
Abstract
Navigating various systems, resources, and supports available for families of children with autism spectrum disorder is challenging. Family navigation is a potentially important support system for families of children with autism spectrum disorder. Family navigators are professionals who engage with families to enhance access to early identification and intervention services via shared navigation plans that help meet the family’s priorities and goals when navigating systems of support. Systematic processes and tools facilitating the development of a shared navigation plan with families following diagnosis are currently limited. This short report describes product development of the Family-Centered Autism Navigation using quality improvement methods including Lean Launch and qualitative methodology.
Lay abstract
When a parent learns of their child’s autism diagnosis, they may be overwhelmed, confused, and frustrated. Family navigation services are designed to improve access to care. While these services are a promising intervention to enhance well-being and developmental outcomes, there are limited tools that can systematically facilitate the development of a shared navigation plan that prioritizes the concerns of the family. The Family-Centered Autism Navigation semi-structured interview guide is designed for family navigators to triage and prioritize caregiver’s needs to coordinate and navigate systems of care after learning of their child’s autism spectrum disorder diagnosis. The goals of the Family-Centered Autism Navigation interview are to (1) identify family and child strengths; (2) identify family/caregiver concerns regarding navigation of services and systems following their child’s diagnosis of autism; (3) measure change in caregiver knowledge, ability and skill as it relates to understanding, remembering, and evaluating information they receive; and (4) assist with the development of a shared navigation plan. When using the Family-Centered Autism Navigation guide, family navigators and caregivers co-create a family-centered, prioritized action plan that supports and prepares caregivers as they navigate systems of care. This short report describes the development process of the Family-Centered Autism Navigation semi-structured interview guide. We utilized brief interviews (n = 42), expert feedback (n = 13), and quality improvement strategies (n = 2 family navigators) to develop the questions and determine the usability of the Family-Centered Autism Navigation interview in practice.
Families of children with autism spectrum disorder (ASD) report challenges navigating various systems of care and locating available resources (e.g. Karst & Van Hecke, 2012). Family navigation approaches help families access and understand systems of care via research-based procedures, models, and tools (Broder-Fingert et al., 2020; Feinberg et al., 2016; Maternal and Child Health Research Program, 2014). Family navigators (FNs) are professionals with lived experience of having a child with ASD or special healthcare needs who engage families to enhance access to early identification and intervention services.
Emerging research describes important components of family navigation (Feinberg et al., 2016) and shows FNs increase service initiation and ongoing engagement (Feinberg et al., 2016). However, research on the development of family navigation interventions primarily focuses on FN training with less attention paid to the protocols and products used by FNs to facilitate or enhance the family navigation process. This short report describes the product development process of the Family-Centered Autism Navigation (Family CAN) semi-structured interview. The Family CAN is a comprehensive interview guide designed for FNs to use while working with families of children recently diagnosed with ASD. Specifically, it helps FNs develop a family-centered, prioritized action plan to support families as they navigate systems of care.
Methods
Design
The Family CAN was developed in three stages utilizing Lean Launch (Blank & Dorf, 2012) and qualitative methodology (i.e. online survey and telephone interviews), and Plan, Do, Study, Act (PDSA) quality improvement methods (Reed & Card, 2015).
Participants
Forty-two participants completed discovery interviews in Stage 1 (Lean Launch). Participants in Stage 1 consisted of professionals (n = 25), parents (n = 12), family members of Children with Special Health Care Needs (CSHCN; n = 4), and self-advocates (n = 1). In Stage 2 (qualitative methods), 13 expert participants completed an online survey assessing question clarity, importance, and emotional tone. Twelve of the 13 expert participants completed a follow-up phone interview. During Stage 3 (PDSA cycles), two FNs utilized the Family CAN with four families whose child was recently diagnosed with ASD. See Table 1 for participant demographics at each stage of the current project.
Demographic information of participants in Stages 1–3.
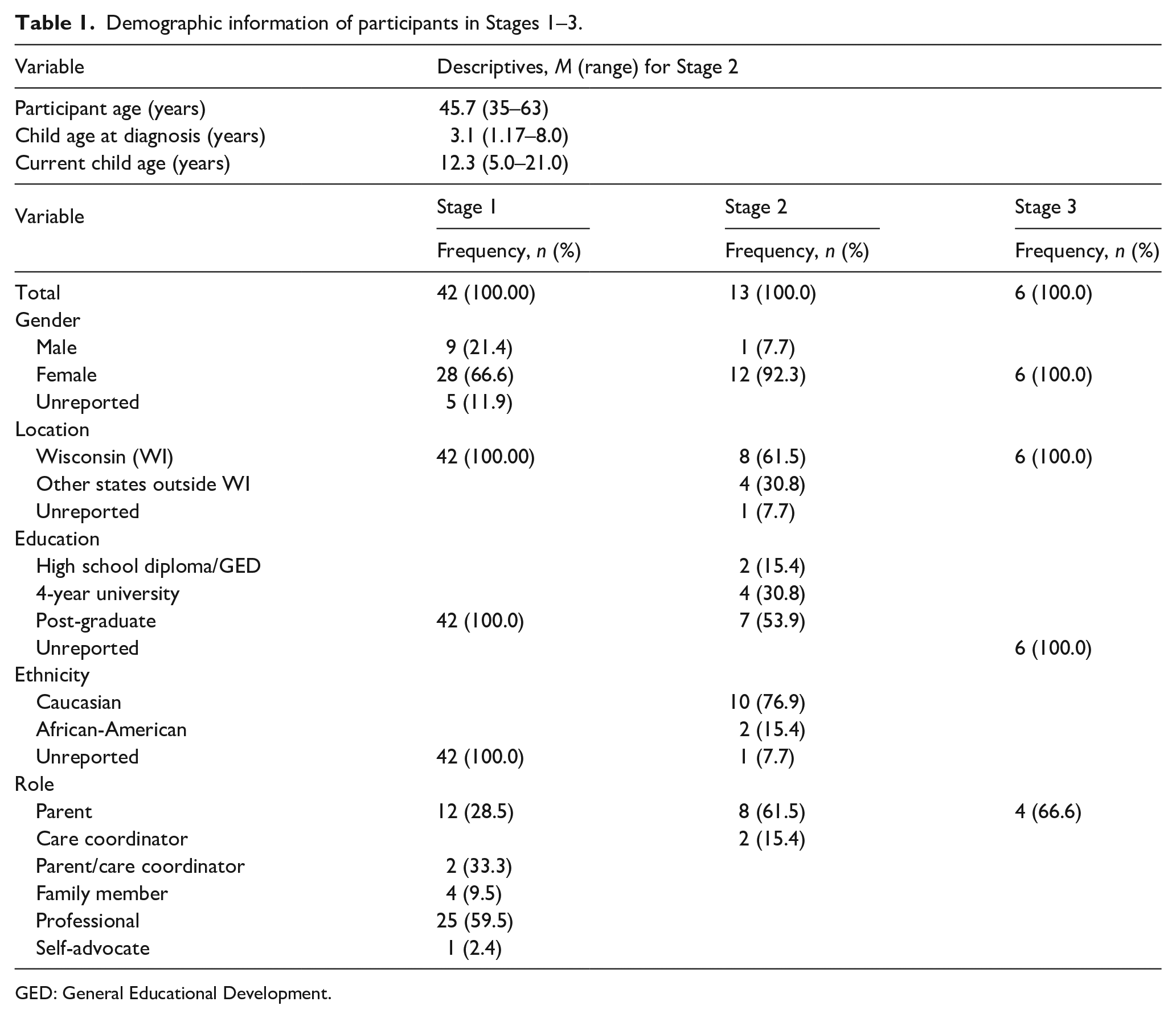
GED: General Educational Development.
Revisions to Family CAN questions based upon expert feedback.
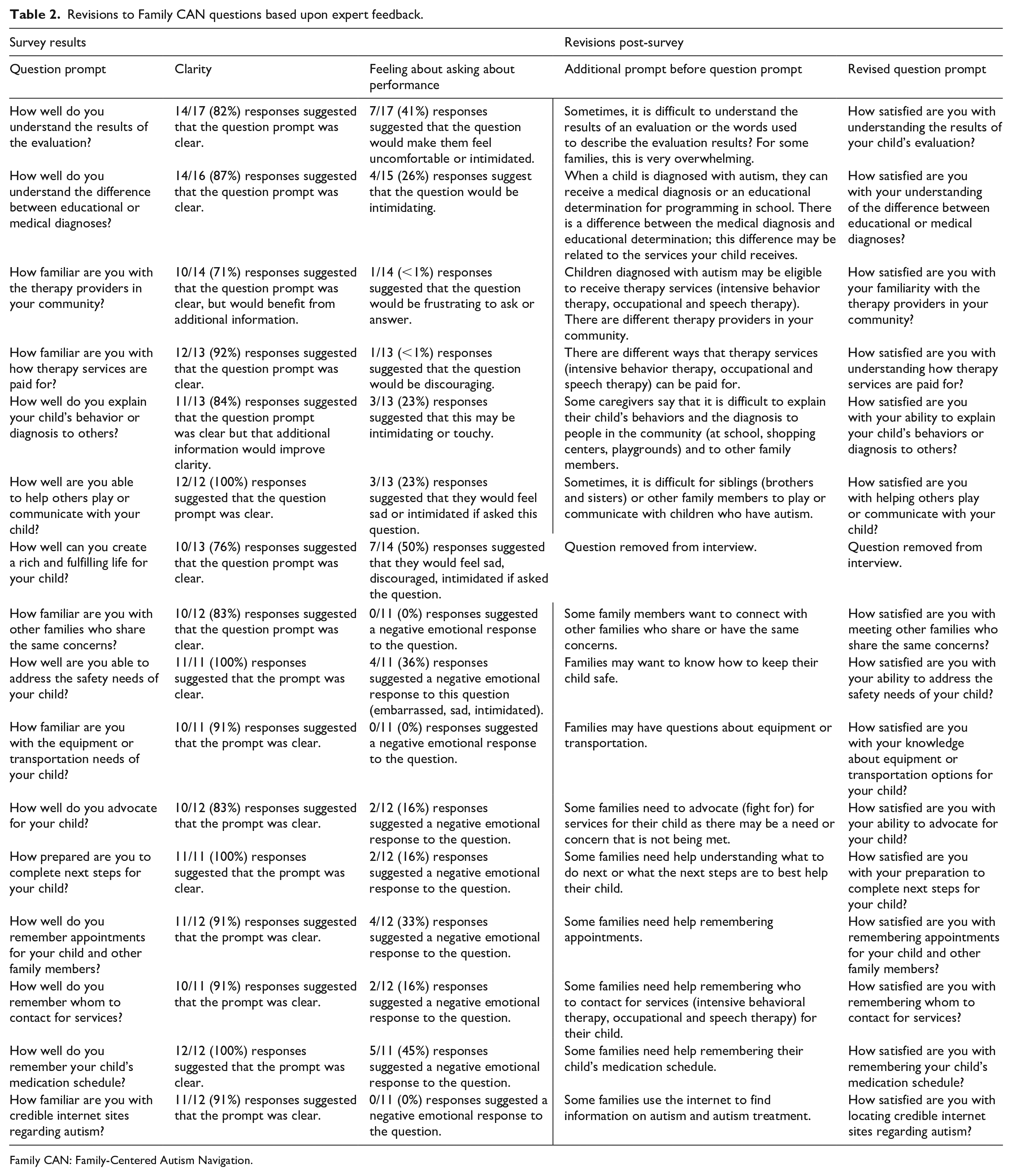
Family CAN: Family-Centered Autism Navigation.
Procedure
This project was deemed exempt as a quality improvement project by the Institutional Review Board at a University in the Midwest and did not require IRB approval.
Stage 1: Lean Launch methodology—discovery interviews
The purpose of the Lean Launch methdology is to gather customer and marketplace feedback quickly resulting in meaningful products and solutions (Udacity, n.d.). Discovery interviews are a quick systematic method to determine areas of specific need (Blank & Dorf, 2012). The interviews start with a general inquiry about pressing concerns with follow-up questions based upon participant responses. The initial prompt was, “What are your most significant challenges?” Follow-up questions assessed what makes this challenge so pressing and identified ways the participants addressed the challenge. Interview questions were hypothesis-driven and based on research conducted with caretakers of CSHCN. The questions facilitated conversation but did not suggest solutions.
Interviews and five feedback sessions with a cohort of discovery teams were used to provide feedback on our team’s minimal viable product (MVP), a basic product with enough features allowing for consumer evaluation (Udacity, n.d.). The discovery interview team consisted of an academic lead, a mentor, and an occupational therapy graduate student. Interviews were conducted during a 5-week period, and the individual interviews lasted between 20 and 90 min depending on interviewee responsiveness. After each interview, two team members reviewed and compared notes to ensure that the participants’ comments were accurately documented.
Stage 2: online survey and phone interview
The discovery team developed a semi-structured interview after a thorough review of the interview notes. Based on research by Pizur-Barnekow et al. (2011) and a client-centered philosophy (Law et al., 1996), the team developed initial Family CAN interview questions. Questions were evaluated by experts (i.e. parents of children diagnosed with ASD and care coordinators), via an online survey and a follow-up phone interview. The survey displayed the question stem, and the experts responded to open-ended question that asked them to (1) comment on the clarity of the stem (What does this question mean to you?), (2) comment on the importance of the stem (How important is this question?), and (3) reflect and report on their emotions when reading the question (How would it feel if you were asked about your performance or the importance of the question?). Constant comparative methods were used to categorize the experts’ narrative responses (Glaser, 1965).
Stage 3: PDSA cycle
Project leads on a state system improvement grant invited FNs at three sites to use the Family CAN during family navigation appointments. Two FNs at one site decided they would use the tool during family navigation appointments. FNs received the interview guide and manual before participating in a 1-h training on use of the Family CAN. The FNs used the interview guide with four families with children recently diagnosed with ASD. Quality improvement methods using PDSA cycles determined if the FNs would adopt the Family CAN as a part of their practice (Reed & Card, 2015). FNs responded to the following questions during the PDSA cycle: (1) What do you hope to learn from this cycle? (2) How will you know the changes are an improvement? and (3) What do you predict will happen?
Data analysis
The project team conducted post-interview debriefings and informal analysis of data collected during Stage 1 interviews. Written comments for Stage 2 were coded and analyzed by a team of three researchers (two graduate students and the principal investigator (PI)) using constant comparative methods (Glaser, 1965) over a 2-month period. The team coded written comments into the following categories: the participants identified if the question stem is clear or unclear, the participants restated the meaning of the question, the participants identified an emotional response to the questions, the participants recommended rewording of the question, or the participants’ responses required additional coding. Subsequently, two members of the research team met to review comments requiring additional coding. This team determined if the comments were generally positive remarks about the question stem, negative remarks about the question stem, an opinion statement, or unclear/ambiguous. The study team revised the Family CAN interview questions based upon the coded feedback from the experts.
Results
Stage 1: discovery interviews
Team feedback during Stage 1 indicated that FNs needed a product or tool to systematically identify challenges that caregivers experience upon learning of their child’s ASD diagnosis. The Stage 1 process resulted in Version 1 of the Family CAN interview questions (17 items) which were then evaluated in Stage 2 by parents of children diagnosed with ASD and care coordinators.
Stage 2: online survey and phone interviews
Participants evaluated question stems. The authors combined categories to represent that the respondents understood the question and added questions based upon survey and interview results. The final interview contained 29 questions.
Stage 3: PDSA cycle
The FNs who used the Family CAN in practice were parent-peer specialists employed by a parent-run support organization. FNs were trained to support caretakers of CSHCN, and they make intervention referrals based upon family needs. The FNs administered a hard copy of the interview in either single or multiple sessions, depending upon family communication style and detail of responses. The FNs indicated they would adopt the Family CAN in their practice and use the interview after an initial introductory visit designed to establish rapport with the family. Some caregivers found the rating system difficult, and the FNs recommended using a shorter Likert-type scale (i.e. 1–5) or using pictures or symbols instead of numbers.
Conclusion
The Family CAN semi-structured interview was developed using Lean Launch methodology, expert review, and PDSA cycles. This method of product design and development is a systematic practice resulting in a tool aimed at enhancing FN services following an ASD diagnosis. Comprehensive evidence-based FN services consist of key components including individually tailored, family-centered care coordination (Broder-Fingert et al., 2020). The Family CAN may fit well within a comprehensive FN program particularly when supporting families following an ASD diagnosis.
While these data suggest that FNs understand the interview and would use it to aid caretakers in navigating systems of care, the current project is limited and does not prove that implementation of the Family CAN leads to effective system navigation. Further, FN is designed to help underresourced families navigate systems of care, but our participants were educated and White and do not represent perspectives from target populations. Non-White or less educated families may find the Family CAN less helpful than the current population. Relatedly, the Likert-type responses were challenging for several participants and therefore adapted; further adaptation may be needed for low-resource/education populations. Another limitation is that the average age post-diagnosis of children whose parents participated in Stage 2 of the study was 12.3 years, suggesting that findings may be affected by recall bias.
Future research should investigate the usability and effectiveness of the Family CAN in underserved and underrepresented populations navigating systems of care to strengthen the validity of the interview with more diverse populations. More research is needed to refine the Family CAN with target populations followed by longitudinal controlled trial data to determine if implementation of the Family CAN leads to better system engagement outcomes for underserved families. Specifically, refinement of the rating system through systematic research may enhance the tool’s usability across a variety of populations.
Footnotes
Acknowledgements
The authors thank the National Science Foundation, Southeastern Wisconsin I-Corps Site: Enhancing Regional Technology Commercialization, and the HRSA funded Autism CARES State Systems Grant Program. We also thank Natalie Froemming and Alexandria Hagen for their assistance on this project.
Compliance with ethical standards
The current study utilized human participants and obtained informed consent from participants within the online survey. Participants were required to indicate that they were at least 18 years old and were participating voluntarily and no one would be penalized if they chose not to participate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding for Stage 1 of this study.