
Abstract
The objective of this study is to evaluate the effectiveness of a multi-component communication intervention on social communication for young children with autism. As many as half of children with autism are not yet talking by age 3, and up to a third of children with autism will remain minimally verbal past age 5. Spoken language outcomes are greatest when parents and clinicians are delivering language interventions to children with autism as compared to parents or clinicians alone. This study incorporates caregiver training, Discrete Trial Teaching, and JASP + EMT + SGD. A total of 68 children between ages 3 and 5 with autism, and their caregivers, participated in this study. Children were randomly assigned to the treatment or control group. Children in the treatment group received 36 sessions of the multi-component intervention in the clinic and at home. Children in both groups received a speech-generating device and the caregivers received an individualized training on how to program the speech-generating device. All participants were evaluated prior to intervention, immediately following intervention, and 4 months following intervention. Children in the intervention group demonstrated significantly greater joint attention than those in the control group immediately following intervention. Children in the intervention group, additionally, demonstrated greater social communication with their caregivers 4 months following intervention. This brief, multi-component intervention may be effective for improving social communication in young children with autism who are at risk for remaining minimally verbal. Future research is needed to understand for whom and under what conditions this intervention is most effective.
Lay abstract
This study reports the results of a randomized trial for preverbal preschoolers with autism that demonstrates the effects of multiple intervention strategies including caregiver training. About 50% of children with autism are not talking by age 3 and up to 30% of children with autism will remain minimally verbal past age 5. Interventions delivered by clinicians and caregivers have the greatest effects on spoken language and may reduce the rate of those who remain minimally verbal. Sixty-eight children ages 3–5 with autism and their caregivers participated in this randomized trial comparing the communication intervention to a comparison group. A brief, multi-component, communication intervention (including a speech-generating device) for children with autism that addresses core deficits may be effective in improving joint attention skills immediately following intervention and social communication skills 4 months following intervention. Future research is needed to understand for whom and under what conditions this intervention is most effective.
Keywords
Children with autism under the age of 8 demonstrate better spoken language outcomes and social communication outcomes after having early interventions that include both direct treatment from a clinician and caregiver-implemented components (Fuller & Kaiser, 2019; Hampton & Kaiser, 2016). At 33 months, about half of children with autism do not yet have meaningful speech (Eaves & Ho, 2004). Although many of these children go on to develop phrase speech, and thus would be classified as preverbal at this age, a third of children with autism remain persistently minimally verbal at age 5 despite early intervention (Tager-Flusberg & Kasari, 2013). Interventions that target spoken language during this transitional stage (ages 3–4) may be critical in reducing the percentage of children who remain minimally verbal at age 5 and beyond.
Two evidence-based early interventions that include clinician-implemented components, and often include parent-implemented components, have demonstrated improvements in social communication and language for minimally verbal and preverbal children with autism: Discrete Trial Teaching (DTT; C. Smith et al., 2004; T. Smith, 2001) and JASP + EMT, an intervention that incorporates components from the Joint Attention, Structured Play, Engagement, and Regulation (JASPER; Kasari et al., 2006) intervention and Enhanced Milieu Teaching (EMT; Kaiser & Hampton, 2017). DTT provides children with massed systematic instructional trials in a structured context to teach a variety of skills related to communication and development. JASP + EMT is a play-based intervention that includes responsiveness, play and language modeling, play and language expansions, modeling and encouraging joint attention, and eliciting new communication through time delays and prompting episodes (see Supplemental Material 1). JASP + EMT is a type of Naturalistic Developmental Behavioral Intervention, which has been shown to result in the generalized use of language and communication skills, fewer behavior problems, more spontaneous initiations of communication (Sandbank et al., 2020; Schreibman et al., 2015), and greater spoken language when verbal input is paired with a speech-generating device (SGD; Kasari et al., 2014).
Although interventions using alternative and augmented communication systems are common components of communication interventions for children with autism, a recent systematic review identified a gap in the research when using these communication systems beyond simple requests (Logan et al., 2017). In addition, some studies that do teach broader communication functions with an SGD notably do not report the maintenance of social communication skills achieved in the study. JASP + EMT + SGD (JASP + EMT with SGD modeling) has been shown to result in improvements in spoken language for older children with autism (ages 5–8) who were minimally verbal (Kasari et al., 2014). Despite overall improvements for the group receiving this intervention, about 25% of participants did not make progress during the first 12 weeks of treatment, suggesting that additional forms of instruction might be needed for some children to benefit.
Some children with autism may benefit less than others from naturalistic interventions such as JASP + EMT + SGD due to poor imitation skills, low receptive language, or unfamiliarity with an SGD (Carpenter et al., 2002; Charman et al., 2003; Dawson et al., 2004; Mundy et al., 1987; Stone & Yoder, 2001; Toth et al., 2006; Weismer et al., 2010; Yoder & Stone, 2006). Given that DTT has been found effective for improving these critical precursors to language in preverbal children with autism (Lovaas, 1987; Paul et al., 2013; Reichow & Wolery, 2009; Smith, 2001), including direct instruction on precursor skills with a naturalistic intervention approach could result in better outcomes (Kasari et al., 2006), especially for this population with severe delays in developing spoken language.
This randomized clinical trial examined the effects of a multi-component communication intervention composed of (1) JASP + EMT + SGD, (2) DTT, and (3) caregiver training for preschoolers with autism between preverbal and first words of language development. The following research questions were addressed: (1) Does a short-term multi-component communication intervention improve social communication for preverbal children with autism? (2) Do outcomes maintain 4 months following intervention? (3) Does caregiver training improve caregivers’ use of language facilitation strategies?
Methods
Trial design
This project was a randomized controlled trial (R40MC27707) of a communication intervention for young children with autism with preverbal or first word language development (Tager-Flusberg et al., 2009). Participants were recruited in Nashville, TN from early intervention programs, preschools, and outpatient clinics between January 2014 and July 2017. The trial was approved by Vanderbilt University’s Institutional Review Board (#141453) and all caregivers provided informed consent.
Participants
The child inclusion criteria were as follows: (1) chronological age between 36 and 60 months; (2) confirmed autism diagnosis on the Autism Diagnostic Observation Schedule—Second Edition, Module 1 (ADOS-2; Lord et al., 2012); (3) a visual reception score greater than 18 months (Mullen, 1997); (4) fewer than 20 different spontaneous words during a 20-min language sample (consistent with previous studies; Kasari et al., 2014); (5) no indicated secondary diagnosis; and (6) the primary caregiver spoke mostly in English at home to the child. Eighty-four children were screened (Figure 1). Children’s participation in outside services was not specified for inclusion in the study, but was monitored at all timepoints. The participating children received outside services ranging from 0 to 38 h per week. Children in both groups received speech/language and behavioral services, and no significant differences in hours per week of intervention were observed between groups (Table 1). Sixty-eight children and their caregivers were randomized to treatment (34) or comparison (34) and included in the analysis (Figure 1). Five children were originally randomized but dropped from participation prior to being informed of their randomization assignment, and hence they were not included in the data analysis due to failure to complete sufficient pre-intervention assessments for analysis. Seven participants (two in the intervention group and five in the comparison group) withdrew from the study prior to post-intervention assessment; three additional participants from the comparison group withdrew prior to the follow-up. These 10 participants were included in the analysis. Caregivers were mothers (n = 57), fathers (n = 8), and grandmothers (n = 3).
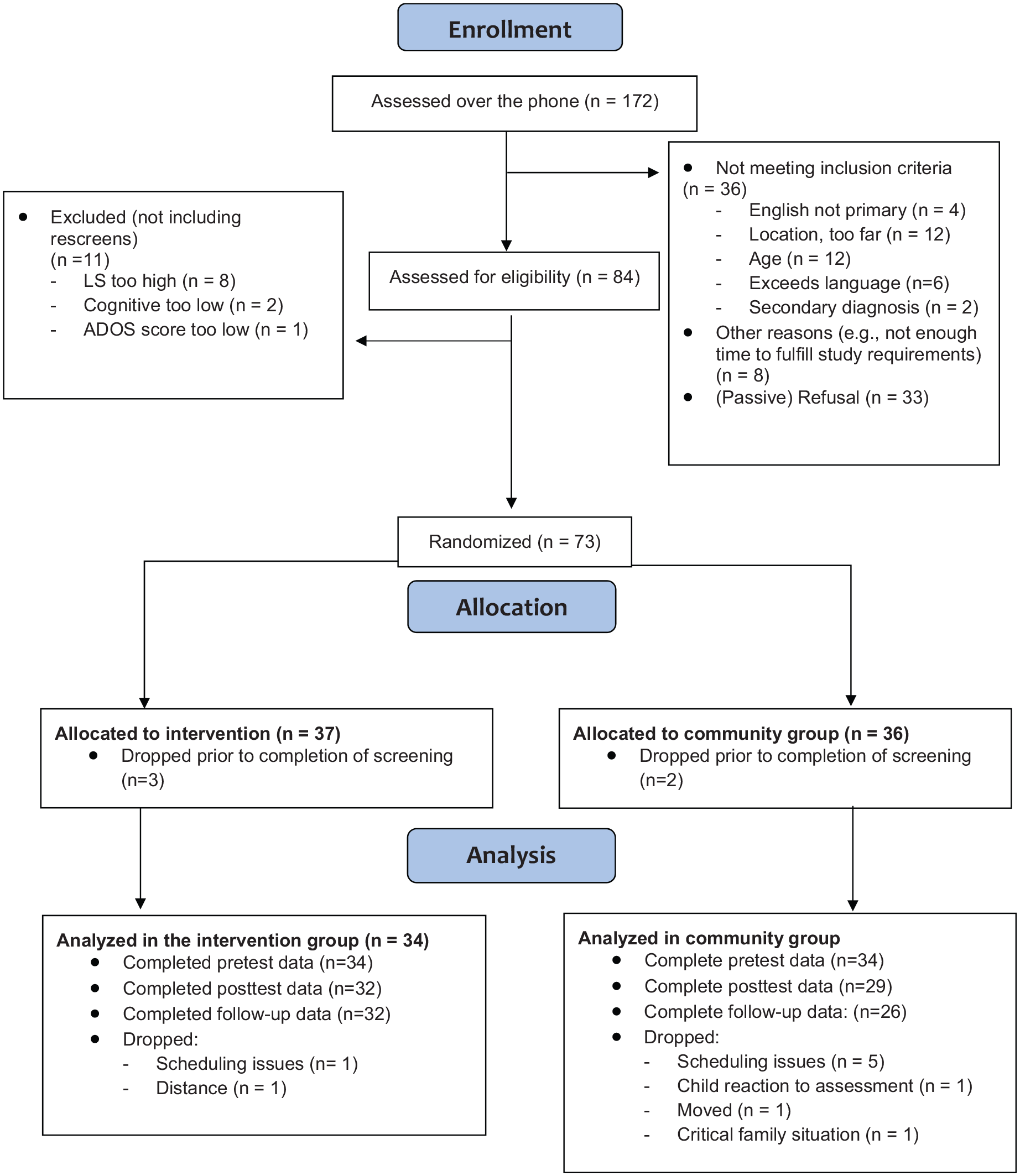
CONSORT diagram.
Child characteristics.

SD: standard deviation; ADOS-2: Autism Diagnostic Observation Schedule—Second Edition.
Cognitive scores were measured from the visual reception subscale of Mullen Scales of Early Learning (Mullen, 1997), and autism severity was measured from ADOS-2, Module 1 (Lord et al., 2012). Low income was defined as a household income falling below 200% of the income-to-needs ratio specified by the Federal Poverty Line during the year of entry into the study. p values were calculated using t tests for continuous variables and chi-square tests for categorical variables. There were no significant differences between groups on any baseline variables.
Randomization
Following initial screening, the participants were randomized to the intervention or the comparison group using the REDcap randomization tool (Harris et al., 2009); all research personnel were blind to the allocation process.
SGD
Participants in both the intervention and comparison groups received an iPad with the Proloquo2Go™ app (AssistiveWare®, 2010) to use throughout the 8-month study participation period. A project staff member provided caregivers with training (45 min) on programming, how to use the device for communication, and setting up activity pages for the child in daily routines. Caregivers were encouraged to use the device across daily activities, model language on the device, and include the device in other therapies/services.
During the initial assessment, the participants completed a short task, “chase the ball,” to identify the best grid size for displaying communication symbols on the SGD. The task for the child was to touch the ball in the display presented on the grid. The grid started in a 2 × 2 layout displaying four basic line drawings of common objects including the red ball. After each trial, the ball changed locations. After every 3–4 trials, the grid size increased until the child was presented with a 5 × 5 grid. Based on the child’s performance, the project staff recommended the grid size in which the child was able to find the ball in the majority of configurations. If the child was unsuccessful in “chasing the ball” across three teaching trials, the 2 × 2 layout was recommended for initial programming.
The Proloquo2Go™ app was used under a custom setting. This was selected to ensure systematic individualization across participants. In the most common configuration (5 × 5), each participant was given a core set of words along the bottom row. These words could be applied to most settings (e.g. “all done,” “more,” “stop,” or “help”). The caregiver and therapist selected these words together. Activity-specific pages were created for at least five common family routines with types of vocabulary presented from left to right to encourage early word combinations: pronouns, verbs, adjectives, and nouns. These basic configurations were adjusted for different grid sizes as appropriate. Example pages are available in Supplemental Material 2.
Comparison group
Participants assigned to the comparison group were referred to community-based services for children with autism. Parents in the comparison group were not instructed on the use of the JASP + EMT or DTT procedures, or how to specifically integrate the SGD into play interactions with their children. Check-ins occurred every 8 weeks to update the SGD software. Participants were offered opportunities to access the experimental intervention following the completion of follow-up testing (this intervention was not available in the community setting).
Intervention group
The children and caregivers assigned to the intervention received three intervention sessions (two clinic and one home) per week for 36 sessions (45–60 min per session) within a 4-month period and three total caregiver intervention workshops. The multi-component adaptive intervention included (1) therapist-implemented DTT with the child to teach foundational skills, including the use of the SGD in the clinic only; (2) therapist-implemented JASP + EMT + SGD during play and routines with the child in the clinic and at home; and (3) caregiver training to implement JASP + EMT + SGD in the clinic and at home (Figure 2). Overall, the intervention was adaptive to individual parent and child performance such that the caregiver practice time was increased in proportion to their skill fluency, parent workshops were introduced as the caregiver mastered communication support strategies, and child DTT was decreased as the child mastered key foundational skills. Therapists were master’s level clinicians who had previously met fidelity criteria for all of the individual components of the intervention. The same therapist implemented all intervention components for a given family.
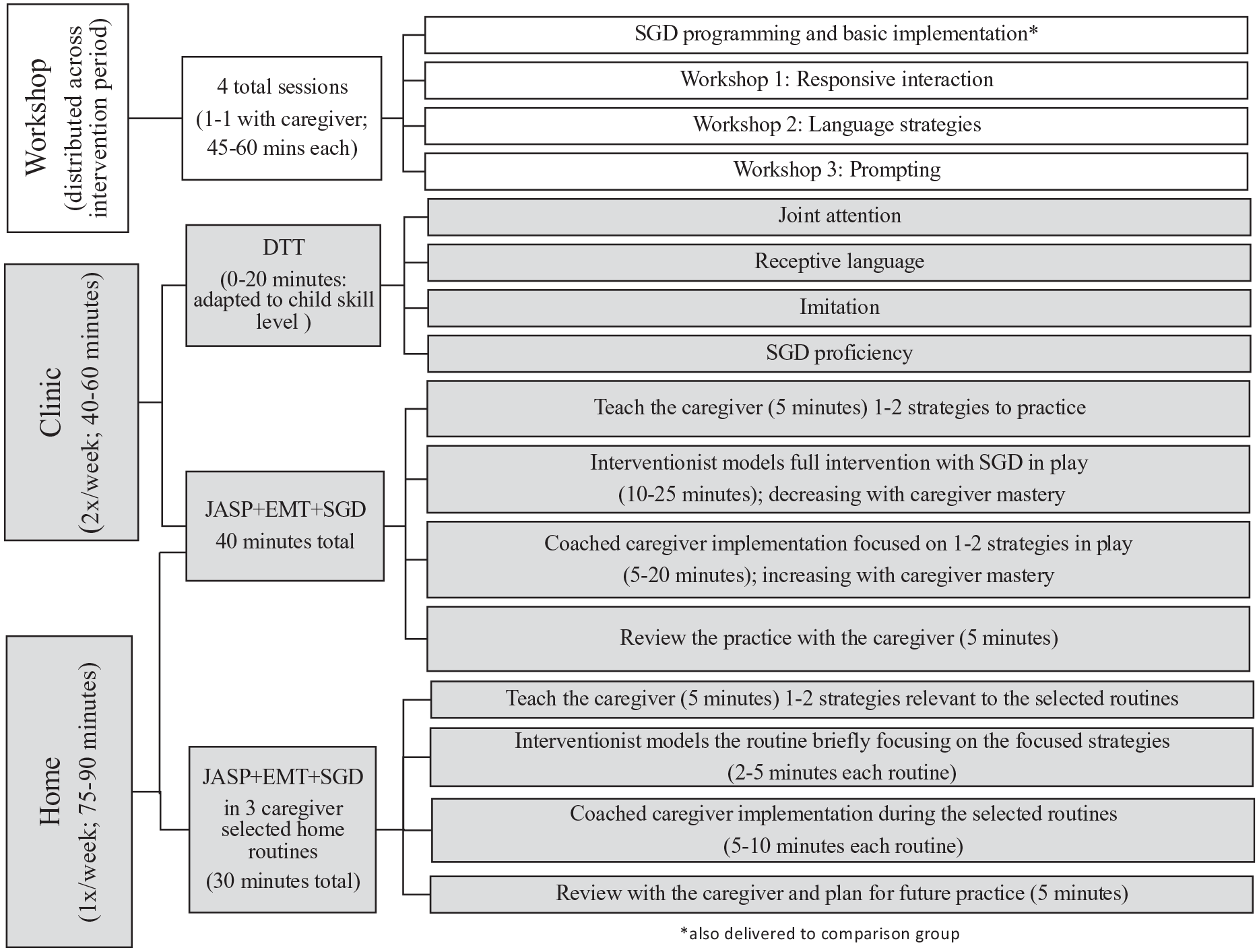
Multicomponent communication intervention components.
DTT
Each clinic-based session (24 sessions) included up to 20 min of therapist-implemented DTT (Eikeseth et al., 2002). This focused DTT instruction was designed to pre-teach the key skills that would also be modeled and used the JASP + EMT + SGD portion of the session, similar to previous applications of the JASPER intervention (Kasari et al., 2006). Based on their performance during DTT baseline assessments (Supplemental Material 3), the child participants received instructions on (1) joint attention, (2) imitation, (3) receptive language, and (4) matching and basic requesting skills using the SGD. Instruction in each program lasted 5 min per session. The four programs used direct instruction to teach skills foundational to learning social communication that could potentially maximize benefits of the JASP + EMT + SGD intervention and provided children with targeted practice in skill areas in which they demonstrated specific deficits. When a child demonstrated criterion levels of performance for all skills in an individual program (80% correct over two consecutive sessions), that program was dropped from the intervention sessions, resulting in a 5-min reduction in overall session length.
JASP + EMT + SGD
The primary component of the intervention was a naturalistic communication intervention: JASP + EMT + SGD implemented by therapists and caregivers described by Kasari et al. (2014). Each child received 30 min of play-based JASP + EMT + SGD during each session (home and clinic). Play and language targets were selected based on initial assessments. Throughout the intervention, the therapist and the caregiver used the SGD to model communication and to provide the child with a nonverbal response mode.
Caregiver training
The strategies used in the JASP + EMT + SGD intervention were introduced to the caregiver during three didactic workshops; workshops occurred before the first intervention session, between sessions 12 and 18, and between sessions 24 and 30. Workshops were individual sessions with the therapist and the caregiver held in addition to the regularly scheduled sessions. The timing of workshops was based on the individual caregiver’s mastery of the intervention strategies, consistent with procedures in prior studies using the Teach-Model-Coach-Review (TMCR) approach (Hampton et al., 2017; Kaiser et al., 2016; Roberts et al., 2014; Roberts & Kaiser, 2012, 2015). Workshops included a rationale for each strategy, video examples of the therapist or caregiver using the strategy with the child, role-playing, discussion of adaptations for the child’s skill level and interests, and opportunities for the caregiver to ask questions.
During each intervention session with the child and the caregiver, the TMCR framework was used (Kaiser et al., 2016; Roberts et al., 2014). The therapist began each session by reviewing two specific JASP + EMT + SGD strategies. The therapist then modeled these strategies with the child. The therapist verbally highlighted her use of the strategies at least twice for each strategy. The caregiver then practiced the strategies with the child and received coaching from the therapist (e.g. the therapist made suggestions for engagement and play and handed the parent play materials, praised the caregiver’s use of specific strategies, prompted the caregiver to use a strategy, and provided limited corrective feedback). The therapist ended the session by reviewing and linking the caregiver’s use of specific JASP + EMT + SGD strategies to the child’s play and communication.
The amount of time the caregiver practiced the intervention strategies with the child systematically increased across the 36 sessions, from 5 min at the beginning of treatment to 20 min at the end. The combined time for therapist-plus-caregiver implementation of JASP + EMT + SGD in each session was 30 min; thus, the amount of therapist-provided direct intervention to the child decreased from 25 to 10 min across the 36 sessions.
Each home session (12 total sessions) included play with toys and two additional home routines, selected by the family, in which the caregiver practiced the use of JASP + EMT + SGD strategies. Typical routines selected by the caregiver included mealtime, hand washing, outdoor play, bath time, dressing, and book reading. Each routine lasted 5–20 min; caregiver training followed the TMCR framework described above. Typically, the therapist modeled the routine the first one or two times the routine was implemented; thereafter, the caregiver practiced the routine and the therapist provided coaching and feedback to support the caregiver. Over the 12 home sessions, the family was encouraged to select different routines such that by the end of the intervention at least six different caregiving routines were practiced.
Fidelity
Fidelity of intervention was measured from video recordings for 17% (210) intervention sessions. Four clinic and two home sessions for each family were randomly selected from their 36 intervention sessions. Fidelity assessments were completed for all components of the intervention (JASP + EMT + SGD, Kasari et al., 2014; DTT, Eikeseth et al., 2002; and caregiver training, Roberts et al., 2014) using a checklist (see Supplemental Material 1) and reviewed on a continuous basis. Overall fidelity for therapist implementation of the JASP + EMT + SGD component was 89.45% (standard deviation (SD) = 4.27), for the DTT component it was 96.62% (SD = 9.93), and for the caregiver training component it was 86.31% (SD = 9.49).
Measures
All assessments were completed by an assessor blind to group assignment in a small clinic room in a different location than the intervention. Following the screening assessment, the full battery of initial assessments was administered over 2 days within a 2-week period. Post-intervention assessments were completed approximately 4 months after the pre-intervention and follow-up assessments were completed 4 months after the post-intervention assessment. Fidelity of assessment administration was measured for 20% of the nonstandardized assessments and averaged 95.28% (range: 80%–100%) across measures.
Naturalistic language sample
Naturalistic language sample (NLS) was a 20-min interaction between the child and an assessor using six novel toy sets. The NLS provided a generalized measure of social communication by observing children in a novel context with novel materials and with an adult who did not use JASP + EMT + SGD strategies. The video-recorded NLS was transcribed and coded for social communicative utterances (SCU), by coders blind to random assignment, using the Systematic Analysis of Language Transcripts (SALT) software (Miller & Chapman, 2008). Each SCU was defined as spoken, SGD, or gestural requests and comments that included a secondary indicator (pointing, showing, giving, eye contact) that confirmed the social intention of the utterance.
Caregiver–child interaction
Similar to the NLS, a 10-min caregiver–child interaction (CCX) including a different standard set of novel toys, was video-recorded, transcribed, and coded for SCU. Similar to the NLS, coders were blind to random assignment. The CCX provided a proximal measure of social communication by observing the caregiver and child in a novel setting with novel materials. The caregiver use of the JASP + EMT + SGD strategies was measured during the 10-min CCX at each major assessment point. Caregiver utterances were transcribed and coded for the use of JASP + EMT + SGD strategies as defined in Table 2.
JASP + EMT + SGD strategies and the corresponding workshops when strategies were taught to caregivers.
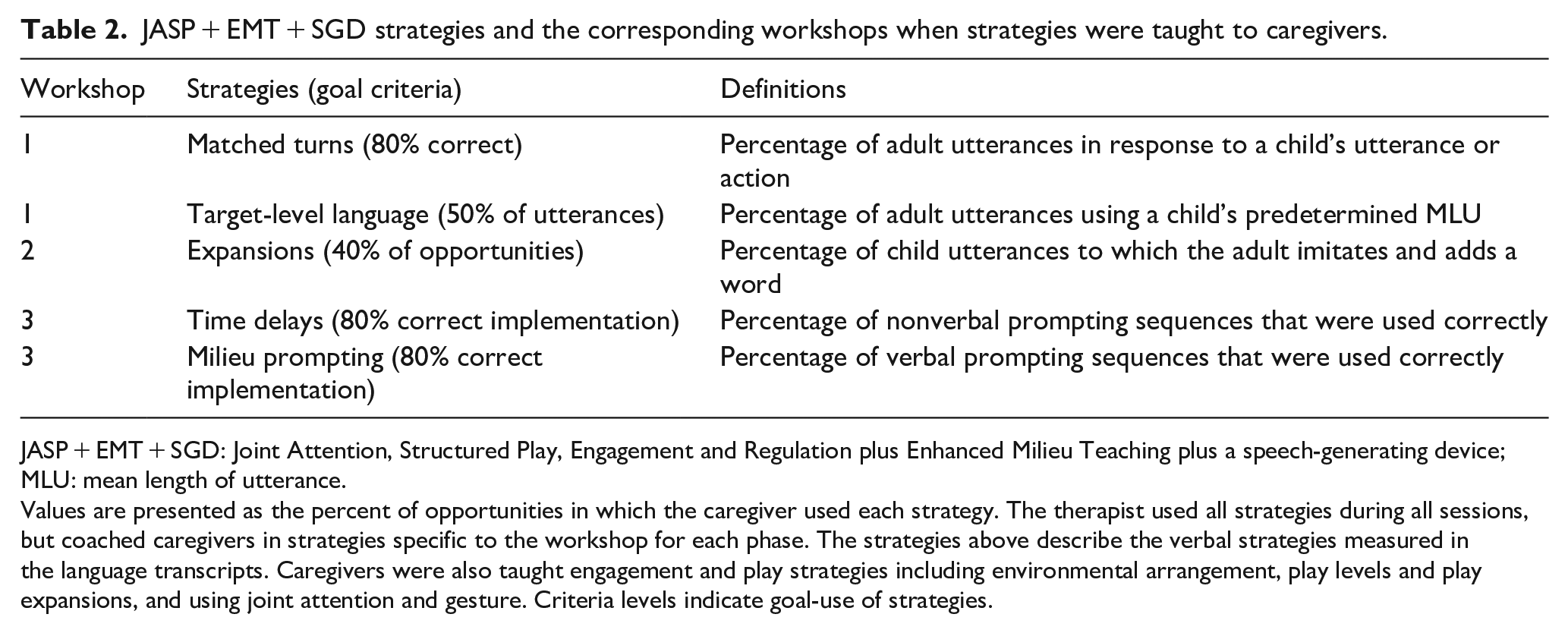
JASP + EMT + SGD: Joint Attention, Structured Play, Engagement and Regulation plus Enhanced Milieu Teaching plus a speech-generating device; MLU: mean length of utterance.
Values are presented as the percent of opportunities in which the caregiver used each strategy. The therapist used all strategies during all sessions, but coached caregivers in strategies specific to the workshop for each phase. The strategies above describe the verbal strategies measured in the language transcripts. Caregivers were also taught engagement and play strategies including environmental arrangement, play levels and play expansions, and using joint attention and gesture. Criteria levels indicate goal-use of strategies.
Early Social Communication Scales
The total number of initiations of joint attention was measured during the Early Social Communication Scales (ESCS), administered by a novel assessor (Mundy et al., 2003). The ESCS is a common and valid observational measure of early social communication behaviors in children with autism who are preverbal or minimally verbal (Trembath et al., 2019).
Preschool Language Scales
Global language was measured using the expressive and receptive language subscales of the Preschool Language Scales, Fifth Edition (PLS-5; Zimmerman et al., 2011). The PLS is a valid measure of language ability in children with autism (Volden et al., 2011) that provides a standard score and age equivalent scores. Raw scores were used in this study due to floor effects for the standard and age equivalent scores for the preverbal participants.
Demographic questionnaire
Demographic information about the children and their families including socioeconomic status (SES) and child participation in therapies in the community was obtained via survey from caregivers at each assessment point.
ADOS-2
At baseline, the child participants were evaluated for symptoms of autism severity on ADOS-2 (Lord et al., 2012). ADOS-2 is the gold standard diagnostic assessment for autism. All participants were administered the first module, based on entry-level language levels. ADOS-2 yields a total score and a 10-point calibrated scale that allows for comparison across participants and over time (Gotham et al., 2009). The raw total score was used as a covariate in all outcome analyses to control for overall autism severity among participants.
Mullen Scales of Early Learning
Participants were assessed for cognitive ability at baseline based on the Early Learning Composite of the Mullen Scales of Early Learning (Mullen, 1997). The visual reception subscale is commonly used as a proxy for a nonverbal intelligence quotient and this standardized score was used to characterize participants at baseline (Bishop et al., 2011).
Caregiver satisfaction
Caregivers in the intervention group completed a brief survey (20 items) at posttest asking to rate their satisfaction with the intervention strategies, effectiveness, and coaching procedures. Each item asked caregivers to rate the intervention on a scale from 1 to 5, with higher scores indicating higher satisfaction with the intervention provided.
Coding and inter-observer agreement
All variables were coded by trained coders blind to the participants’ group assignment. Inter-observer agreement (IOA) for the observational assessments was completed by having a second independent coder score the video-recorded measures for at least 20% of the assessments distributed across timepoints (pre, post, follow-up), participants, and groups. IOA was calculated as the total agreements divided by the sum of agreements and disagreements. IOA for SCU-CCX was 89.21% (range: 73.00%–100%). IOA for SCU-NLS was 91.00% (range: 71.10%–100%). Intraclass correlation coefficients (ICCs) were calculated for the ESCS as suggested by the coding manual (Mundy et al., 2003), which were consistent with the published literature (joint attention: ICC = 0.903; confidence interval (CI): 0.83–0.94).
Statistical analyses
Prior to beginning the analyses, scores for each variable were examined for outliers and nonnormal distributions. Outlying scores were verified for accuracy. All child variables were transformed to adjust for normality. Variables that did not have a skew between −1 and 1 and a kurtosis between −2 and 2 were transformed using square roots prior to imputation so that all variables fell within this acceptable range of normality (George & Mallery, 2010). All proposed baseline covariates were examined using a correlation matrix. None of the proposed covariates (autism severity, pre-intervention scores, see below) had a correlation greater that r = −0.532, thus mitigating the concern of collinearity, given that standards indicating values that exceed a correlation of 0.90 are a concern for multicollinearity (Hair et al., 2016, p. 196).
Multiple imputation of missing data was used to complete the proposed intent-to-treat analysis using SPSS (IBM Corp., 2017). Data for all participants who completed the screening assessments (Mullen, ADOS-2, and NLS) were analyzed regardless of whether they completed intervention sessions, post-intervention, or follow-up assessments. The five participants who were randomized but dropped prior to completing baseline assessments were the only participants excluded from imputation due to incomplete Mullen scores. Fully conditional specification using an iterative Markov chain Monte Carlo method with 50 iterations was used. The comparison and intervention groups were imputed separately. Given the range of missing data for each variable of interest (0%–21%), 20 imputations were created as recommended (Graham et al., 2007). All child-level analyses were completed on each of the 20 imputed data sets; inferences were based on the pooled results using Rubin’s (2004) rules.
Model building
A model building approach was used to test the model fit of four possible covariates (age, autism severity, nonverbal intelligence quotient (IQ), and pre-intervention scores of the dependent variable), identified a priori. Covariates were entered in the order listed. Among the four dependent variables of interest, inclusion of autism severity and pre-intervention scores resulted in an improved model fit as measured by a significant change in the F statistic. Autism severity and pre-intervention score of the dependent variable were maintained in all of the subsequent models as covariates. The model fit was evaluated using an F statistic of the model fit of the original (nonimputed) data. Each model had a statistically significant F statistic (p < 0.05) indicating that the included predictors significantly improved the model fit, with the exception of caregiver use of expansions at follow-up (p = 0.06), caregiver use of time delays at posttest (p = 0.21) and follow-up (p = 0.052), and caregiver use of milieu prompts and follow-up (p = 0.13). However, given that the models approached significance, the pretest variable was maintained in each model for consistency across models.
Results
Means and standard deviations of all observed covariates, pre-intervention variables, and outcome variables are summarized in Table 3. Independent-samples t tests (for continuous variables) and chi-square tests (for categorical variables) indicated no significant between-group differences at baseline for any included variables (Table 1).
Observed means and standard deviations of communication outcomes and regression outcomes at posttest and follow-up.
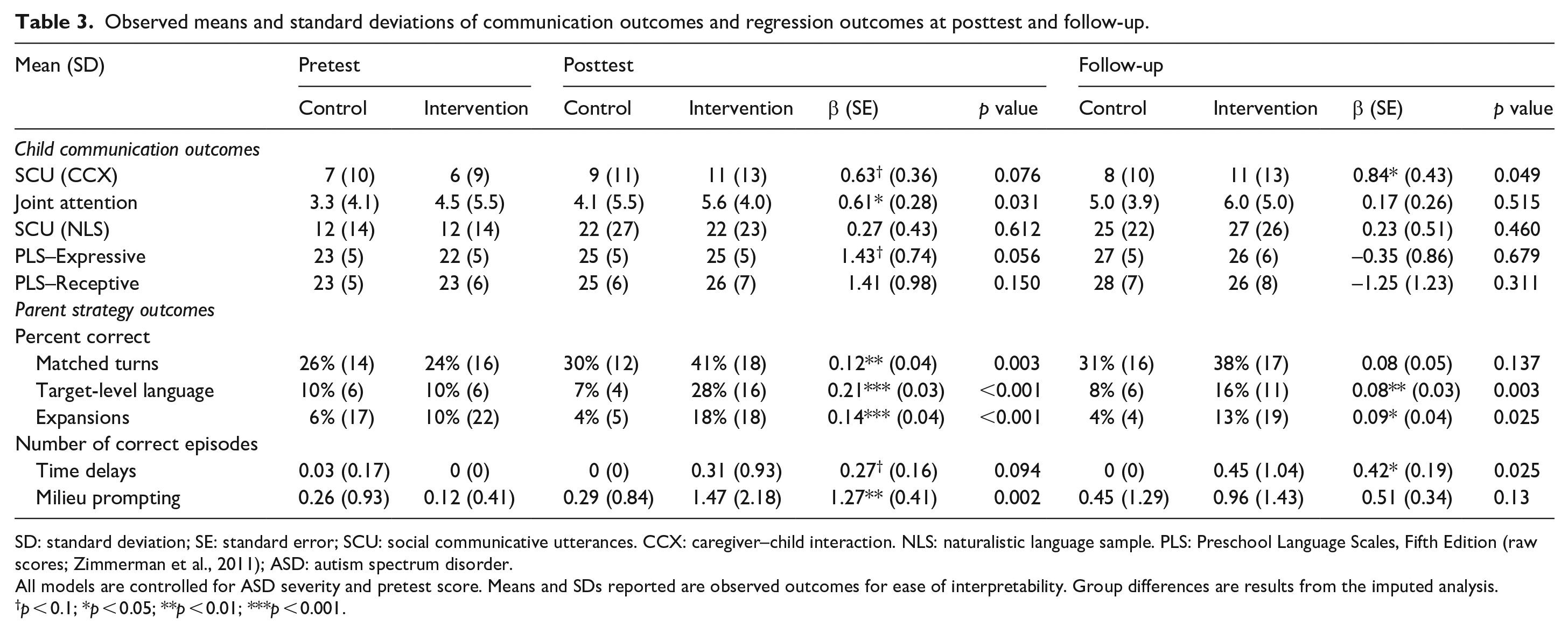
SD: standard deviation; SE: standard error; SCU: social communicative utterances. CCX: caregiver–child interaction. NLS: naturalistic language sample. PLS: Preschool Language Scales, Fifth Edition (raw scores; Zimmerman et al., 2011); ASD: autism spectrum disorder.
All models are controlled for ASD severity and pretest score. Means and SDs reported are observed outcomes for ease of interpretability. Group differences are results from the imputed analysis.
p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
Post-intervention
To test the hypothesis that the intervention improved language and communication outcomes, separate linear regression analyses were completed for the four dependent child communication variables of interest at the post-intervention and follow-up timepoints, controlling for autism severity and pre-intervention scores. There was a significant effect of group assignment on joint attention at post-intervention (p = 0.031). On average, group assignment predicted increases in SCU-CCX (p = 0.076), SCU-NLS (p = 0.612), and PLS–Expressive/Receptive raw scores (p = 0.056 and p = 0.150, respectively), but these increases were not significant. It is important to note that SGD utterances averaged less than one occurrence in each NLS or CCX; changes in SCU were primarily improvements in spoken language. All results are shown in Table 3.
Follow-up
At the follow-up, group assignment did not significantly predict a between-group difference on joint attention (p = 0.515). There was a significant difference between groups in SCU-CCX (p = 0.049) but no significant between-group differences on SCU-NLS (p = 0.460) or PLS–Expressive or Receptive (p = 0.679 and p = 0.311, respectively) at follow-up (Table 3).
Caregiver outcomes
Caregivers trained in the intervention group at post-intervention used significantly more target-level language (p < 0.001), matched turns (p = 0.004), expansions (p < 0.001), and correct prompting strategies (p = 0.003). At follow-up, trained caregivers used significantly more target-level language, expansions, and time delay strategies (p < 0.05; Table 2). At post-intervention, caregivers in the intervention group rated their satisfaction with the intervention high with an average rating of 4.76/5.0 (SD = 0.43).
Discussion
Main findings
Children assigned to intervention demonstrated significant improvements in initiated joint attention immediately following this short-term multi-component communication intervention compared to the comparison group. This improvement in joint attention represents a moderate to small effect size (d = 0.312) and is consistent with previous research reporting effects of early intervention on social communication outcomes (Fuller & Kaiser, 2019). Although these effects were no longer significant at follow-up, the differences at follow-up represent a small effect size (d = 0.223) which is also similar to previous results for this population. Positive, but nonsignificant, results were observed for all other communication measures, and importantly posttest differences on the PLS expressive subscale were significant at the 0.1 level. In addition, caregivers learned most intervention strategies and retained most of these strategies at follow-up including target-level talk, language expansions, and time delay strategies. At follow-up, caregiver matched-turn responsiveness declined slightly from intervention levels and correct episodes of milieu prompting decreased markedly from intervention levels, suggesting that booster training sessions may be required to maintain high levels of responsiveness and precise use of prompting procedures as individual children’s language and communication changes over time.
The relative difference in joint attention did not maintain at the 4-month follow-up. However, children in the intervention group used significantly more SCU during the CCX at follow-up, indicating that the intervention group maintained some aspects of improved proximal social communication after the intervention. Although this difference was small (d = 0.259), the improvement was observed primarily in spoken language (rather than SGD use) in this early verbal population. On average, children in the intervention group used five more utterances in a 10-min sample from pretest to follow-up, nearly doubling their rate of communication, which is a considerable increase for a population characterized by their low rate of communication. However, the majority of participants in both groups remained at a first-words or preverbal classification (fewer than 20 different words used spontaneously in a 20-min language sample) at follow-up (64% of the intervention group and 73% of the control group; Tager-Flusberg et al., 2009). Caregivers implemented and maintained key JASP + EMT + SGD intervention strategies at follow-up which likely contributed to the observed improvements in child SCU-CCX at follow-up.
Strengths
This randomized controlled trial of a multi-component communication intervention is the first to examine the effects of combining direct teaching and naturalistic intervention strategies with the use of an SGD for preverbal or early verbal preschool children with autism. For this population at high risk for remaining minimally verbal, a significant improvement in early communication skills is a promising indicator that language trajectories might be improved with a longer application of this multi-component intervention. Although previous trials have identified effective intervention strategies for improving core autism symptoms (Kasari et al., 2006; Schertz et al., 2013), this study is the first to identify core improvements in the subset of children with autism at the greatest risk for developing fluent speech. These findings are consistent with previous evidence that the inclusion of an SGD in early intervention does not inhibit the development of spoken language (Kasari et al., 2014; Schlosser & Wendt, 2008). Increases in SCU in both groups were predominantly spoken communication, with communication using the SGD accounting for an average of less than one utterance per observation.
This study also represents a feasible and acceptable implementation of a multi-component intervention that requires three sessions of parent training per week. Although the total dosage in this study was low (36 sessions), the dosage of three sessions of parent training per week was relatively high compared to other studies (Heidlage et al., 2020; Roberts et al., 2019). Overall, parents rated the intervention as highly acceptable.
Limitations
The results of this study should be considered in light of specific limitations. First, the relatively small sample size and attrition may have impacted the ability to detect significant differences between groups (Lipsey, 1990; McClelland, 2000). Second, although the quantity of outside services was recorded in hours per week and did not differ between groups, the quality and/or components of these services were not measured and may have contributed to the outcomes for all children in both groups. Finally, this study implemented the individual components of the combined treatment at lower doses than previous studies for both the DTT component (Reichow et al., 2012) and the clinician implementation of JASP-EMT + SGD (Kasari et al., 2014), which may have impacted the effectiveness of the overall model. For example, in the original study of JASPER, children received 30 min per day of clinician-implemented JASPER and DTT to teach precursor skills in addition to a 6 h/day early intensive intervention program, for 6 weeks, a more frequent therapist-implemented dosage than this study; however, the immediate post-intervention effects of the two interventions for joint attention were similar. In addition, although results of the follow-up study of the effects of the JASPER with DTT intervention indicated long-term effects on spoken language for a broad range of children with autism (Kasari et al., 2008), these effects have yet to be replicated in a sample of minimally verbal children with autism. Future research should consider study designs that allow for the analysis of the relative contributions of individual components of the intervention and individualization of dosage of these components based on participant skills and response to intervention (Chow & Hampton, 2019).
Although the results of this study were modest, the participants in this study represented the severe range of the autism spectrum and were at high risk for remaining minimally verbal. Autism severity in this sample, as rated on the 10-point calibrated scale of ADOS-2 (Gotham et al., 2009), averaged above 7 with more than a third of participants scoring a 9 or 10 (Table 1). Therefore, the small gains observed in this study following the relatively brief intervention may be especially important in indicating the need for early multi-component interventions for this population. Future research should focus on optimizing dosage and intensity of this multi-component approach for these most impacted children on the autism spectrum.
Conclusion
A brief multi-component communication intervention may be effective for immediately improving joint attention in children with autism in the early stages of language learning and increasing SCU with their trained caregivers 4 months after intervention. Child outcomes appear to be associated with the demonstrated caregiver acquisition and maintenance of components of the intervention. Future research should evaluate the effects of longer-term or higher-dosage applications of this intervention consistent with recommended dosages of early intervention for this population, examine potential moderators and mediators of outcomes, and analyze how individual components, including caregiver interaction strategies, directly relate to long-term progress.
Supplemental Material
Supplement_1__Fidelity – Supplemental material for Multi-component communication intervention for children with autism: A randomized controlled trial
Supplemental material, Supplement_1__Fidelity for Multi-component communication intervention for children with autism: A randomized controlled trial by Lauren H Hampton, Ann P Kaiser and Elizabeth A Fuller in Autism
Supplemental Material
Supplement_2-_SGD_pages-20200310 – Supplemental material for Multi-component communication intervention for children with autism: A randomized controlled trial
Supplemental material, Supplement_2-_SGD_pages-20200310 for Multi-component communication intervention for children with autism: A randomized controlled trial by Lauren H Hampton, Ann P Kaiser and Elizabeth A Fuller in Autism
Supplemental Material
Supplement_3._DTT – Supplemental material for Multi-component communication intervention for children with autism: A randomized controlled trial
Supplemental material, Supplement_3._DTT for Multi-component communication intervention for children with autism: A randomized controlled trial by Lauren H Hampton, Ann P Kaiser and Elizabeth A Fuller in Autism
Footnotes
Acknowledgements
Thank you to Mark Lipsey and Tiffany Woynaroski who contributed their expertise to the analyses of the results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported through the Health Resources and Services Administration Grant (No. 5R40MC27707) and the US Department of Education Grant (No. H325D070075).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.