
Abstract
All 50 US states have enacted mandates requiring insurers to cover autism-related services. We assessed whether and to what extent variation in generosity of state insurance mandates has been associated with rate of growth in the health workforce for children with autism spectrum disorder: including board-certified behavioral analysts, child psychiatrists, and pediatricians. Drawing data from the National Conference of State Legislatures and Area Health Resource Files, we evaluated eight mandate policy features, utilizing a fixed-effect longitudinal regression framework to examine their relationships with workforce growth during a 15-year period (2003–2017) over which 44 states enacted a mandate. Aspects of mandate generosity included ages covered, spending caps, and types of services covered. We found that mandate generosity was closely associated with the magnitude of increase in supply of board-certified behavioral analysts and—to a lesser extent—child psychiatrists. States with the most generous mandates would be expected to have 39% more board-certified behavioral analysts and 17% more child psychiatrists in 2017, compared to states with least generous mandates. We found no association between mandate generosity and supply of pediatricians. Collectively, our results suggest that the degree of generosity afforded by mandates may be as important as the passage of mandate legislation itself for encouraging workforce growth.
Lay abstract
To improve access to health services for children with autism spectrum disorder, US states have passed laws requiring health insurers to cover autism-related care, commonly known as state insurance mandates. However, the features of mandates differ across states, with some state laws containing very generous provisions and others containing very restrictive provisions such as whether the mandates include children aged above 12 years, whether there is a limit on spending, and whether there are restrictions on the types of services covered. This study examined the relationship between generosity of mandates and growth in the health workforce between 2003 and 2017, a period during which 44 states passed mandates. We found that states that enacted more generous mandates experienced significantly more growth in board-certified behavioral analysts who provide behavioral therapy as well as more growth in child psychiatrists. We did not find differences in the growth of pediatricians, which is a less specialized segment of the workforce. Our findings were consistent across eight different mandate features and suggest that the content of legislation may be as important as whether or not legislation has been passed in terms of encouraging growth in the supply of services for children with autism spectrum disorder.
Introduction
Over one million children under the age of 18 years in the United States have autism spectrum disorder (ASD) (CDC, 2018). While characteristic features of ASD—such as social cognitive impairment and restrictive/repetitive behaviors (Seltzer et al., 2003)—vary substantially cross affected children, most have significant clinical needs: children with ASD often require physical and behavioral health care (Chiri & Warfield, 2012), as well as social and cognitive developmental supports (Benevides et al., 2016). With regard to physical and behavioral health care, comorbid conditions such as attention deficit hyperactivity disorder, epilepsy, and depressive disorder are prevalent among children with ASD (Gurney et al., 2006; Moseley et al., 2011; Simonoff et al., 2008). For example, over 10% of children with ASD have epilepsy (Viscidi et al., 2013). In terms of developmental supports, early intervention strategies often include applied behavioral analysis (ABA), occupational therapy, and other school-based supports (Case-Smith & Arbesman, 2008; Hyman et al., 2020; Novak & Honan, 2019).
Collectively, the diverse physical and behavioral health needs of children with ASD often require a team-based medical home model of care (Todorow et al., 2018). One recent estimate places the average cost of these collective services at US$50,000 per year among children with ASD without intellectual disability (ID) and almost US$90,000 per year among those with ID (Buescher et al., 2014). ABA alone can cost as much as US$46,000 per year or a rate of US$120 per hour (Special Learning Inc., 2020). Over the past several decades, a significant portion of these costs have been borne out-of-pocket by families (Callaghan & Sylvester, 2019a; Parish et al., 2015). Furthermore, the paucity of ASD-related services covered by insurance on average appears related to significantly reduced parental employment, due to caregiving demands on family members (Maich et al., 2019). One recent study found that children with ASD are 9% less likely to have both parents employed and that family earnings of children with ASD are 28% lower compared to family earnings of children with no health limitations (Cidav et al., 2012). A separate study found that both mothers and fathers of children with ASD average fewer hours worked, and the reduction in hours for mothers may be larger for children with corresponding ID (McCall & Starr, 2018).
One state policy response to reduce the financial burden of ASD on families has been legislation requiring health insurers to provide coverage for autism-related services. As of 2019, all states have enacted such policies (National Conference of State Legislatures, 2019). These laws, known as state insurance mandates, have led to modest increases in autism-related healthcare utilization and spending. Barry and colleagues (2017) found that mandates have been associated with a 3.4% increase in monthly service use and a US$77 increase in monthly health expenditure (Barry et al., 2017). Similarly, found average annual spending on ASD-related services increased by US$912 following mandate enactment. However, evidence also suggests that out-of-pocket spending has increased following the introduction of mandates, though the share of out-of-pocket spending has declined (Candon et al., 2019). In addition, the introduction of mandates has correlated with a modest increase in the supply of autism-related health care: McBain, Cantor, and colleagues (2020) found that mandates were associated with a 16% increase in board-certified behavioral analysts (BCBAs) who provide ABA, and 7% increase in child psychiatrists. From a classical economic perspective, lowering the financial burden of care to families resulting from mandates should lead to greater care seeking and higher provider wages in the short run which, in turn, stimulates providers to enter the market or move to states with mandates in the long run (Dave & Fernandez, 2015; Mankiw, 2017). This supply-side effect of expanded insurance coverage has been observed in other contexts such as Medicaid expansion and implementation of the Children’s Health Insurance Program (He & White, 2013; Hill et al., 2019).
While the average effect of state-level mandates on the supply and demand of autism-related services has been modest, these effects likely vary with mandates’ generosity—that is, in terms of the benefit provisions they offer. Mandates vary based on benefit type, amount, and duration across states (Callaghan & Sylvester, 2019b; Choi et al., 2020). For example, while 37 mandates require that insurance benefits are extended to adolescents (children aged above 12 years), 26 states have extended these benefits to those aged 18 years and older. To further illustrate: since 2012, California’s mandate has included coverage for those aged 18 years and older, incorporated a specific provision for ABA, and contained no annual or total spending caps for general or behavioral therapy benefits (State of California, 2012). By contrast, Louisiana’s state insurance mandate has not included coverage for those aged 18 years and older or incorporated a provision for ABA; it also has limited total benefits to US$36,000 per year, and this limit is not indexed to inflation (State of Louisiana, 2011).
This variation in mandate policy features raises an important question: do more generous mandates result in greater changes in the supply of healthcare providers for ASD? If this were in fact the case, then it would suggest that more generous legislation could partially address an ongoing shortage of mental health services for children with ASD in the United States (Gordon-Lipkin et al., 2016; R. K. McBain, Kareddy, et al., 2020). To study this question, we examined the effect of mandate generosity on growth of the state-level mental healthcare workforce across all 50 states, from 2003 to 2017. Specifically, we examined growth in child psychiatrists, BCBAs, and pediatricians—three professions that support the behavioral, developmental, and physical needs of children with ASD, and for which we have detailed inventories on annual workforce supply at the state level. While pediatricians are common providers for children with ASD (Cummings et al., 2016), they represent generalists with a broadly distributed caseload. Comparatively, child psychiatrists and—to a greater extent—BCBAs represent specialized cadres providing focused supports for children with ASD.
We examined whether and to what extent growth in health providers per 100,000 children related to eight mandate policy features. We hypothesized that states with more generous policy features over the study period would have more rapid growth in child psychiatrists and BCBAs and that this effect would be more muted among pediatricians based on their larger numbers and lack of specialization for this clinical population.
Methods
Sampling frame
This study examines autism insurance mandate legislations across all 50 US states from 2003 to 2017, a period during which 44 states introduced insurance mandates. (Indiana and Maryland already had mandates in 2003; Idaho, North Dakota, Washington, and Wyoming did not introduce legislation over this period.) We aggregated all data at the state level. The District of Columbia was not included because the limited geographic area and population had the potential to distort prevalence estimates. The research protocol for this study was deemed exempt from review by the lead author’s Institutional Review Board.
Measures
Seven data sets were merged to capture information on state insurance mandate legislation, workforce information, and state-level demographic information to incorporate as covariates in our models. Below, we describe each of these categories in further detail.
State insurance mandates
Mandates and the constituent features of this legislation were abstracted from the National Conference of State Legislatures’ (NCSL) Autism and Insurance Coverage Data set (National Conference of State Legislatures, 2019) and the American Speech Language Hearing Association (ASHA, 2019) Insurance Data set. As these data sets are semi-structured inventories of state legislation, the two sources were used to cross-reference one another, and where discrepancies arose we reviewed original legislative language. Building on a coding schema developed by Callaghan and Sylvester (2019a, 2019b), for each year within the data set (2003–2017), we identified states as having either (1) no policy, (2) a restrictive policy, or (3) a generous policy, along eight axes—specifically, whether the policy: (1) covered individuals aged above 12 years; (2) covered individuals aged above 17 years; (3) contained a general spending cap (i.e. total expenditure) up to which the mandate applied; (4) contained a healthcare spending cap up to which the mandate applied; (5) contained a behavioral therapy spending cap up to which the mandate applied; (6) contained a lifetime spending cap; (7) indexed spending caps (if they existed) to inflation; and (8) contained a limit on the number of behavioral therapy hours to which the mandate applied. Each policy feature was coded as three dummy variables: no policy, restrictive policy, and generous policy.
In addition to the categorical measures, we used Callaghan and Sylvester’s total generosity score as a continuous measure, from 0 to 8. In short, this continuous measure summates scores across a majority of policy features and takes into account whether spending caps are above/below the national median. A full description can be found in Callaghan and Sylvester (2019).
Workforce
We abstracted annual data on mental health workforce supply from the Department of Health and Human Services’ Area Health Resource File (AHRF), which includes state-level numbers of child psychiatrists and pediatricians updated on an annual basis and routinely used for research purposes. For pediatricians, we included only general pediatricians; we did not include developmental pediatricians, as they represent a qualitatively unique and small cohort of specialized providers (n = 673, as of 2017). BCBA workforce supply at the state level was abstracted from the Behavior Analyst Certification Board (BACB, 2019), which represents a comprehensive, routinely updated database of providers as all BCBAs obtain certification from the BACB and register to practice. Specifically, this data set contains the state of registration and practice of all active BCBAs on a rolling basis. As a common measure of workforce supply, we calculated number of providers per 100,000 children for each year. The US Census Bureau reports annual counts of children and adolescents 0–19 at the state level, which served as the basis of the denominator in this calculation (U.S. Census Bureau, 2017).
Covariates
We included four additional measures as covariates, three of which have been previously demonstrated to correlate with the supply of behavioral health services: income per capita, race, and ethnicity (Cook et al., 2017; Cummings et al., 2017). With regard to income per capita, we assessed median income per capita at the state level–based data reported annually by the US Department of Commerce—measured as personal income, which includes wage and salary as well as sources of noncash income (e.g. employer-provided insurance) (U.S. Department of Commerce, 2019). With regard to race/ethnicity, we included two further covariates from the US Census Bureau. First, percentage of Black non-Hispanic, and second, percentage of Hispanic. For each of these, we assessed the percentage of the total state population represented by these categories (U.S. Census Bureau, 2017).
As a fourth covariate, we included an indicator variable for states that listed ABA as an essential health benefit (EHB) within Marketplace plans following passage of the Affordable Care Act (n = 32 states), which came into effect beginning 1 January 2014 (Autism Speaks, 2018). We considered this as a potentially confounding health policy affecting generosity of autism-related services that occurred over the time period of interest.
Statistical analysis
After evaluating the distributional characteristics of variables within our data set, we made two adjustments to address non-linearities: first, we log-transformed outcome measures (providers per 100,000 children) to reduce right skewness. Second, we created indicator variables for each year in the data set to account for non-linear growth trends in the number of providers from 2003 to 2017. We then estimated multivariable linear regression models, with fixed effects for year and state (Meyer, 2018). The rationale for state fixed effects is to account for the potential of omitted variable bias—for example, time-invariant features of states such as quality of social amenities that might influence workforce supply. State fixed effects remove this state-specific variance component (Wooldridge, 2012). Year fixed effects serve a similar purpose: namely, to account for secular growth trends in the workforce supply that might otherwise be attributed to mandate ratification.
The independent variable of interest, mandate generosity, was incorporated with a 1-year lag to permit a sufficient period of time after law passage for mandates to have an effect on workforce supply. More extended time lags were considered and demonstrated similar results, but we limited ourselves to this duration in order to minimize the potential for external policies and programs to influence observed results. We also considered an event study modeling framework; however, due to heterogeneity in treatment effects and (in particular) the potential for ratified legislation to be repealed—which was observed in states, such as Texas—we prioritized an expanded difference-in-difference specification (Abraham & Sun, 2018).
The model included time-varying covariates as described above and clustered standard errors at the state level. Our primary specification included total mandate generosity score (0–8) as the outcome measure. Secondary models examined dummy variables for each policy feature to individually assess the effect of restrictive policies versus no policies and generous policies versus no policies. All test statistics were two-sided, with an alpha-level of 0.05, and conducted in Stata 16.0 (StataCorps, 2014).
To facilitate interpretation of the results, we estimated predictive margins using Stata’s margins command. This provides predicted counts for each provider type, as well as an associated standard error and 95% confidence interval (CI), based on fitted models calculated over the full distribution of covariate values within the data set.
Results
Descriptive results
Between 2003 and 2017, 44 states implemented state insurance mandates to cover services for ASD: 2 states had mandates by 2003 and 46 states in 2017. As indicated in Figure 1, this shift predominately reflected an expansion of generous policies, with a majority of states having a generosity score of 3 (or 4) out of 8. Mandates in only five states produced a generosity score of 8 out of 8 by 2017: California, Colorado, Indiana, Massachusetts, and Minnesota.
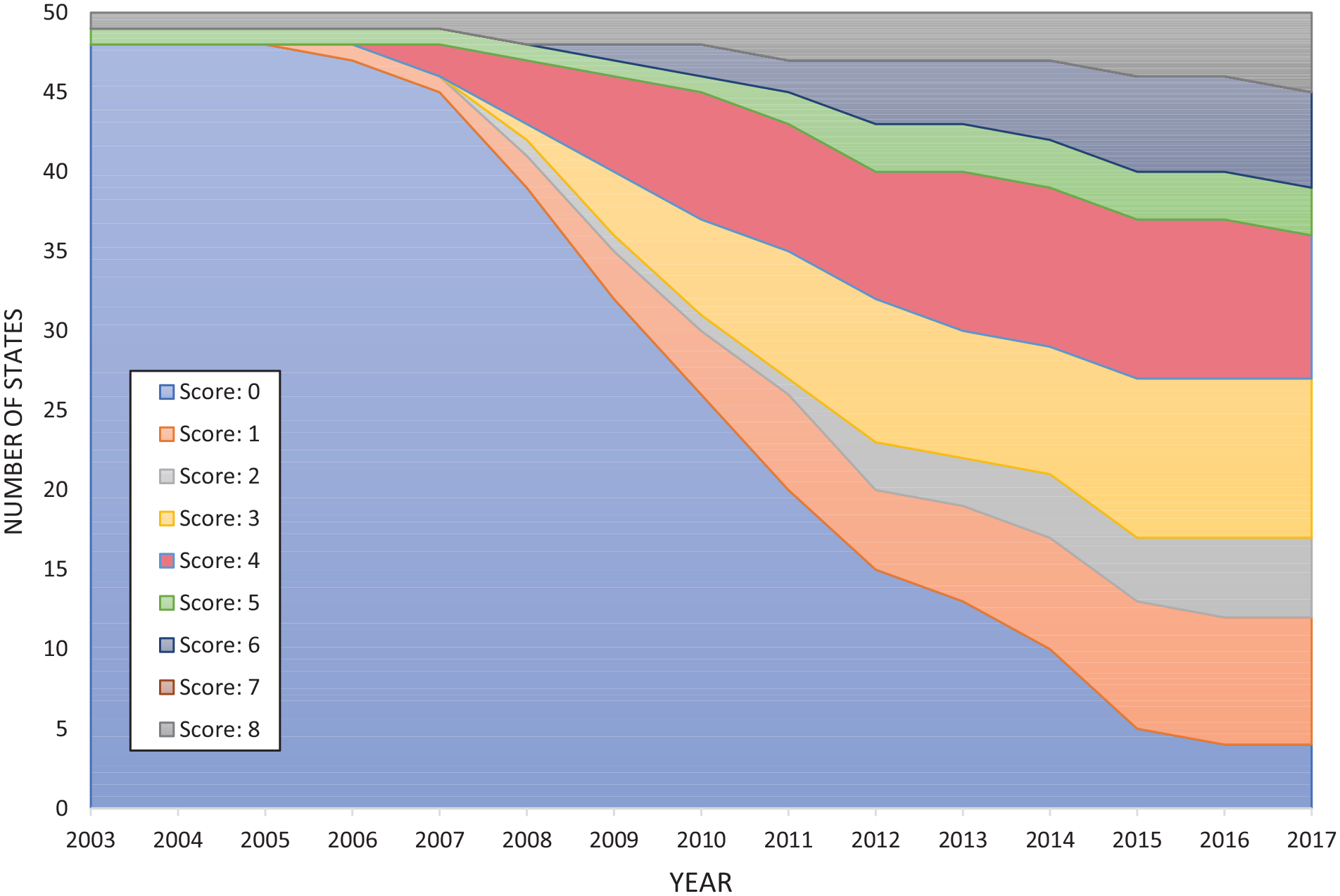
Number of states with mandate generosity score 0–8, by year.
As indicated in Table 1, there was considerable variation across states in terms of mandate restrictions. For example, in 2017, only 10 of 46 states with mandates restricted benefits to children 12 years or younger, but 37 included an annual total benefit limit.
Restrictive features of state insurance mandate (2003–2017).

From 2003 to 2017, the number of child psychiatrists per 100,000 children in the United States increased from 7.40 to 10.03; the number of BCBAs per 100,000 children increased from 1.34 to 29.88; and the number of pediatricians per 100,000 children increased from 62.35 to 68.86. As indicated in Figure 2, the growth of providers—according to each provider type—diverged by state insurance mandate status: for each provider type, the states with generous mandates experienced the highest growth, followed by the states with restrictive mandates, while states with no mandates experienced the lowest growth.

Providers per 100,000 children (2003–2017)—by state insurance mandate status.
Regression analyses
The primary analysis, which predicted the number of providers per 100,000 children based on state insurance mandate generosity as a continuous measure (0 to 8), showed a significant relationship between mandate generosity and level of BCBAs (β = 0.039, 95% CI: 0.011, 0.066, p = 0.005) and child psychiatrists (β = 0.021, 95% CI: 0.003, 0.040, p = 0.02). The relationship between mandate generosity and level of pediatricians was non-significant (β = 0.005, 95% CI: −0.0003, 0.011, p > 0.05).
Using the regression results, we generated the expected level of providers per 100,000 children according to year and mandate generosity, as summarized in Table 2. For BCBAs, states with no mandates would expect an increase of 17.08 BCBAs from 2003 to 2017, compared to 17.90 in states with a restrictive mandate (score: 1, on scale from 0 to 8) and 24.95 in states with a generous mandate (score 8, on scale from 0 to 8). For child psychiatrists, states with no mandates would expect an increase of 1.62 child psychiatrists per 100,000 children from 2003 to 2017 versus 1.66 child psychiatrists in states with a restrictive mandate and 1.94 child psychiatrists in states with a generous mandate.
Expected number of providers per 100,000 children—by provider type, year, and mandate generosity.

BCBA: board-certified behavioral analysts. Bold values are significant at p<0.05.
The values represent expected number of providers per 100,000 children based on predictive margins from multivariable regression analyses, with year of interest 2003 or 2017. The values in parentheses represent standard errors. “No mandate” reflects a score of 0 on the continuous generosity measure (0–8), while “restrictive mandate” reflects a score of 1 and “generous mandate” reflects a score of 8. The “change” column represents the absolute magnitude of change in expected number of providers from 2003 to 2017, according to provider and mandate type.
Multivariable regression analyses examining individual policy features identified a consistent pattern of results (see Table 3): When examining BCBAs, states with generous mandates (vs no mandate) were associated with higher levels of BCBAs across all eight policy features (β’s = 0.11–0.15, p < 0.05), whereas restrictive policy features were associated with higher levels of BCBAs for four features: whether spending caps were indexed to inflation (β = 0.13, 95% CI: 0.03, 0.23, p < 0.05), whether there was a behavioral therapy spending cap (β = 0.15, 95% CI: 0.04, 0.25, p < 0.01), whether there was a total spending cap (β = 0.12, 95% CI: 0.03, 0.21, p < 0.05), and whether individuals aged 18 years and older qualified for benefits (β = 0.12, 95% CI: 0.01, 0.24 p < 0.05). In a similar vein, when examining child psychiatrists, states with generous mandates (vs no mandate) were associated with higher levels of child psychiatrists across all eight policy features examined (β’s = 0.05–0.10, p < 0.05). However, we did not observe any restrictive policy features (vs no mandate) that were associated with higher levels of child psychiatrists. No policy features were associated with levels of pediatricians per 100,000 children.
Average effect of individual state insurance mandate policy features on mental health workforce.

BCBA: board-certified behavioral analysts.
The values represent the number of additional providers (BCBAs, child psychiatrists, and pediatricians) 1 year after mandate introduction, relative to states without mandates. The values in parentheses represent 95% confidence intervals. *p<0.05, **p<0.01.
Discussion
To our knowledge, this is the first study to examine the relationship between generosity of state insurance mandates and growth in the health workforce for ASD. While prior studies have examined the effect of mandates on healthcare utilization, spending, and workforce (Barry et al., 2017; McBain, Cantor, et al., 2020), they have focused on mandates as all-or-nothing pieces of legislation and have not accounted for the wide variation in policy features (Callaghan & Sylvester, 2019b; Choi et al., 2020). Our findings show a consistent pattern of results whereby more generous mandates are associated with increased growth in BCBAs and child psychiatrists, indicating that the content of legislation passed may be as important as whether any legislation has been passed. This finding is particularly important because of a growing literature demonstrating a shortage of providers—including child psychiatrists (R. K. McBain, Kofner, et al., 2019), BCBAs (Zhang & Cummings, 2019), and pediatricians (Mazurek et al., 2020)—equipped to meet the needs of children with ASD in the United States, and the potential of well-crafted legislation to stimulate growth in this workforce. An increase in the number of providers may reduce the amount of unmet demand for treatment for children with ASD and alleviate the caregiving burden for parents of children with ASD.
With regard to overall generosity of mandates, measured as a scale from 0 to 8, we found that more generous mandates were associated with a significant increase in BCBAs and child psychiatrists. A state in 2017 with a generosity score of 1—the lowest possible score for states with mandates—would be expected to have 18.9 BCBAs per 100,000 children, compared to 26.8 BCBAs in a state with a generosity score of 8, more than a 40% difference. This difference in service coverage is significant and clinically meaningful, particularly when viewed in light of BCBA shortages in key geographic areas of the United States (Behavioral Analyst Certification Board, 2017). For child psychiatrists, this difference is not only smaller but also significant: roughly 17% (1.66 vs 1.94 child psychiatrists per 100,000 children).
While it may be the case that states with more generous mandates are qualitatively different from states with restrictive mandates or no mandates, our analytic approach examined the average effect of mandate generosity at 1 year after ratification. Prior research has similarly found that variation in the generosity of policies is associated with magnitude of change. For example, one recent study found the effect of transitioning from Medicaid to Medicare for pharmacological treatment varied as a function of generosity in Medicaid drug benefits (Madden et al., 2015). A large pool of literature has also found that level of health service utilization and spending depends, in part, on generosity of insurance benefits—similar to those benefits protected by mandates (Friedman et al., 2019; Wehby et al., 2019).
We also found that mandate generosity reflected in individual policy features is consistently associated with greater increases in BCBAs and child psychiatrists over the 2003–2017 timeframe. Across all eight policy features examined, generous policy features were associated with significantly larger increases in BCBAs and child psychiatrists, compared to states with no mandate. By contrast, restrictive versions of these policy features, relative to no mandate, were only associated with provider increases in three of eight instances (in the context of BCBAs) or one instance (in the context of child psychiatrists). These findings are consistent with the trajectory of BCBA growth over the study period, as this provider group was rapidly expanding from 2003 to 2017 (Behavioral Analyst Certification Board, 2017), and BCBAs have the option of working in states with more favorable reimbursement policies for their services. The overall pattern also signals an important lesson for policymakers: legislation, which may be construed as a political win, may nevertheless fail to yield positive outcomes if substantive benefits are not provided.
With regard to child psychiatrists, we found that the relationship with mandate generosity is more muted. This could be viewed from three complementary perspectives. First, relative to BCBAs, growth in child psychiatrists has been much slower over the past decade (McBain, Kareddy, et al., 2020), in part due to a relatively low rate of recruitment of medical graduates to psychiatry (Brenner et al., 2017). Second, children with ASD comprise a relatively small proportion of the patients with whom child psychiatrists interface (Siegel, 2014), so legislation that specifically relates to ASD is liable to have a proportionally smaller influence on this profession. Third, child psychiatrists are already strained with respect to demand for their services, and many do not accept fee-for-service insurance (Bishop et al., 2014)—in which case, changes in insurance benefits resulting from mandates may play less of a role. A future study might look at the relationship between fee-for-service acceptance rates and the impact of mandates on service utilization and workforce growth. It should also be noted that, given the time lag in entry to the market for prospective child psychiatrists, the trends we observe may be attributable to individuals completing residency who elect to practice in states with mandates or shifts in the existing supply of providers within and outside the United States to states with more generous reimbursement practices.
Finally, we did not find a significant relationship between pediatrician levels and the passage of mandates. Prior research indicates that pediatricians may not feel adequately trained to provide autism-related healthcare services and refer these individuals to more specialized care (Carbone et al., 2010; McBain, Kareddy, et al., 2020; Nolan et al., 2016). Moreover, compared to BCBAs and child psychiatrists, pediatricians provide health care for a general population of children and adolescents, making children with ASD a small proportion of population to which they provide care. Similar to child psychiatrists, pediatricians’ high demand for services and stable salaries prior to mandates may have weakened the effect of these laws (Basco et al., 2013). Our findings indicate that an increased supply of pediatric services for children with ASD would be contingent on more targeted policies and programs such as medical school curricula that provide further training with this population (Havercamp et al., 2016). Encouragement to specialize as developmental pediatricians may also be warranted given the limited number of these practitioners, which also precluded our ability to analyze this provider type.
We note several study limitations. First, our study is observational, and thus causality should not be implied. It may be the case that, for example, states in which generous mandates are passed offer a more favorable environment for mental healthcare provision more generally. Our approach to analyses, which used a quasi-experimental interrupted time series approach and included state fixed effects, was designed to address some of these concerns, but may still include omitted variable bias. Second, we had limited information on providers—including their exact locations of practice and volume of patients they serve. Unmet need could vary as a function of providers’ engagement in practice. Third, we restricted our analyses to the1-year period after mandates went into effect—in order to limit the potential for extraneous policies to influence observed results. However, this time period is relatively short for observing supply response to changes in market conditions, particularly when considering the duration of training required for additional market entry. Some of the workforce growth observed in states may be accounted for by existing providers shifting their location of practice. Fourth, due to the fact that mandates are implemented at the state level, we had a limited number of observations and corresponding statistical power. This also led us to narrow the provider types examined to those with sufficient data reported. Secondary analyses did not include an adjustment for multiple comparisons because we were testing a priori hypotheses.
Conclusion
In summary, we find that generosity of mandates is associated with the magnitude of increases in supply of BCBAs in the United States, and—to a lesser extent—child psychiatrists. Our results suggest that the degree of generosity afforded by mandates may be as important as the passage of legislation. That said, the number of states with very generous mandates—as indicated by an 8 out of 8 on the continuous generosity measure—was still very low as of 2017 (n = 3 states), suggesting significant room for policy revisions that could influence workforce supply for children with ASD. Future research should examine the impact of additional legislation, such as Medicaid expansion, on workforce growth.