
Abstract
Autism services in Qatar are expanding rapidly, but focus predominantly on young children. The shortage of qualified autism providers and minimal opportunities for autistic youth to participate in school, work, and community have led to a growing population of autistic youth transitioning to adulthood with substantial unmet needs for behavioral support and instruction in critical life skills. Our objective was to identify the needs and preferences for respite care for autistic adolescents and young adults in Qatar utilizing family and stakeholder input. Researchers from the United States collaborated with researchers and community leaders from Qatar to evaluate perspectives regarding respite care with families of autistic people (n = 11) and providers/community stakeholders (n = 20) through surveys and focus groups. Four main themes emerged including (1) a need for trust and reliability of individuals and of systems to support autistic adults, (2) prioritizing quality of life for autistic individuals and their families, (3) seeking meaningful inclusion, and (4) challenges stemming from service delivery systems. Families in Qatar endorsed clear interest in respite care services for young adults with autism, regardless of their child’s age. This study highlights the value of including both provider expertise and family concerns in developing new services for an under-served community.
Lay abstract
Qatar is expanding the services that it offers for autistic people, but these services focus mainly on diagnosing and treating young children. Because there are not enough autism providers in Qatar and few opportunities for autistic youth to participate in the community, more and more autistic teens and young adults have unmet needs during their transition to adulthood. The goal of this study was to conduct a needs assessment of transition-age autistic youth in Qatar and their families in order to inform the development of an adult respite care and support center. Respite care is a service that provides families with stress relief and time to participate in activities that are more difficult to do when their loved one with a disability is with them. The objective of this study was to use family and stakeholder input to identify the needs and preferences for respite care for autistic youth in Qatar. The project was conducted with a local research team in Qatar and a team of clinical researchers in the United States specializing in autism. Stakeholders, including parents of autistic people and providers working with individuals with autism, completed surveys and participated in focus groups. Families and providers in Qatar were very interested increasing services for young adults with autism to improve quality of life, although wanted to make sure the service providers would be reliable and trustworthy. Implications from this study may substantially improve the lives of autistic adults in Qatar.
Keywords
Introduction
Due to its nature as a neurodevelopmental disorder with significant genetic etiology, autism spectrum disorder (ASD) is generally considered to be invariant across sociocultural contexts. However, cultural factors are highly relevant to developmental outcomes and quality of life for individuals with ASD and their families (Norbury & Sparks, 2013). This study aimed to evaluate needs for transition-age autistic youth in Qatar and their families as the first step in the development of an adult respite care and support center, based on previously identified priorities from a local non-governmental community organization providing autism supports in the area. Autism is diagnosed at lower rates in the Middle East than in Western Europe and North America (Qoronfleh et al., 2019); however, unlike many other regions with lower diagnostic rates of ASD, many Middle Eastern countries have access to important health, educational, and fiscal resources. Leveraging their financial resources, along with a culture of strong commitment to the advancement of scientific and medical knowledge within these countries (Falagas et al., 2006), the Gulf Cooperation Council (GCC) region (which includes, Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates) has made considerable advancements in expanding both research and access to services for autism. Nonetheless, there are continued challenges in making services widely available to autistic people and their families.
Within the GCC, Qatar has made a specific public commitment to advancing research and services for individuals with ASD and their families, beginning with their leadership on the United Nations resolution establishing World Autism Awareness Day in 2007 (United Nations, 2008), the recognition of autism as an official disability category by the national government in 2012 (Qatar Ministry of Development Planning and Statistics, 2016), and more recently with the announcement of the Qatar National Autism Plan (Ministry of Development, 2020). There has been substantial progress in access to services over the past few decades, through hospitals and medical centers, therapeutic centers for children with disabilities, and expanding school supports and educational centers (F. A. W. Alshaban, 2018; Guldberg et al., 2017). Autism advocacy also continues to progress through leadership by the Qatari Autism Society. Despite these important advances, individuals diagnosed with ASD in Qatar have high rates of co-occurring intellectual disability and high support needs, with few services available to them (F. Alshaban et al., 2019). Furthermore, parents of youth with ASD in Qatar report low quality of life, particularly with respect to mental health, with significant concerns over unmet service needs for their children (N. Kheir et al., 2012).
These stressors are particularly high for families of autistic adults, for whom there are almost no services available in Qatar. This reflects a worldwide trend, as autistic adults have become recognized throughout the world as an under-served, and under-researched, population (Baker-Ericzén et al., 2018). Autistic adults across all cognitive ability levels report lower quality of life compared to typically developing adults (Moss et al., 2017; van Heijst & Geurts, 2014). Adaptive behaviors, which are critical to independent living, are impacted in ASD (Matthews et al., 2015; Pugliese et al., 2015; Smith et al., 2012). Autistic adults routinely struggle to care for themselves and to navigate the complex systems required to work, obtain appropriate medical and mental health care, manage finances, and accomplish all the other tasks needed to live independently as an adult (Camm-Crosbie et al., 2019; Farley et al., 2009; Shattuck et al., 2013), thus relying on supported living arrangements or, more commonly, residing with family (Barneveld et al., 2014; Orsmond et al., 2013). Many autistic adults are socially isolated and have few opportunities for interaction with others (Billstedt et al., 2005; Orsmond et al., 2013). The difficulties faced by autistic adults are exacerbated by the fact that there are relatively few services available for them, even in countries with relatively well-developed service systems for autistic youth (Camm-Crosbie et al., 2019; Shattuck et al., 2013). The transition to adulthood is an extremely challenging time for autistic youth and their families. This is especially true in Qatar, where families report that there are insufficient supports for autistic children and a profound lack of supports for autistic adults (Guldberg et al., 2017; N. M. Kheir et al., 2012).
The difficulty obtaining appropriate supports for autistic youth and adults has driven attention to the well-being of their families as well. Caregivers of individuals with ASD experience significant stress throughout the lifespan (Smith et al., 2010). Parents of adolescents and adults with disabilities often describe feeling isolated and unsupported, particularly once their children are no longer in school (McKenzie et al., 2017; Shattuck et al., 2013), which removes a source of direct intervention and support for families. Thus, in Western nations, respite care often becomes a critical service for families with transition-age autistic youth. Respite care is a service that provides appropriate supervision and support for individuals with disabilities while they are away from their families. The primary goal of respite care is to provide families with time away from caregiving to relieve stress and enable caregivers to attend to activities that are more difficult when their loved one with a disability is with them (e.g. personal medical appointments, leisure activities with family or friends, and household tasks; Jeon et al., 2005). Findings from Western countries generally indicate that families experience decreases in stress, improved marital and family relationships, and even benefits in physical and emotional well-being when their loved ones participate in respite care (Harper et al., 2013; Pilapil et al., 2017; Whitmore, 2016). There have also been findings of direct benefits for individuals with disabilities, including improved physical health, enhanced social skills and relationships, and gains in life skills (Spruin et al., 2017).
Experts on respite care emphasize the importance of taking individual and family preferences into account to be maximally effective. Even in areas where respite care services are well-established, families encounter obstacles to utilizing these services such as: difficulties navigating systems to access care, lack of knowledge of available services, and lack of trust in care providers, who are sometimes perceived as underqualified and/or dismissive of family concerns (Jeon et al., 2005; Pilapil et al., 2017; Wodehouse & McGill, 2009). To increase the acceptability and utility of respite care, providers must consider each family’s circumstances and values in caring for their disabled loved ones and effectively communicate with families about expectations for respite care. This necessarily includes training in culturally competent practices and consideration of religious and cultural factors in providing appropriate respite care. Cultural considerations may be particularly important in the provision of respite care in Qatar, where many of the service providers for individuals with ASD and other disabilities are from notably different cultural backgrounds (e.g. the United Kingdom, the United States, and Western Europe) than many of the Qatari and non-Qatari families receiving services, who are more often from other GCC countries or Muslim backgrounds (Guldberg et al., 2017). This also requires examination of the ways in which these needs are currently met; in Qatar, as in many countries around the world, daily care and living needs are often attended to by family and other non-professional caregivers (Verbakel et al., 2017). In Qatar, many families employ in-home nannies or housemaids who provide care to children or in some occasions hire in-home professional help for their child (N. M. Kheir et al., 2012).
This study was undertaken as a partnership between a Qatar-based non-governmental community organization and a team of clinical researchers from a large autism specialty center at an academic medical setting in the United States, with the stated goal of identifying stakeholder priorities for adults’ services in Qatar, with a primary focus on the provision of formal respite care services. The objectives of this study were to use stakeholder input from focus groups to identify service priorities for autistic adults in Qatar, define key considerations for provision of services to autistic adults and their families, and generate recommendations to guide the development of services for autistic adults.
Methods
Procedures
The goal of this study was to conduct a needs assessment of transition-age autistic youth in Qatar and their families in order to inform the development of an adult respite care and support center, in line with stakeholder priorities previously identified by the Qatar-based non-governmental community organization. The project was conducted collaboratively with a local research team in Qatar associated with the team intending to develop the care center, and a team of clinical researchers in the United States specializing in ASD. This project was conducted in compliance with standards established by the United States institution’s Institutional Review Board (IRB). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Needs were assessed through surveys and focus groups conducted in the context of a 2-day workshop. The workshop brought together stakeholders to review the state of services for transition-age youth with ASD in Qatar and to learn more about respite care models in the United States. As the trusted, on-the-ground organization, the local team in Doha, Qatar, led the recruitment process. Utilizing advertisements (e.g. flyers and emails) and leveraging their connections with local clinics, schools, and non-profit organizations for individuals with ASD and their families, the Qatar team recruited key stakeholders for participation in two stakeholder focus groups. The parent stakeholder (“parents”) group included mothers of individuals with ASD in Qatar. The provider stakeholder group (“providers”) included medical and therapeutic providers, clinical diagnosticians, educators, and leaders of non-governmental organizations and relevant governmental ministries working with the autistic community in Qatar. See ‘Participant’ section for complete details. As noted, focus groups were conducted along with workshops over the course of 2 days, with the first day focused on providers and the second day focused on parents. Notably, participants in the parent focus groups first participated in an educational workshop that provided an overview of respite care (i.e. goals and various models of respite care, and considerations in making decisions about respite care), presented by the US team. This overview was identified as a critical first step by the Qatar team, as many families in Qatar were likely to be unfamiliar with the concept of respite care, and therefore would have limited ability to provide input on how it could be implemented in Qatar without some background. After a break, parent participants then participated in focus groups.
Across both days, participants were divided into two focus groups, with each focus group co-led by a team of two clinical researchers from the US team. Parent participants were divided into two separate focus groups on the basis of language preference, with one group conducted entirely in English and the other group conducted in Arabic, with live, sequential interpretation by a bilingual member of the Qatar team. Focus groups were guided by the clinical-researcher teams, using open-ended questions generated by the full team, with distinct questions for providers versus parents. Both providers and parents completed brief written surveys to provide basic demographic information. Parents also responded to survey questions about their potential respite care needs and priorities. Prior to data collection, the survey and focus group questions were translated from English to Arabic by a certified translator and then checked by a bilingual researcher who agreed with the translation.
Participants
The total sample included 31 stakeholder participants across all four focus groups, with 11 parent participants and 20 provider participants. All participating parents were mothers and ten of their children were male (one female). Most were married (91%), were not currently employed (73%), had a college degree or higher (82%), and were raising multiple children at home M = 3.8 and SD = 2.0). Their autistic child’s age ranged from 5 to 31 (M = 16.8 and SD = 7.2). They were evenly divided between Qatari citizens (45%) and expatriates/foreign nationals (55%). Most of their children had previously received or currently received educational supports (73%) and some form of therapeutic intervention (73%). Approximately half indicated that they were active members of a parent advocacy group. Half (n = 6) preferred to communicate in Arabic, with the other half (n = 5) preferred or felt equally comfortable in English. Table 1 presents additional details.
Parent survey.
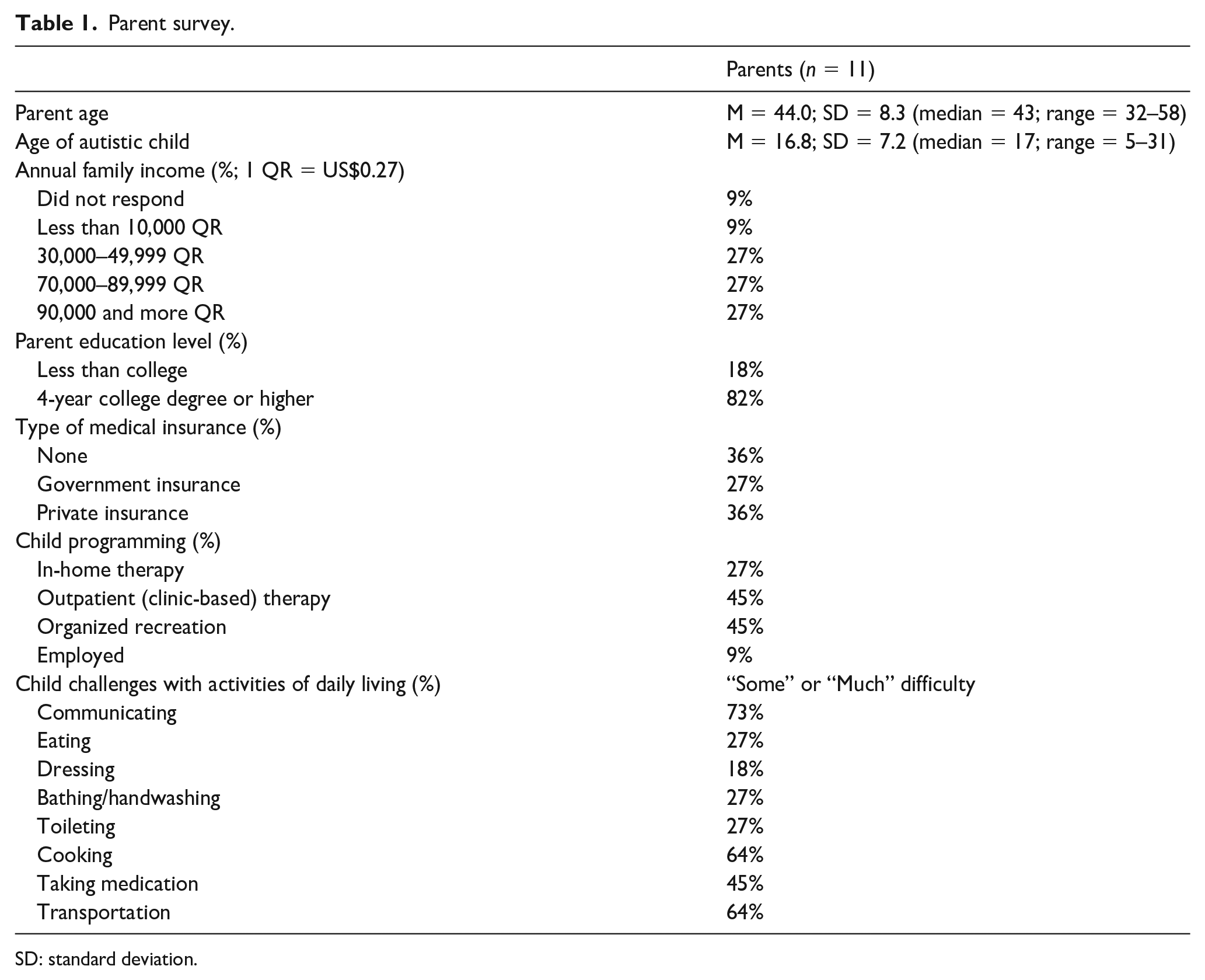
SD: standard deviation.
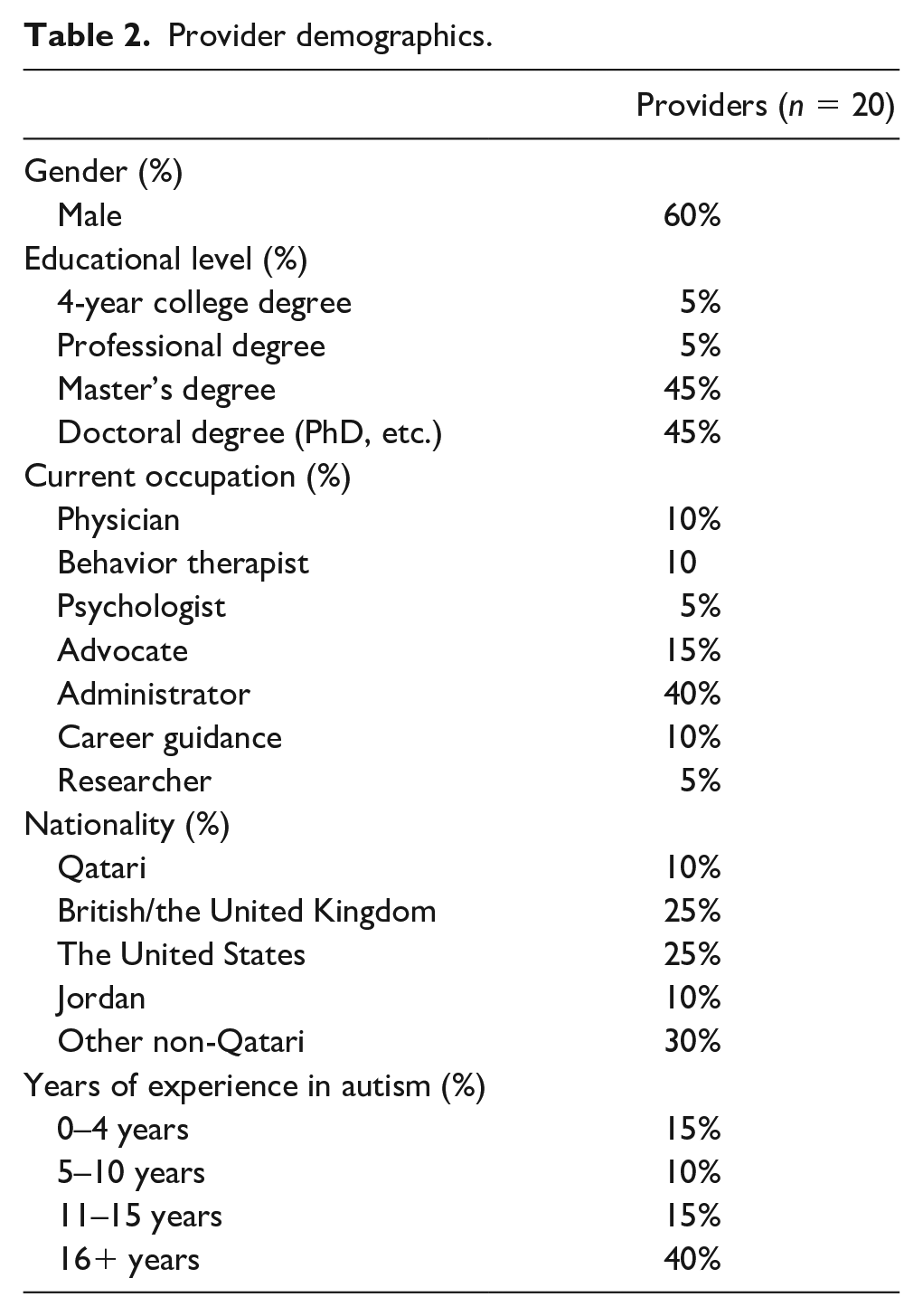
Providers, by contrast, universally preferred to communicate or were equally comfortable communicating in English. Most providers were administrators (generally in educational settings), with others identifying as therapists, medical providers, or vocational specialists, and a smaller number employed primarily in research and/or policy. Providers were overwhelmingly non-Qatari in nationality, most often from English-speaking countries. This is common in Qatar, where nearly 90% of the populace is composed of foreign nationals (Statista Research Department, 2020). The rapid economic growth of the GCC countries, including Qatar, during the 20th century following the discovery of new energy sources, led to the increase in recruitment of foreign national workers from all over the world, and it is expected that the demand for foreign workers in the GCC will continue to increase (Sheikh et al., 2019). Participants in the sample were also highly educated and highly experienced, with nearly all having advanced degrees and the vast majority having a decade or more of experience working with autistic individuals. Table 2 presents the additional details.
Provider demographics.
Data analytic approach
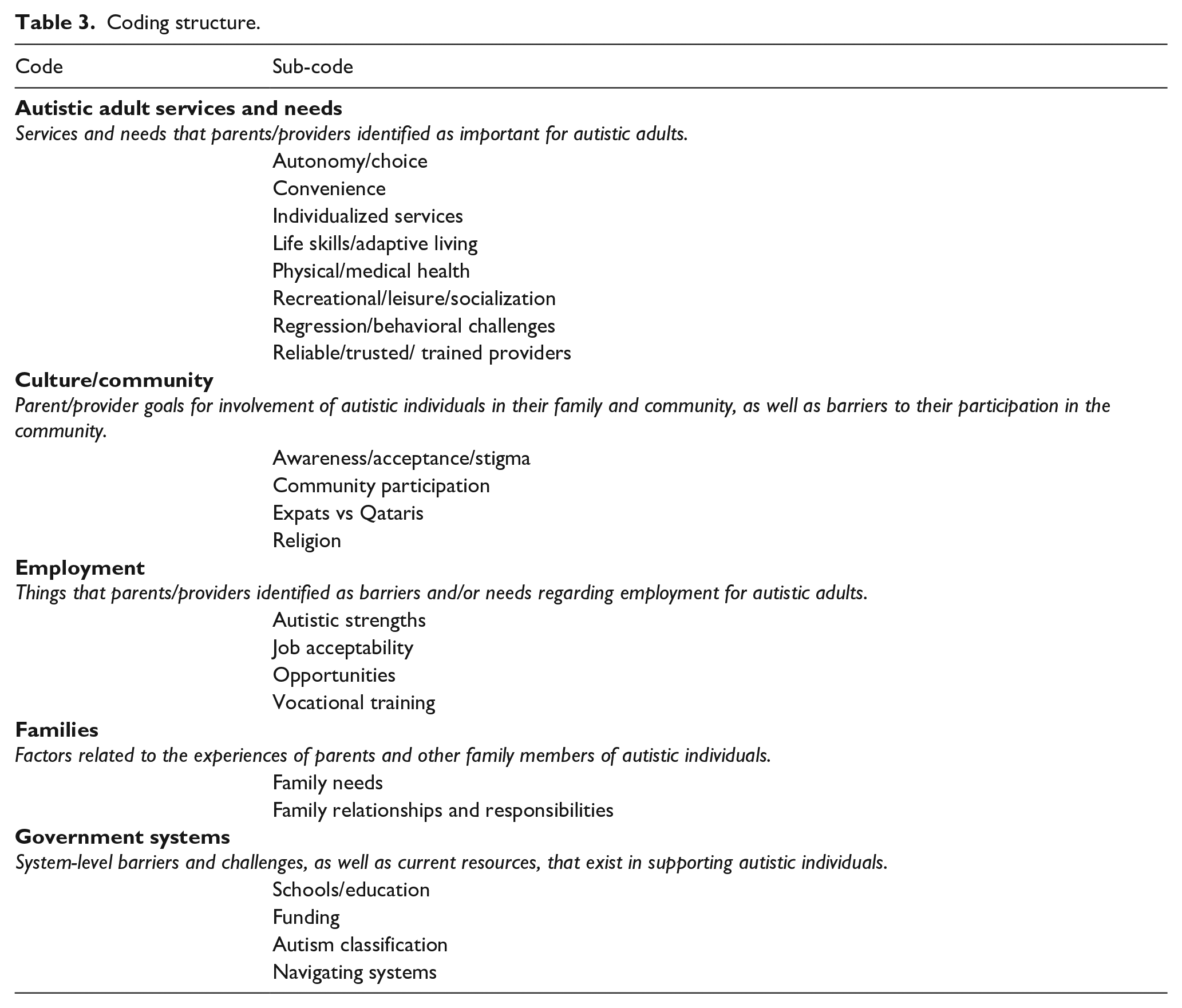
All focus groups were audio-recorded. English focus groups were transcribed by a research assistant and reviewed by a second research assistant. Any inconsistencies were reviewed by the author S.H. and clarified. The Arabic interview was professionally translated and transcribed and reviewed by a bilingual researcher (S.A.). The codes and transcripts were imported into Dedoose for data management and coding. A thematic analysis approach (Braun & Clarke, 2006) was utilized for qualitative analysis of the transcribed focus group data. All four members of the US team (S.H., A.R., A.V., and C.P.) read the transcriptions and generated proposed codes. The team then met to review proposed codes and worked jointly to create a final consolidated coding structure (Table 3). This coding structure was then reviewed by the lead members of the Qatar team (S.A.) to provide validation from their local and cultural expertise that the coding structure was appropriate. All four transcripts were then independently coded by two members of the US research team (S.H. and A.V.), allowing for more than one code to be applied to each excerpt. A consensus coding approach was used, such that the independent codes were then reviewed by both raters, and each excerpt was assigned a final code (or codes) by identifying the code(s) assigned by both raters in the independent phase. If the two independent raters had not assigned any overlapping codes, the excerpt was discussed and a consensus code was assigned by both raters. For each excerpt in which raters had to work jointly to identify a consensus code, a third rater (A.R.) reviewed the excerpt and proposed consensus code to ensure that the final consensus code was accurate. Inter-rater reliability in the independent coding phase, defined as agreement on at least one code for a given excerpt, was strong overall (k = 0.82). Once all four transcripts had been completely coded, the US team (S.H., A.R., A.V., and C.P.) reviewed the coded transcripts and worked collaboratively to identify themes, utilizing an inductive approach, and the final themes were reviewed by the leader of the Qatar team (S.A.).
Coding structure.
In order to enhance the trustworthiness (reliability and validity of qualitative research) of the data, the two researchers who primarily coded the qualitative data (S.H. and A.V.) reflected on their positionality in interpreting the data. One researcher (S.H.) is an Arab American woman with experience in ASD research within the Arab community. At times, this was disclosed to focus group participants to increase trust and improve participants’ openness in responding to questions. The second researcher was a European American woman, with research experience in ASD but limited experience working with Arab communities. This allowed her to approach data analysis with a more objective view. The quantitative responses of families to the surveys were tabulated and are presented here in tables. No statistical analysis of the quantitative data was conducted, given the small sample size.
Community involvement statement
A director of a school serving children with ASD in Qatar reviewed and provided feedback on the survey questionnaires and focus group questions prior to the implementation of the study. No other members of the autistic or autism communities were involved in the development, implementation, or interpretation of this study.
Results
Parent surveys
On survey questionnaires, parents indicated that their children struggled with several activities of daily living, with the greatest levels of need identified in transportation, cooking and meal preparation, and communication (Table 1). Parents varied widely in the level of supervision they felt was needed for their child; some indicated that their child should remain in eyesight at all times to ensure safety (27%), while others endorsed that their child could be left alone for brief or even extended periods. On average, parents did not feel that their child’s behavior was particularly difficult (average rating = 3.3 on 10-point scale; 1 = not difficult and 10 = extremely difficult). Consistent with these ratings, less than half of parents endorsed child problems with inappropriate behaviors (36%) or elopement (36%), with none indicating that their child engaged in self-injurious or physically aggressive behaviors on the surveys.
Parents were broadly interested in potentially utilizing respite care, with the most strongly endorsed barriers to respite care being its lack of availability at present (73%) and concerns about provider training (55%). Some parents also acknowledged feelings of guilt (18%) and difficulty trusting other caregivers (18%). Parents most commonly indicated that they would seek respite care services for stress relief (54%), although increasing their ability to effectively care for their son/daughter (54%) and attending to personal business (36%) were also frequently endorsed. When asked to identify factors that would increase their comfort with seeking respite care services, parents most strongly valued that caregivers have prior experience in autism (73%) and appropriate supervision (73%). There was no clear consensus or pattern among parents regarding the potential length of time that respite care would be provided, perhaps reflecting the fact that these services do not yet exist, and making it difficult for families to consider these types of specific details.
Parent and provider focus groups
Following completion of the structured surveys, participants were placed into smaller focus groups as described above (see “Procedures”). There were no notable differences between parents and providers in terms of codes endorsed. The results below reflect the primary themes endorsed by participants, as identified through the inductive thematic analysis. A brief summary of the codes and sub-codes endorsed is presented in Table 3.
Autistic adult services and needs
Participants repeatedly highlighted the importance of having reliable, trusted, and well-trained providers. One provider said, If the purpose of the respite care [. . .] is to alleviate the pressure valve which is there for the families, our parents would feel twice as stressed handing their child over to people who don’t know their child [. . . there is a] massive need there for the parents to be able to, with absolute confidence, have another adult [they] actually trust.
Parents echoed this sentiment, emphasizing that “we know our children the best, and we want to feel safe regarding our children.” Providers also discussed the roles of nannies and housemaids in caring for autistic adults, as there was a common theme across focus groups that it is often assumed that care of autistic adults and children will fall to these untrained individuals. Providers emphasized, however, that the demands placed on nannies and housemaids are high and that if they are to become primary caregivers, they require additional training. As one provider explained, The thing about the maid or nanny culture is this: They don’t have a choice in the care of this child [. . .] she is put in a situation where it could be dangerous for her, difficult for her. If something happens to the child, she is held responsible although she has no training and she has no choice.
Variables related to quality of life for both autistic individuals and their families were often discussed. Participants mentioned the importance of developing adaptive living skills so that adults are less vulnerable to problematic or dangerous situations. Furthermore, quality of life was discussed in terms of young adults having opportunities for recreation, leisure, and socialization. One parent said, “we want him to be confident, to achieve something.”
Relatedly, participants expressed that without the appropriate stimulation and support, young adults may regress in their functioning or develop significant behavior problems. Parents described challenging behaviors from their autistic sons and daughters, such as “scream[ing] if [they] didn’t fill his request” or throwing objects across the room when upset.
Participants also highlighted the importance of individualizing services for autistic adults, given heterogeneity in functioning across the autism spectrum. Along with this, the value of respecting an individual’s autonomy was mentioned by providers: I think [. . .] it’s all people having an element of control and choice of their own future [. . .] Starting with them, with their needs, with their wants, with their aspirations, and providing that pathway forwards.
Parents also described a desire for providers to provide tailored and individualized services in this way. As one parent stated: “We are not aiming to get rid of our son. We are trying to find the place where he will benefit and rehabilitate.” Many emphasized that their child had skills that were being overlooked or that their child’s unique aptitudes had not been identified or developed, despite years of treatment and education.
Culture/community
Participants highlighted a number of issues related to ASD awareness, acceptance, and stigma in Qatar. Some participants felt that stigma persists and makes life more challenging for families. One parent expressed, “It’s society awareness is the problem [. . .] Then it ends up for the families to stay at home sitting with the kids because they cannot bear the society look to them.” However, other participants identified that ASD-related stigma has decreased somewhat in Qatar as awareness has steadily increased. One provider shared that, “everyone has now heard about autism, everybody at least knows someone in the family or in other families [. . .] I feel like we have done a lot of progress in terms of awareness.” Despite this increase in awareness, some participants felt that actionable change has not yet followed, particularly in terms of adequate funding for resources. Many providers and parents expressed a continued interest in increased inclusion and community participation.
Another topic that emerged specific to the culture in Qatar was differences between foreign national residents (i.e. “expats”) and Qatari citizens. Participants shared that certain benefits, like a social allowance and national health insurance, are only available to Qatari citizens but not to foreign nationals. In addition, one provider highlighted that most workers in the field are foreign nationals who go back to their home countries for the summer (as is true across employment sectors in Qatar, as nearly 90% of the population is made up of foreign workers; Statista Research Department, 2020), severely limiting access to ASD services during this time.
Employment
Both parent and provider participants highlighted that employment and vocational opportunities for autistic adults in Qatar are limited. Providers mentioned that the lack of opportunities may be stemming, in part, from employers having inadequate training to employ autistic individuals: [. . .] there is a willingness of employers to bring onboard people with special needs, also people with autism. However they are afraid because they are not trained. They don’t know how to handle them, there is a lot of misinformation that they can be aggressive, they can be difficult, they can have tantrums, which yes, it might be, but this is not a general case.
Parents also highlighted the difficulty identifying vocational opportunities, and at times suggested that facilities set up in a sheltered workshop model would provide safe ways for their adult sons/daughters to have appropriate jobs. Others suggested specific activities at which their own children would excel (e.g. working at a coffee shop) based on their individual interests and skills, relating back to messages throughout the conversation about the individuality of autistic people. One parent stated that, “maybe he’s not qualified for academic studying, but he has strong memorizing skills, he memorizes Quran. If he memorized the Prayer calling, he would perform it.”
Frustration about currently available employment opportunities was also notable. Although participants appreciated governmental policies requiring that large employers designate positions for individuals with disabilities, they indicated that many employers feel unable to actually accommodate these employees in the workplace. In these situations, they described that employers reportedly may provide a salary to an autistic adult, but do not give them any job responsibilities (e.g. “the employer tells them to stay at home because they are problematic”). Another factor related to the availability of job opportunities, as brought up by providers, was that not all jobs for autistic young adults may be acceptable to all families: There is a lot of cultural implications in this region, so maybe a parent is not okay with a child working at the supermarket. But he is okay with the child working at the national library stacking books, so what I am trying to say is that there is definitely a cultural component here [. . .] there are things that parents will be okay or you know, the culture will be okay with, and things that wouldn’t [. . .]
Interestingly, parents did not necessarily agree with this perspective, with some emphasizing that any opportunity for their child to be engaged in meaningful work would be welcome: My son has some skills but the state didn’t help him to put my son in any place where he can perform something like wrapping gifts, work in a factory, or newspapers; maybe other mother won’t accept that but I’ll accept to put [my son] in any place in the state.
Families
Participants identified extensive family needs during the focus groups related to parental burden and stress. One parent described that mothers often find themselves lacking sufficient support: Culturally speaking [. . .] for them to find support from their spouses or what not, especially when there is a single bread winner, so [that] spouse kind of assumes that their job is to feed them, everything is on you. So, I mean, so there are a lot of stressed parents in the community undoubtedly that don’t have any support at all in any way.
Providers mentioned instances of parents feeling a significant burden leading to abuse, neglect, and child abandonment: We have some cases from the age of four, five, they get to the [inpatient unit] after which they refuse to take them home. And they stop visiting and they stay for five, ten years. Some [. . .] I’m really sorry to say this but they left their children, and they went back home.
Relatedly, parents described the difficult decisions they face in caring for their autistic child while also trying to uphold other familial relationships and responsibilities as well as the increasing challenges in caring for them as they age: Consumed . . . the mother is always consumed, and we gave up on schools and jobs. Taking care of them is a full-time job, and every day they are getting older and stronger. When I go to mall with [Child] and his brothers, he pulls me, thanks to God that I’m wearing a veil so when my tears drop no one can see them.
Government systems
Financial and funding–related issues were often discussed. For example, parents and providers both discussed that services are often too expensive, and insurance does not adequately cover what is needed. In particular, a provider mentioned that funding is limited for adult-focused programs and that, “people will pay for early intervention, but they would not pay for adults.”
Participants, particularly providers, also explored the challenges of navigating government systems: We don’t have authorities vested with the responsibility of producing policies and strategies [. . .] so we are working in silos and each one is doing different things [. . .] Responsibility is like a ping pong, the ministry of health, the ministry of social affairs the ministry of education, the ministry of I-don’t-know-what, and in between there is this huge void, that you have the people with special needs and their families.
In terms of navigating systems, participants highlighted one specific challenge, lying within which system is responsible for supporting autistic individuals: the ministry of health or the ministry of education. One parent expressed that this is in part due to parents advocating against highlighting autism as a category in the healthcare system.
Although the focus groups were focused on young adult needs, some providers and parents also acknowledged issues related to schools and education, highlighting that the lack of preparation in school for transition to adulthood exacerbates the difficulties faced by families later on. One parent expressed that considering this is important when exploring adult needs because, “it also affects the level of respite care that will be required at the later stage because they don’t get the education now, you are looking at the worse population.” This idea was echoed by a provider who shared that, “[. . .] you can’t, at this point expect that a young adult with autism has necessarily received education or if they did receive an education, was it really tailored to their needs.”
Themes
Cutting across the codes and sub-codes discussed the following themes emerged across the focus groups (Figure 1):
Theme 1: a need for trust and reliability of individuals and of systems to support autistic adults emerged as a relevant theme. Participants are seeking trust in providers, employers, and government leaders to address the needs of young adults and are looking to ensure they can rely on those entities to provide and support.
Theme 2: prioritizing quality of life for autistic individuals and their families emerged as an important theme across focus groups. Participants endorsed the need for autistic young adults to engage in meaningful experiences, unique to their individual needs, in terms of safety, adaptive living, socialization, leisure, and employment. Such factors were discussed as way to also indirectly improve parents’ quality of life, which was presented as significantly impacted.
Theme 3: the theme of meaningful inclusion emerged across codes and sub-codes, highlighting the importance to families of feeling included in their communities. Within this theme, participants identified barriers such as societal stigma and lack of training among potential employers and other community members. Participants also focused on increasing autistic adults’ involvement in the community through employment, as well as through activities such as volunteering, which could highlight the ways in which autistic adults have the potential to contribute to their communities more broadly.
Theme 4: service delivery systems emerged as a theme and highlighted that many challenges trickle down from regulations set in place by the government, including schools, funding issues, insurance coverage, and system silos. Many of these factors differentially impact Qatari citizens and foreign national residents.

Identified themes and associated codes.
Discussion
The goal of this project was to collect stakeholder input from parents and providers to inform key decisions regarding services for autistic adults in Qatar, driven by an interest in responding to the need for respite care for autistic adults. Stakeholder information was gathered through four focus groups, which included parents and providers for autistic individuals in Qatar, as well as through brief parent surveys. Parents and providers both endorsed respite care services for autistic adults as a clear area of need in Qatar and emphasized the importance of creating high-quality, comprehensive services that promote meaningful inclusion and quality of life for autistic adults in Qatar. Analysis of stakeholder input identified the following themes as critical to understanding the needs of autistic adults in Qatar: trust and reliability, quality of life, meaningful inclusion, and service delivery systems. These themes align closely with priorities identified in studies of respite care and adult needs in Western nations, which have highlighted the challenges in navigating the transition to adulthood and associated systems of care, the important of trust in adult respite providers, and the needs of autistic adults for wholistic care and meaningful engagement in their communities (Farley et al., 2009; Jeon et al., 2005; Płatos & Pisula, 2019; Shattuck et al., 2013).
Along with the advancements that have been made in supporting autistic adults in Qatar, we provide the following recommendations based on the findings from this project. Respite care programs in Qatar should clearly and directly address improving quality of life for autistic adults and their families. It will be important to engage families in identifying activities and goals that enable meaningful inclusion for each young adult, using a strength-based approach. Stakeholders repeatedly emphasized the wide diversity of skills and interests among autistic individuals and the corresponding need for programs to provide individualized supports and activities. However, creating these programs requires accessible service delivery systems that employ trustworthy and reliable providers. Doing so will ensure that the adults will spend their time in a meaningful way, adapted to their unique goals. Suggestions on ways to do so include as follows:
Provide opportunities for young adults to learn valuable adaptive living skills.
Take a strength-based approach to all learning.
Family members should be involved in designing programming and providing specific input about their loved one’s unique needs.
Ensure that all providers are adequately trained to work with adults with disabilities and partner actively with families and autistic adults on priorities.
Actively address barriers to accessibility in designing a respite care program.
A primary goal of respite care programs is often to provide stress relief to parents, which was also the primary goal endorsed by participating parents. Along with indirectly supporting parents by appropriately programming for their adult children, we recommend considering ways to directly improve parents’ quality of life:
Address psychosocial stressors faced by parents.
Consider providing in-home support for parents.
Stakeholders discussed how employment may be an achievable and important goal for many autistic adults. Furthermore, the government mandate to employ people with disabilities (Government of Qatar, 2020) means that job opportunities for autistic adults should be available. We recommend addressing barriers to employment, both by working with adults with autism and with employers:
Create training programs for employers to learn how to support individuals with autism in the workplace.
Vocational training programs are required to support individuals with autism in preparing for employment.
A number of the challenges identified as part of this study cannot directly be addressed through the development of the respite care program, but rather lie in the hands of national service delivery systems. The Qatar team and local individuals who convened for this project are well-situated to begin advocating for and facilitating such change. Recommendations on how to do so include as follows:
Map out the autism-related stakeholders in Qatar.
Convene stakeholders regularly to discuss and address barriers to supporting autistic adults.
Finally, Qatar faces a unique challenge in that there is a shortage of nationally trained professionals and the vast majority of its population and workforce are composed of foreign nationals, many of whom do not intend to stay in the country long term (Sheikh et al., 2019). Thus, it is critical that Qatari citizens and long-term foreign residents lead the development of organizations that can set priorities and work actively with the foreign workers who cycle in and out of the country. This should occur alongside current government initiatives focused on increasing training and capacity among Qatari citizens in order to serve in these professional roles (Qatar Ministry of Development Planning and Statistics, 2018).
Limitations
A number of limitations should be considered in understanding these data. The team recognized the potential for implicit cultural biases to impact the collection and interpretation of the data from the inception of this project. In order to enhance the trustworthiness of the data, the US team partnered with the local research team in Qatar on each stage of the research project. Furthermore, the US researchers reflected on their positionality in interpreting the data. In the qualitative analysis process, the Qatar team provided feedback on the coding structure. Implicit cultural biases may have also emerged on behalf of the participants; responses may have been altered due to their comfort level with the international researchers.
Given that the primary language of the US research team and the standard business language in Qatar was English, the study was primarily conducted in English. Parents had the option to complete the focus group in Arabic, and all participants had the option to complete questionnaires in Arabic. Language differences may have impacted our interpretation of the data. Another limitation of the study is the potential for sample bias. The research team leveraged established stakeholder partnerships for recruitment, such that participants were all active and committed stakeholders, considered leaders within the parent and/or provider communities, lending strength to the perspectives they expressed. However, parents who were unable to participate due to any number of barriers (e.g. stigma, lack of childcare, socioeconomic limitations, work commitments, and distance from home), and providers unconnected to the systems of care provided through the Qatar team’s organization, and/or those who were less comfortable in English, may not have had their views fully represented. It is notable, however, that parents repeatedly discussed the challenges of families who were not able to participate in the focus groups. Future studies should explicitly focus on obtaining a needs assessment from families who could not participate in this study due to the aforementioned barriers. Finally, the project was undertaken with a primary goal of understanding the needs of autistic adults as they relate to respite care, based on priorities previously identified by the stakeholder community and local researchers. Although the entire research team worked to broaden the scope of inquiry and ensure that priorities outside of respite care were invited and heard, as reflected in the data, the foundation of the project centered on respite care needs, and this necessarily influenced the questions asked and interpretation of the data.
Conclusion
There is enormous potential to develop effective service delivery systems to support autistic adults and their families in Qatar, due to a dedicated community of specialists, cutting edge research expertise, and support from the national government, as highlighted in the National Autism Plan. In particular, the desire for cross-collaboration between service providers and families (both Qataris and foreign nationals) foreshadows tremendous potential for developing meaningful and high-quality service delivery systems. A direct first step in supporting autistic adults, previously identified by local stakeholders and supported by the results of this study, is to develop a respite care program that can directly improve quality of life for both parents and young adults. Such programming, as well as engaging appropriate stakeholders, can lead to indirectly supporting autistic adults by ensuring employment opportunities and facilitating cross-system communications. Together, these can lead to a bright future for adults with autism in Qatar.
Footnotes
Acknowledgements
The authors thank Her Highness Sheikha Moza bint Nasser, Chairperson of Qatar Foundation, and the leadership of the Qatar Foundation. The authors also acknowledge members of the WISH and Qatar foundation for the immense amount of support provided throughout this project: Sultana Afdhal, Walid Qoronfleh, Neil Moors, Sherri Miller, Faisal Al-Hitmi, and Mahmoud El-Achi. The authors also share our gratitude with the stakeholders who work tirelessly to support those with autism in Qatar including those who participated in focus groups and workshops included, among others, individuals from the following organizations: Hamad Medical Corporation, Child Development Center, Al Shafallah Center for Persons with Disabilities, Qatar Biomedical Research Institute (QBRI), Al Maha Centre for Children and Young Adults, Renad Academy, AWSAJ Academy, Qatar Career Development Center, the Assistive Technology Center of Qatar (MADA), Qatari Autism Society, and Sidra Hospital. Finally, the authors thank the following individuals from Children’s National Hospital for their help and support throughout the project: Lauren Kenworthy, Alyssa Ware, and Shadi Sadeghi.
Authors’ note
As individuals on the autism spectrum demonstrate a range of self-identification, we use both person-first and identity-first language in this manuscript (Kenny et al., 2016).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.