
Abstract
This study examines the construct validity of the First-Year Inventory 2.0 with respect to other established instruments in a sample of high-risk infant siblings of children with Autism Spectrum Disorder. The First-Year Inventory 2.0 is a parent-report screening instrument designed to identify 12-month-old infants at risk for an eventual diagnosis of Autism Spectrum Disorder and consists of two domains: Social-Communication and Sensory-Regulatory. Although the First-Year Inventory 2.0’s screening psychometrics have been examined, its construct validity has not been investigated. In a sample of 112 high-risk 12-month-olds, we examined the First-Year Inventory 2.0’s associations with the Autism Observation Scale for Infants, an observer-based Autism Spectrum Disorder screener, and with other developmental instruments measuring similar areas in social communication and regulatory functioning in young children. Findings generally supported the First-Year Inventory 2.0 associations with other instruments in expected ways. The First-Year Inventory 2.0 Social-Communication domain was notably associated with the Autism Observation Scale for Infant’s total score and with language and communication domains of the Vineland and the Mullen. The Sensory-Regulatory domain showed minimal associations with other instruments that only had a few sensory items. Considering different objectives and strengths of assessments, researchers and clinicians are encouraged to utilize a variety of instruments in a comprehensive evaluation of a child.
Lay abstract
The First-Year Inventory 2.0 is a parent-report screening instrument designed to identify 12-month-old infants at risk for an eventual diagnosis of Autism Spectrum Disorder. This instrument focuses on Social-Communication and Sensory-Regulatory areas of infant behavior. Although the First-Year Inventory 2.0 screening performance has been previously studied, its validity has not been examined. Establishing validity of an instrument is important because it supports the effectiveness and the reliability of the instrument. In this study, we examined relationship between the First-Year Inventory 2.0 (Social-Communication and Sensory-Regulatory areas) and other instruments that measure similar areas of infant behavior in a sample of high-risk infant siblings of children with Autism Spectrum Disorder. These other instruments share some common aims and theoretical areas with the First-Year Inventory 2.0: the Autism Observation Scale for Infants, the Mullen Scales of Early Learning, the Vineland Adaptive Behavior Scales-II, and the Infant Behavior Questionnaire. Findings generally supported the validity of the First-Year Inventory 2.0 with other instruments. In particular, the Social-Communication area of the First-Year Inventory 2.0 showed greater commonality with other instruments than in the Sensory-Regulatory area. The Sensory-Regulatory area seemed to be a unique feature of the First-Year Inventory 2.0 instrument. Considering different aims and strengths of assessments, researchers and clinicians are encouraged to utilize a variety of instruments in a comprehensive evaluation of a child.
With the prevalence of Autism Spectrum Disorder (ASD) rising in recent years (Centers for Disease Control and Prevention, 2018), the development of reliable and valid instruments to detect early signs of ASD is paramount. ASD is a neurodevelopmental disorder characterized by impairments in social communication and repetitive and restricted behaviors (American Psychiatric Association, 2013), with many individuals also exhibiting atypical sensory features (Ben-Sasson et al., 2019). A diagnosis of ASD is typically not made by clinicians until a child reaches 3 or 4 years of age (Jo et al., 2015), therefore, the early signs of ASD have been typically detected using parent-report screening instruments (McPheeters et al., 2016).
The First-Year Inventory (FYI Version 2.0; Baranek et al., 2003) is a screening instrument that asks parents of 12-month-olds about infant behaviors that indicate risk for later ASD (Baranek et al., 2003; Reznick et al., 2007). Since screening surveys are easy and fast to fill out and require low resources, such as in trained staff, time, and equipment, the FYI 2.0, like similar early screeners, is often administered first to identify children who are likely to develop ASD and benefit from further resource-heavy diagnostic processes. For example, in a large community sample study by Turner-Brown et al. (2013), the FYI 2.0 yielded 44.4% sensitivity, 98.9% specificity, 30.8% positive predictive value, and 99.3% negative predictive value using a two-domain cut-off criterion (⩾22.5 for the Social-Communication (SC) domain and ⩾14.75 for the Sensory-Regulatory (SR) domain) at 12 months for an eventual diagnosis of ASD at age 3 years. A child identified with an elevated risk for ASD in the FYI 2.0 using the cut-off may be subsequently recommended for further diagnosis or surveillance until the child becomes older. Thus, screeners like the FYI 2.0 are cost-effective ways to identify a higher risk sub-sample of a population that includes those without ASD.
While the screening performance of the FYI 2.0 has been previously validated (Turner-Brown et al., 2013; Lee et al., 2019), evidence that its two main constructs measure what they intended to measure is lacking. Specifically, the FYI 2.0 consists of SC and SR areas of functioning. Language and social communication development in early childhood have served as crucial markers for typical (Gleason & Ratner, 2017) and atypical development including ASD (Geurts & Embrechts, 2008). Sensory function is also another important component underlying children’s behavior, although often neglected as an independent behavioral outcome. For example, sensory processing has been implicated in multiple areas of functioning, including cognitive (Gallese & Lakoff, 2005), affective (DeSantis et al., 2004), and motor domains (Johansson & Cole, 1992) in typical (Fox & Polak, 2004) and atypical development (Kern et al., 2007). Atypical sensory features refer to infants’ unusual sensory interests and responses across modalities (e.g. tactile, visual, and auditory) that are often categorized as over-responsivity, under-responsivity, and seeking patterns of behavior (Ben-Sasson et al., 2019). In infancy, atypical sensory behaviors can be operationalized by measuring infants’ exaggerated (over-responsivity) responses, lack of/delayed responses (under-responsivity), or repetitively seeking responses to various sensory stimuli including loud noise (sound), bright color (visual cues), and unusual sensation/touch (tactile) (Baranek, 1999).
Given the FYI 2.0’s SC and SR focus, patterns of associations with other instruments measuring infants’ social communication/language and sensory behaviors can demonstrate the FYI 2.0’s construct validity. The FYI 2.0 SC includes a variety of social-communicative and language items related to typical and atypical development around 12 months of age. Similarly, well-established standardized developmental instruments like the Vineland Adaptive Behavior Scales (VABSs; Sparrow et al., 1984) and the Mullen Scales of Early Learning (MSEL; Mullen, 1989) assess young children’s socialization, communication, and language, among other skills. A higher score in the FYI 2.0 indicates more atypical functioning, whereas higher scores in the VABS and MSEL indicate greater competencies in social communication and language skills. All three instruments have items measuring some aspect of how well the child understands and expresses intentions or concepts through speech and gestures, as well as using non-verbal cues.
Next, the FYI 2.0 SR includes items related to infants’ affective responses, approach-avoidance responses to sensory stimuli, and SR behavior to assess atypical sensory behaviors. The Infant Behavior Questionnaire (IBQ; Rothbart, 1981) similarly assesses infants’ affective and regulatory responses to external stimuli from a parent report, based on a temperament perspective. Since the basis of individual differences in reactivity and regulation is rooted in differences in sensory processing and behavior (Fox & Polak, 2004), similar areas of behavior as the FYI 2.0’s SR are assessed under the broader dimensions of affect and regulation in the IBQ.
Finally, in addition to examining similar constructs, an association between the FYI 2.0 and another screener can corroborate the purpose of the FYI 2.0 as an early ASD screening instrument. The Autism Observation for Infants (AOSIs; Bryson et al., 2008) is a 19-item observer-rated ASD screening instrument that includes items related to atypical social-communicative/language behaviors and other early behavioral markers associated with ASD. An association between the FYI 2.0 and the AOSI would illustrate the extent to which two ASD screeners may tap shared constructs.
This study aimed to investigate associations between the FYI 2.0 and other established instruments that share similarities at the construct (VABS, MSEL, and IBQ) and the scale level in a sample of 12-month-old infant siblings of children with ASD. Because the infant siblings of children with ASD are generally more likely than infants from a low-risk community sample to undergo clinical assessments utilizing ASD screening and standardized instruments due to their risk status, examination of the associations among the instruments in this high-risk sample seemed particularly pertinent. To examine construct validity, the FYI 2.0 SC and SR related dimensions from the VABS, MSEL, and IBQ were extracted and classified as Related Constructs. Four Related Constructs were Language, Socialization, Regulation, and Affect. Motor behavior was also extracted from the measures but it was classified as a Less Related Construct. For the Related Constructs, we hypothesized that the FYI 2.0’s SC construct and subscales would be related to the Language and the Socialization constructs. We also expected associations between the FYI 2.0 SC and the Affect related constructs since Affect plays an important role in the social aspect of communication. For the FYI 2.0 SR, we hypothesized that the construct would be associated with Affect and Regulation related constructs, considering that SR items ask parents about infants’ affective and regulatory responses to certain sensory experiences and internal systems (e.g. sleep/wake). Finally, we hypothesized that the FYI 2.0 total score and the AOSI total score would be at least moderately associated given their shared ASD screening purpose.
Methods
Participants
A sample of 112 high-risk infants (63 male and 49 female) who had an older sibling with ASD and their caregivers from three Canadian sites (Toronto, Ontario; Hamilton, Ontario; Halifax, Nova Scotia) were recruited from local clinics and neighborhoods. The infants were born at 36–42 weeks gestation with a birth weight >2500 g. The FYI 2.0 and all other assessments were completed when the infants were 12 months of age (M = 12.42 months, SD = 0.52). Table 1 provides demographic details for the sample.
Participant Demographic Characteristics (N = 112)

Mullen T-score summary; ELC = early learning composite scor.
Measures
The FYI 2.0 (Baranek et al., 2003) is a 63-item survey that asks parents about their infants’ behavior. It consists of 46 items that ask parents to endorse infant behaviors using a four-point Likert-type scale, from “1 = Never” to “4 = Often,” and 14 multiple-choice items, with three or four choices each (Table 2). Each item score is converted into a risk score, which is weighted based on the frequency of probabilities in the normative sample. Three other items include two open-ended items and one item asking about the infants’ consonant sound production. The two open-ended items and nine items that did not load in the two construct scoring factors in Reznick et al. (2007) study were excluded in the analysis (see Reznick et al., 2007 for more details of scoring). Previous publications have used “domain” and “construct” to describe the SC and the SR and their subcomponents, respectively, in previous FYI 2.0 publications (e.g. Baranek et al., 2003; Turner-Brown et al., 2013). To be consistent with other instruments, however, we used “constructs” for the SC and SR components and “subscales” for their subcomponents below.
The First-Year Inventory (Version 2.0) item summary.
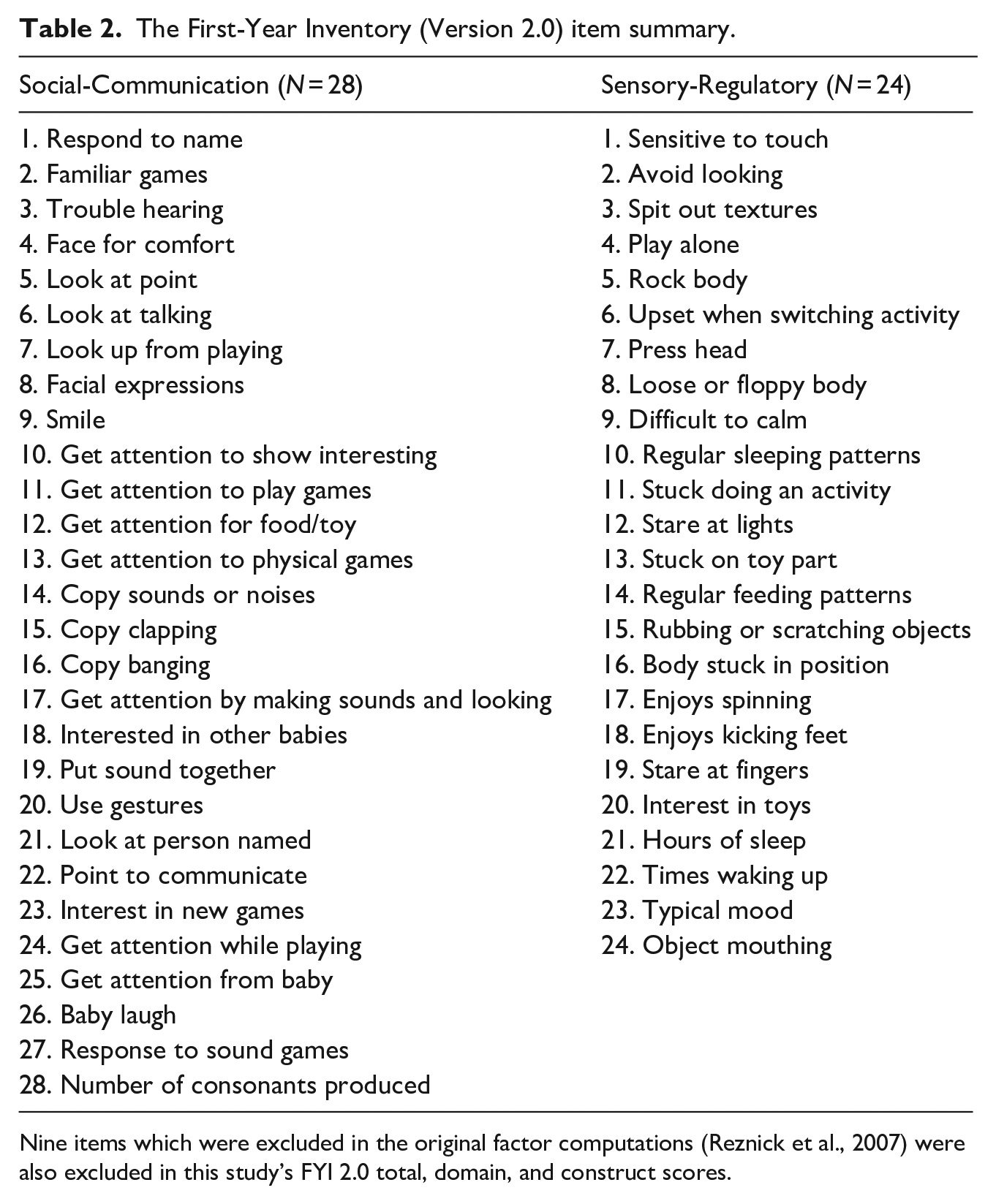
Nine items which were excluded in the original factor computations (Reznick et al., 2007) were also excluded in this study’s FYI 2.0 total, domain, and construct scores.
The FYI 2.0 items are organized into two main constructs based on both factor analysis and a theoretical approach supported by Classical Test Theory (Allen & Yen, 2002). Each construct is composed of four subscales. The SC consists of Social Orienting and Receptive Communication (SORC), Social-Affective Engagement (SAE), Imitation (IM), and Expressive Communication (EC) subscales. The SR consists of Sensory Processing (SP), Regulatory Patterns (RPs), Reactivity (RE), and Repetitive Behavior (RB). Raw scores are converted to weighted risk scores (see Reznick et al., 2007) with higher scores suggesting more atypical behaviors in each subscale and construct. A total risk score on the FYI 2.0 can be calculated by adding the two constructs.
The Autism Observation Scale for Infants (AOSI; Bryson & Zwaigenbaum, 2014) is a 19-item direct interactional and observational measure consisting of standardized activities designed for observation of early emerging ASD-related behaviors during examiner and infant interaction. During play, the examiner elicits a target behavior with a set of systematic presses; these target behaviors are related to attention, social engagement, communication, and atypical sensory-motor behavior. The examiner scores the infant from 0 (typical) to 2 (atypical), or 3 (extremely atypical), based on the occurrence or non-occurrence of behaviors. A score of 1 indicates either delayed or questionable atypical behavior. Higher values indicate greater atypicality up to a maximum total score of 50. The inter-rater reliability correlation coefficient on the total score is excellent at 0.90. The test–retest reliability is 0.63.
The MSEL (Mullen, 1995) is a standardized developmental assessment for children from birth to 68 months of age. It consists of five scales: Gross Motor (GM), Visual Reception (VR), Fine Motor (FM), Receptive Language (RL), and Expressive Language (EL). Four of the five scale scores (VR, FM, RL, and EL) are combined to produce the Early Learning Composite (ELC) summary score, which is a standard score with a mean of 100 and a standard deviation of 15. The overall reliability of the scale is good (0.82–0.85 for birth to 24 months) and its inter-rater reliability is excellent (0.91–0.99).
The VABS (VABS; Sparrow et al. 1984; VABS-II;) is a standardized semi-structured parent or caregiver interview assessing four areas: Communication (receptive and expressive), Daily Living (personal, domestic, and community), Socialization (interpersonal relationship, play and leisure time, and coping skills), and Motor (GM and FM for children under 6 years of age). The items are scored from 0 (seldom or never present) to 2 (always present), with higher scores indicating better adaptive behavior in the real world. The sum of four scales (Communication, Daily Living Skills, and Socialization) scores produces an Adaptive Behavior Composite (ABC) score, which measures infants’ overall everyday adaptive functioning (Sparrow et al., 2005). Standardized scores were used for this study. The VABS reports high internal consistency (0.93–0.94) and strong convergent validity values (0.93) (de Bildt et al., 2005; Volkmar et al., 1993). For this study, only relevant constructs (Communication, Socialization, and Motor) were used for analyses.
The IBQ (Rothbart, 1981) is a parent-report measure of infant temperament designed for infants between 3 and 12 months of age, consisting of items that relate to six areas of infant behavior: Activity Level, Smiles and Laughter, Fear, Distress to Limitation, Soothability, and Orienting Duration. Parents are asked to report the frequency of occurrence of specific infant behaviors based on the previous 2 weeks, using a seven-point Likert-type scale ranging from 1 (never) to 7 (always), or does not apply (NA) if the event did not occur. The IBQ has mean item-scale correlations ranged from 0.41 to 0.77, and coefficient alphas from 0.67 to 0.84. For this study, Smile and Laughter, Fear, Distress to Limit, and Soothability were used for analyses.
Statistical analysis
To ease data interpretations, constructs from the MSEL, VABS, and IBQ were organized into varying levels of relevance to the FYI 2.0 SC and SR constructs, that is, Related Constructs and Less Related Constructs. For example, RL and EL from the MSEL and Communication from the VABS were grouped under a newly created summary construct, Language. The “Related Constructs” consisted of Language, Socialization, Regulation, and Affect. The “Less Related Constructs” consisted of Motor. The AOSI was examined separately as a “Related Purpose” instrument with the FYI 2.0.
Spearman correlation coefficients were calculated for concurrent measurements of the FYI total, construct, and subscale scores with each of the aforementioned constructs and summary constructs. Although various multiple group comparison methodologies (e.g. Bonferroni and Benjamini–Hochberg) were initially considered, because the costs of the adjustment outweighed their benefits, they were not used. Literature suggested that the adjustments are useful and appropriate when there are a relatively small number of multiple comparisons, but not when the cost of false negatives becomes very high in a large number of comparisons (e.g. McDonald, 2014; Rothman, 1990). Also, given that the main purpose of this study is to explore potential relationships rather than to assert the statistical significance of the extent in which a particular coefficient estimate is true or not, we interpreted correlation coefficients with respect to the magnitude of associations rather than p values. In this study, a zero correlation would indicate that the measures were independent of each other and is just as important as a high correlation, despite lack of statistical significance.
To help interpret the magnitude of correlation coefficients, we used a guideline provided by a meta-analysis study that characterized <0.2 as small, 0.2–0.3 as medium, and >0.3 as large magnitudes (Hemphill, 2003). Instead of p values, 95% confidence intervals were calculated with the Fisher z-transformation. The confidence intervals provide information about the robustness of the point estimates and clarify the precision of estimates of minimal correlation (Supplemental Appendix). Data were analyzed using SAS for Windows, Version 9.4 (SAS, Cary, NC, USA).
Results
Correlation between FYI 2.0 and AOSI
Table 3 shows the range of values, means, and standard deviations, and Table 4 shows correlations between FYI 2.0 risk scores and total AOSI scores. The FYI 2.0 SC total score and three of its subscales—SORC, SAE, and EC—were moderately correlated with the AOSI score. The AOSI showed low correlations with the SR construct and its subscales. Post hoc analyses of associations between the FYI 2.0 SR and the AOSI items relevant to the sensory domain (i.e. reactivity and atypical sensory behavior) revealed a small magnitude of association between the SR’s SP and the AOSI’s atypical sensory behavior (r = 0.14).
Distribution characteristics of FYI variables.
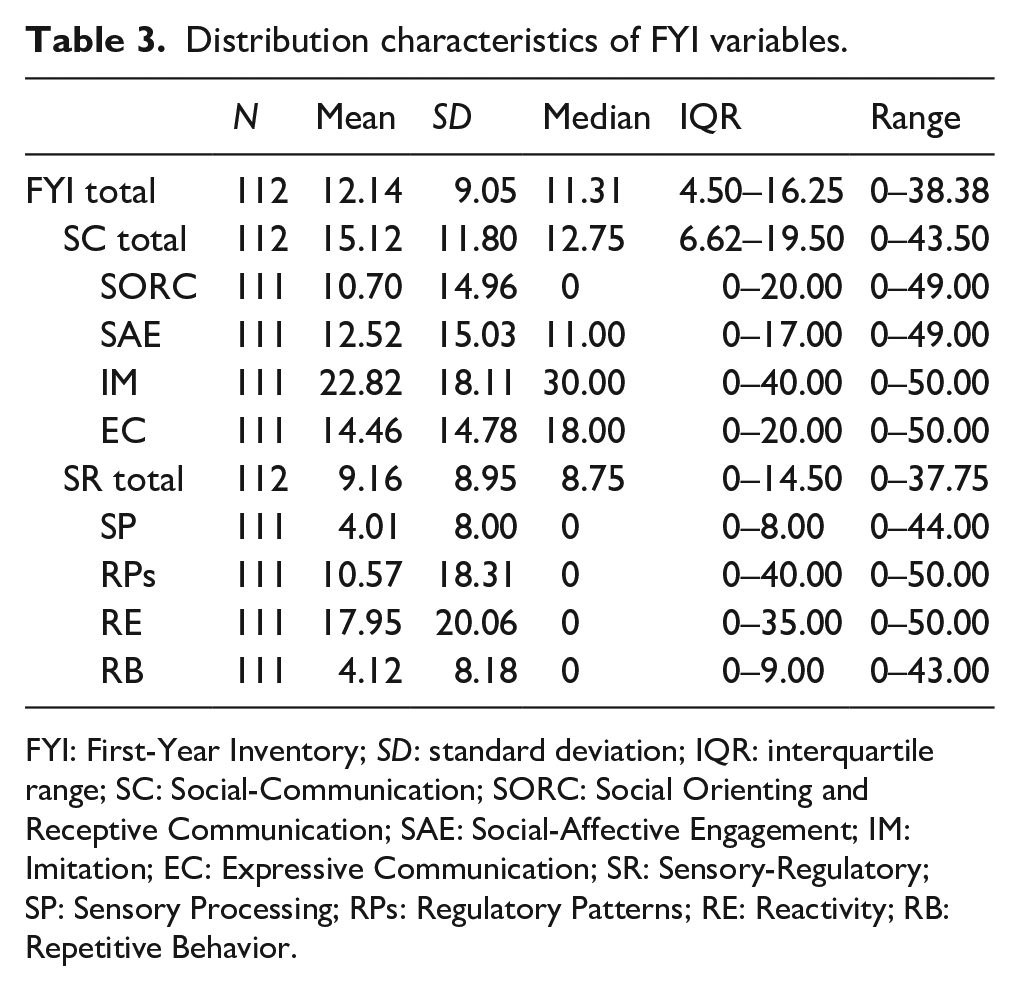
FYI: First-Year Inventory; SD: standard deviation; IQR: interquartile range; SC: Social-Communication; SORC: Social Orienting and Receptive Communication; SAE: Social-Affective Engagement; IM: Imitation; EC: Expressive Communication; SR: Sensory-Regulatory; SP: Sensory Processing; RPs: Regulatory Patterns; RE: Reactivity; RB: Repetitive Behavior.
12-month Spearman correlations between the FYI 2.0 and other measures.

FYI: First-Year Inventory; SC: Social-Communication; SORC: Social Orienting and Receptive Communication; SAE: Social-Affective Engagement; IM: Imitation; EC: Expressive Communication; SR: Sensory-Regulatory; SP: Sensory Processing; RP: Regulatory Patterns; RE: Reactivity; RB: Repetitive Behavior; AOSI: Autism Observation Scale for Infants.
Expected Correlation indicates the direction of the expected relationship. Source of the subscale:
MSEL.
VABS.
IBQ.
When expectations for correlations are in the opposite direction for scales used in the average, the signs of the correlations for one of the scales is restated so that the average correlations do not cancel each other out.
Correlation between FYI 2.0 and Related Constructs
Language
The FYI 2.0 total and SC construct and subscale scores were generally moderately correlated with the MSEL’s RL and EL (Table 4). The FYI 2.0’s subscales EC and SORC showed mostly large correlations with Language constructs from the VABS (Communication) and MSEL (RL and EL). The FYI 2.0’s SAE subscale was moderately correlated whereas the IM subscale showed a low correlation, with Language constructs of the VABS and MSEL. The FYI 2.0’s SR construct and subscales, in general, showed low correlations with Language constructs, except for the RE subscale. The FYI 2.0’s RE subscale was moderately correlated with the MSEL’s EL construct.
Socialization
The FYI 2.0 total and the SC construct scores showed large correlations with the VABS Socialization domain, except for the IM subscale, which was moderately correlated. The FYI 2.0’s SR construct score and RE subscale showed low correlations. The FYI 2.0’s SP, RP, and RB subscales were all moderately correlated with the Socialization construct.
Regulation
The FYI 2.0’s total scores showed a low correlation with the Regulation construct, the IBQ’s Soothability construct. This low correlation pattern was observed for most of the SC and the SR constructs and subscales, except for two subscales. The SC’s SORC subscale and the SR’s SP subscale were moderately correlated with the Soothability construct.
Affect
The FYI 2.0 total score showed a low correlation with the MSEL’s positive and negative affect constructs. However, the FYI 2.0’s SC construct as well as SORC and SAE subscales showed large correlations with the IBQ’s Smiles and Laughter construct. The EC subscale was moderately correlated with Smiles and Laughter, whereas the IM subscale showed a low correlation. The SC and SR showed generally stronger associations with the positive affect construct, Smiles and Laughter, than with the negative affect Fear construct of the IBQ. The FYI 2.0’s SR construct and subscales showed low correlations with both positive and negative affect.
Correlation between FYI 2.0 and Less Related Constructs
Motor
The FYI 2.0 total score was moderately correlated with Motor constructs, except for FM. The FYI 2.0’s SC construct showed moderate to large correlations with Motor constructs. The SC’s subscales also showed similar moderate to large correlation patterns with Motor constructs, except with FM. The SR construct and subscales generally showed low correlations with Motor constructs, with some exceptions. For example, the FYI 2.0’s RP subscale was moderately correlated with Motor constructs, except for FM.
Discussion
This study investigated the FYI 2.0’s construct validity with other established assessments that share similar constructs and purpose in a sample of high-risk infants at 12 months of age. In general, expected patterns of correlation of the FYI 2.0 with other measures were more evident for the SC construct than the SR construct. The AOSI total score showed a large correlation with the FYI 2.0 SC construct but small correlations with the FYI 2.0 total score and SR construct. The magnitudes of correlations between the FYI 2.0 SC subscales and the AOSI were generally moderate, except for a small correlation with respect to IM. It is possible that because the OSI items were not separated by similar SC and SR constructs, the correlations between the FYI 2.0 SC subscales and the AOSI total score were attenuated. The magnitude of associations may have also been affected by differences in sources of data (i.e. trained professionals for AOSI and parents for FYI 2.0). In addition to clear differences in opportunities to observe behavior (i.e. a single, relatively brief semi-structured session with specific presses for behavior versus the child’s behavior in the natural day-to-day environment), differences in informant perspectives (such as between a parent and a professional) can influence results with individual biases about expected infant behavior (De Los Reyes, 2011; Grills & Ollendick, 2002). Disagreements between observer and parent ratings are common (e.g. Stifter et al., 2008), and low correlations have been also found between the AOSI and its parent-report version, the Autism Parent Screen for Infants (APSI; Sacrey et al., 2018).
A closer comparison of items revealed differences between the FYI 2.0 and the AOSI. Even when similar concepts were tapped, the nuances of wording and description made no items the same. For example, a small correlation between the FYI 2.0 SC IM subscale and the AOSI total score may be attributable to the two instruments’ differences in target imitative behaviors, scopes, and underlying evaluation processes involved. The one AOSI IM item was rated based on infants’ ability to imitate an examiner’s actions during a specific interactional context, while the FYI 2.0’s IM subscale consisted of six items asking parents about infants’ broader imitative behaviors in everyday situations.
The correlation between the FYI 2.0 SR and the AOSI total score was small, perhaps due to their differences in focus and scale development. As previously noted, the FYI 2.0 is a longer instrument with the SR construct specifically designed to assess the sensory features of infant behavior. This domain of the FYI 2.0 indeed seems unique because sensory features of ASD generally have not been a focus of most early ASD screening or developmental instruments. Many similar instruments, for example, the Modified Checklist for Autism in Toddlers (M-CHAT; Robins et al., 2014), Ages and Stages Questionnaires (ASQs; Bricker et al., 1999), and Communication and Symbolic Behavior Scales (CSBS; Wetherby & Prizant, 2002), largely focus on typical and atypical language development and social-communicative functioning in early childhood. However, recent findings suggest that many, although not all, infants at risk for developing ASD show atypical early sensory behavior (Turner-Brown et al., 2013; Wolff et al., 2019) and this behavior may serve as an early predictor of later ASD diagnosis (Sacrey et al., 2018). Considering a high prevalence of atypical sensory features in ASD (DuBois et al., 2017) and their recognition as important features of ASD diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2013), the sensory dimension would be an important area to assess in future studies.
The FYI 2.0’s SC associations with Language and Socialization related constructs across the MSEL and VABS showed expected patterns of positive associations of moderate to large size based on their similar theoretical interests and measurement objectives. Higher scores in the FYI 2.0 SC construct scores were related to lower RL and EL scores on the MSEL and Communication score in the VABS. However the FYI 2.0 SC subscales showed small associations in the areas of infant functioning such as in Motor and temperament-related Regulation constructs with less clear overlap. For a broad concept like the VABS Socialization domain, three of four SC subscales showed large associations, with a moderate association for the fourth subscale of IM, suggesting that a wide range of social communication skills are required for adaptive social interaction.
In support of our hypothesis, the FYI 2.0 SC construct and subscales (SORC, SAE, and EC) showed moderate to large associations with an affect-related construct, Smile and Laughter. This finding is in line with the literature that indicates that socially-oriented infants tend to smile more often to engage and support social interaction (Kagan, 1989). In regards to Regulation related constructs, the SC SORC subscale showed a moderate association with the Soothability construct. This is consistent with the literature suggesting that infants who are difficult to soothe tend to experience dysregulation of arousal that interferes with social interaction and communication (Olafsen et al., 2012; Mills-Koonce et al., 2012). However, the SC construct and other SC subscales showed small associations for either type of Regulation constructs, suggesting minimal similarities.
Next, the hypothesis that the FYI 2.0 SR construct would associate with Regulation constructs was supported with small correlations. Most SR subscales also showed small associations with Regulation constructs, except for SP, which was moderately associated. This may be because infants who show sensory processing limitations tend to show difficulty modulating their arousal, which can affect their ability to be soothed (Keuler et al., 2011).
Finally, the FYI 2.0 SC and SR constructs and subscales were examined with the Less Related Construct, which consisted of Motor-related constructs from the VABS and MSEL. Although little association was expected, Motor constructs (except for FM) showed moderate to large correlations with the FYI 2.0 SC construct and its SORC, SAE, and EC subscales. The SC IM subscale was moderately related to GM but only weakly related to the FM construct. This may be because the FYI 2.0 IM items are more relevant to gross movements than to subtle FM skills and because FM skills usually do not become fluent until toddlerhood (Piek, 2006). As a part of broader self-regulation development, motor control relies on the development of a voluntary system over a subdominant response (Als, 1989; Kochanska et al., 2000). Development of a network of such subcomponents is foundational to language and social communication development in early childhood (Ruff & Rothbart, 2001). Infants in this study similarly showed that their motor functioning and social-communicative skills were closely linked.
The FYI 2.0 SR construct and subscale correlations with the Less Related Construct were generally small except for a few cases. The SR construct score showed a moderate correlation with GM but showed small associations with Motor constructs. Only RP and RE subscales showed moderate associations with different Motor constructs, again suggesting a link between motor and self-regulation development. In the temperament literature, 4-month-old infants who exhibited high motoric activity and reactivity were more likely to show negative affect and dysregulation a year later (Kagan, 1989; Kagan & Snidman, 1991). It could be that behaviors associated with RP and observational learning of motor skills rely on a broader self-regulation ability (Ferrari, 1996).
This study was a first effort to examine and demonstrate the construct and scale validity of the FYI 2.0 with other instruments along with relevant areas of infant behavior. However, there are study limitations to be acknowledged. Although validity with such instruments in a high-risk sample may serve a practical purpose since these children would be more likely to be examined for ASD diagnosis and developmental status, validity also needs to be examined in low-risk samples to elucidate the extent to which these findings can be generalized. Besides examining construct validity, comparing the FYI 2.0 with another parent-reported screener instead of a professional-administered screener like the AOSI could provide insight that is more accurate to the scale level validity of the instrument. It is possible that associations could have been larger if the FYI 2.0 was compared to another parent-report screener. Other factors that could have contributed to small correlations may have been restricted range, variance, and small sample size (Goodwin & Leech, 2006). Even though the FYI 2.0 construct and subscales generally showed adequate distributions for each of the constructs and total score, some FYI 2.0 subscales, particularly the SR subscales, had restricted range and median values, which could have contributed to small correlations. Moreover, the pattern of associations between measures involving the VABS and the MSEL could have been confounded by the levels of functioning of the children even after using their age-appropriate standard scores for analyses, since these instruments measure developmental skills. Although this study sample was not selected based on ability levels, their high-risk status as siblings of children with ASD suggests compromised levels of functioning for some. According to the diagnostic outcomes detailed in another publication (Lee et al., 2019), approximately 24% of the sub-sample of this study was diagnosed with ASD at 3 years of age. A future study with a larger sample size with varied risk status is necessary to replicate the study findings.
In sum, this study assessed the FYI 2.0’s validity with the MSEL, VABS, IBQ, and the AOSI at the construct and the scale levels in a sample of high-risk infant siblings of ASD. Notably, the FYI 2.0 SC’s associations were generally more robust and larger with related constructs, such as Language, Affect (positive) and Socialization than those with less theoretical overlap. Generally, the SR construct and subscales exhibited smaller associations than the SC construct and its subscales, possibly because the selected instruments included a few sensory items. Instruments differ in their purposes and utilities and this study underscores the importance of utilizing a variety of instruments that capture behavior across a range of relevant domains to gain a more comprehensive understanding of a child’s developmental status. Future research will benefit from identifying salient domains relevant to an ASD (or other developmental disorder) diagnosis, and assure that the testing protocol captures information that fully characterizes all of these domains.
Supplemental Material
Supplementary_table – Supplemental material for Construct validity of the First-Year Inventory (FYI Version 2.0) in 12-month-olds at high-risk for Autism Spectrum Disorder
Supplemental material, Supplementary_table for Construct validity of the First-Year Inventory (FYI Version 2.0) in 12-month-olds at high-risk for Autism Spectrum Disorder by Helen Y Lee, Cheryl Vigen, Lonnie Zwaigenbaum, Isabel M Smith, Jessica Brian, Linda R. Watson, Elizabeth R. Crais and Grace T Baranek in Autism
Footnotes
Author contributions
The following authors have contributed to the manuscript: H.Y.L., University of Southern California, Mrs. T.H. Chan Division of Occupational Science and Occupational Therapy, Los Angeles, CA, USA; C.V., University of Southern California, Mrs. T.H. Chan Division of Occupational Science and Occupational Therapy, Los Angeles, CA, USA; L.Z., University of Alberta, Department of Pediatrics, Alberta, Canada; I.M.S., Dalhousie University/IWK Health Centre, Nova Scotia, Canada; J.B., Bloorview Research Institute, Toronto, Canada; L.R.W., University of North Carolina at Chapel Hill, Division of Speech and Hearing Sciences, Chapel Hill, NC, USA; E.R.C., University of North Carolina at Chapel Hill, Division of Speech and Hearing Sciences, Chapel Hill, NC, USA; and G.T.B., University of Southern California, Mrs. T.H. Chan Division of Occupational Science and Occupational Therapy, Los Angeles, CA, USA.
Compliance with ethical standards
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional boards at each of three sites (Hamilton, Halifax, and Toronto) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Canadian Institutes of Health Research (CIHR) and Autism Speaks Canada. L.Z. was supported by the Stollery Children’s Hospital Foundation Chair in Autism Research. S.B. and I.M.S. were supported by the Joan and Jack Craig Chair in Autism Research.
Informed consent
Informed consents were obtained from all individual participants (parents).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.