
Abstract
Insomnia subtypes have not been characterized in severely affected youth with autism spectrum disorder. We examined indices of clinical impairment (i.e. length of hospital stay, autism severity, nonverbal intelligence quotient, and adaptive and maladaptive behaviors) across insomnia subtypes in 427 psychiatrically hospitalized children with autism spectrum disorder (mean age = 12.8 ± 3.4; 81.3% male). Multivariate analysis with Bonferroni adjustment tested for differences in clinical impairment across insomnia subtypes adjusting for age and sex. Per parent report, 60% (n = 257) of children had at least one form of insomnia. The distribution of subtypes was sleep onset (26.1%, n = 67), sleep maintenance (24.9%, n = 64), early morning waking (4.3%, n = 11), and combined (44.7%, n = 115). There was a significant multivariate effect of insomnia subtypes on clinical impairment (Pillai’s Trace = 0.25, F = 2.78, p < 0.001). Sleep maintenance and early morning waking were associated with longer hospital stays. Early morning waking was also associated with greater autism symptom severity. In general, children with sleep-maintenance or combined insomnias scored lower on adaptive behaviors and higher on maladaptive behaviors. Sleep-maintenance and combined insomnias appear to be more indicative of or consequential for impaired behavioral functioning.
Lay abstract
Insomnia subtypes are not well understood in the most severely affected children with autism spectrum disorder. We examined length of hospital stay, autism severity, nonverbal intelligence quotient, and behavioral functioning across insomnia subtypes in 427 psychiatrically hospitalized children with autism spectrum disorder (mean age = 12.8 ± 3.4; 81.3% male). Per parent report, 60% (n = 257) of children had at least one type of insomnia. The distribution of subtypes was difficulty falling asleep (26.1%, n = 67), difficulty staying asleep (24.9%, n = 64), early morning awakening (4.3%, n = 11), and multiple insomnia symptoms (44.7%, n = 115). Difficulty staying asleep and early morning awakenings were associated with longer hospital stays. Early morning awakening was also associated with higher autism symptom severity. In general, children with difficulty staying asleep or multiple insomnia symptoms scored lower on adaptive behaviors (e.g. communication, self-care, socialization) and higher on maladaptive behaviors (e.g. irritability, hyperactivity, emotional reactivity, and emotional dysphoria). Difficulty staying asleep or having multiple insomnia symptoms appears to be most strongly related to impaired behavioral functioning. Conversely, early morning awakenings may be more closely tied with autism spectrum disorder itself. Further research is needed regarding insomnia subtypes at the severe end of the autism spectrum.
Background
Insomnia is highly common in youth with autism spectrum disorder (ASD) and is often associated with other aspects of clinical impairment (Hollway et al., 2013; Souders et al., 2017). However, the clinical relevance of insomnia subtypes has been overlooked in youth with ASD. In the non-ASD literature, converging evidence suggests that different insomnia subtypes may have different pathogeneses (Bragantini et al., 2019b; van der Meijden et al., 2016) and divergent consequences (Bragantini et al., 2019a; D. J. Taylor et al., 2005). Insomnia symptoms are treatable through various bio-behavioral interventions and thus may be leveraged to improve daytime functioning in youth with ASD. Understanding the clinical correlates of insomnia subtypes in youth with ASD may contribute to the development of targeted treatments.
There are three primary subtypes of insomnia: sleep-onset insomnia (characterized by difficulty initiating sleep), sleep-maintenance insomnia (characterized by difficulty staying asleep), and early morning waking with the inability to return to sleep. Sleep-onset insomnia is the most common in youth with ASD (Richdale & Schreck, 2009; Souders et al., 2009); however, sleep-maintenance insomnia and early morning wakings are highly prevalent in ASD as well (Ivanenko & Johnson, 2008; Richdale & Prior, 1995). Sleep problems are linked with numerous maladaptive behaviors in youth with ASD (Aathira et al., 2017; Anders et al., 2012; Henderson et al., 2011; Rzepecka et al., 2011); however, the unique contribution of insomnia subtypes is not understood. To date, two studies have attempted to identify how clinical features of children with ASD vary across distinct insomnia subtypes. A large cluster analysis yielded two distinguishable “sleep phenotypes”: stable sleepers and unstable sleepers (S. Cohen et al., 2017). The unstable sleepers exhibited shorter sleep duration, earlier wake times, and greater variability in sleep timing. The unstable sleepers also had significantly lower intelligence quotient (IQ) scores and poorer adaptive functioning. A second study conducted an exploratory factor analysis which yielded a sleep-onset factor and a night-waking factor (Krakowiak et al., 2008). Higher scores on both factors were associated with lower cognitive and adaptive functioning. While these studies provide convergent evidence that sleep problems are clinically relevant, the role of distinguishable insomnia subtypes and their overlap is still unclear.
Understanding the importance of distinct insomnia subtypes may be particularly important for youth with ASD who exhibit severe functional deficits, maladaptive behavior, and ultimately require psychiatric hospitalization, as sleep disturbance has been identified as a risk factor for psychiatric hospitalization (Righi et al., 2018). Thus, psychiatric inpatient units specialized for the treatment of youth with ASD provide a unique opportunity to study clinical correlates of insomnia subtypes in an at-risk group. Here, we seek to extend the current literature on insomnia in ASD by evaluating indices of clinical impairment across subtypes of insomnia in a clinical sample of severely affected youth with ASD at the time of admission to psychiatric units.
Method
Participants
The current study is a secondary data analysis of a large data set derived from a multi-site study of psychiatrically hospitalized youth with ASD. Participants were enrolled in the Autism Inpatient Collection (AIC), a study being performed by six inpatient psychiatry units, specialized for the treatment of children with ASD and other developmental disabilities. The methods of the AIC study have been previously published (Siegel et al., 2015). Institutional review board (IRB) approval was obtained at all participating sites of the AIC. Briefly, caregivers were asked whether they would like to participate on the day of admission and provided signed informed consent if they did. There was no monetary compensation for participation in the AIC. Caregivers were often parents but could also be other relatives, foster parents, or caretakers in residential facilities. Youth ages 5–20 years old with a score of 12 or greater on the Social Communication Questionnaire (Rutter et al., 2003) were eligible to participate. Participants in the current analysis had a mean age of 13.0 (SD = 3.4) and were 80.1% male (Table 1). Confirmation of ASD diagnosis was conducted by research-reliable examiners using the Autism Diagnostic Observation Schedule–Second Edition (ADOS-2) (Gotham et al., 2012), Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria, chart review, and inpatient behavioral observation. Only participants with an ADOS-2-confirmed ASD diagnosis and a final clinical diagnosis of ASD are included in the AIC data set (available to approved investigators at base.sfari.org). A total of 427 had complete data on caregiver-reported insomnia symptoms and all indices of clinical impairment.
Unadjusted sample characteristics by insomnia symptom group.
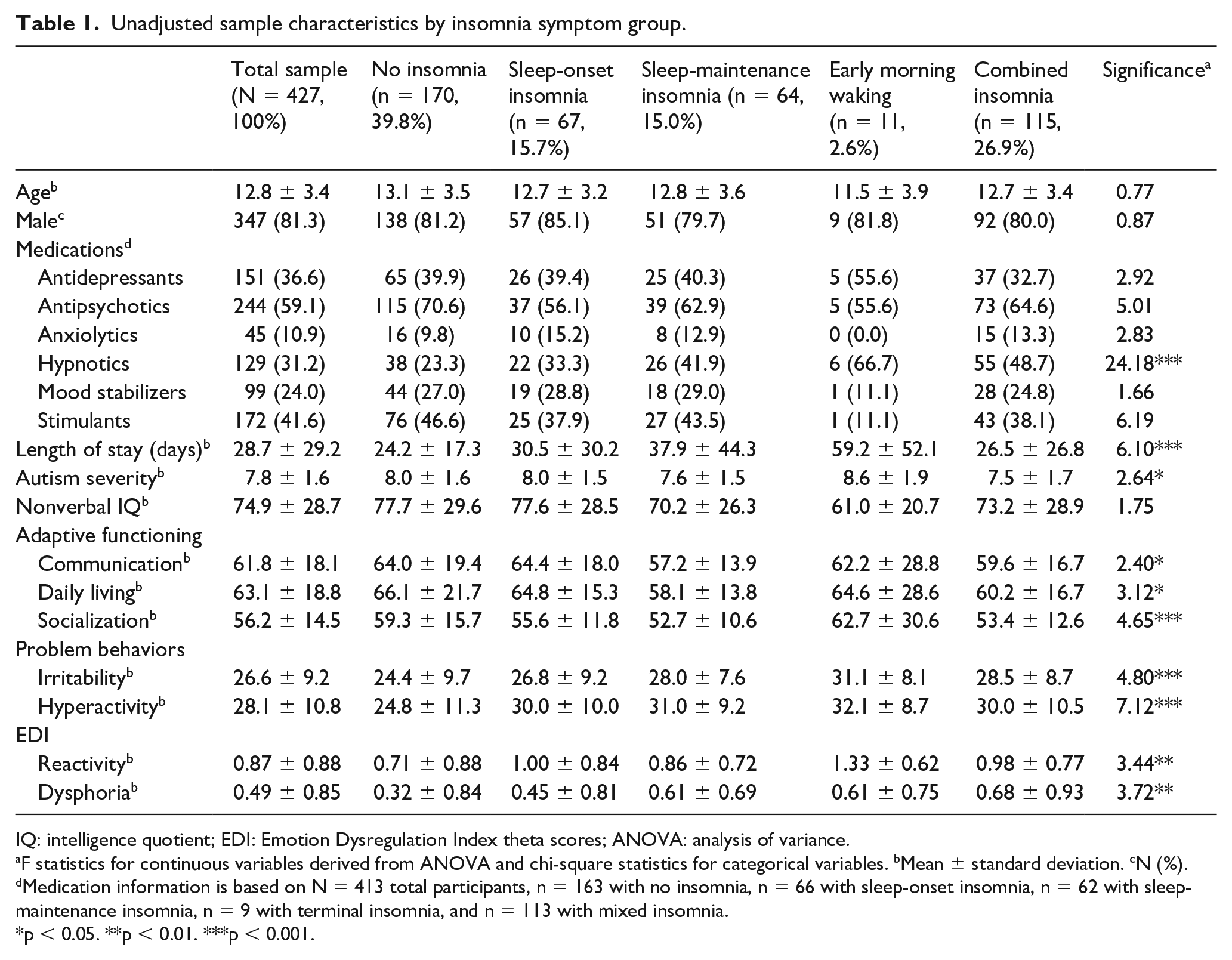
IQ: intelligence quotient; EDI: Emotion Dysregulation Index theta scores; ANOVA: analysis of variance.
F statistics for continuous variables derived from ANOVA and chi-square statistics for categorical variables. bMean ± standard deviation. cN (%). dMedication information is based on N = 413 total participants, n = 163 with no insomnia, n = 66 with sleep-onset insomnia, n = 62 with sleep-maintenance insomnia, n = 9 with terminal insomnia, and n = 113 with mixed insomnia.
p < 0.05. **p < 0.01. ***p < 0.001.
Procedure
Within 10 days of admission, children’s primary caregiver completed a series of questionnaires to measure the presence of suspected insomnia symptoms, adaptive behaviors (i.e. communication, activities of daily living, and socialization), and maladaptive behaviors (i.e. irritability, hyperactivity, emotional reactivity, and emotional dysphoria). During the participants’ hospital stays, trained members of the study staff measure two core features of clinical impairment: autism severity via the ADOS-2 (Gotham et al., 2012) and nonverbal IQ via the Leiter International Performance Scale (Roid et al., 2003). Length of hospital stay was recorded at discharge as an additional indicator of clinical impairment.
Measures
Symptoms of insomnia
At the time of admission on the intake forms, caregivers were asked whether their child had a current significant sleep problem. If they responded yes, they were asked to specify whether the problem was with falling asleep (i.e. a symptom of sleep-onset insomnia), staying asleep (i.e. a symptom of sleep-maintenance insomnia), and/or other (a free response section that allowed caregivers to write in additional problems or information). Under “other sleep problems,” 23 caregivers reported that their child experienced very early morning awakenings (early morning waking). Other write-in responses were less common. For instance, several caregivers reported frequent nightmares or night terrors (n = 11), sleeping all day (n = 9), and sleep apnea or snoring (n = 7). Given the small representation of these other sleep problems, we chose to focus on sleep-onset insomnia, sleep-maintenance insomnia, and early morning waking as the three subtypes for analysis. Caregivers were not restricted to selecting a single sleep problem; thus, participants could have sleep-onset insomnia, sleep-maintenance insomnia, early morning waking, or a combination of insomnia subtypes (i.e. combined insomnia). Although a diagnosis of insomnia cannot be made solely on the basis of parent-reported difficulties with falling asleep, staying asleep, or early morning awakenings, these statements are indicative of the three primary types of insomnia. For readability, symptoms of insomnia are referred to throughout the document as the subtype of insomnia they are symptomatic of (e.g. a child with a symptom of sleep-onset insomnia is described as a child with sleep-onset insomnia).
Core features of clinical impairment
ADOS-2
The ADOS-2 is a semi-structured assessment of communication, social interaction, play, and restricted and repetitive behaviors that allows for the accurate diagnosis of ASD (Gotham et al., 2012). The ADOS-2 produces two subscale scores (social affect and restricted repetitive behaviors), a total score, and a comparison score that indicates autism severity based on population age norms, which ranges from 1 to 10, with 10 indicating most severe. The comparison score was used in these analyses.
Leiter International Performance Scale–Third Edition (Leiter-3)
The Leiter-3 is a nonverbal measure of intelligence, ideal for individuals with developmental delays/disorders (Roid et al., 2003). The instrument utilizes a battery of subtests to measure cognitive function across four dimensions: reasoning, visualization, memory, and attention. Performance across the subtests is converted into a nonverbal IQ that can be compared with traditional IQ values. In the general population, the Leiter-3 has a mean of 100 (SD = 15).
Adaptive behavior
Vineland Adaptive Behavior Scales–Second Edition (VABS-2)
The Parent/Caregiver Rating Form version of the VABS-2 was administered to caregivers (Sparrow, 2011). The current study used the VABS-2 standardized domain scores for communication, self-care (i.e. activities of daily living), and socialization. Standardized domain scores are based on a mean of 100 (SD = 15). Using the VABS-2, caregivers report on the extent to which their child does or does not perform behaviors without needing help or reminders.
Maladaptive behavior
Aberrant Behavior Checklist–Community (ABC-C)
The ABC-C is a 58-item questionnaire, designed to measure the severity of problem behaviors in children and adults with intellectual and/or developmental disabilities (Aman et al., 1995). The ABC-C was used to measure two problem behavior areas that are most common in hospitalized children with ASD: irritability and hyperactivity. The ABC-C asks caregivers to rate the severity of indicators of irritability and hyperactivity, reflecting on the child’s behavior over the last 4 weeks. The Irritability subscale captured externalizing behavior/agitation and demonstrated excellent internal consistency in our sample (Cronbach’s α = 0.998). Normative data for the ABC-C subscales vary by age and gender with irritability means for children ages 5 to 20 ranging from 7.67 (SD = 7.89) to 10.33 (9.58) for males and from 9.18 (SD = 6.95) to 13.07 (10.73) for females (Aman et al., 1985). The Hyperactivity subscale captured impulsivity/non-compliance and demonstrated excellent internal consistency in our sample (Cronbach’s α = 0.998). For the age ranges reflected in our sample, average hyperactivity scores range from 10.38 (SD = 10.77) to 14.27 (SD = 11.70) for males and 10.34 (SD = 8.94) to 18.72 (SD = 13.25) for females.
Emotion Dysregulation Inventory (EDI)
The EDI is a parent-report questionnaire derived from a 30-item bank, designed for measurement of emotion regulation impairment in children with the full spectrum of ASD (Mazefsky et al., 2018). The EDI produces two subscales: Reactivity and Dysphoria. The EDI asks caregivers to rate the severity of emotional reactivity and dysphoria, reflecting on the child’s behavior over the last 7 days. The Reactivity subscale captures the extent to which negative emotional reactions are intense, rapidly escalate, and are sustained. The Reactivity subscale demonstrated excellent internal consistency in our sample (Cronbach’s α = 0.992). Mean Reactivity scores were 0.91 (SD = 0.80) for inpatient youth with ASD and −0.30 (SD = 0.85) for a community sample of youth with ASD (Mazefsky et al., 2018). The Dysphoria subscale captures the absence of positive affect and motivation as well as increased nervousness and negative affect and demonstrated good internal consistency in our sample (Cronbach’s α = 0.805). Mean Dysphoria scores were 0.55 (SD = 0.83) for inpatient youth with ASD and −0.18 (SD = 0.87) for a community sample of youth with ASD.
Statistical analysis
Multivariate linear models were used to evaluate clinical impairment in hospitalized children with ASD across symptoms of insomnia. Indices of clinical impairment included length of hospital stay, autism severity, nonverbal IQ, adaptive behaviors (i.e. communication, activities of daily living, and social interaction), and maladaptive behaviors (i.e. irritability and hyperactivity, emotional reactivity, and emotional dysphoria). Based on caregiver endorsement of insomnia symptoms, participants were categorized as having the subtypes of sleep-onset insomnia, sleep-maintenance insomnia, early morning waking, or combined insomnia. Multivariate analysis was chosen to control for Type I error, given the high number of statistical tests being performed. Bonferroni adjustment further controlled for Type I error when examining pairwise comparisons across symptoms of insomnia. Multivariate analyses were adjusted for age and sex, as sleep problems are known to vary with age and sex in both typically developing and psychiatric populations (Goldman et al., 2012; Zhang et al., 2016). A sensitivity analysis was conducted wherein we adjusted for psychotropic medications (i.e. antidepressants, antipsychotics, anxiolytics, hypnotics, mood stabilizers, and stimulants) at admission, as they are known to impact sleep and are intended to target one or more indicator of clinical impairment. Medications at the time of admission were taken from medical charts and reflect what the inpatient psychiatrist prescribed on the day of admission. The sensitivity analysis was conducted on 413 participants, as 14 participants were missing admission medication data.
Results
Caregivers reported that 60.2% (n = 257) of children had a significant sleep problem (Table 1). Of those with sleep problems, 26.1% (n = 67) had symptoms of sleep-onset insomnia, 24.9% (n = 64) had symptoms of sleep-maintenance insomnia, 4.3% (n = 11) had symptoms of early morning waking, and 44.7% (n = 115) had multiple symptoms of insomnia (i.e. combined insomnia). Of the 115 participants in the combined insomnia subtype, 104 (90.4%) had both sleep-onset and sleep-maintenance insomnia, 1 (0.9%) had sleep-onset insomnia and early morning waking, 5 (4.3%) had sleep-maintenance insomnia and early morning waking, and 5 (4.3%) had all three types of insomnia. There were no age or sex differences across insomnia subtypes. Hypnotics were the only medication class to vary between insomnia groups with a higher proportion of those with sleep-maintenance insomnia, early morning waking, and combined insomnia taking hypnotics relative to those with no symptoms of insomnia (χ2 = 24.18, p < 0.001). There was a significant moderate multivariate effect of insomnia subtype on the indices of clinical impairment (Pillai’s Trace = 0.26, F = 2.76, p < 0.001,
MANCOVA Results.
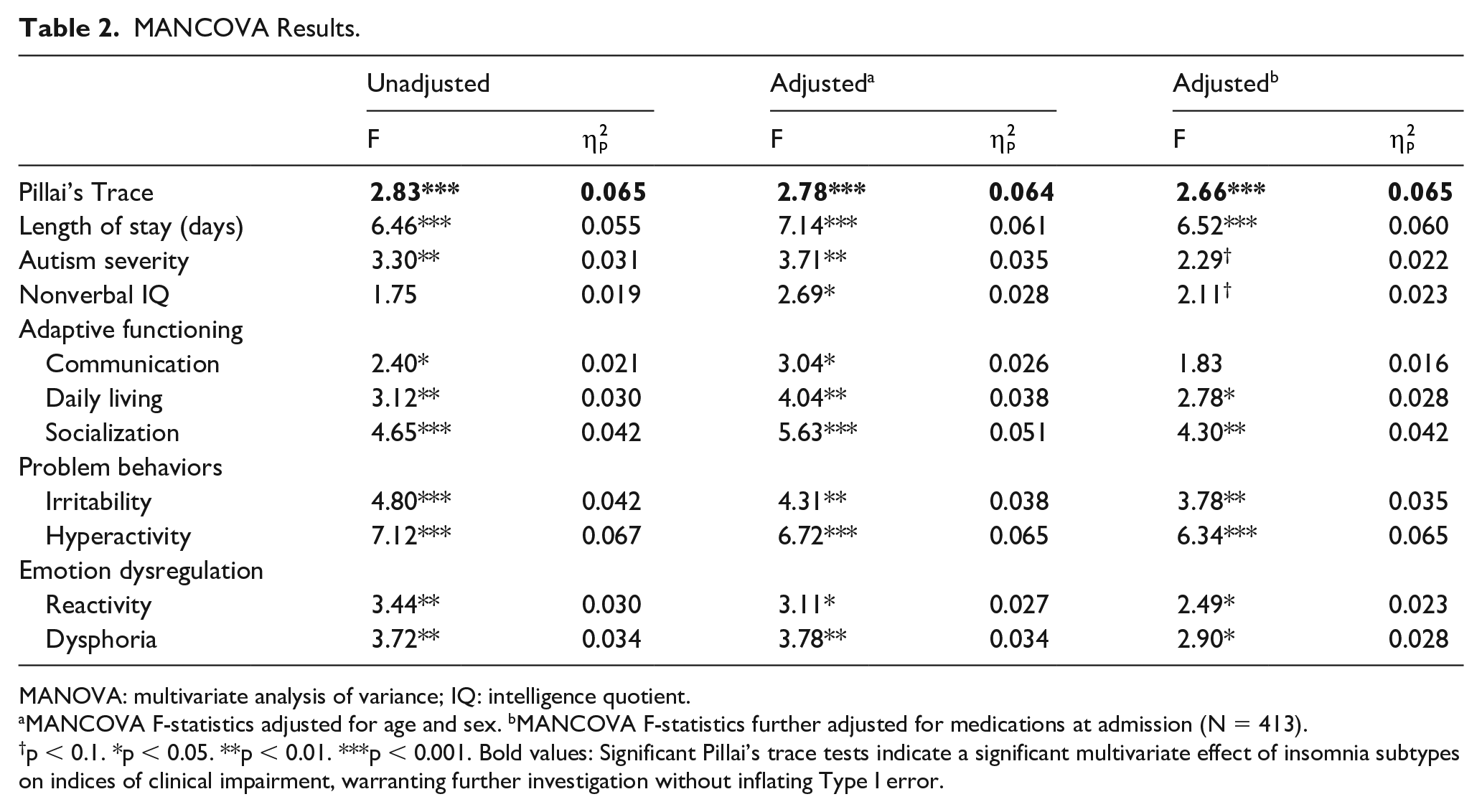
MANOVA: multivariate analysis of variance; IQ: intelligence quotient.
MANCOVA F-statistics adjusted for age and sex. bMANCOVA F-statistics further adjusted for medications at admission (N = 413).
p < 0.1. *p < 0.05. **p < 0.01. ***p < 0.001. Bold values: Significant Pillai’s trace tests indicate a significant multivariate effect of insomnia subtypes on indices of clinical impairment, warranting further investigation without inflating Type I error.
Bonferroni-adjusted pairwise comparisons
Hospital stay and core features of clinical impairment
Length of hospital stay was significantly longer in those with early morning waking relative to those with no insomnia symptoms (Cohen’s D = 1.26), sleep-onset insomnia (Cohen’s D = 1.02), or combined insomnia (Cohen’s D = 1.16) (Figure 1). Length of stay was also significantly longer in those with sleep-maintenance insomnia relative to no symptoms of insomnia (Cohen’s D = 0.49). Early morning waking was also associated with significantly higher ADOS comparison scores (indicating greater autism severity) relative to those with no insomnia symptoms (Cohen’s D = 1.14), sleep-onset insomnia (Cohen’s D = 0.99), sleep-maintenance insomnia (Cohen’s D = 1.15), and combined insomnia (Cohen’s D = 1.07) (Figure 2). There were no significant differences between insomnia subtypes on nonverbal IQ before or after Bonferroni adjustment; however, it should be noted that mean nonverbal IQ was in the range of intellectual disability (i.e. <70) for those with early morning waking only. All other groups had a mean nonverbal IQ ⩾ 70.
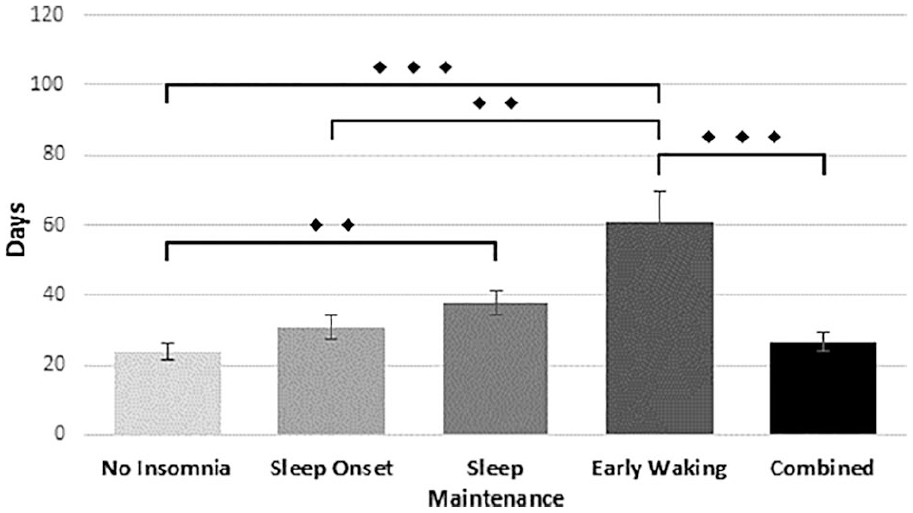
Length of hospital stay by insomnia subtype.
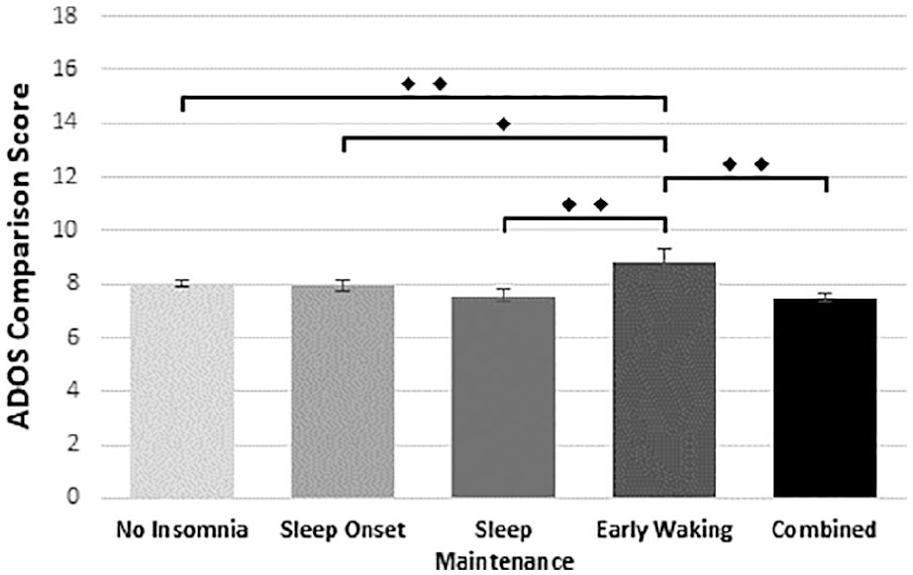
Autism severity by insomnia subtype.
Adaptive behaviors
Children with no insomnia symptoms had better functioning in activities of daily living relative to children with sleep-maintenance insomnia (Cohen’s D = 0.47) and children with combined insomnia (Cohen’s D = 0.48) (Figure 3). Children with no insomnia symptoms also had better functioning in socialization relative to children with sleep-maintenance insomnia (Cohen’s D = 0.36) and children with combined insomnia (Cohen’s D = 0.44).
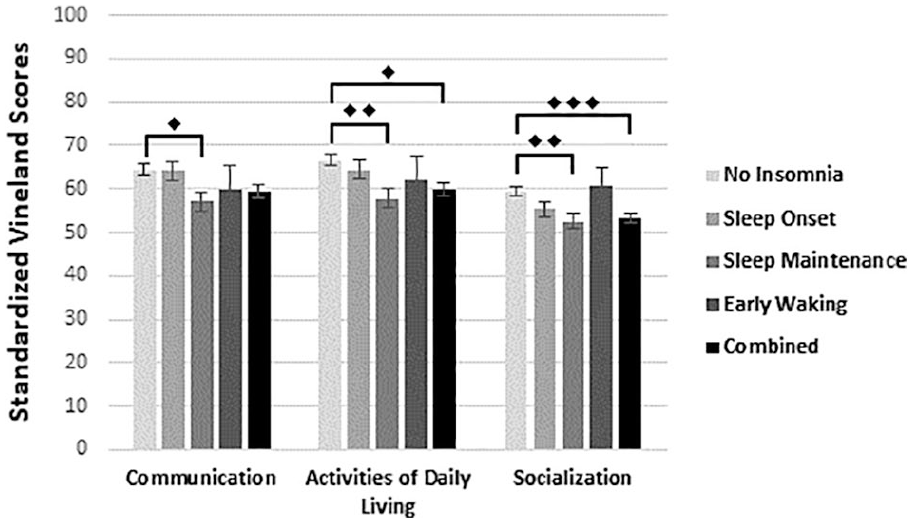
Adaptive behaviors by insomnia subtype.
Maladaptive behaviors
Irritability was significantly higher in children with combined insomnia relative to children with no insomnia symptoms (Cohen’s D = 0.41) (Figure 4). Hyperactivity was significantly higher in children with sleep-onset insomnia (Cohen’s D = 0.45), sleep-maintenance insomnia (Cohen’s D = 0.55), and combined insomnia (0.45) relative to children with no insomnia symptoms. Emotional dysphoria was also significantly higher in children with combined insomnia relative to children with no insomnia symptoms (Cohen’s D = 0.44). There were no differences in emotional reactivity between the insomnia subtypes.
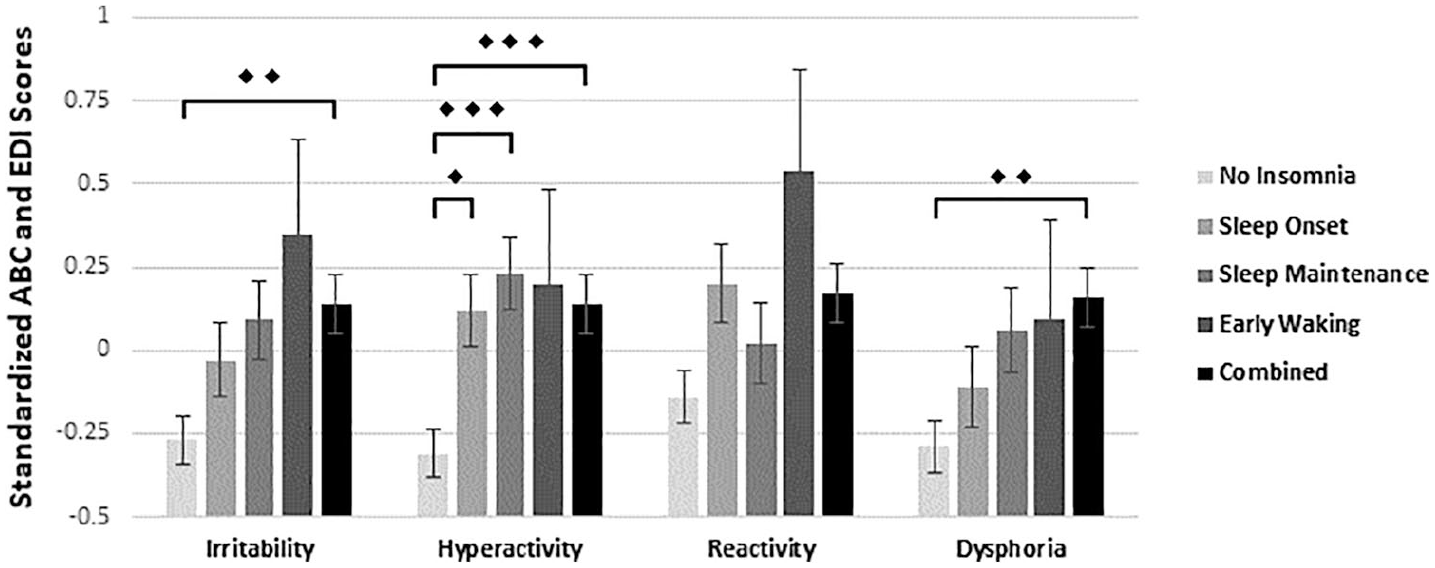
Maladaptive behaviors by insomnia subtype.
Adjusting for medications
Many results were robust to adjustment for antidepressants, antipsychotics, anxiolytics, hypnotics, mood stabilizers, and stimulants at the time of admission (Table 2). After adjustment for medications, previously statistically significant differences in autism severity and adaptive functioning in communication between insomnia groups were no longer present. Specifically, autism symptom severity was no longer significantly greater in children with early morning waking relative to all other groups, and adaptive functioning in communication was no longer significantly lower in children with sleep-maintenance insomnia relative to children with no insomnia symptoms.
Discussion
The current study is the first to evaluate the clinical relevance of specific insomnia subtypes in a sample of primarily severely affected youth with ASD. Insomnia symptoms were common, with just under two-thirds of the sample having parent-reported significant difficulty with falling asleep (i.e. sleep-onset insomnia), staying asleep (i.e. sleep-maintenance insomnia), early morning waking, or a combination of sleep problems (i.e. combined insomnia). There was a moderate effect of insomnia subtype on the indices of clinical impairment (
Our results are largely consistent with a growing body of evidence supporting the connection between poor sleep and both poor adaptive functioning and increased maladaptive behavior (Souders et al., 2017). Moreover, insomnia can contribute to chronically lower sleep duration which is a known risk factor for poor adaptive functioning and increased internalizing and externalizing behaviors in youth with ASD (Sikora et al., 2012; M. A. Taylor et al., 2012).
The particular importance of sleep maintenance has been identified in non-ASD pediatric samples. For instance, sleep-maintenance insomnia has been associated with greater risk for psychiatric and behavioral problems (Belanger et al., 2018; Kouros & El-Sheikh, 2015; McGlinchey et al., 2017; Mesman et al., 2017; Nrugham et al., 2008). In a large epidemiological sample of non-ASD adults, combined insomnia has been associated with greater depression relative to all other insomnia subtypes (D. J. Taylor et al., 2005), and combined insomnia symptoms have been related to more severe levels of daytime impairment relative to those with single insomnia symptoms in primary care outpatient adults (Leger et al., 2010).
Sleep-maintenance insomnia and combined insomnia may act on behavioral functioning by dysregulating central nervous system processes involved in executive functioning (Kuula et al., 2015; Philbrook et al., 2017) and/or dysregulating peripheral nervous system processes relevant to the stress response and emotion regulation (El-Sheikh et al., 2007). In addition, studies have shown that combined insomnia is the most stable form of insomnia over time, followed by sleep-maintenance insomnia (Pillai et al., 2015). Thus, if insomnia is causally related to clinical impairment, the chronic insult of combined insomnia and sleep-maintenance insomnia may accumulate over time.
The increased clinical significance of sleep-maintenance insomnia may also be due to the greater impact of sleep-maintenance insomnia on daytime sleepiness. A large study of non-ASD adults found that sleep-maintenance insomnia more than doubles the likelihood an individual will experience excessive daytime sleepiness (Hara et al., 2011). Daytime sleepiness has been associated with increased hostility in youth with ASD (Mazurek & Sohl, 2016) and with greater problem behavior in children with mild ASD symptoms (Lindor et al., 2019). Daytime sleepiness has been identified as more common in youth with ASD relative to healthy controls (Allik et al., 2006; Baker et al., 2013; Miano et al., 2007), which may be due to the higher prevalence of insomnia symptoms in this population or a decreased ability to cope with insomnia. Daytime sleepiness has also been shown to moderate the strength of association between sleep loss and overall cognition in neurotypical samples, suggesting that insomnia symptoms may show a stronger association with impairment in cognitive functioning when sleepiness is high (Lowe et al., 2017). Cognitive control is necessary for adaptive functioning, behavior regulation, and emotional control, and is already compromised in many youth with ASD (Craig et al., 2016; Mazefsky & White, 2014). Thus, fragmented sleep in those with sleep-maintenance insomnia and subsequent daytime sleepiness may act on neural vulnerabilities already present in many ASD youth and contribute to impaired behavioral functioning. Unfortunately, our study lacks an adequate measure of daytime sleepiness and so we were unable to test this hypothesis.
Treatment options for sleep-maintenance insomnia are somewhat limited and may be particularly important to examine. For instance, although melatonin is the most accepted pharmacological treatment for sleep problems in ASD, its efficacy for treating sleep-maintenance problems is widely contested (Bruni et al., 2015) and the relative efficacy for individuals at the severe end of the autism spectrum is not established. Limited research does suggest that behavioral intervention, with the inclusion of parent training, has successfully improved sleep-maintenance problems in children with ASD and co-morbid intellectual disability (Kirkpatrick et al., 2019). Greater attention toward behavioral interventions that involve family members and break counterproductive routines may be particularly helpful.
Substantially less is known about early morning waking and its treatment relative to other insomnia subtypes. Despite frequent anecdotal reports of its prevalence and disruptiveness to caregivers, there is a dearth of literature regarding early morning waking in ASD. In the current study, early morning waking was associated with greater autism severity and longer hospital stays. This finding may suggest that early morning waking may be an area for particular clinical focus. However, this finding should be interpreted with caution as our sample of those with early morning waking was small and these results were no longer significant after adjusting for medications, which may have been due to greater use of medication for those with greater autism severity. It should also be noted that the prevalence of early morning waking may be underestimated in our sample as our caregiver survey did not ask specifically about early morning awakenings. Instead, parents volunteered this as an “other sleep problem” using a free response question format. Future studies should seek to oversample for early morning waking to better understand how it may contribute to or be reflective of clinical features in youth with ASD. Symptoms of insomnia and indices of clinical impairment may reflect underlying central nervous system dysfunction. For instance, in separate lines of research, abnormal functional connectivity (typically under- or hypo-connectivity) in various neural regions has been identified in patients with ASD versus controls (Xu et al., 2019) and in patients with insomnia versus controls (Dai et al., 2020). Similarly, abnormal functional connectivity has been associated with worse adaptive functioning (Denisova et al., 2017), problem behaviors (Ibrahim et al., 2019; Wang et al., 2019), and emotion regulation (Kleinhans et al., 2016) in those with ASD. Thus, interconnections between insomnia symptoms and other domains of impairment may be due to pre-existing pathology in the central nervous system. Longitudinal studies of insomnia, clinical impairment, and neural mechanisms are needed to evaluate temporal precedence among these factors.
Behavioral and environmental factors may also help us to understand the etiology of insomnia subtypes in youth with ASD. Sleep-onset associations that help an individual fall asleep at bedtime but which cannot be maintained throughout the night may result in disrupted sleep. Understanding sleep-related behaviors and the home sleep environment may provide a more robust depiction of factors that contribute to sleep problems in severely affected youth with ASD.
The current study had several note-worthy limitations. First, we were unable to test several proposed explanations for our pattern of results, as the current study is a secondary analysis of a data set, not specifically designed to examine insomnia and other aspects of sleep health. As such, we have no measures of sleep duration, circadian factors, daytime sleepiness, or sleep apnea in this sample. Information regarding the severity of sleep problems and the extent to which these problems meet diagnostic criteria for insomnia are also unknown and we lacked objective sleep data. Finally, systematic tracking of insomnia symptoms across hospital stay may have shed light on the association between early morning waking and longer length of hospital stay. Future studies should strive to objectively measure habitual sleep data via actigraphy or other objective methods and use a 24-h approach to fully capture not only sleep problems but rest-activity rhythms and daytime sleeping. In addition, polysomnography assessments may provide useful information regarding how individual differences in sleep architecture influence patterns of associations between insomnia symptoms and indices of clinical impairment. As polysomnography studies are particularly challenging with this severely affected individuals with ASD, novel approaches to examining electroencephalography during sleep should be pursued for this population.
Sleep apnea and other medical conditions may also explain the pattern of results seen here. Sleep problems are common in those with obstructed breathing during sleep (Ong & Crawford, 2013), restless leg syndrome (Turk et al., 2018), epilepsy (Nunes & Bruni, 2015), chronic pain (de la Vega et al., 2018), and many other medical issues. Some medical issues, such as sleep apnea, have been shown to have consequences for clinical outcomes such as adaptive functioning (Perfect et al., 2013), challenging behavior (Tachibana et al., 2016; Xanthopoulos et al., 2015), and emotional processing (Kheirandish-Gozal et al., 2014). The role of medical comorbidities, including sleep apnea, should be evaluated in future studies to understand their contribution within the framework of insomnia subtypes and clinical impairment in youth with ASD.
The limitations of this study were offset by several strengths. The current study had unique access to a severely affected population of youth with ASD who are often difficult to recruit for studies from the community and have been shown to be underrepresented in treatment studies in ASD (Stedman et al., 2019). In addition, severely affected individuals with ASD are often not included in clinical research due to their increased behavioral problems and decreased compliance with research procedures. Thus, severely affected individuals with ASD are not well understood despite being among those most in need of help. The current sample is also deeply characterized and each participant has a clinical diagnosis of ASD confirmed by an ADOS assessment. Finally, a majority of studies in this area have treated sleep problems globally rather than looking at the relative contribution of different insomnia subtypes. The current study contributes to the broader literature by suggesting that sleep-maintenance insomnia may be particularly consequential for or indicative of clinical impairment. Longitudinal and intervention research is needed to determine whether insomnia symptoms contribute to or are caused by indices of clinical impairment or, conversely, are reflective of neural or physiological abnormalities that drive clinical impairment. Finally, additional research is needed to examine the relative efficacy of various insomnia treatment approaches across insomnia subtypes and various autism phenotypes.
Conclusion
The current study evaluated subtypes of insomnia in a group of primarily severely affected, hospitalized children with ASD in relation to indicators of clinical impairment. Children with sleep-maintenance insomnia exhibited significantly more impairment in adaptive functioning, challenging behaviors, and emotional dysphoria while children with early morning waking exhibited significantly greater autism severity and longer hospital stays. Interventions targeting sleep-maintenance insomnia may have particular clinical utility and may help to elucidate whether sleep-maintenance problems are causally related to impairment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Simons Foundation and the Nancy Lurie Marks Family Foundation.