
Abstract
Families provide a critical context for the overall growth and development of a child. The health of a family is foundational to the everyday life in which a child and family can flourish. For families raising a child with autism, the chronic, intense nature of everyday life affects family health in part due to increased parental stress and potential centralization of the child with autism in family functioning. The present study sought to understand how families of children with autism perceived and experienced their own family health and to identify what factors and processes families identified as contributing to their health. Researchers conducted semi-structured interviews with 16 families with a child with autism ages 2-17. Interviews occurred in person and with all members present to the extent possible based on parental and child choice. Sixteen mothers, eight fathers, and 32 children (18 with autism) participated. Interviews were about the family as a unit and conducted in a casual dialogue style. Interviews were audiorecorded and transcribed verbatim. Researchers analyzed data using inductive content analyses to generate results. Findings suggest families experience family health as a journey grounded within family identity and marked by five themes: connection, balance, the centralization of autism, stress, and support systems. Findings contribute relevant considerations for service providers working to support children with autism and their families.
Lay abstract
Families are important for the overall growth and development of a child. The health of a family is foundational to the everyday life in which a child and family can blossom. Families with a child with autism have a family life that has challenges for many reasons including that parents can be stressed from trying to figure out how to be a good parent for their child with autism. We wanted to know two things: (1) what is family health for families of a child with autism and (2) what affects families trying to be their healthiest. We wanted to know the answers to these questions from families themselves, including parents (not just moms), children, and children with autism, because they are the best experts. We talked to 16 families including 16 mothers, 8 fathers, and 32 children (18 with autism). Families shared that being a healthy family was a journey with ups and downs and that families were not always perfect. It helped when families knew about themselves as a family such as knowing what they liked and did not like to do, and knowing what the different people in the family needed. Families said that what helped and influenced their family’s health was being together, keeping their days not too busy, stress, autism itself, having helpers like friends, grandparents, therapists, and having money to pay for services. We hope that knowing these answers will guide service providers of people with autism to think about healthy families from a holistic perspective.
Introduction
Families are the consistent and primary context for the overall growth and development of most children. The health of a family is foundational to the everyday experiences in which both a child and family can flourish. Family health is broadly defined as “the dynamic ways members holistically care for one another using communication, cooperation, and caregiving to develop and sustain health routines within the contextually embedded household” (Denham, 1999, p. 149). Weeks and OʼConnor (1994) conceptualize family health as “a perception of physical, emotional, social, and spiritual commitment and energy that varies with culture, values, and time that is based on, and reflected in, the connectedness between people who value each other and have hopes for the future” (p. 209). These definitions reflect family health as a dynamic, evolutionary process involving changes and adaptations over time.
Smith and colleagues (2017) expanded upon these definitions by identifying the specific factors and mediating processes that support robust family health. Factors include balance within schedules and member time for self and whole family, togetherness for promoting connection among the family, and purposeful living including deliberateness and intention around family decision-making and enacted everyday routines (Smith et al., 2017). Processes mediating robust family health include family awareness and reflection about their health as well as family adaptation through problem-solving and communication.
Families of a child with autism create family life within an environment influenced by complexity and challenge including elevated parental stress, decreased parenting sense of efficacy, strained quality of co-parenting relationships, and significant financial implications (Galpin et al., 2018; Karst & Van Hecke, 2012; Sim et al., 2018). Evidence suggests that families with a child with autism tend toward centralization of family functioning around the child with autism, detracting from holistic family functioning needs (DeGrace et al., 2014). Families may also experience over-routinization, which can be both supportive and restrictive on family functioning (Boyd et al., 2014). For parents of children with autism, the family environment predicts parental quality of life, which includes the communication, cooperation, relational support, and ways of problem-solving between parents and family members (Derguy et al., 2018).
Within the family, siblings of children with autism also experience challenges that affect their own outcomes and experiences of health. Siblings of children with autism have significantly more difficulty with sibling relationships and experience internalizing behavioral problems, and difficulties with psychological and social functioning, as compared to siblings of typically developing individuals (Shivers et al., 2019). Siblings qualitatively articulate challenges “fitting into the family” and feeling “unseen” or “forgotten” within the family due to the perception that parents constantly address the needs of their sibling with autism (Leedham et al., 2020, p. 9) while also describing experiences of love, affection, and appreciation for the unique qualities and interests of their sibling with autism.
Despite documented threats to the health of families of children with autism, evidence of intervention effectiveness on family level outcomes is minimal, as outcomes overwhelmingly focus on the child with autism (Karst & Van Hecke, 2012; Kuhaneck et al., 2015). Shifting impairment and child-focused services for children with autism toward those that prioritize the ecological context of the family as the mechanism of intervention have the potential to generate generalizable, efficient, and sustainable outcomes for both the child and family. De Jaegher (2013) proposes leaving behind the traditionally implemented “disembodied individualism” (p. 14) common in child autism interventions in which the child’s functioning is compartmentalized into structures and functions within the child yet which exists outside the child’s context of meaning making in a dynamic environment. Similarly, Danforth’s (2013) ecological model of autism suggests that the measure of progress for individuals with autism is not as much within individual change, but rather in the individual’s ability to interact and participate successfully within their environment, which inherently includes the critical family environment. This contextualized perspective aligns with that of families, who report that existing interventions help their child but do not necessarily meet parents’ needs, leaving parents with feelings of social isolation and community alienation (Galpin et al., 2018). Families want relational support services that consider the needs of the whole family including the intricate and complex relationships among members, as well as social and psychological supports, along with the impairment-focused interventions that their child receives (Derguy et al., 2015; Galpin et al., 2018).
In addition to contextualized interventions, Dingfelder and Mandell (2011) highlight the need for autism research to situate itself in the real-life contexts in which researchers anticipate changes to occur. Adopting an ecological model of understanding families as a mechanism for intervention aligns with the perspective of researchers who clearly delineate the importance of community embedded and stakeholder engaged research that has potential for real-life contextual change (Dingfelder & Mandell, 2011). Applying socioecological approaches within research on families with a child with autism can optimally capture the nuanced experience of the interrelationships among multiple family members (Greenlee et al., 2018; Tint & Weiss, 2016) rather than relying on traditionally reported maternal perspectives alone. Cridland et al. (2014) specifically underscore the need for qualitative research approaches to investigate the multifaceted relationships between individual members within families of a child with autism.
Understanding the health of families with a child with autism can ultimately support provision of relevant interventions that maximize child and family outcomes through authentic understanding of family complexity. The purpose of this study is to understand how families with children with autism perceive and experience their own holistic family health and to identify what factors and processes families identify as contributing to family health. In alignment with qualitative inquiry, family health was not defined a priori to conducting this research. Rather, this study sought to understand what “family health” meant to participant families of children with autism. This study sought to answer the following research questions:
RQ1. What is the experience of family health for families with children with autism?
RQ2. What factors and/or processes contribute to family health for families with children with autism?
Methods
Methodological approach
This qualitative study used a phenomenological approach in order to elicit and understand families’ experiences of their own health processes. Phenomenology is a qualitative research approach that affords a mechanism for understanding deeply how people experience, describe, and feel about a particular phenomenon (Patton, 2015, Module 14), in this case, family health for families of children with autism.
Participant families were recruited using nonprobability convenience sampling methods via posted flyers in pediatrician offices, therapy clinics, and community centers; emails to professional and personal contacts; and social media postings. Participants were recruited from both urban and rural areas primarily within the Northeastern United States. The inclusion criteria were families: (1) who had a child diagnosed with autism as confirmed by a parent-signed statement of such, (2) whose child with autism lived in the home, and (3) who spoke fluent English. Participant families were excluded if autism was not the primary diagnosis of their child. For the purposes of this study, family was defined as the persons who had a shared history and future with the child and who cared for the child physically and emotionally on a regular basis. The University of New Hampshire Institutional Review Board approved this study to ensure researchers implemented ethical guidelines for the protection of participants including informed consent and assent, and maintaining participant confidentiality. Participants received a US$25 gift card for research participation. Community members were not involved in the study design, implementation, or dissemination of findings. However, this study specifically elicited the perspectives of community members and reflected those in this article.
Participants
Sixteen families with a child with autism participated in this study including 16 mothers, 8 fathers, and 32 children (n = 56). Eighteen children had autism. Table 1 presents the detailed child and family characteristics.
Participant characteristics.
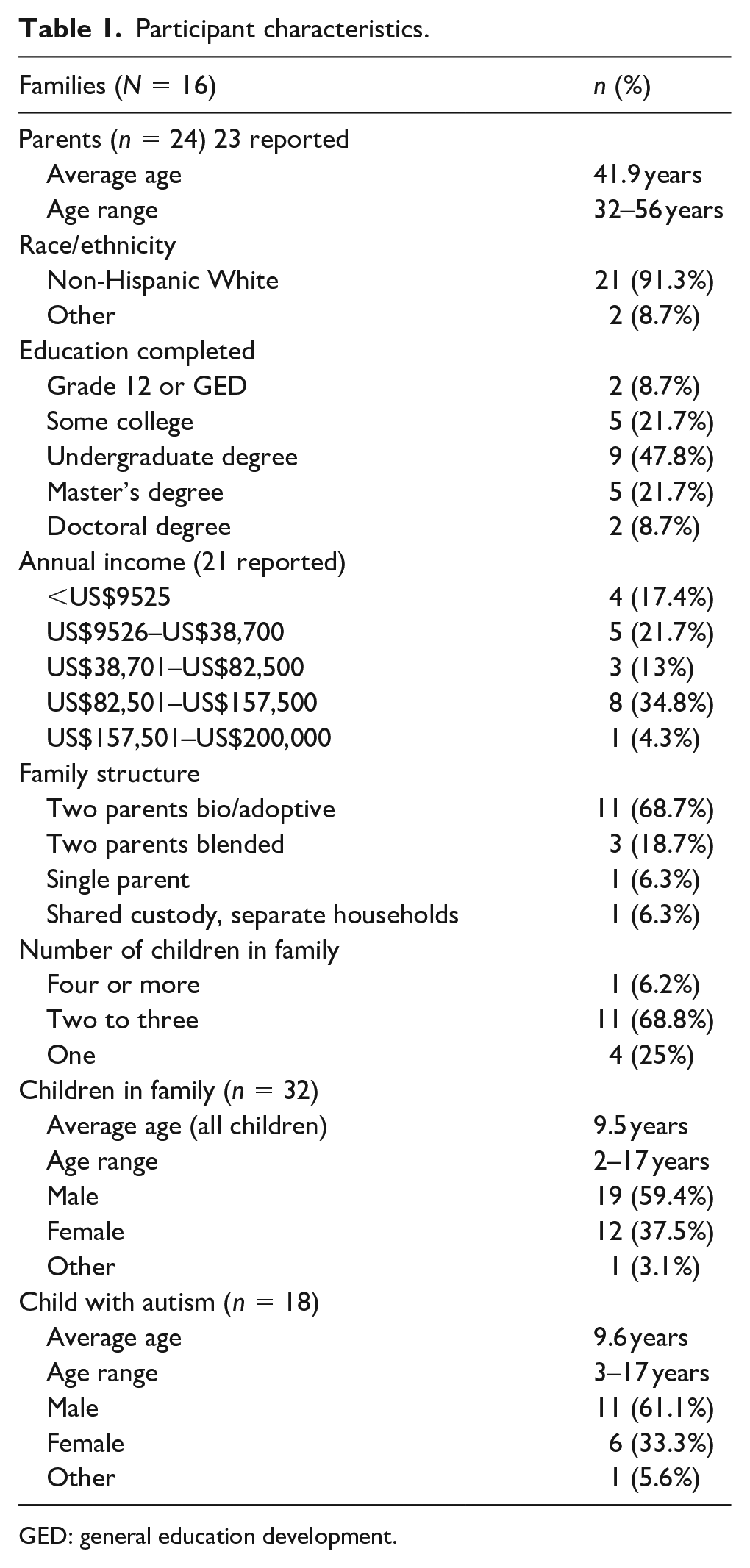
GED: general education development.
Data collection
Researchers collected data via an in-person 45 to 60-minute interview conducted in a location of mutual convenience, primarily in participant homes. Both parents and children were present to the extent possible in order to obtain a full family perspective inclusive of all parent and children’s voices. Some parents chose not to include their children. For those who did, researchers ensured family members participated in a conversation about the family unit as a whole and, in consideration of ethical boundaries, did not discuss characteristics of or concerns about individual family members. Interviews followed a semi-structured format with questions about the family as a unit that were intentionally designed to encourage open-ended reflective answers about families lived experiences and based on previous family health research (See Appendix I for interview questions; Smith et al., 2017). Prior to commencing all interviews, researchers journaled their thoughts and feelings about what it meant to be a family of a child with autism, and how families might experience health in order to surface researcher assumptions. Researchers held these perspectives at the forefront of the data collection and analysis processes to situate awareness about potential assumptions influencing analyses.
During the interview, the researchers facilitated a casual family dialogue in order to elicit child, sibling, and parent perspectives collectively. One researcher interviewed the family while the other researcher observed and wrote field notes. The interviewers intentionally paused and waited throughout the interview in order to encourage reflective responses, and used probes as needed to afford families further opportunity to articulate their lived experiences of family health. Furthermore, after each interview, researchers independently documented thoughts and impressions. Interviews were audio-recorded and transcribed verbatim by the second author. The first author then verified transcripts for 100% accuracy by listening to the audio recordings and ensuring matching transcripts. These transcription and verification steps served as an initial step in phenomenological data analysis as researchers situated themselves across hours of listening to participants’ voiced perspectives.
Data analysis
The two-member research team held 12 multi-hour meetings over 4 months to analyze data. Utilizing systematic, inductive content analysis methods (Patton, 2015), researchers first independently read interview transcripts one at a time. In the first coding round, researchers openly highlighted words and phrases that suggested phenomenological meaning and reflected “how” families described their health and “what” factors contributed to their health. Researchers then met to discuss, debate, and reach consensus on merged codes (n = 29). During this consensus process, researchers referred to field notes to assist in decision-making when researchers needed additional insight about particular family situations or perspectives not represented in the interview texts. Researchers consolidated merged codes into initial categories (n = 12) which were explicitly defined based on the data and reflected family health. After deliberations, researchers then decided on eight focused categories that reflected family health.
Researchers made decisions about data reduction during this iterative process through dialogue in which each researcher presented their perspective on the extent to which initial categories related and fit one another in order to determine focused categories. Categories that did not hold across multiple or all families or those that did not clearly link to the research question were not sustained. Focused categories were further refined into final themes that represented the experience of, and factors contributing to, family health. Table 2 presents examples of the data condensing process. Throughout the data analysis process, researchers compared emerging findings with original data to confirm that findings reflected participants’ original intent. Researchers had prolonged engagement with the data during interviews, interview transcription and verification, and data analysis that supported dependability of findings.
Data analysis condensing process examples.

ASD: autism spectrum disorder.
Results
Families with children with autism described family health as a journey, which for many was grounded within family identity. Families described five distinct themes surrounding their family health journey: connection, balance, the centralization of autism, stress, and support systems.
The experience of family health: the journey and family identity
Families with children with autism overwhelmingly described family health as a journey: a dynamic process consisting of periods of relative strength and stability mixed with challenge and chaos. Anchoring the family health journey for many participants was a family identity that reflected who families were and wanted to be. This identity reflected families’ essence, drive, goals, and vision. Some families were confident in their identity and viewed family health as a process. This process was marked by a constant fluidity between (1) the implications and experience of having a child with autism within everyday family life and (2) their expectations for family joy, belonging, and participation in their desired family life.
Families’ overarching sense of family health was of its ever-evolving nature, filled with moments of health that were sometimes fleeting, but generally moving in alignment with their identity. Families repeatedly expressed how their family health was constantly growing and changing, reflecting that family health was not an achieved state, but rather a process that resulted in a journey experience. One father shared this perspective about a time of strong family health reflecting the family health experience as a journey: I think we grow stronger the more knowledge we obtain. So a specific time is hard for me to pinpoint. I think right now we’re getting a little bit stronger. Since [son] has started to develop some verbal language it’s been remarkably helpful to the family. We all feel stronger when we can help meet his needs and therefore meet everybody else’s needs. So right now, I think we’re growing stronger. We’re learning a lot, we have some great supports in this current moment. It’s changing, it’s evolving.
Another family expressed the process of finding family health as a “rocky road,” depicting both a challenging element to family health as well as its nature as a journey as depicted by this mother: Well, I mean it’s been difficult, it’s definitely been an uphill battle, it hasn’t been typical, you know. Just seeing how things have changed throughout the years, and the current medication that he’s on [son with autism] has definitely been life-changing . . . because it’s been a really rocky road . . . you know, with aggression and outbursts, you know? It’s just like [snaps fingers] flick of a switch. You know, there is no real rhyme or reason to it, you know, he can be cool as a cucumber, and then it’s off the deep end . . . so things are definitely on the upward swing, but it’s been a rocky road to get to where we are.
Families described that viewing health as a journey encouraged them to accept the challenges inherent in everyday life, knowing that they were not under pressure to achieve perfection in a moment and that they could work toward future goals. Understanding family health as a journey provided comfort in the challenging moments and vision for the future. One mother put it this way: There are days where it feels so stressful and so hard to manage, but then when I think about the real messages and the real, like, what we’re trying to achieve, and I say it out loud, it doesn’t seem all so . . . you know, some days seem hard, but I’m thankful that the ultimate goals are still really in sight, and achievable. Often achievable.
Families each described themselves at a point in their respective journeys. They spoke about their experiences, daily challenges, routines, and hopes for their family. However, underlying these daily experiences, families possessed unique outlooks that influenced their approach to daily life and their vision of their family. Some families articulated a strong family identity and described a high degree of connectedness with each other. These families tended to express confidence in their family’s journey and purpose. Having a family vision outlook seemed to provide a foundation that anchored families’ perspective of the journey. One mother described identity this way: I adore him [son with autism]. And I think he’s supposed to be ours . . . I have a greater faith, I’m not a hundred percent sure in what that is, but I have a greater faith that he’s supposed to be a part of our family, and I’m supposed to be his mom. So I try to use that as the guiding sense of even if today’s hard, this is where we’re supposed to be right now. And we’ll get through it. Blood, sweat and tears, we’ll get through it.
Another family articulated their identity as stability in the midst of a challenging journey. A father expressed a mind-set that reflected their stability as a family despite the sometimes-volatile circumstances that presented themselves: Maybe you’re asking, kind of, the difference between climate and weather. Right? Weather changes from hour to hour, but climate is, in general, this is what it’s like. In general, I think it’s really good, we tend to have strong bonds, and in general, we smooth out the pits and rises from day to day, it’s really good. But there are pits and rises from day to day. Some days it’s an actual roller coaster within that day. And sometimes after the third or fourth roller coaster loop, we’re like, you know what, you [daughter with autism] go looping, I’m staying where I am [family laughter].
This family’s daughter with autism added her perspective: “and sometimes it’s just a downward spiral” to which the whole family further erupted in laughter. For the families in this study, these mind-sets of purpose-imbued, identity-driven family life were the driving and centralizing force behind families’ experiences of their journeys toward family health.
Themes surrounding family health
Participant families with children with autism experienced their health in a broad sense based on their journey guided by identity. Specifically, participants described five prominent themes surrounding their family health journey: connection, balance, the centralization of autism, stress, and support systems.
Connection
The most frequently reported theme regarding family health was connection. Every participant family described that physically being together in shared space and time supported their family health by promoting opportunities to communicate and connect with each other. One mother highlighted the unique strength of family time for connection, noting that their family was the primary social support for their two children with autism: The more that we gain momentum finding things to do together, the more it bonds us. And I think too that for a family like ours, we don’t have someone else calling to ask [our children] to do anything, and so we really have to be creative.
Another father shared how doing activities with his family afforded opportunities to bring in past interests from his childhood, adding a generational element to his family’s connection: I like doing stuff together with the family, so like, the different activities. Mom is the one who comes up with the activities usually. Some of it’s just hanging out at home. That’s my favorite part of our family. I like sharing stuff that I was interested in to see if the kids will like it. Sometimes they do, sometimes they don’t.
Another mother expressed that being together made them feel most like a family: If we are going to the beach, going camping, it unplugs us. You know, we interact more, we play more. We have things like—we have a football that we will toss around. There are toys that we play with; we build sand castles together. When we camp we have campfires. And my husband brings his guitar and we all sing badly around the fire. It’s awesome.
Balance
Families described balance as both a theme contributing to health and as a process facilitating health. Families categorized balance in two ways: balance between individual member and whole family needs, and balancing the specific schedule demands of their child with autism with unstructured down time.
Individual member and whole family needs
Families consistently described a pull between satisfying the needs of individual members within the family and satisfying the needs of the family unit as influencing their family health. This balance related to creating time and space to meet personal needs of members such as self-regulation for the child with autism, attention focused on siblings, and self-care needs of parents such as sleep and exercise. Families expressed how their family health was stronger when they struck a balance between individual member and whole family needs as described by this mother: I think a really balanced, healthy day for our family would look like making sure everybody is in a good, regulated space, that they’ve all had their individual needs met so that they can then come together and be present and participate as a family unit. Whereas, if all of their individual needs are not met, they can’t be available to join us in family activities.
Families expressed this balance as foundational to feeling like a healthy family during their journey such as this father described: We try to always have positive activities that we can do with our family . . . it’s really trying to appease everybody’s interests, cause the four of us are all very different people in this household. So it’s really about just constantly trying to give everybody, you know, what it is that they need. I think that is part of the health of this family, but also trying to do things where we can connect, and be a family as much as possible, which is hard . . . but we do try to keep that a regular routine as much as we can.
However, at some points, this balance was difficult to find, and families expressed how differences between individual needs and needs of the whole family were constant features of family life. One mother and father collectively shared how they sought to keep participating in community activities, particularly in light of the impact and lessons such participation had for siblings:
Yeah, so basically, we don’t shy away from bringing [son with autism] to different parties and stuff. Obviously he may not interact with other kids at other parties, and same thing with just regular family stuff, you know, he may not want to interact necessarily with others, but it doesn’t mean he’s gonna be left behind and not be part of the family when we do things. I think it’d be unfair to him. At least let him be offered up the experience as well, being out there. If he chooses not to interact, then, ok, then he’s been introduced anyway.
I think it also is because of the fact that we have three sons, and [son with autism] is the baby, son two is the middle one and he’s the non-autistic, so we don’t want the non-autistic one to think, “oh, well we can’t go to do these things because of my brother.”
Or that he’s the one we brought along, and one of us is behind with our son with autism.
Right.
That’s not right either.
Families expressed how this pull between individual needs and whole family needs was frequently a struggle in light of the influence of autism in their family.
Schedules and activities
Families also reflected the need for balance in everyday activities and routines, particularly around those related to intensive autism interventions. Families depicted how their journey broadly fell into patterns of “routine/non-routine” time as well as “programmed” versus “spontaneous” time that influenced family health. Families expressed a need for stability in daily life, but found that life frequently became busier and more regimented than desired. Participants expressed the challenge of connecting with each other during the busyness of their normal routines, which often precluded time for authentic connection with each other. One father shared a common perspective described by many participant families about how his son with autism’s schedule disrupted family connection at home: I mean, he has programs within an inch of his life . . . we have the OT and speech, we have social therapies, we have tai-kwon-do, we have swimming sometimes, depending, so and some of that obviously is fun, and some of that is like autism stuff. So a lot of the time I just really, like, I’m loathe to stop the kid from just flopping down in front of the goddamn television for an hour, cause he puts in long days, and if I come home from getting him and I’m exhausted, then I can only imagine where he’s at on that.
Many families shared that vacations—breaks from routine—were supportive to their family health. A break from routine allowed for time to recharge, spend time focused on togetherness, take a break from intensive therapies, and gain perspective apart from their daily life. One mother of two teenagers with autism shared: When we have family time to do activities . . . and vacations in general . . . we can kind of let go of how structured our life is so much the rest of the time. It gives us a chance to just like experience things in a different way.
The chronic scheduling experienced by many families seemed related to their experience of vacation as a healthy and connected time for their families. Vacations from regular routines also provided an opportunity for families to experience times of rest, relaxation, and purposeful togetherness as reflected by this father: Those are the things, actually, that make me feel like most like a family, where we’re all somewhere different together . . . just trying new things or exploring. Because we’re removing ourselves from—that’s why people go on vacations. You’re removing yourself from stressors and anxieties and the quotidian sort of worries that you have, and you’re just in a new place so you can focus on you and everyone else.
The importance of spending time together was consistent throughout all families’ descriptions of family health, and was present not only in vacation time but also throughout everyday moments of the journey.
Centralization of autism
The third theme all families consistently described as influencing the family health journey was the pervasive influence of autism. Most families articulated that their child’s overt behaviors, self-regulation, and social communication needs were the greatest autism influence that caused families to centralize decisions, choices, and routines around their child with autism. Families described this centralization affecting several areas of everyday life. For example, one mother described how they did not spend time with extended family due to their child’s reactive behavior: We ultimately want to have, you know, connection and support with cousins and aunts and uncles, and all of these people, but it’s been really hard, because of sometimes his behavior. Even neighbors, you know, because sometimes his behavior was so bizarre that it was very isolating. We just didn’t quite know what to do. So when [son with autism’s] in a good space, I feel like it sort of drives whether our family’s in a good space or not—more than anything, you know, that the three of us (mom, dad, sibling) could ever do.
Another mother shared how her son with autism’s challenges with self-regulation affected the family’s emotional health and centralized the family’s attention toward their son: [Son] is at the center of our focus, unfortunately a lot of the time, because when he is off, which he’s a very disregulated little guy, he struggles significantly with anxiety and stress, and he can tip that scale from emotional regulation very quickly in the environment, so that everybody else can be impacted and we are sort of affected by his situation. So we work really hard as a family to maintain as much of a healthy state as we can. But it fluctuates, in all honesty. Dependent upon what he may be going through. And it can be very impactful, whatever state he’s in can be very impactful on our daughter. And then certainly on us as parents . . . even the dog picks up stress.
Not only did participation in family activities change in response to the influence of autism, families made decisions and plans for the future around the child with autism. Many parents described determining their children’s educational plans, living locations, and job decisions based on the needs of their child with autism.
Stress
Stress, especially parental stress, seemed to be an almost-constant theme ingrained in everyday life that created anxiety. Many parents expressed the challenges associated with autism as being especially stress inducing. For example, one mother shared her difficulty being fully present to her family when she felt mentally overwhelmed: It’s a constant anxiety about when is the health insurance gonna bring the chop down? Well we earn too much for Medicaid and so we’re at the mercy of [private health insurer]. And so a lot of my emotional energy is taken up thinking about when his ABA therapy will be withdrawn . . . the OT is already gone, so that impacts me, my emotional life quite a lot, and to the constant fighting of the school board, the school system . . . this kind of stuff . . . So a lot of my headspace is taken up with that kind of stuff . . . it’s very hard sometimes for me to clear my head appropriately.
As another parent described the processes involved in supporting their children with autism, the stress was evident in the volume of work that was present in each day: You know, all the little things, like nobody thinks of, like you’ve got a doctor’s appointment, and you’ve got to get your haircut, and we’ve got to run to the store so you can have sneakers for soccer. You know—the mental load—the work that doesn’t look like work. It was one thing when you know you just pick the kids up. But, now, you know, I’m having war with the school district about [daughter’s] IEP. I’m talking to two different schools because she’s not going to go to the public school, she’s gonna go to a charter school and, it’s just coordinating everything . . . and then all of the outside therapy appointments. Right now she’s got—she goes to therapy in the other town. Her speech, you know, she’s hopefully going to start for PT and then we’ve got ABA therapy . . . And then we are trying to find, I don’t want to say we’re trying to find services for my oldest, but he could definitely use a maybe little guidance from someone other than mom and dad because it’s just not cutting it.
For many parents, the stress of constant planning, seemingly unending work, and inability to take breaks led to feelings of burnout, helplessness, and compromised family health.
Support systems
While the daily experience of families’ journeys was variable, stressful, and sometimes chaotic, all families overwhelmingly pointed to the theme of support systems as the glue that held them together through the challenging family health journey. The method of support varied, but common support systems consisted of extended family, friendships, therapy services, and financial resources. Families’ support systems provided encouragement on challenging days, respite care for parents to take breaks, and resources to mediate challenges experienced by their child with autism. One mother described how her parents were a support system that was necessary to get her through challenging days: When the days get a little tough I just say let’s go to Mommy and Papa’s, let’s just reset. And often times Papa can distract them in the garden, or you know, give me ten minutes to just catch my breath.
Another family’s support system came in the form of professionals that offered training and resources to work with their children in challenging times as shared by one mother: I know I am really lucky that I had the preschool team that I had, because when I got into the school system, it was like [sound effect suggesting overwhelmed] and they took care of me . . . like I have been so trained, I’m so lucky to have the education and the experience that I have gotten through them.
Children also reflected the importance of support within the family unit itself as providing a sense of stability provided by understanding and knowing each other as described by this teenager with autism:
The relationships between me and my brother are really strong, and we’re all in this together, and we seem to know that. And so we support each other.
I want an audio recording of this later [laughter] . . . because she’s saying we’re all in this together!
I don’t usually admit that [laughs] . . . we support each other, and we’ve got each other’s back. Even when it doesn’t seem like it, I know I can count on someone else here.
One 8-year-old son with autism confirmed this perspective stating a healthy family is “a family that gets along nicely and that each member of the family is there for one another.” While the content of each family’s support system varied, most families were consistent in expressing that their support systems provided stability and resources in the midst of situations that threatened their family’s health. One mother shared: I honestly think it’s the support. I think it’s that we have, beyond just the internal struggles that we face, because sometimes the communication issues and the previous traumas do impact our ability to parent successfully together or to be calm in a storm together, I think the external support has been astronomical for us.
While other themes such as balancing individual and whole needs, the centralization of autism, stress, and connection brought variety and a “roller coaster” effect to families’ everyday journeys, families consistently articulated that support systems were a key element that encouraged families along their journey toward health.
Discussion
The purpose of this study was to understand families’ experience of family health for families with children with autism, and to identify those factors and processes that contributed to families’ experiences of health. Results suggest families with children with autism depict family health as a journey, fueled for many, by a family identity. The journey was influenced by families being connected together; finding a balance between individual and whole family needs and schedules; centralizing autism itself within family functioning; experiencing stress of chronic planning and advocacy; and activating needed internal and external family supports. Considered collectively, the resultant themes raise new and insightful considerations for providers working to support children with autism and their families.
Family health as journey grounded in identity
The current finding of the journey experience as a manifestation of the process of experiencing family health provides new insight within the autism literature. Previous autism research examines family identity surrounding the diagnosis of autism (Hays & Colaner, 2016), but not the relationship between family identity and health. Perhaps as families gain traction and grounding in the formation of their identities, they create space through which they can then move and grow more confidently in the world around them. Extension of family identity from the past into the present and future of the family journey may support navigating everyday life after diagnosis. This identity can then act as a gauge from which families can measure the extent to which their everyday enacted lives match who they are and who they want to be, serving as a barometer about the overall family health climate.
Families in this study who had difficulty articulating an identity, or describing priorities for the years ahead, seemed to describe less intention and more reactivity to daily life. These families shared perspectives of being out of control, on a roller coaster, or experiencing chaos. These perspectives align with previous research describing the clearly stressful and at times chaotic family life for families with a child with autism (Bessette Gorlin et al., 2016). However, for other families, the chaos was still there, but experiences of instability were understood within a context that the chaos was part of, but was not the whole. These families were able to detach their identity as a family from their difficulties related to autism in order to maintain a larger perspective of family health. Providers can help families reflect on who they are as a family including what makes them unique, not only in terms of having a child with autism but also toward a broader awareness of family identity. Supporting families to develop and articulate family identity potentially may help to ground families during a well-documented journey of ups and downs.
Family member connection
Every family consistently described that being together in shared time and space promoted their family’s health. These findings align with previous evidence suggesting that families of children with disabilities who perceive themselves to be doing well and resilient feel connected to one another within the family (Breitkreuz et al., 2014). Yet the very interventions families diligently participate in to support their child with autism often create overwhelming schedules that leave families with limited time or energy necessary for togetherness. The potential for intensive interventions for a child with autism to inadvertently negatively impact family health exists. Families in this study described that often when they carved out down time, members were exhausted from the intensive schedule, leaving little to no energy necessary for connection. In addition, families frequently described that inherent to autism, social interaction was a critical focus of the child’s intervention program and as such when their child with autism was home, the child needed a break and disengagement from social interactions, which in turn detracted from opportunities for family connection.
Providers can promote family member connection by engaging natural opportunities for social interaction. For example, clinic-based sessions can be designed to incorporate multiple members of the family and teach healthful patterns of social interaction to facilitate family time for togetherness outside of therapy. Providers can support families to create routines that intentionally foster opportunities for togetherness and enjoyment of family members, building on literature supporting the use of routines as protective of family functioning (Boyd et al., 2014).
Providers can also consider the extent to which they inadvertently contribute to family disconnection by asking if recommended interventions include families as the very context and mechanism through which the child’s development occurs. Literature suggests a shift from viewing families of children with disabilities as needing to adapt to the needs of a child with a disability as though the child is the problem, toward providers recognizing the socioecological value of the family as the context of change (McConnell et al., 2013).
Parent-mediated interventions provide one evidence-based model of contextualized family care with improved family level outcomes such as family cohesion, empowerment, and adaptation (Factor et al., 2019). McConnell and colleagues (2013) caution providers from providing interventions that are “slotted” (p. 154) into existing routines and instead underscore the need for authentically contextualized interventions that are part of the everyday family life fabric. Parent coaching approaches offer another example of a contextual autism intervention (Little et al., 2018), although further research is needed to examine parent coaching interventions addressing the family as a unit.
Decentralizing autism within family routines
This study’s finding regarding the centralization of a child with autism within family functioning strongly resonates with previous literature highlighting the influence of autism on family life. Parents of children with autism report their child’s communication, sleep, self-care skills, and diet as the most challenging areas leading to decreased community engagement due to parental anxieties regarding other’s perceptions and potential disruptions by their child in the community (Galpin et al., 2018). In addition, the sensory experiences of family activities such as the sounds or the tactile elements influence parental decisions about the types of activities families do, the amount of planning required, and the perception of shared meaning within family activities (Bagby et al., 2012). This planning around the sensory experiences in turn centralizes the focus on the child with autism in everyday family life.
Families experience restricted participation when routines become overly patterned potentially compromising spontaneity, flexibility, and adaptability (Boyd et al., 2014). At the same time, family routines are essential for providing structure and stability for families of young children and adolescents with autism (Bagatell, 2016; Larson, 2006). Evidence suggests that families of children with disabilities perceived as having resiliency intentionally carry on with “business as usual” (p. 352) within normal family routines (Breitkreuz et al., 2014). Rather than not participating in family routines, these families modified aspects of the activity to support the child with a disability to participate. Families perceived as less resilient of those studied tended to centralize family routines around the child with a disability when describing their family characteristics (Breitkreuz et al., 2014).
Attention to sibling needs within families of children with autism can also support families to balance individual and whole family needs by shifting focus from the child with autism to siblings. Parents having intentional awareness and communication with siblings decentralizes the child with autism, and potentially mitigates negative sibling outcomes exhaustively described in the literature (Leedham et al., 2020; Shivers et al., 2019). Including relevant questions to parents about siblings can foster parental perspective taking and awareness about individual sibling needs within the family unit.
Providers can encourage family reflection on the influence of autism in the family dynamic, thus cultivating awareness around patterns of functioning that may centralize around the child with autism. Encouraging families to develop intentional responses to the influence of autism continues to build upon research understanding the centralization of autism and extends previous work by considering balance of family member needs as the potential mechanism of change toward decentralizing the child with autism within family functioning. Providers can work with client families to identify areas where whole family needs and individual needs may compete for familial energy, and can help families develop contextualized, specific solutions to balance and respect the needs of all family members.
Role of support systems in stress mediation
Every family in this study consistently identified the role of internal and external support systems in promoting their family health journey. The chronic and impactful stress of parents with a child with autism is clearly outlined in previous literature (Bonis, 2016; Mancil et al., 2009). Mancil et al. (2009) articulate that both formal and informal social supports can mediate parental stress by serving as a coping mechanism. Formal supports can include parental support groups or family therapies, while informal supports can include friends, family members, or neighbors problem-solving together, thus decreasing a sense of family isolation. This study adds to the literature on parental stress and support systems by placing these considerations in the whole family context. Perhaps support systems are not only a stress mediator for parents but also a health mediator for the family unit, which in turn supports both child and parental outcomes. Providers can work with families to develop robust and multifaceted support systems through teaching self-advocacy and advocating for client and family needs.
Limitations and future research
This study specifically examined family health for a subset of families of children with autism. Generalizability is not the intent of qualitative research; however, some elements of the depicted family health journey may be unique within this subset of families. These include the pull between individual and whole family needs magnified by the pull of autism and stress surrounding care for the child with autism. In addition, a lack of member checking limited confirmation of findings by participant families. Finally, the demographic of participant families was limited in diversity of structure and ethnic background, perhaps excluding elements of family health that may be important to diverse populations. The unique geographic region in which participants lived provided access to family activities not necessarily accessible by families of other geographic areas. Future research could include a purposive sample to include families from diverse backgrounds within a variety of geographic areas.
Currently, a few holistic measurement tools to identify family health needs and measure change exist for families of children with autism. Existing tools include measures of specific constructs such as parent stress (Autism Parenting Stress Index, Silva & Schalock, 2012) and family resilience (Family Resilience Assessment Scale, Gardiner et al., 2019). Future research could include development of family health measures that evaluate complex interactions such as those identified by participants in this study. In turn, these measures could harmonize the current dissonance between measuring everyday life participation valued by families and community members with widely used tools measuring children with autism’s specific impairments (McConachie et al., 2015).
Conclusion
This study sought to examine experiences of family health for families of a child with autism through a socioecological lens to capture interrelationships and obtain a holistic family unit perspective. Understanding the transactional nature among relationships maximizes and sustains the full potentiality of developmental outcomes of children with autism by understanding the nuanced complexity within the child’s family. Sixteen families were interviewed in a casual, conversational way that garnered interactive co-constructed perspectives from children and parents. Findings suggest that family health for families of a child with autism is a journey guided for many by family identity, encouraged by a support system, and impacted along the way by experiences of connection, balance, the centralization of autism, and stress. These family perspectives can inform future research on these constructs and can contribute to developing interventions that specifically address family identity formation, strategies for supporting balance, decentralizing the child with autism within the family perspective, and stress management through contextually relevant supports in order to foster families’ journeys toward flourishing family health.
Footnotes
Appendix 1
Acknowledgements
The authors thank the participant families for sharing their homes, time, and experiences with us and without whom this study would not have been possible. The authors also thank the University of New Hampshire Hamel Center for partially funding this research study. Finally, the authors thank Margaret Arms, PhD who provided constructive guidance with the discussion section and editing.
Author contributions
S.L.S. was responsible for study oversight including study concept and design. Both S.L.S. and H.B.M. were responsible for data collection, analyses, result generation, and manuscript development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The University of New Hampshire Institutional Review Board for the Protection of Human Subjects in Research approved all procedures for this study, IRB#6923.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the University of New Hampshire Hamel Center. The findings were presented at the 2019 American Occupational Therapy Association Conference in New Orleans.
Patient consent
Written adult and parent consent was obtained by all participants. Oral child assent was obtained for children ages 2–12 years and written assent was obtained for children ages 13–18 years. For a child of any age with a disability that precluded written assent oral or non-oral assent or dissent was obtained.