
Abstract
Children with autism spectrum disorder are at increased risk for obesity compared to typically developing children. Many obesity intervention programs exclude children with autism spectrum disorder. There is little research on developmentally inclusive approaches to pediatric weight management. We examined the outcomes of children and families with autism spectrum disorder in an inclusive, comprehensive behavioral family-based lifestyle intervention. A secondary analysis of a randomized controlled trial on families enrolled in a comprehensive behavioral family-based lifestyle intervention was conducted. Analyses included chi-square or Fisher’s exact tests to examine family and child differences in program completion rates and multivariate regression analysis using generalized estimating equation to further examine differences in weight outcomes between children with autism spectrum disorder versus no autism spectrum disorder accounting for other covariates. There were 158 families; 15 families had children with autism spectrum disorder. There were no significant differences in demographics, program completion, or weight outcomes between the two groups. Children who completed the intervention had a significant decrease in body mass index Z-scores, but no change in their percentage of the 95th percentiles. Families of children with autism spectrum disorder participated in a comprehensive behavioral family-based lifestyle intervention alongside children without autism spectrum disorder with similar outcomes. Comprehensive behavioral family-based lifestyle intervention can meet the weight management needs of children with autism spectrum disorder using an inclusive approach, expanding access to needed obesity interventions.
Lay abstract
Children diagnosed with autism are likely to be more overweight than children who do not have autism. There are many group programs that help children to be more physically active and improve their eating habits to achieve healthy weight, but most of these programs do not allow children with autism to participate. We studied a program that was specially adapted so children with autism could participate together with peers who do not have autism. The program lasted 8 weeks and was offered in the evening at a large healthcare center in a big city. The children participated with a parent or another adult who takes care of them. We analyzed data that were part of a previous project where we studied how physical activity trackers called Fitbit help overweight children to change their eating and exercise habits so they can achieve healthier weight. Out of 158 families in the study, 15 families had a child or children with autism. We measured changes in the weight of children with and without autism and compared how many of the children completed the program. Children who had autism had similar results in achieving healthy weight and finishing the program compared to their peers without autism. Our study found that when a group weight management program is slightly changed to meet the needs of children with autism, they can successfully participate and benefit similarly to their peers who do not have autism.
Registration
This trial was registered with ClinicalTrials.gov (NCT03215641).
Introduction
Worldwide, pediatric overweight and obesity affect more than 38 million children under 5 years of age and over 340 million children and youth ages 5 to 19 years (World Health Organization, 2020). Childhood obesity remains the most significant risk factors for developing adult obesity and its comorbidities (Singh et al., 2010). Overweight and obesity negatively impact children’s quality of life and their mental health, which may be also hindered by lack of success in weight management interventions (Buttitta et al., 2014; Kelly et al., 2016).
In the United States, population-level studies report that 19.4% of youth with autism spectrum disorder (ASD) are overweight and 23.05% are obese compared to 14.9% overweight and 15.91% obese among typically developing youth (Healy et al., 2019; McCoy et al., 2016; McCoy & Morgan, 2019). Adolescents with ASD have a higher incidence of chronic health conditions linked to overweight and obesity such as high blood pressure and diabetes and are two to three times more likely to be obese compared to their typically developing peers (Cermak et al., 2010).
Children and adolescents with ASD are especially vulnerable to overweight and obesity because of the following challenges:
Restricted food preferences and other dietary challenges (Cermak et al., 2010; J. Marshall et al., 2014; Minihan et al., 2007; Schreck et al., 2004);
Side-effects of some psychotropic medications (Barnard et al., 2002; Esbensen et al., 2009);
Lower caloric needs due to low muscle tone and lower levels of physical activity (Cermak et al., 2010; J. Marshall et al., 2015; McCoy et al., 2016; McCoy & Morgan, 2019);
Challenges with postural control, balance, visual motor, and gross motor coordination (Green et al., 2009; Reynolds et al., 2011);
Sensory processing challenges including significant differences in proprioceptive, vestibular, tactile, and visual information processing (Ben-Sasson et al., 2009; Tomchek & Dunn, 2007);
Preference for screen time and sedentary activities (Reynolds et al., 2011; Srinivasan et al., 2014).
In addition to these challenges, diminished opportunities for participating in both physical and social activities can contribute to overweight and obesity among children and youth with ASD (Hinckson et al., 2013; Pan, 2008). For example, children and youth with ASD are less likely than typically developing peers to play outside with other children in their neighborhood and often lack access to organized sports at school and in the community (Raghavendra et al., 2011). Ethnographic research on children with ASD in fully inclusive classrooms has shown that during school recess, they may experience rejection and ridicule if their typically developing peers are insufficiently informed about ASD (Andron, 2001; Kramsch, 2002; Solomon, 2008).
Internationally, numerous public health and policy guidelines and recommendations have been published to address the increase in pediatric overweight and obesity among children with and without developmental disabilities in the United Kingdom Australia (Haby et al., 2006), China (Xiong et al., 2009), Kuwait (Elkum et al., 2016), Oman (Al-Kindi et al., 2016), Turkey (Bicer & Alsaffar, 2015), Iran (Hajian-Tilaki & Heidari, 2013), and other countries (Cole et al., 2000). In the United States, multi-level programmatic recommendations to address pediatric overweight and obesity have been published by the Obama’s administration’s ‘Let’s Move!” campaign (Executive Office of the Force WH, 2010), Institute of Medicine (Kumanyika et al., 2010), the National Institute of Health Strategic Plan for Obesity Research (Spiegel & Alving, 2005), Healthy People 2020 Initiative (Koh et al., 2011); (“Healthy People 2030,” n.d.; Koh et al., 2011), and the Healthy Weight Research Network (Curtin et al., 2017). Achieving these top-down recommendations to any degree requires significant and sustained federal, state, and local investments in infrastructure for multi-site networks of research, program development, and program evaluation (Curtin et al., 2017). If available, such resources would have had the capacity to transform population-level recommendations into empirically based strategies directly applicable to the everyday lives of children, families, and communities (Green, 2006).
The Institute of Medicine recommends that, given the shortage of promising approaches and paucity of empirical evidence for effectiveness of existing weight management interventions, the criteria for what constitutes evidence of effectiveness in overweight and obesity prevention and management should reflect what is possible rather than what is desirable (Kumanyika et al., 2010). This would allow for a broader range of approaches to be considered by the stakeholders in the problem.
In 2015, we began a funded randomized control trial ((National Institute of Diabetes and Digestive and Kidney Diseases supported Academic Pediatric Association Research in Academic Pediatrics Initiative on Diversity program, NIH R25DK096944)) to evaluate participation and weight outcomes in an inclusive group weight management program BodyWorks (BW). The program is a moderate intensity, manualized Comprehensive Behavioral Family-Based Lifestyle Intervention (CBFLI) offered at our institution’s pediatric primary care clinic, a federally qualified health center (FQHC; Espinoza et al., 2017; Office of Women’s Health, 2009). During the analysis phase of the original study, we found a high rate of participation of families with children with ASD. In this article, we describe the findings of a secondary analysis of these data focused on evaluating the participation and outcomes of children with ASD. Our hypothesis was that families with children with ASD participated at the same rate as families of children without ASD and that there would be no differences in weight outcomes.
Methods
Design
This was a secondary data analysis of a prospective randomized controlled trial (RCT) to evaluate the impact of physical activity tracker usage on families enrolled in a CBFLI. This trial was registered with ClinicalTrials.gov: NCT03215641.
Participants and setting
We enrolled families that met the following eligibility criteria: they had at least one child ages 7 to 18 years with a BMI ⩾85th percentile for age and gender, consistent with the definition of overweight and obesity in children (CDC & NCHS, 2000), had at least one parent or caretaker able to attend the sessions with the child, and had not previously attended a BW program. Families who repeated the program were only included in the study based on the first time they participated. There were no exclusion criteria on the basis of developmental disability. In many families, more than one child participated in BW. Families were recruited to participate in the study during their first session of BW. There were no families that declined participation in the study. The program was conducted at an FQHC within a General Pediatrics clinic at a large, urban, university-affiliated healthcare center between August 2015 and October 2017. The hospital and FQHC Institutional Review Boards approved this study’s protocol, IRB# (IRB number anonymized). All participants provided written informed consent or assent, as appropriate for age.
BW intervention
Recruitment
BW was offered as a free program to all children who received their primary care at the FQHC clinic. Ninety-three percent of the 27,000 patients in the FQHC are Medicaid recipients, and 76% identify as Hispanic/Latino. Clinic pediatricians referred any child with a BMI ⩾ 85th percentile for age and gender by placing a referral in the electronic health record. A BW program coordinator then called the family to provide an overview of the program and its schedule, and inquire about language preferences as the program was offered in Spanish and English. The program coordinator gathered information about the parent’s concerns related to their child’s health, weight status, or eating and physical activity habits. The program coordinator also confirmed the family’s intention to participate and how many family members planned to attend.
Parents were asked if their children had any social, behavioral, or physical needs and were informed about ways in which the team might support the child’s participation in activities. Families were asked to identify support strategies successful in other environments. If a child had access to resources such as additional supportive family members or behavioral interventionist who could provide one-on-one support, the families were encouraged to invite these individuals to attend the program as well. The team then determined whether additional accommodations were needed to increase the child’s access to the program. At least one adult and one child had to participate in the program, and siblings and other members of the immediate household were also invited to join the program at no cost.
BW program
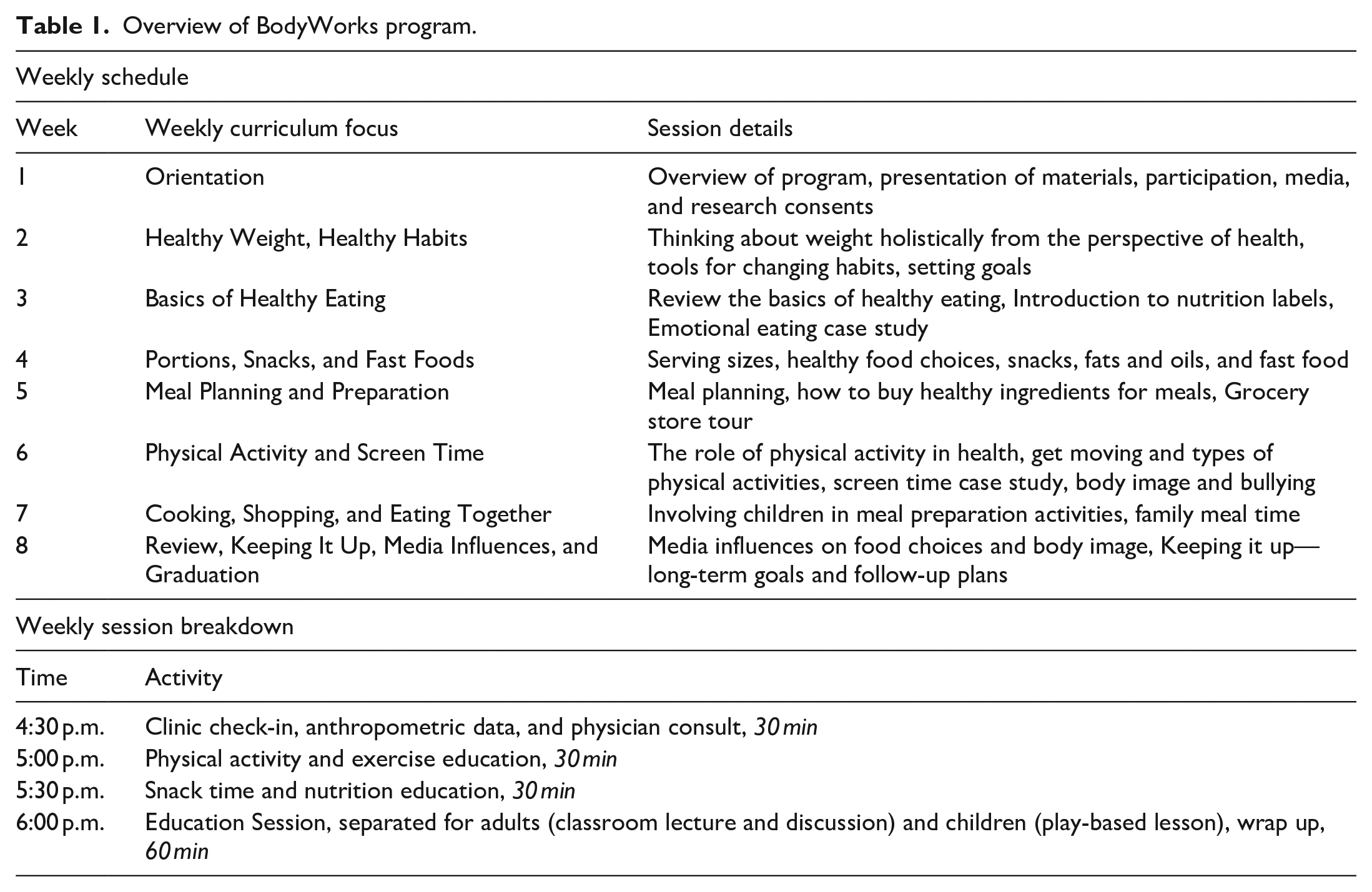
BW has been described in detail elsewhere (Department of Health and Human Services Office on Women’s Health, 2009, 2013; Borden et al., 2012). The program consisted of 8 weekly sessions, including one general program orientation (Table 1). Each session involved a brief visit with a pediatrician, ~30 min of group physical activity such as yoga or Zumba, a snack break that incorporated health food alternatives, and a didactic session that lasted approximately 1 h. Physical activity and snack time occurred with parents and children participating together. For the didactic part, parents and children had different sessions, with the child group using play-based and/or age-appropriate learning techniques to convey the same information covered by the parent group. Topics ranged from cooking, shopping, eating together, meal planning and preparation, and media influences on eating behavior. There was also a grocery store tour which built upon didactic sessions focused on understanding nutrition labels, food advertising, creating and adhering to shopping lists, reducing impulse buying and how products are placed to enhance weekly store specials. At the store, shopping for produce and purchasing groceries was a child-directed task with one-on-one support from child group facilitator. Parents were encouraged not to make any purchases at the grocery store during this visit.
Overview of BodyWorks program.
BW program adaptations
Because the BW program was originally developed for parents (Department of Health and Human Services Office on Women’s Health, 2009, 2013), we adapted the content of the program to be understandable and engaging for children, including children with ASD. Adaptations included the development of a supportive social environment, predictable structure and routines, encouraging self-directed participation, modeling physical activity and food exploration, providing visuals to encourage practice at home, and training the child’s behavioral interventionist to provide one-to-one support. Several BW facilitators who were occupational therapy doctoral residents were present during each session to provide additional support to any child who needed help to participate. Some parents commented informally that these adaptations turned out to be especially helpful for their children with ASD.
Predictable structure and routines
The groups were structured to support behavior change through the development of a new routine (i.e. attending groups) and new health behavior habits. This routine was emphasized with written agendas, visual schedules, and sequencing of activities in a predictable order. Children with ASD learned what to expect in groups and parents benefited from being able to prepare and coach their children before and during groups.
Sensory environment
During each session, the sensory environment was considered, including light, ambient and outdoor sounds, placement of tables and chairs, and body space. For children who required additional support for behavioral or attention needs, the team strived to increase the adult to child ratio and provided one-on-one support if needed. The inclusive child groups also included siblings, so that the groups were diverse in ages, personalities, intellectual and social functioning, body type, and strengths.
Food sensitivity and limited diet
Group facilitators introduced families of children with ASD and children without ASD to new foods that were nutrient dense and easy to prepare at home. The goal was to engage all participants in positive experiences with nutritious foods having different textures, tastes and smells. While exploring the sensory aspects of foods, children also reviewed nutrition facts, learned meal preparation techniques, and practiced combining different food groups. The intent of this instruction was to generalize this knowledge to meals prepared at home. Providing positive reinforcement and opportunities for group modeling were powerful tools to promote food acceptance. All children received positive reinforcement for the smallest attempt to engage with new foods. Parents were introduced to try new ways to engage with and support children in meal preparation activities, and to get their children involved and interested in making better choices at home. Anecdotally, some parents reported that the content on food sensitivity and limited diets was especially helpful for children with ASD, given additional challenges with food selectivity.
Physical activity promotion
As children with ASD often experience motor challenges that make physical activity less enjoyable, group facilitators adapted physical activities to emphasize play, enjoyment, and body awareness. By emphasizing the social aspects of physical activity through activities like yoga, Zumba, and WII Just Dance, group leaders modeled and encouraged peer social engagement. To address the sensory challenges, physical activity sequences were gradually increased in intensity. Families were encouraged to identify other activities such as walking in a park, or making trips to the zoo. Families were provided with lists of low-cost community resources such as Special Olympics and local YMCAs. Providing a predictable structure and gradual physical challenges helped all children engage more actively, even during activities that required increased levels of motor control and motor planning.
Supportive coaching
In addition to the physical challenges of movement and motor coordination, engagement in physical activities has social, emotional, and cognitive aspects. Supportive engagement in physical activities was carried out through modeling, feedback, encouragement, and coaching for all participants. Focus was made on listening to bodies, taking rest breaks, social encouragement, and experiencing success as a team with flexibility for setting a personal pace. Children, including those without ASD, and parents who experienced social anxiety and physical limitations, benefited from modified physical activities.
In summary, the delivery of the program content was the same for all children; however, the organization and the social environment of the program made it accessible and enjoyable for children with ASD. In addition, children with ASD benefited from having BW support personnel (i.e. several occupational therapy doctoral residents) who were trained to facilitate their participation in the meetings.
Outcomes
The primary study outcomes were changes in BMI Z-scores and percentage of the 95th percentile among children with and without ASD, adjusting for sociodemographic and program characteristics. The secondary study outcome was completion rates among children with ASD compared to those without ASD.
Weight outcomes
Child body mass index (BMI) was calculated from height and weight, which were obtained weekly to monitor progress. Only the baseline and post-intervention BMIs were used. BMI percentiles for age and gender or BMI-for-age percentiles were calculated based on the Centers for Disease Control and Prevention growth charts (CDC Growth Charts, 2000). BMI percentiles were converted into Z-scores and percentage of the 95th percentile (Gulati et al., 2012). Using BMI percentiles, overweight was defined as ⩾85th to <95th percentile, obesity was defined as ⩾95th percentile. We examined severe obesity, defined as ⩾120% of the 95th percentile as a descriptive statistic only (Wickham & DeBoer, 2015).
Program completion
Program completion was defined as a family attending the orientation session and at least 4 of 7 intervention sessions, which was based on data from meta-analyses of randomized controlled obesity intervention trials among children and adolescents that have included ⩾4 weeks as the basic threshold used in obesity interventions (Kelley et al., 2015; Knowlden et al., 2015).
Establishing a diagnosis of ASD
The electronic medical record for all participants was manually reviewed to identify relevant ICD-9/10 codes for ASD (299.0 and F84.0, respectively). The presence of any of these diagnostic codes two or more times within 3 years of the child’s participation in BW was used to categorize that child as having ASD. History of diagnosis of ASD was verbally confirmed with participating parents. No patient had Pervasive Developmental Disorder or Asperger’s Disorder as a diagnosis in their medical record. All other children were analyzed as the non-ASD group.
Sociodemographics
Parents completed one demographic survey per family. Variables measured included ethnicity, language preference, English proficiency, household income, and household size. Limited English proficiency (LEP) was defined as answering anything other than “very well” to the US Census question on English language proficiency (Karliner et al., 2008). Household income and size were used to calculate Percent of the Federal Poverty Level (FPL) following the 2016 FPL guidelines for California.
Statistical analysis
Descriptive statistics were used to summarize and describe the distribution of demographic variables. Continuous variables were summarized as means and standard deviations for normally distributed variables, whereas medians and inter-quartile ranges for non-normally distributed variables. We examined family and child demographic differences between the ASD families and all others by conducting Chi-square and Fisher exact tests, and differences in age and weight outcomes by conducting two-sample t-tests. Repeated measures analysis of variance (ANOVA) was used to evaluate the change in BMI Z-scores and BMI percentage of the 95th percentile from baseline to post-intervention between children with and without ASD who completed the program.
Then, multivariate regression analysis using generalized estimating equation (GEE) was conducted to further examine the changes in BMI Z-scores and percentage of the 95th percentile between children with and without ASD in taking into account sociodemographic and program characteristics. The non-additive effects of children with ASD compared to children without ASD was also examined (e.g. whether the change from baseline to post-intervention differed between children with and without ASD) by including the interaction terms. Covariates included visit, age, gender, LEP, and program completion. The arm randomization of the original parent study was also included as a covariate in order to account for possible interference. The significance level was set at 5% with two-sided tests. All statistical computations were done in SAS 9.4 (SAS Institute Inc, Cary, NC) and Stata/SE 15.1 (College Station, TX).
Community involvement
Patients were not involved in the design, conduct, or analysis of this research. Patients did contribute significantly to the implementation of the BodyWorks program. Each family with a child with ASD was contacted prior to their participation in order to understand their specific needs. Program leads checked in with families after each session to understand if they were receiving the level of support needed. At the end of each cycle, feedback was solicited form all participants on how to improve the program.
Results
There were 174 families that participated in BW during the study period (Figure 1). There were 11 families excluded from the analysis because their only participating child was younger than 7 years of age. Five families were excluded because it was their second or third time going through the BW program. The remaining 158 families with a total of 225 children were included in this analysis. There were 20 children with ASD from the 15 different families who participated in BW (Figure 1). Three families had 2 children with ASD, and one family had 3 children with ASD. One child with ASD from a family of 3 children with ASD was excluded from the analysis because he was younger than 7 years of age. Cycle enrollment ranged from 14 to 23 families. Families with children with ASD participated in 6 of the 10 cycles in the two-year study period. The number of families with a child with ASD in each cycle ranged from 0 to 5. An average of 3 families with children with ASD participated in each of the intervention cycles. Completion rates across cycles were similar regardless of the presence of families with ASD.
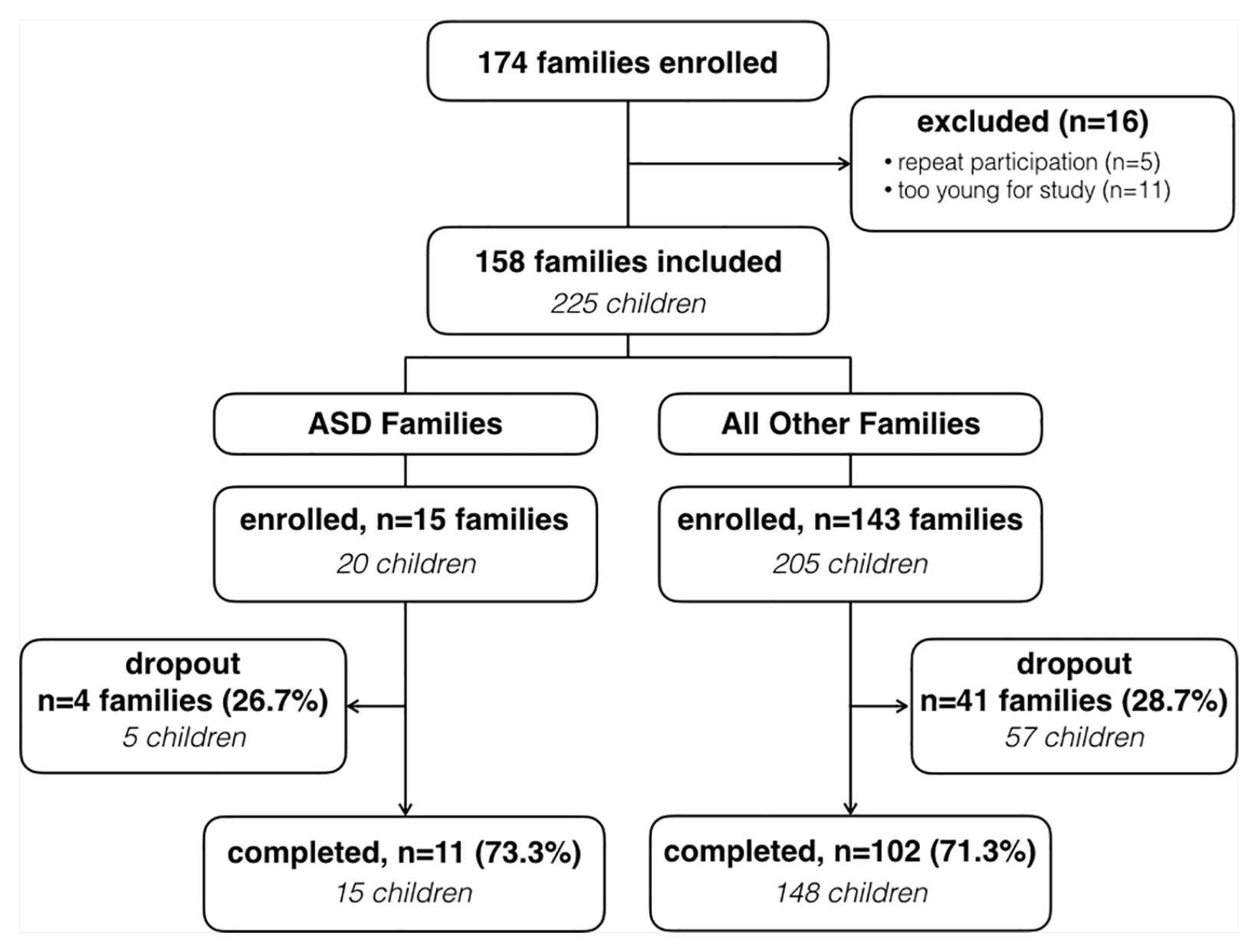
Study CONSORT diagram.
Sociodemographics and anthropometrics: family and child level
Family level
The demographics of BW participants were reflective of the clinic from which they were recruited and the local community (Table 2). The majority of families identified as Latino, had limited English proficiency, and had household incomes below 200% of the FPL. There were no significant differences in demographics between ASD families and families without ASD (Table 2).
Sociodemographic characteristics of families and children with and without ASD.
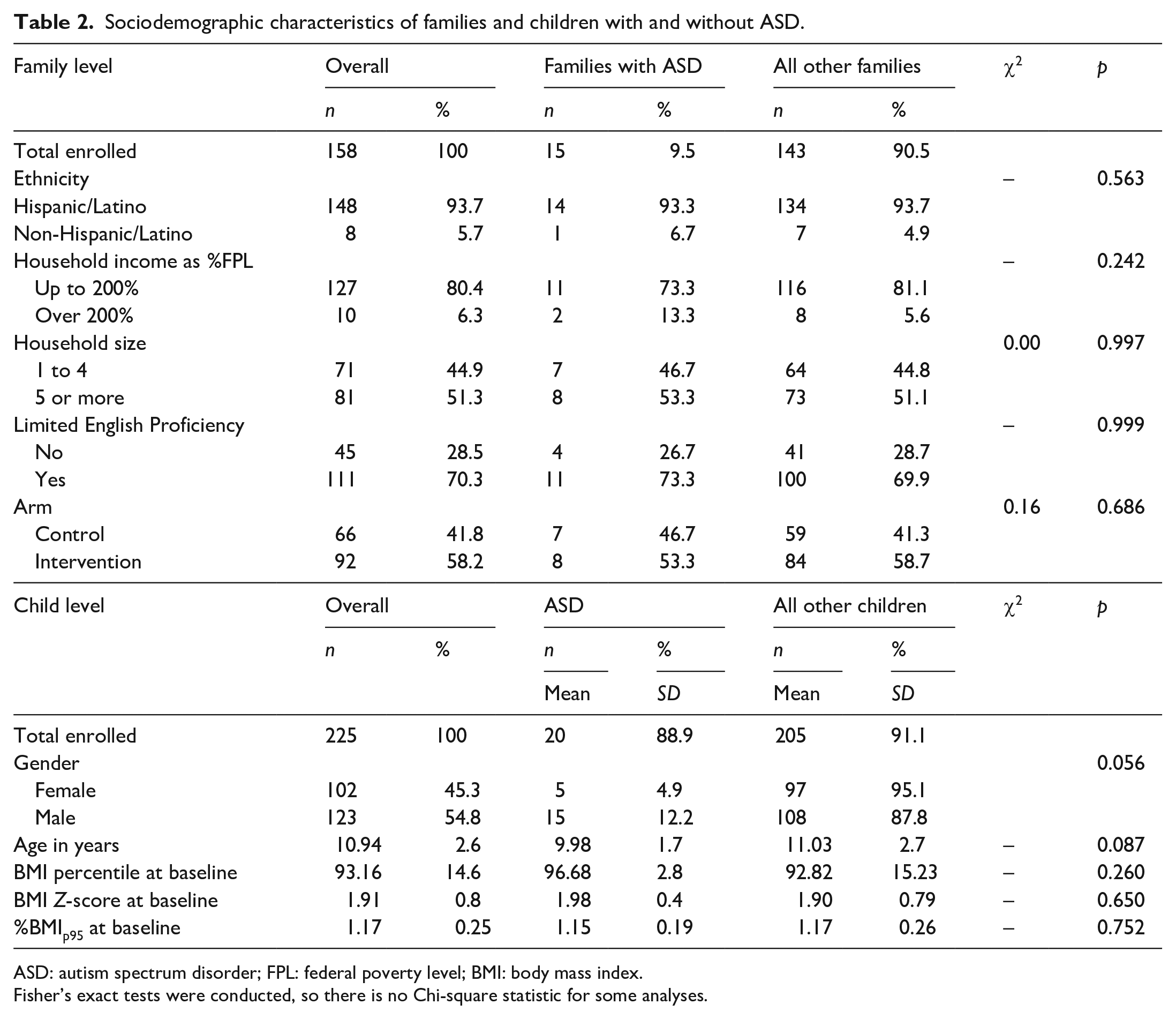
ASD: autism spectrum disorder; FPL: federal poverty level; BMI: body mass index.
Fisher’s exact tests were conducted, so there is no Chi-square statistic for some analyses.
Child level
There were no significant differences in demographics between children with ASD and children without ASD. There were no differences in weight distributions at baseline between children with and without ASD.
Program completion
There were 11 (73.3%) families having children with ASD that completed the program and 102 families having children without ASD (71.3%) that completed the program (Table 3). There were no significant differences in program completion among families with children with ASD and families with children without ASD, p = 0.999. There were 15 children with ASD who completed the program (75%) and 148 children without
Program completion rates among children with and without ASD.
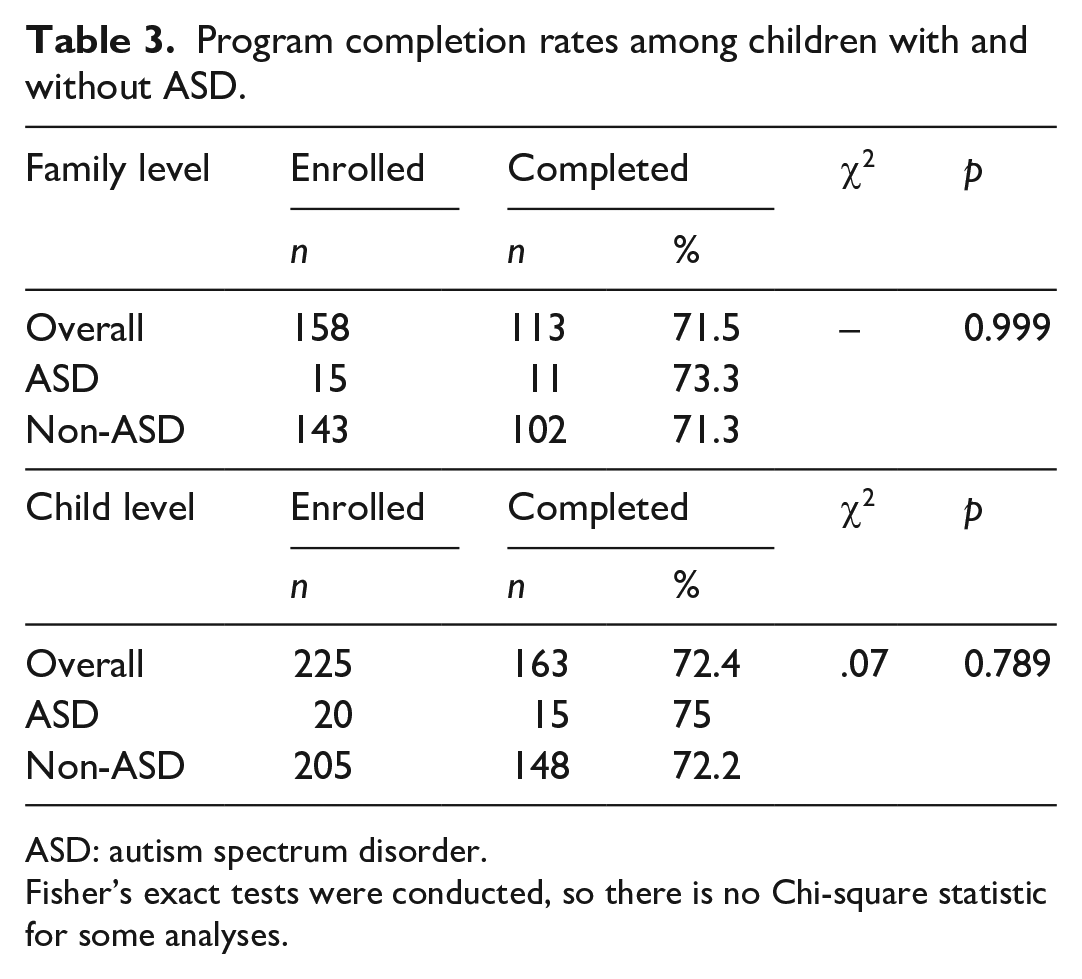
ASD: autism spectrum disorder.
Fisher’s exact tests were conducted, so there is no Chi-square statistic for some analyses.
Weight outcomes
Unadjusted weight outcomes
Table 4 provides more details about anthropometrics and obesity classification of children with ASD who participated in the program from baseline to post-intervention. The weight outcomes are presented in Table 5 among all children, and among children who completed the intervention. Among all children, there were no differences in the change of BMI Z-scores between children with and without ASD (M = −0.04, SD = 0.10) versus (M = 0.02, SD = 0.11), p = 0.557. Similarly, there were no differences in the change of the percentage of the 95th percentile between children with and without ASD (M = 0.01, SD = 0.03) versus (M = 0.01, SD = 0.03), p = 0.768. Among children who completed the intervention, there were no differences in the change in BMI Z-scores between children with and without ASD (M = −0.04, SD = 0.10) versus (M = −0.03, SD = 0.12), p = 0.774. There were also no differences in the change in percentage of the 95th percentile between children with and without ASD (M = −0.01, SD = 0.03) versus (M = −0.01, SD = 0.03), p = 0.947.
Individual anthropometrics for all participating children with ASD.

ASD: autism spectrum disorder; BMI: body mass index.
%BMIp95 = Percent BMI of the 95th percentile; BMI-for-age ⩾ 85th to < 95th percentile = overweight; BMI-for-age ⩾ 95th percentile = obese; BMI-for-age ⩾ 120% of the 95th percentile = severe obesity.
Weight-related outcomes among all children and children who completed the intervention.
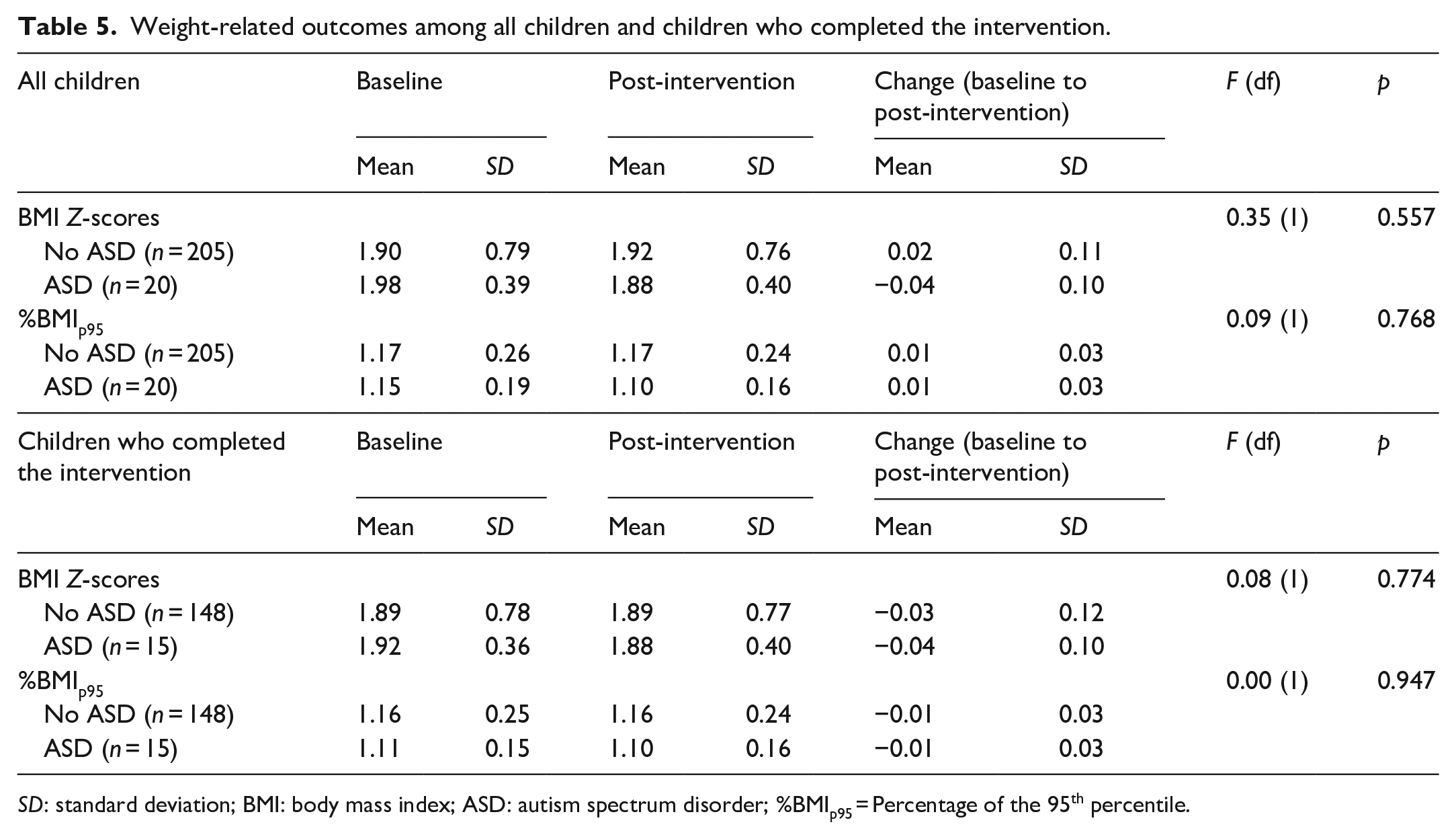
SD: standard deviation; BMI: body mass index; ASD: autism spectrum disorder; %BMIp95 = Percentage of the 95th percentile.
Adjusted weight outcomes
The adjusted multivariate analysis in Table 6 indicated that there were no statistically significant differences in the change in BMI Z-scores between children with and without ASD after adjusting for all sociodemographic and program characteristics (β = −0.003, p = 0.980). However, there were significant differences in the change in BMI Z-scores from baseline to post-intervention (β = −0.02, p = 0.018) after accounting for covariates. Although there was a decrease in BMI Z-scores for children who completed the program compared to those who did not complete the program, it was not statistically significant (β = −0.06, p = 0.611). For the interaction of ASD × number of visits, there were no significant differences in BMI Z-scores between children with and without ASD from baseline to post-intervention (β = −0.004, p = 0.865).
Multivariate regression model on BMI Z-Scores and Percent BMI of the 95th Percentile.
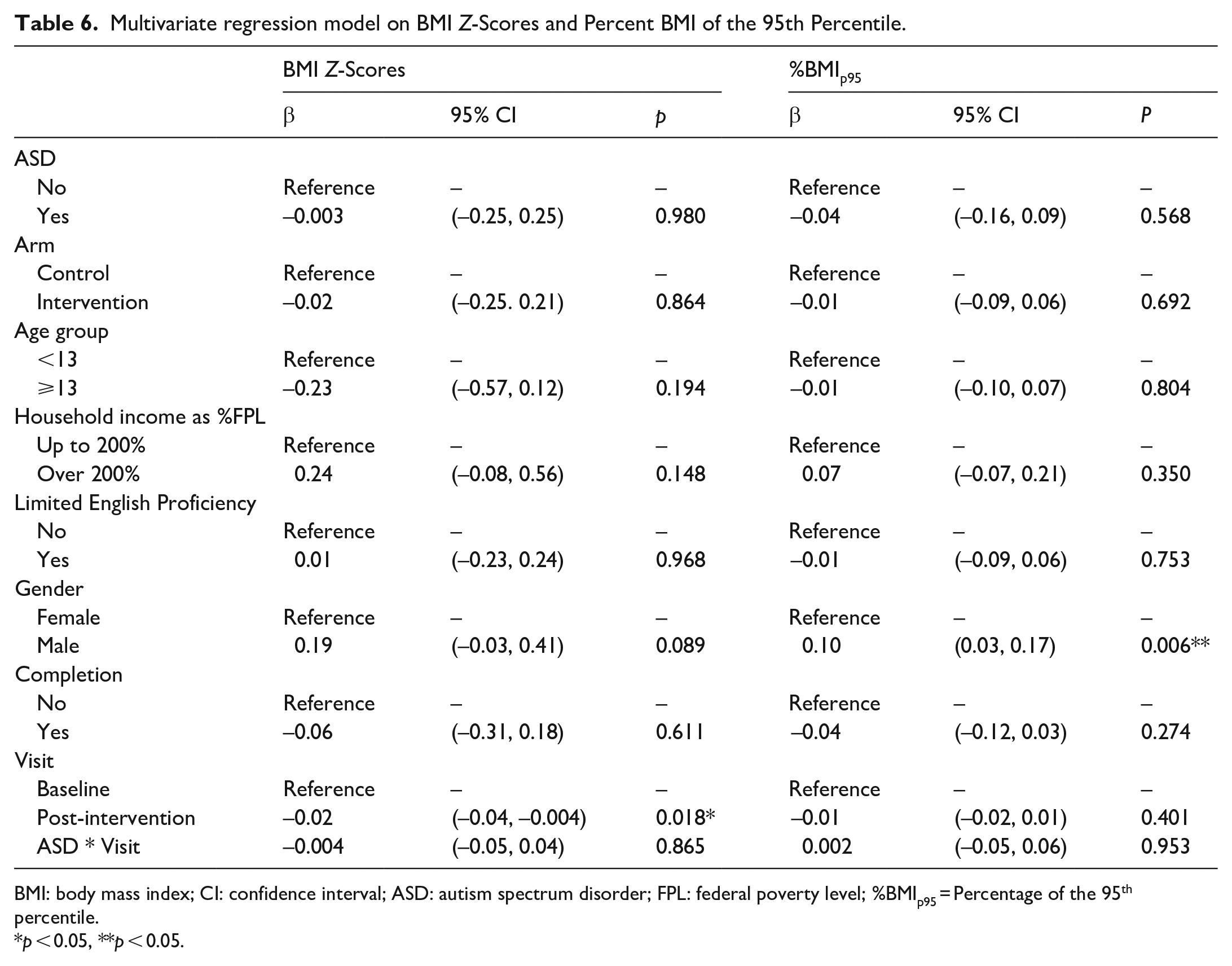
BMI: body mass index; CI: confidence interval; ASD: autism spectrum disorder; FPL: federal poverty level; %BMIp95 = Percentage of the 95th percentile.
p < 0.05, **p < 0.05.
The adjusted multivariate analysis in Table 6 demonstrated that there were no statistically significant differences in the percentage of the 95th percentile change between children with and without ASD after adjusting for sociodemographics and program characteristics (β = −0.04, p = 0.568). There were also no differences in the percentage of the 95th percentile change from baseline to post-intervention (β = −0.01, p = 0.401). However, there was a significant difference in percentage of the 95th percentile change between males and females (β = 0.10, p = 0.006). For the interaction ASD × number of visits, there were no significant differences in percentage of the 95th percentile change between children with and without ASD from baseline to post-intervention (β = 0.002, p = 0.953).
Discussion
To our knowledge, this is the first study to evaluate the weight outcomes and completion rates of children with ASD participating alongside children without ASD in an inclusive CBFLI program. The findings of this study support our hypothesis, demonstrating that regardless of ASD diagnosis, the families of children with and without ASD completed the program at similar rates, and the children themselves had similar weight outcomes. The predominantly low-income, Hispanic/Latino, Spanish-speaking families that participated in BodyWorks were representative of the community served by our FQHC in Los Angeles. Socioeconomic status is an important factor in pediatric obesity. Low-income children, and children from racial and ethnic minority backgrounds are at the highest risk of obesity and related health problems (Haidet et al., 2010; Hales et al., 2017; Neckerman et al., 2010).
The inclusive BW intervention demonstrated positive results, as all children who completed the intervention had slightly decreased BMI Z-scores or maintained their percentage of the 95th percentiles. In addition, there were no differences in weight outcomes among children with ASD compared to those without ASD, indicating that the intervention did not benefit one group more than the other. The findings highlight the effectiveness of the BW program in a low resource setting, the resilience of the families who participated, and the importance of program completion.
Benefits of participating in an inclusive program may be present for all participants. Increased opportunities for socialization in structured settings among children with ASD has been beneficial, as well as being exposed to positive behavior modeling by their typically developing peers (Ausderau et al., 2019; Pan et al., 2011). Children without ASD receive the benefit of additional staff and volunteers trained to support all children, regardless of disability, on topics such as picky eating, introducing new foods that are nutrient dense, and increasing fresh fruit and vegetable intake.
Families with children with ASD represented 9.5% of all families in the study, which is higher than the nationally reported 1.9% (1 in 54) prevalence (Maenner et al., 2020). This relatively high percentage of children with ASD in our sample is due to two factors. First, our primary care clinic is associated with an academic medical center that serves a significant percentage of families who have children with medical, developmental and behavioral complexity, many of whom have been diagnosed with ASD. Second, because BW is promoted at our institution as an inclusive program, primary care providers in the clinic routinely refer patients with ASD to BW.
Our results should be interpreted with the following literature in mind: first, children with ASD are at increased risk of overweight and obesity compared to their typically developing peers, with McCoy et al. (2016) reporting by 27% and 72%, respectively, from the 2011 to 2012 National Survey of Children’s Health, and Healy reporting similar findings from 2016 National Survey of Children’s Health (Healy et al., 2019). This increased risk for obesity is multifactorial, and multiple physical, behavioral, and metabolic mechanisms have been proposed (Esbensen et al., 2009; J. Marshall et al., 2015; Pan et al., 2011). The co-incident rise in pediatric obesity and ASD over the last few decades has created an acute need for obesity intervention appropriate for individuals with ASD.
Second, children with ASD are often excluded from obesity interventions. The 2007 Barlow Report proposed a framework for pediatric obesity interventions divided into four stages, starting with prevention and education, and escalating toward pharmacotherapy and bariatric surgery (Barlow & Expert Committee, 2007). Behavior modification is foundational at every stage of intervention. As such, individuals who are not expected to be able to comply with more significant behavioral and lifestyle changes have often been excluded from obesity interventions (Broder-Fingert et al., 2014). For children with ASD, this is particularly troublesome, as not only are they more likely to have obesity, but they are more likely to develop obesity-related comorbidities like Type 2 Diabetes (Chen et al., 2016). Children with ASD have also been excluded from more intense intensive obesity interventions like bariatric surgery, despite recent evidence that they have similar outcomes to their peers without ASD. Goddard et al. (2019) recently published a retrospective study of adolescent patients with developmental disabilities (4 out of 10 patients had ASD) that underwent bariatric surgery. They found no difference in early weight outcomes or complications between the patients with DD and a frequency-matched cohort. They also did not report differences in some of the complications that arise from poor compliance with behavior and dietary modifications, such as dehydration, vitamin and mineral deficiencies, and reduced durability of weight loss. The authors identified a selection bias toward patients with strong social support when offering bariatric surgery, again underlying the important role of the family in childhood obesity (Goddard et al., 2019), as well as socio-communicative skills that are often a challenge for children and youth with ASD.
Third, recently there has been growing recognition of the importance of adapting obesity interventions for children with ASD, and an increasing awareness that the bias surrounding the “inability to comply” with behavior modification may be unfounded. The experience of the present study suggests otherwise, however, the “ability to comply” evidenced by the children with ASD in our study was made possible by the BW team’s attention to their specific needs to participate.
Fourth, in pediatric obesity, and particularly among school age children (6 to 12 years old), the principal drivers of weight management are parental education and behavior modification (Golan et al., 2006; Jull & Chen, 2013). Some studies have even shown that parent-only interventions can be just as effective as family-based interventions that involve the affected child (Bouttell, et al. 2017; Chai et al., 2019/). This suggests that excluding children with ASD may not be justifiable when there is a parent or caretaker who can meaningfully participate in the program, although they may need additional support in implementing changes at home. Overall, our study demonstrated that families with children with ASD enrolled in a CBFLI have similar participation rates, attrition rates, and weight outcomes compared to their peers without ASD. This suggests that healthcare professionals leading obesity intervention programs should consider making modifications and adaptations to include patients with ASD and other developmental disabilities in their programs.
Limitations and next steps
This was a secondary analysis of data from a study meant to evaluate the impact of physical activity trackers on weight outcomes in patients participating in a CBFLI. Randomization into the two study arms of the original study was included as a variable in our multivariate analysis, and was found not to be statistically significant for the current study. The original study did not consider ASD diagnosis in randomization or other study protocols. As a clinical program, BW has had a developmentally inclusive approach since its inception in 2012, thus the study team did not initially plan to focus on participants with ASD. As such, although the original study is a prospective, RCT (Espinoza et al., 2017), and some of its robustness may have carried over into the current study, this analysis is more accurately described as a retrospective cohort study, and its evidence and conclusions should be evaluated using that study design. Self-selection bias is inherent in our current study; families had already agreed to participate in an intensive, structured weight management program prior to study initiation, suggesting increased motivation at baseline. Whether these findings generalize to a larger, less motivated population, is unknown.
The generalizability of our findings to other populations may also limited by both the small number of participants with ASD and the lack of phenotypic characterization. Another limitation is the relative homogeneity of the setting and participant demographics, consisting predominantly of low-income, Hispanic/Latino, Spanish-speaking families living in an urban environment. In future studies, a more rigorous characterization of the sample could result in a more personalized and tailored approach to treatment. Another factor limiting dissemination is that two of our program leads collectively have decades of professional experience with children with ASD in their clinical practice (as a nutritionist and an occupational therapist) outside of the BW program. While there were no explicit protocols or systematic accommodations for participating children with ASD, their experience informed the program’s overall approach to inclusion and accommodation. They were also more readily able to adapt as needed when children with ASD experienced behavior difficulties during the program. For other pediatric weight management programs that are considering an inclusive approach, it may be of value to consider adding team members in educational and clinical roles that have experience caring for children with ASD. It has been extensively discussed in the research literature on school settings that inclusion is more than just physical placement of children with ASD with typically developing peers in the same classrooms (Ochs et al., 2001). Our study extends this argument for weight management settings, showing that inclusion of children with ASD in such settings requires certain adaptations (e.g. predictable structure and routines, sensory environment, as outlined above) to allow for meaningful participation.
Finally, there were several aspects of the diagnosis of ASD that were not captured by our study because an evaluation of ASD was not part of the original study design. Cognitive capacity, physical mobility, global assessment of function, communication skills, and specific behavior challenges were not systematically assessed as part of this study, all of which are variables that can impact a child’s participation in a CBFLI. The lack of these data makes it difficult to generalize our findings to specific individuals or populations with ASD. The BW team reported working with patients with a wide variety of physical and cognitive capacity, as well as communication skills and behavioral issues. The fact that there were no significant differences in outcomes with children with ASD and children without ASD suggests that these factors may not be as influential, but future studies should more systematically characterize the developmental and behavioral status of children with ASD.
Conclusion
Our urban health center has adapted the BW program to meet the needs of our low-income, primarily Medicaid, Latino population. BW has been a successful intervention in stabilizing or decreasing BMI in participants who complete the program. Families with children with ASD were capable of participating in BW alongside peers without ASD and have similar completion rates and weight outcomes. Results suggest that CBFLI programs can meet the weight management needs of children with ASD using an inclusive approach and can potentially expand access to much needed obesity interventions for children with ASD.
Footnotes
Acknowledgements
We are grateful to all the families who participated in the program and made this study possible. We also would like to acknowledge Licetz Montoya, Patricia Castillo, Jennifer Zipkin, Aric Ponce, Lisa Lopez, and Audrey Lai who helped run the BodyWorks program and contributed to data collection efforts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the NIDDK-supported APA Research in Academic Pediatrics Initiative on Diversity (RAPID) program (NIH R25DK096944, PI: Glenn Flores). The funding source had no involvement in the study design, in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. This work was supported by grants UL1TR001855 and UL1TR000130 from the National Center for Advancing Translational Science (NCATS) of the U.S. National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.