
Abstract
Children with autism spectrum disorder are often reported to have more sleep deficits and poorer sleep quality compared with children with typical development. However, most previous studies have serious methodological limitations, such as varying sample sizes in the comparison groups, wide age range of participants, and body mass index not matched between participants. This study investigated whether sleep patterns differed between children with autism spectrum disorder and those with typical development using a carefully matched case–control design and incorporating both actigraphy and sleep log assessments. A total of 78 children diagnosed with autism spectrum disorder were matched with 78 typical development controls in this study. The matched variables included age, gender, and body mass index. The results showed that children with autism spectrum disorder had shorter sleep duration, reduced sleep efficiency, longer sleep-onset latency, and longer wake after sleep onset than children with typical development (ps < 0.05). Further studies are needed to explore the mechanisms underlying these sleep deficits in children with autism spectrum disorder.
Lay abstract
This study compared the sleep pattern between children with autism spectrum disorders and children with typical development using a matched case–control design (matched age, gender, and body mass index). Significant differences were found in night-time sleep duration (total amount of sleep at night), sleep efficiency (percentage of time spent asleep), sleep-onset latency (length of time that it takes to transit from awake to asleep), and wake after sleep onset (total amount of time spent awake after defined sleep onset). Findings showed that children with autism spectrum disorder had poorer sleep quality than children with typical development. Mechanisms underlying the differences should be further explored in order to develop an effective treatment intervention.
Introduction
Autism spectrum disorder (ASD) is defined as a group of complex neurodevelopmental disorders that often present at a young age (World Health Organization, 2016). The prevalence of ASD has increased rapidly in recent years. In Hong Kong, the prevalence of ASD is reported at 14.6 per 1000 children, and the trend of increasing prevalence is expected to continue (Centers for Disease Control and Prevention, 2012). Children with ASD are characterized by significant impairments in social interaction and communication (in varying degrees), accompanied by restricted and repetitive patterns of behavior (American Psychiatric Association, 2013). Apart from these core symptoms, sleep problems are also commonly reported among this population. The most frequently reported sleep problems include sleep-onset delays, night waking after sleep onset, decreased total sleep duration (SD), and decreased sleep efficiency (SE; Elrod & Hood, 2015). Because adequate sleep is critical for children’s brain development, concerns have been voiced about the detrimental effect of sleep disturbance for children with ASD. Existing literature suggests that poor sleep is associated with core ASD symptoms such as stereotypic behaviors (Park et al., 2012), social and communication impairments (Richdale & Schreck, 2009; Taylor et al., 2012), and other maladaptive behaviors (see Cohen et al., 2014, for a review). In addition, sleep problems in children with ASD have also been related to poor sleep hygiene in their parents (Levin & Scher, 2016), which imposed a heavy overall family burden.
When compared with children with typical development (TD), children with ASD tend to have more sleep problems (Cortesi et al., 2010). For example, the prevalence of insomnia in children with ASD ranged from 60% to 80% (Goldman et al., 2012), which was two to three times greater than rates of insomnia in children with TD (Calhoun et al., 2014). In addition to studies in Western countries, several studies have been conducted in Asian regions, where the social culture and living environment differ from those in Western countries (Jose & Bellamy, 2012). For example, Hirata et al. (2016) noted that in Japan, children with ASD experienced significantly more sleep problems (e.g. sleep apnea and parasomnias) compared with children with TD; similar findings were also reported in studies from Taiwan (Chou et al., 2012), Korea (Park et al., 2012), and China (Wang et al., 2013, 2016).
However, these previous studies had several methodological limitations that might affect their conclusions. First, Wang et al. (2016) used retrospective parental reports, where the data for ASD and TD children were collected in different years (2016 vs 2013). Second, sample sizes between children with ASD and children with TD in previous studies differed (e.g. Wang et al., 2016, ASD:TD = 80:917; Hirata et al., 2016, ASD:TD = 193:965). Third, the wide age range of participants in previous studies (e.g. Park et al., 2012, 3–15 years) may also be a confounder for interpreting sleep patterns, as there may be age-related changes in sleep patterns throughout childhood and adolescence (McLaughlin Crabtree & Williams, 2009). Moreover, most previous studies used subjective measures, such as parent-reported questionnaires and scales (e.g. Hirata et al., 2016; Park et al., 2012; Wang et al., 2013), and few studies used objective assessment (e.g. actigraphy, as in Surtees et al., 2019) to compare the sleep problems between ASD and TD groups. Finally, none of the previous matched control studies matched participants’ body mass index (BMI) between the two groups. This is a potential problem as BMI is a major contributor to sleep apnea, which can decrease SE (Zuckerman et al., 2014). In this study, we addressed these issues with a carefully matched case–control study design using both objective and subjective sleep measurements (i.e. actigraphy and sleep log assessments) among children with ASD and TD in Hong Kong.
Methodology
Participants
In total, 156 children (mean age = 10.05 years; standard deviation = 1.08 years) were recruited for this matched case–control study. This group comprised 78 ASD cases and an equal number of TD controls matched by age (8–12 years), gender, and BMI (±5%). Cases were defined as those diagnosed with ASD by a psychiatrist based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (American Psychiatric Association, 2013), and recruited from five local special schools for children with mild intellectual disability in Hong Kong. We excluded children with one or more comorbid psychiatric disorders, complex neurological disorders (e.g. epilepsy, phenylketonuria, fragile X syndrome, and tuberous sclerosis), or that took medication that may affect sleep (e.g. melatonin supplements and anti-depressants). Information on the nonverbal intelligence quotient (IQ) of each child with ASD was collected from their school records, based on assessment by educational psychologists using the Wechsler Intelligence Scale for Children (Chinese revised) (for more information, see Gong & Cai, 1993). Children’s autism severity was determined with the Social Responsiveness Scale, Second Edition (Constantino & Gruber, 2012).
Controls were defined as children with TD who did not have a previous medical history of ASD (based on parental report), were healthy, and did not take any medicine during the study period. A control child was selected for each ASD subject by matching their age, gender, and BMI. Control children were recruited from 10 mainstream primary schools in Hong Kong. All participants were living with their parents at home. This study was announced to all primary schools and special schools for mild intellectual disability in Hong Kong through mass email. Written consent was obtained from children’s parents or guardians. This study was approved by the relevant ethics committee. Demographic data for the two groups are shown in Table 1.
Demographic statistics of participants in each group.
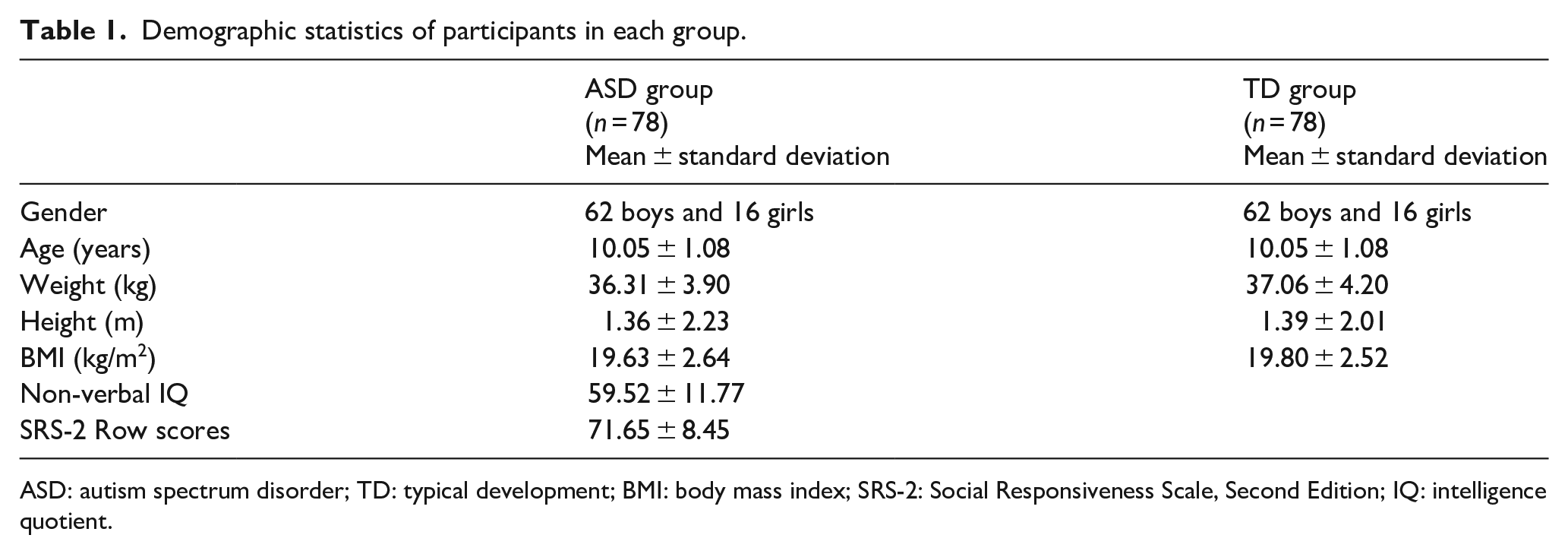
ASD: autism spectrum disorder; TD: typical development; BMI: body mass index; SRS-2: Social Responsiveness Scale, Second Edition; IQ: intelligence quotient.
Procedure
Each child participated in a 1-week assessment, during which their habitual sleeping patterns were assessed with an actigraphy accelerometer (ActiGraph Model GT3X) and a sleep log. Participants were requested to wear a GT3X accelerometer on their non-dominant wrist for seven consecutive days (from Monday to Sunday), and take it off only during bathing or water activity. Four sleep parameters were measured: SE (actual sleep time divided by time in bed, expressed as a percentage), sleep-onset latency (SOL, length of time to fall asleep, expressed in minutes), SD (expressed in hours), and wake after sleep onset (WASO, length of time awake after initially falling asleep, expressed in minutes). The Sadeh algorithm was implemented to identify sleep onset and sleep offset, where actigraphy data were translated into 1-min sleep-wake epochs (Sadeh et al., 1994). For the sleep log assessment, participants were assisted by their parents to recall specific sleep patterns (e.g. bedtime, sleep start, sleep end, wake-up time, and SD) and record them in a sleep log the next morning each day for the duration of the assessment.
Data analysis
Actigraphy assessment parameters were averaged across the weekdays (Monday to Friday) and the weekend (Saturday and Sunday) for each participant. Appropriate descriptive statistics were used to summarize all study variables. Mann–Whitney and Wilcoxon signed-rank tests were used for pair-wise between- and within-group comparisons. Spearman’s correlations were used to determine the relationship between actigraphy assessments and sleep log for two sleep parameters (SE and SD) to check the validity of the sleep log. All statistical analyses were conducted using SPSS (version 23.0) for Windows (SPSS Inc., Chicago, IL, USA). p-values less than 0.05 were considered statistically significant. The results are presented as mean (standard deviation).
Results
Actigraphy assessment
The Mann–Whitney tests indicated there were significant group differences in SE, WASO, and SD during the weekday and weekend periods (all ps < 0.05). Children with ASD had lower SE (ps < 0.05), longer WASO (ps < 0.001), and shorter SD (ps < 0.05) than children with TD during the weekdays and weekend. For within-group comparisons, the Wilcoxon signed-rank tests revealed there were significant differences in both WASO and SD between weekdays and the weekend in each group (all ps < 0.05). Both the ASD and control groups had shorter WASO (ps < 0.001) and longer SD during the weekend than during the weekdays (ps < 0.05). However, there was no significant difference between weekdays and weekend in SE in either group (ps > 0.05) (refer to Table 2 for more information).
Sleep parameters during weekday and weekend sleep measured by actigraphy and sleep log assessments.

ASD: autism spectrum disorder; SD: standard deviation.
Sleep log assessment
The Mann–Whitney tests revealed there were significant group differences in SE (weekend), SOL (weekday and weekend), and SD (weekday) (all ps < 0.05). Compared with the TD group, the ASD group had lower SE during the weekend (p = 0.02), longer SOL during both weekdays and the weekend (ps < 0.001), and shorter SD during weekdays (p = 0.008). For within-group comparisons, the Wilcoxon signed-rank tests showed there were significant differences in SOL between weekdays and the weekend in both groups (all ps < 0.05). Both the ASD and control groups had shorter SOL during the weekend than during weekdays (ps < 0.05). No significant differences between weekdays and the weekend were found in SE and SD in either group (ps > 0.05) (refer to Table 2 for more information).
Correlations between actigraphy assessment and sleep log
To check the validity of the sleep log for children with ASD, the average values of the sleep parameters (i.e. SE and SD) over the assessment period were determined. The correlation between the two assessments on SE and SD were 0.24 (p = 0.04) and 0.60 (p = 0.001), respectively.
Discussion
This study compared sleep quality profiles of children with ASD with carefully matched (age, gender, and BMI) control children with TD drawn from normal mainstream schools. Consistent with previous studies (Souders et al., 2017), children with ASD had lower SE, longer SOL, longer awake time after sleep onset, and shorter SD (by nearly an hour) than children with TD, regardless of whether it was a weekday or the weekend. These findings confirmed that children with ASD had poorer sleep quality than children with TD.
As shown in Table 2, the SD in children with ASD and children with TD was significantly longer during weekend. A possible explanation for this is that children were free from schooling during weekend and therefore could sleep for a longer duration. This weekend catch-up sleep phenomenon was also observed in a recent local territory-wide study (Huang et al., 2019), where children had sufficient sleep on weekends and holidays but not weekdays. Nevertheless, the amount of sleep in children with ASD was still considered inadequate, even on the weekend. According to a recent evidence-informed guideline on the recommended amount of sleep for pediatric populations (Paruthi et al., 2016), children aged 6–12 years should have at least 9 h of sleep. In this study, the average SD of children with ASD on both weekdays and the weekend (measured by different assessments) was less than 9 h per night.
For the WASO and SOL sleep parameters, this study revealed there were major significant differences between weekdays and the weekend in both groups. Both groups showed significant drops in WASO and SOL from weekdays to the weekend. This was particularly evident in the control children with TD, where the WASO during weekdays dropped to almost half that during the weekend. We suspected that academic stress may contribute to such differences. It is generally believed that academic stress during weekdays would be higher than that during the weekend. In Hong Kong, academic stress is regarded as a prominent source of stress for primary school children (Leung et al., 2006), and studies have shown that it could negatively impact the circadian rhythm (Van Reeth et al., 2000). Åkerstedt et al. (2007) also discovered that bedtime stress and worries could impair sleep with lower SE and increased WASO and SOL. Because our participants were free from schooling during the weekend, it is reasonable to believe that their academic stress and bedtime worries were lower and therefore their WASO and SOL dropped significantly from the weekday values. Other conditions, such as the potential increased physical activity level and natural sunlight exposure during the weekend, may also play in a role in the significant drop of WASO and SOL over the weekend. Further studies that investigate the influence of these factors are warranted.
We found moderate to strong correlations for SE (0.24, p = 0.04) and SD (0.60, p = 0.001) measured by actigraphy assessment and sleep logs, respectively. Similar to our previous study (Tse et al., 2019), these results suggested that both assessment methods could be used interchangeably to measure the habitual sleep patterns of children with ASD. However, compared with actigraphy assessment, parents’ reports tended to underestimate the SD of their children. This may be attributable to a general bias among parents. In Hong Kong, it is common for parents to complain that their children did not have sufficient sleep because of increased homework and extracurricular activities. We suspect that this general belief meant that parents tended to be conservative in estimating the SD of their children.
Despite the strengths of this study, several limitations require attention when interpreting the results. First, we did not measure the IQ of all participants in this study and therefore could not determine whether any difference was due to intellectual disability. Future studies should consider incorporating such measurement for all participants. Second, we did not collect any information about after-school group therapy (e.g. occupational therapy, speech therapy, and behavioral therapy) from the parents of children with ASD. Without this information, we did not know if these activities could have affected our findings. Third, there was no comprehensive ASD diagnosis for the ASD severity of participants; subsequent studies should consider using diagnostic characterization (such as Autism Diagnostic Interview–Revised (ADI-R) and Autism Diagnostic Observation Schedule (ADOS)) to provide more comprehensive data on ASD severity. Finally, there was no measurement to assure that none of the children with TD were on the ASD spectrum, although oral reports were collected from their parents that none of these children were diagnosed with ASD before this study.
Conclusion
This study was the first large-scale matched case–control study comparing sleep patterns between populations of children with ASD and TD in the Asian region using both objective and subjective sleep assessments. The differences in sleep parameters between children with ASD and children with TD shown in this study provide more evidence of sleep deficits in children with ASD. It is therefore important to address this issue by investigating the underlying mechanisms of sleep deficits in children with ASD, which may lead to development of effective treatments for these problems.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was financially supported by EdUHK departmental seed funding (Ref no.: R4002).