, bullying experiences are often recurrent, and tend to afflict socially vulnerable individuals more than once (Sourander et al., 2010). Repeated and chronic traumatic events have been shown to exert a powerful impact on one’s interpersonal relationships and core beliefs about the self and the world. Thus, it is quite possible that traumatized individuals with ASD in fact experience chronic, complex trauma, as opposed to single events, thereby yielding a broader, more severe clinical picture more akin to complex PTSD (CPTSD; Brewin et al., 2017; Herman, 1992). To the best of our knowledge, CPTSD has yet to be studied among adults with ASD (Taylor & Gotham, 2016), and further studies in this area are needed.
In addition, we have shown a gender by group interaction regarding trauma exposure. Our findings indicate that females (but not males) with ASD face an increased risk of experiencing potentially traumatic events compared with typical females. One explanation for this finding may be that the ASD diagnosis for females usually occurs later in life, compared with males. This may expose females to a longer period of being misunderstood and potentially mistreated not only by their peers but also by authority figures such as teachers or employers, with little appropriate support. Furthermore, in recent years, findings about the tendency of females with ASD to camouflage their characteristics (e.g. Dean et al., 2017) suggest that females may be exposed to traumatic experiences in the social realm, without being properly noticed and supported. Camouflaging in females with ASD has been shown to associate with more anxiety and depression (Bargiela et al., 2016; Lai et al., 2011). Future studies should examine if part of this clinical picture also includes PTSD.
The final aim of this study was to examine whether ASD-probable PTSD co-occurrence entails higher symptom severity. We have found that, compared with individuals diagnosed only with ASD, those with ASD and probable-PTSD report greater deficits in social skills. This is in line with previous studies, showing that having two or more diagnoses was associated with worse functioning, specifically social functioning: Chiang and Gau (2016) found among youth with ASD that co-occurring psychiatric conditions (e.g. anxiety, depression) mediated the association between autistic symptoms severity and social dysfunction. Zukerman and colleagues (2019) found that adaptive behavior (e.g. social skills and communication) were negatively correlated with social anxiety and OCD symptoms among students with ASD. In contrast, Kerns et al. (2015) have found that youth with co-occurring ASD and anxiety disorders had better parent-reported functional communication than youth with ASD alone. Therefore, further research is required. As for PTSD, previous studies have similarly shown that the disorder’s severity was associated with the existence of co-occurring conditions, including depression and substance abuse (e.g. Shah et al., 2012). To the best of our knowledge, this is the first study to examine ASD-PTSD co-occurrence in this context. Our results provide preliminary evidence that ASD and probable-PTSD co-occurrence exacerbates at least some symptoms of ASD. Due to the small number of individuals meeting the cutoff for probable PTSD in our sample, we were unable to examine this question for PTSS severity as well. Thus, further studies are needed in this area, based on larger samples.
It is important to remember, however, that participants were labeled with a probable PTSD diagnosis based on their self-report on the PCL. Whereas these reports may indeed represent a co-occurrence of both conditions, reliance on self-report measures that have not been adapted for the use of individuals with ASD may bias our results in different ways: on one hand, they may be insufficiently sensitive to the unique symptoms or the different manifestation of symptoms following trauma among individuals with ASD. On the other hand, such measures may overpathologize individuals with ASD given that some symptoms of ASD and related co-occurring conditions (e.g. anxiety, depression) could resemble and elevate scores on a PTSD measure erroneously (Cassidy et al., 2018). Hence, a clinical assessment for PTSD among participants with ASD may be warranted. Noteworthy, even with a clinical evaluation in place, the differential diagnosis between autistic and post-traumatic symptoms may be complicated, especially with regard to socio-emotional functioning and sensory experiences (Stavropoulos et al., 2018). Therefore, the diagnosis of PTSD among individuals with ASD calls for the establishment of clear clinical guidelines.
This study is limited by its focus on adults with ASD and no intellectual or verbal impairments. Therefore, the generalization of findings to the wider autistic spectrum may be limited. Our study was also based on a cross-sectional design, thus excluding the possibility of establishing causal relationships between assessed factors. It is therefore possible that some of the social difficulties attributed to the ASD phenotype were actually PTSS. We recommend that future studies employ prospective, longitudinal designs, in order to more accurately assess the temporal relationships between specific events and their post-traumatic implications among individuals with ASD. Finally, our sample size was quite modest, and thus statistical power was sometimes insufficient to conduct certain analyses. This was especially apparent when examining the probable PTSD diagnosis, as only few participants passed the PCL threshold.
Nonetheless, this study is novel and important in several ways. Studies examining PTSD among adults with ASD are very rare. These individuals are trying to integrate and function in society, but often face significant challenges and hardships. Future studies are encouraged to examine exposure to potentially traumatic events and PTSD in different contexts, as well as among individuals with ASD in different age groups, developmental and intellectual levels. Our findings indicate that there are potentially traumatic events, most notably negative social events, that are not included in standard trauma measures, and are central in the experience of individuals with ASD. Therefore, further research is needed to create and validate measures of trauma exposure, PTSD, and complex PTSD among children and adults with ASD. These measures should also be sensitive to gender differences in symptom manifestation and trauma exposure. These methodological complexities attest to the fact that the vast majority of trauma studies to date have been conducted among typical individuals, thus neglecting a wide variety of populations that may experience trauma differently and carry unique post-traumatic scars. Finally, following the improved identification of trauma and PTSD among males and females with ASD, future studies should focus on developing novel interventions for treating trauma-exposed clients with ASD, and assessing their effectiveness. While evidence-based psychotherapy has massively developed for PTSD and ASD separately, we currently know only of case studies describing psychotherapy for individuals who have co-occurring ASD and PTSD (Rumball, 2018).
We conclude that individuals with ASD show increased vulnerability to trauma and enhanced PTSS, particularly due to social stressors; that females with ASD may be at an increased risk for trauma, and that adults with ASD may show a unique profile of PTSS. This study is preliminary in nature, as it is based on a small sample, using self-report measures. Its novel findings should be taken as a first step in this under-explored area. There is a pressing need for future research based on larger samples and more complex methodologies and study designs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All participants were informed about the study and provided written informed consent before the study. The study was approved by the Institutional Review Board of Bar-Ilan University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Parts of this study were supported by a grant from the Autism Treatment and Research Center, The Association for Children and Risk, Israel.