
Abstract
Multimorbidity, defined as having two or more chronic health conditions, is associated with elevated polypharmacy and mortality. Autism spectrum disorder is a whole-body chronic health condition in which comorbidities – in particular co-occurring intellectual disability – contribute to high clinical heterogeneity, polypharmacy and premature mortality. We aimed to determine specific multimorbidity patterns among autism spectrum disorder + intellectual disability adults, and to identify participants’ subgroups based on multimorbidity features. We used baseline examination data from a previous exploratory prospective multicentric study that included 63 autism spectrum disorder + intellectual disability adults. Multimorbidity patterns and subgroups were determined using clustering approaches. We observed 84.1% multimorbidity, significantly associated with age. We identified a dominant multimorbidity pattern, combining immune dysfunction, gastrointestinal disorders, neurological, and joint diseases. Four participants’ subgroups could be distinguished by multimorbidity, autonomy and polypharmacy. Two clusters were distinguished by the prevalence and consequences of multimorbidity. One cluster involved women with endocrine disorders. The final cluster was composed of older adults with the lowest autism spectrum disorder severity but greater multimorbidity, including cardiovascular and kidney diseases. Our results support a role for the gut–brain axis in the pathophysiology of autism spectrum disorder + intellectual disability multimorbidity. Furthermore, we identified patient subgroups with specific needs, underscoring the importance of a holistic approach for autism spectrum disorder + intellectual disability adults.
Lay abstract
Multimorbidity relates to having multiple chronic health conditions. It is a risk factor for poor health and reduces life expectancy. Autistic people have multiple chronic health conditions and die prematurely, especially if they have an intellectual disability (autism spectrum disorder and intellectual disability). Certain pathophysiological processes observed in autism spectrum disorder are common to those related to the genesis and/or maintenance of multimorbidity. Furthermore, multimorbidity could be helpful in better identifying patient subgroups in autism spectrum disorder. It is therefore essential to better characterize multimorbidity and its consequences in the subgroup of autism spectrum disorder + intellectual disability individuals to offer them personalized care. We conducted a preliminary study of 63 autism spectrum disorder + intellectual disability adults to classify them according to their multimorbidity and search for a specific combination of chronic health conditions. We observed high and early multimorbidity in this sample and identified four classes of participants, distinguished by their multimorbidity status, independence and number of treatments. In addition, we observed a dominant combination of multimorbidity in our sample, combining immune dysfunction and gastrointestinal disorders, neurological and joint diseases. These findings support the hypothesis that an altered gut–brain relationship is involved in the risk of autism spectrum disorder, its outcome, and its association with chronic health conditions. Although larger studies are needed, our results suggest that subgroups of autism spectrum disorder + intellectual disability individuals can be identified based on their multimorbidity and potentially different ageing trajectories. A more comprehensive and personalized approach is needed to reduce the burden of multimorbidity and increase the quality of life and life expectancy in autism spectrum disorder/ intellectual disability.
Introduction
Comorbidities are concomitant acute or chronic disorders associated with a primary health condition. A disorder (primary or comorbid) is considered to be chronic if it evolves slowly, lasts over time, and induces long-term functional disability (Bernell & Howard, 2016). Chronic disorders can be classified into categories called chronic health conditions (Kirchberger et al., 2012). Multimorbidity is defined as the association of at least two chronic health conditions. Multimorbidity affects 23.2% of the general population and has been found to occur earlier and more frequently for adults with mental disorders (Barnett et al., 2012). The prevalence of multimorbidity increases with age, reaching 58% of individuals above the age of 65 years (Kirchberger et al., 2012). The underlying pathophysiological processes that lead to multimorbidity include inflammageing, a systemic chronic low-grade inflammation frequently found in chronic diseases throughout ageing (Calderon-Larranaga et al., 2019a; Candore et al., 2010; Chung et al., 2009; Pupek et al., 2016). Multimorbidity is a crucial public health issue (Uijen & van de Lisdonk, 2008), as it is associated with severe disability (Marengoni, Angleman, & Fratiglioni, 2011), functional impairment, alterations in the quality of life (Marengoni, Angleman, Melis, et al., 2011), polypharmacy (Calderon-Larranaga et al., 2019b) and mortality (Gijsen et al., 2001). Awareness of multimorbidity is central to improving care (Pefoyo et al., 2015; Sinnott et al., 2013).
Autism spectrum disorder 1 (ASD) is characterized by social communication impairment associated with restricted interests and repetitive and stereotyped behaviours (American Psychiatric Association, 2013). This condition is frequently associated with other neurodevelopmental disorders (NDDs) (Morris-Rosendahl & Crocq, 2020), such as intellectual disability (ID), affecting from 30% to 70% of autistic individuals (Christensen et al., 2016; Matson & Shoemaker, 2009). Multiple health conditions are also associated with ASD (Bishop-Fitzpatrick & Rubenstein, 2019; Croen et al., 2015; Fortuna et al., 2016; Gilmore et al., 2021; Hand et al., 2020; Weir et al., 2021), including immune dysfunction, gastrointestinal disorders and neurological diseases, in particular epilepsy (McElhanon et al., 2014; Sala et al., 2020). Co-occurring psychiatric disorders are also frequent in ASD, such as hyperactivity, anxiety, sleep disturbances and depression (Hollocks et al., 2019; Hudson et al., 2019; Lai et al., 2019). Comorbidity prevalence rates in ASD vary depending on the study (Lai et al., 2019), age (Bishop-Fitzpatrick & Rubenstein, 2019; Wise et al., 2017) and associated ID (Amiet et al., 2008; Bishop-Fitzpatrick & Rubenstein, 2019).
The frequency of co-occurring comorbidities in ASD suggests that it is not so much a brain disease as a complex whole-body chronic health condition. Moreover, autistic individuals show specific inflammatory (Masi et al., 2015) and nutritional patterns (Zimmer et al., 2012), two factors known to influence multimorbidity in the general population (Calderon-Larranaga et al., 2019a). Furthermore, these patterns are often associated with a higher number of drug prescriptions and high healthcare costs for autistic adults (Vohra et al., 2017). The quality of life of autistic individuals is also negatively influenced by comorbidities and a poor health status (Hossain et al., 2020; Turcotte & Shea, 2021). In addition, premature mortality has been reported in ASD to be associated with polypharmacy and chronic health conditions, in particular, mental disorders, epilepsy and ID (Bishop-Fitzpatrick & Rubenstein, 2019; Hirvikoski et al., 2016; Hwang et al., 2019; Smith DaWalt et al., 2019; Woolfenden et al., 2012). Evidence suggesting a role of multimorbidity in ASD includes the complexity of this global health condition, a high comorbidity burden, polypharmacy and premature mortality. ID appears to be an exacerbating factor for poor physical health in ASD. Indeed, ASD + ID individuals show higher polypharmacy, use of psychotropic medications (Saqr et al., 2018), and mortality (Hwang et al., 2019) than individuals with single ASD.
Thus, as described for individuals with single ID (Cooper et al., 2015; Hussain et al., 2020), there is also likely to be a high frequency and early onset of multimorbidity in ASD, characterized by both a reduced life expectancy and pathological or premature ageing, in particular, in the ASD + ID subgroup (Wise, 2020). Nonetheless, there have been a few studies focusing on multimorbidity and its consequences in ASD and ASD + ID.
The clinical heterogeneity of ASD is well known, and the challenge lies in identifying clinical subgroups of autistic individuals potentially related to endophenotypes that can be used to understand the underlying physiopathology and propose personalized treatment (Lombardo et al., 2019). In the literature, clinical subgroups have been identified based on diverse variables, such as autistic symptoms (social communication level (Di Rezze et al., 2016)), intellectual level (Demetriou et al., 2019; Seng et al., 2021), or motor patterns (Craig et al., 2021)), neuronal physiology (electroencephalogram patterns (Capal et al., 2018) and neuroanatomical patterns (Yamagata et al., 2019). However, comorbidities have been, paradoxically, rarely considered, despite their frequency in ASD. In addition, available studies concern the prevalence of comorbidities or their risk factors, but not the identification of clinical subgroups in ASD. Moreover, findings have highlighted heterogeneity in the long-term outcome trajectories of autistic individuals (Baghdadli et al., 2018), which may suggest that ageing trajectories are also heterogeneous. The use of multimorbidity to distinguish subgroups of individuals appears to be useful for identifying distinct ageing trajectories. In addition, analysing patterns of multimorbidity in a well-described ASD + ID population would help to identify common pathophysiological processes underlying various chronic health conditions during ageing (Smith et al., 2018). Ultimately, addressing multimorbidity in ASD could improve the quality of life, as well as the preventive and overall care of this population, and reduce mortality. The aim of our exploratory study was to uncover specific multimorbidity patterns and to identify clinical subgroups defined on the basis of their associated chronic health conditions in a well-characterized sample of ASD + ID individuals.
Methods
Participant recruitment
The EFAAR (Frailty Assessment in Ageing Adults with Autism Spectrum and Intellectual Disabilities) study is an ongoing prospective multicentric study. Participants were recruited between 2015 and 2018 from 10 medico-social institutions where they lived, in the south of France. The study protocol has been thoroughly described in a previous publication (Miot et al., 2019). All participants had a confirmed diagnosis of ASD + ID and were aged over 20 years. Sixty-three participants were included in the EFAAR study and are being followed up for 5 years. The present exploratory study is based on the baseline examination data.
Measures collected at baseline
Baseline assessment was performed in the participant’s residence by two evaluators, a physician and a psychologist. It consisted of observing the participant, doing a medical examination, a participant’s daily helpers interview to complete questionnaires, and considering the participant’s medical record.
Participants were divided into two age subgroups: ‘adults’, aged under 50 years, and ‘older adults’, aged 50 years and over. We chose a cut-off of 50 years based on previous studies performed on people with ID (Hermans & Evenhuis, 2014; Schoufour et al., 2017).
ASD severity was assessed using the Childhood Autism Rating Scale (CARS) (Schopler et al., 1986), a behavioural rating scale completed by the evaluators. Information from clinical observation and a proxy report were used to assign the CARS ratings.
Adaptive functioning was assessed using the Vineland Adaptive Behaviour Scale II (VABS-II) (Sparrow et al., 1984), a semi-structured interview completed by the evaluator in collaboration with daily helpers. The daily-life subscore was used to evaluate the participants’ autonomy.
Pharmacological treatment data were collected using medical records, with polypharmacy defined as the prescription of at least five different daily medications. The Drug Burden Index (DBI) was calculated for each participant using the anticholinergic burden calculator (www.anticholinergicscales.es/calculate). The DBI is defined as the sum of anticholinergic and sedative effects for each prescribed drug and is indirectly related to psychotropic drug use (Byrne et al., 2018).
Comorbidities were assessed using multiple sources: medical records, biological check-ups, standard medical examination of participants and questionnaires. Biological data were extracted from the last health check-up of <1 year before. The physical examination included cardiovascular, vascular, pulmonary, abdominal, neurological, ENT (ear, nose, throat), skin, lymph node and thyroid examination, with vital measures added to search for orthostatic hypotension. Neurocognitive disorders were screened using the Dementia Screening Questionnaire for Individuals with Intellectual Disabilities (DSQIID) (Deb et al., 2007). This hetero-questionnaire dedicated to people with ID is completed during an interview with the participant’s carer. It assesses changes in behaviour and autonomy during the prior 6 months. Mental disorders were screened using the Reiss scale (Kishore et al., 2010; Reiss, 1987). This hetero-questionnaire assesses co-occurring psychiatric disorders, for individuals with ID through an interview with the participant’s carer.
A developmental quotient (DQ) was estimated from the daily-life subscore of the VABS-II using Stern’s formula (Stern, 1914): developmental age (defined based on the daily-life subscore of the VABS-II)/chronological age × 100. Indeed, an intelligence quotient (IQ) cannot be calculated because participants could not participate in the classic psychological tests due to lack of instructions’ understanding (Miot et al., 2019).
Outcomes
Forty-four comorbidities, described in a previous article (Miot et al., 2019), were screened and grouped into 14 categories of chronic health conditions: eye diseases, cardiovascular diseases, endocrine disorders, joint diseases, gastrointestinal disorders, mental disorders, kidney diseases, neurological diseases, immune dysfunction, hypertension, stroke, cancers, lung diseases and liver diseases (Supplementary Table 1). These categories were previously used in the general population of older people to identify the prevalence and patterns of multimorbidity (Kirchberger et al., 2012). For the mental disorders category, ASD and ID were not considered to be mental disorders because these NDDs were included within our population characteristics. A chronic health condition was considered only if present at the time of inclusion. For example, having recovered from cancer was not considered to be a chronic health condition, whereas therapeutically controlled hypertension was. Multimorbidity was defined as the coexistence of at least two chronic health conditions.
Community involvement statement
Community members were not involved in the study.
Management of missing data
Twelve participants had missing data for chronic health conditions: three for hypertension and nine for kidney diseases. The missing data were replaced through multiple imputations using chained equation imputations that assumed the data to be randomly missing. Among the 100 imputed tables, missing data were imputed by the absence of disease for more than 90% for kidney diseases and 70% for hypertension. We thus assumed that these nine participants had no kidney disease, which was consistent with other clinical data. By contrast, due to the heterogeneity of imputations on hypertension, no choice was made for the three participants. To retain the three participants in our cluster analysis, their missing hypertension data were first analysed using the R package ‘missMDA’ before multiple correspondence analysis (MCA). Thus, the imputed data for these three participants did not contribute to the creation of any factors.
Statistical analysis
Mean values with standard deviations (SDs) or medians with interquartile ranges (IQRs) are reported for continuous variables, depending on the normality of the data distribution, and frequencies with percentages for categorical variables. Characteristics of the participants were compared using chi-square or Fisher’s tests, as appropriate, for categorical variables and the Wilcoxon Mann–Whitney test or analysis of variance (ANOVA) regression for continuous variables.
To guarantee the reliability of the results, only chronic health conditions with a prevalence ⩾10% were used to (1) explore multimorbidity patterns and (2) identify clinical subgroups (Hermans & Evenhuis, 2014) (Supplementary Table 1).
First, patterns of multimorbidity were investigated by clustering the variables with a hierarchical ascending classification (HAC) approach using the ward method (R package ‘ClustOfVar’). We examined the frequencies of multimorbidity patterns by assigning patients to a pattern if they had at least two chronic health conditions in the corresponding pattern. Differences in multimorbidity patterns were assessed by age group.
Second, an MCA was performed to reduce the dimensions of the data set using active and non-redundant variables that reflect chronic health conditions: eye disease, cardiovascular disease, endocrine disorder, joint disease, gastrointestinal disease, mental disorder, kidney disease, neurological disease, immune dysfunction and hypertension. The number of factors was defined using the elbow criteria. The factors derived from the MCA were (1) compared to the patterns of multimorbidity obtained previously and (2) used to perform the cluster analysis.
Third, a cluster analysis was performed to identify participant subgroups with multimorbidity endophenotypes (R package ‘FactoMineR’). The clustering was based on a mixed method combining: (1) an HAC to determine the optimal number of classes using semi-partial R-squared and the barycentre of each class (the Euclidian distance and Ward’s method were used for the HAC) and (2) a K-means method to define the final clusters by assigning each patient to one of the classes. The number of classes and the barycentre of each from the HAC were used to initiate the K-means method. The stability of the classification was checked by modifying the number of factors of the MCA.
The characteristics of the clusters were compared using chi-square tests for categorical variables and ANOVA regressions or the Kruskal–Wallis test for continuous variables. Pairwise comparisons were performed using the Bonferroni post hoc test. Descriptive variables used to characterize the subgroups of participants included the sex, age, number of chronic health conditions, presence of multimorbidity, CARS score, VABS-II daily-life subscore, polypharmacy and DBI.
All statistical tests were considered significant for p < 0 .05. Statistical analyses were performed using SAS Enterprise Guide version 7.13 (SAS Institute Inc., Cary, NC, USA) and R software version 4.0.2.
Results
Sample characteristics
Sixty-three participants were included in the EFAAR cohort: 27% women and 73% men. The median age was 46 years (IQR = 26–57), with 33 participants aged under 50 years (adults) and 30 aged 50 years or over (older adults) (Table 1). Older adults had a more severe ID and a better VABS communication subscore. Clinical characteristics of the whole population and according to each age subgroup are described in Table 1.
Characteristics of participants according to their age group.

IQR: interquartile range; VABS-II: Vineland Adaptive Behaviour Scale II; SD: standard deviation; CARS: Childhood Autism Rating Scale.
Characteristics of whole population, adults and older adults’ groups are expressed in percentage, mean ± standard deviation or median with interquartile ranges.
p-values are described for the comparison of characteristics between adults and older adults.
Significant differences between these two groups are considered for p-value<0.05 and are indicated in bold.
Multimorbidity prevalence rates
The prevalence of multimorbidity was 85% for the whole sample, 79% for adults and 90% for older adults (Table 1). Older adults showed significantly more multimorbidity than adults aged under 50 years (p-value < 0.01). The whole population had 3.29 (±1.83) chronic health conditions. The number of chronic health conditions increased significantly with age (2.58 (±1.39) for adults vs 4.07 (±1.95) for older adults, p-value < 0.001). The most frequent chronic health conditions in the whole population were gastrointestinal disorders (58.7%), neurological diseases (42.9%), mental disorders (41.3%), endocrine disorders (36.5%), immune dysfunction (27.0%) and kidney diseases (23.8%) (Table 2). Older adults had a significantly higher prevalence of kidney diseases (46.7% vs 3.0% in adults, p-value < 0.001) and cardiovascular diseases (33.3% vs 9.1% in adults, p-value = 0.02). Older adults showed a higher prevalence of hypertension (20.7% vs 12.9%), eye diseases (30.0% vs 12.1%) and joint diseases (26.7% vs 12.1%) than adults but the differences were not statistically significant (Table 2).
Prevalence for each chronic health condition in the EFAAR cohort.
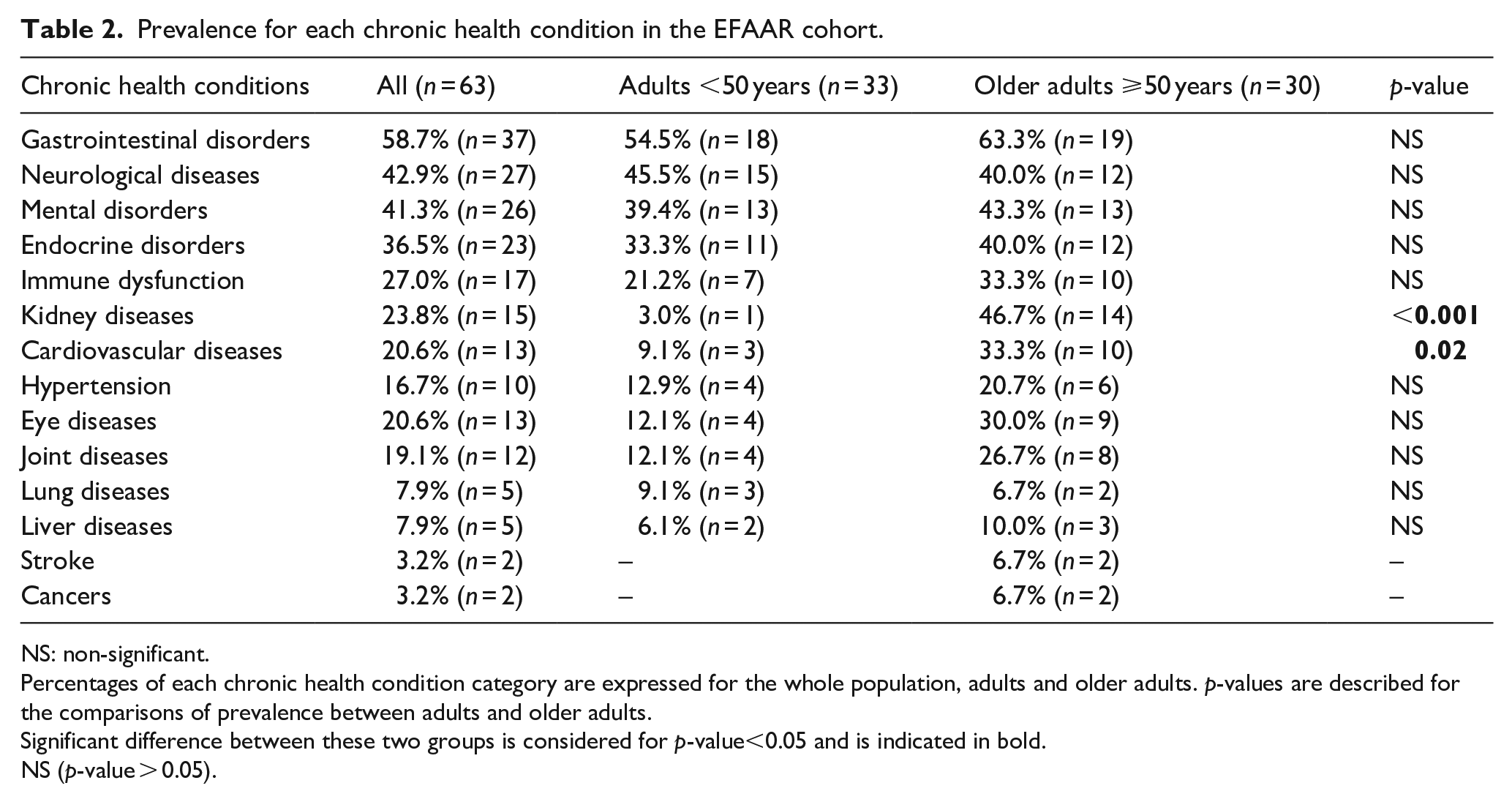
NS: non-significant.
Percentages of each chronic health condition category are expressed for the whole population, adults and older adults. p-values are described for the comparisons of prevalence between adults and older adults.
Significant difference between these two groups is considered for p-value<0.05 and is indicated in bold.
NS (p-value > 0.05).
Multimorbidity patterns
Associated chronic health conditions were grouped using HAC to identify specific multimorbidity patterns. Four groups were found: (A) cardiovascular diseases-hypertension, (B) mental disorders–eye diseases, (C) kidney diseases–endocrine disorders and (D) immune dysfunction–gastrointestinal disorders–neurological–joint diseases (gain in cohesion 41.8%). The assignment of multimorbidity patterns to participants indicated an over-representation of the immune dysfunction–gastrointestinal disorders–neurological–joint diseases pattern (31 participants), whereas other patterns were under-represented (Table 3). Twenty-six participants did not belong to any pattern, 26 belonged to only one pattern and 11 belonged to at least two patterns. We used the MCA analysis to consolidate the identification of multimorbidity patterns (Supplementary Table 2). The first MCA axis contrasted subjects with gastrointestinal disorders, neurological, and joint diseases with subjects without any gastrointestinal disorders, consistent with group D obtained above.
Chronic health conditions groups.
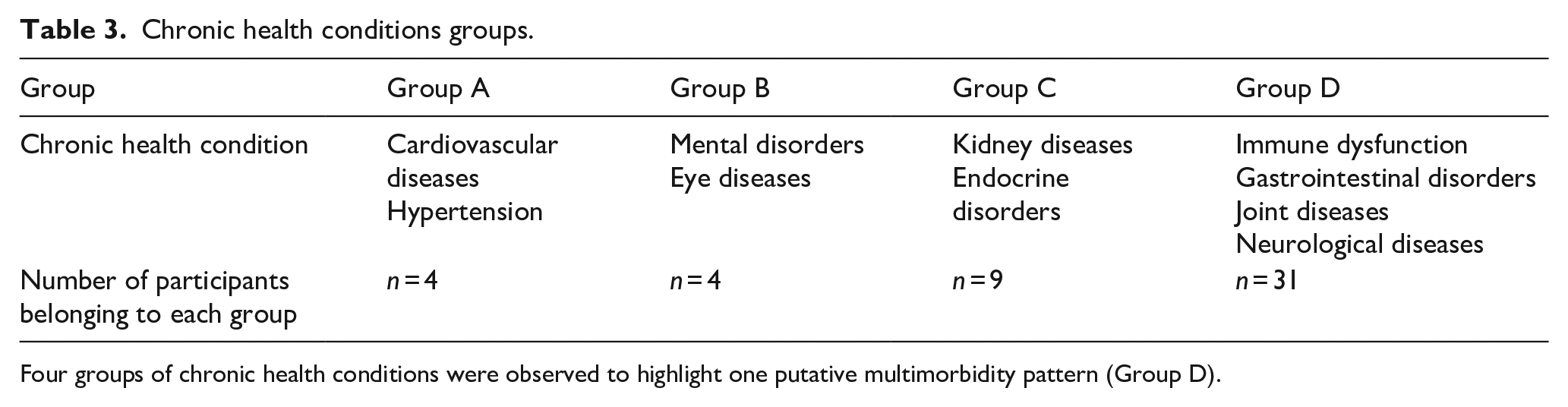
Four groups of chronic health conditions were observed to highlight one putative multimorbidity pattern (Group D).
Multimorbidity patterns for age subgroups were not stable due to the small sample size and are thus not presented.
Multimorbidity subgroups
Four clusters of participants were identified according to their associated chronic health conditions using the mixed method (Tables 4 and 5). Due to the small size sample, centre-effects could not be analysed. Nevertheless, the repartition of centres between the participant clusters was homogeneous (Supplementary Table 3).
Clinical characteristics for each cluster of participants.
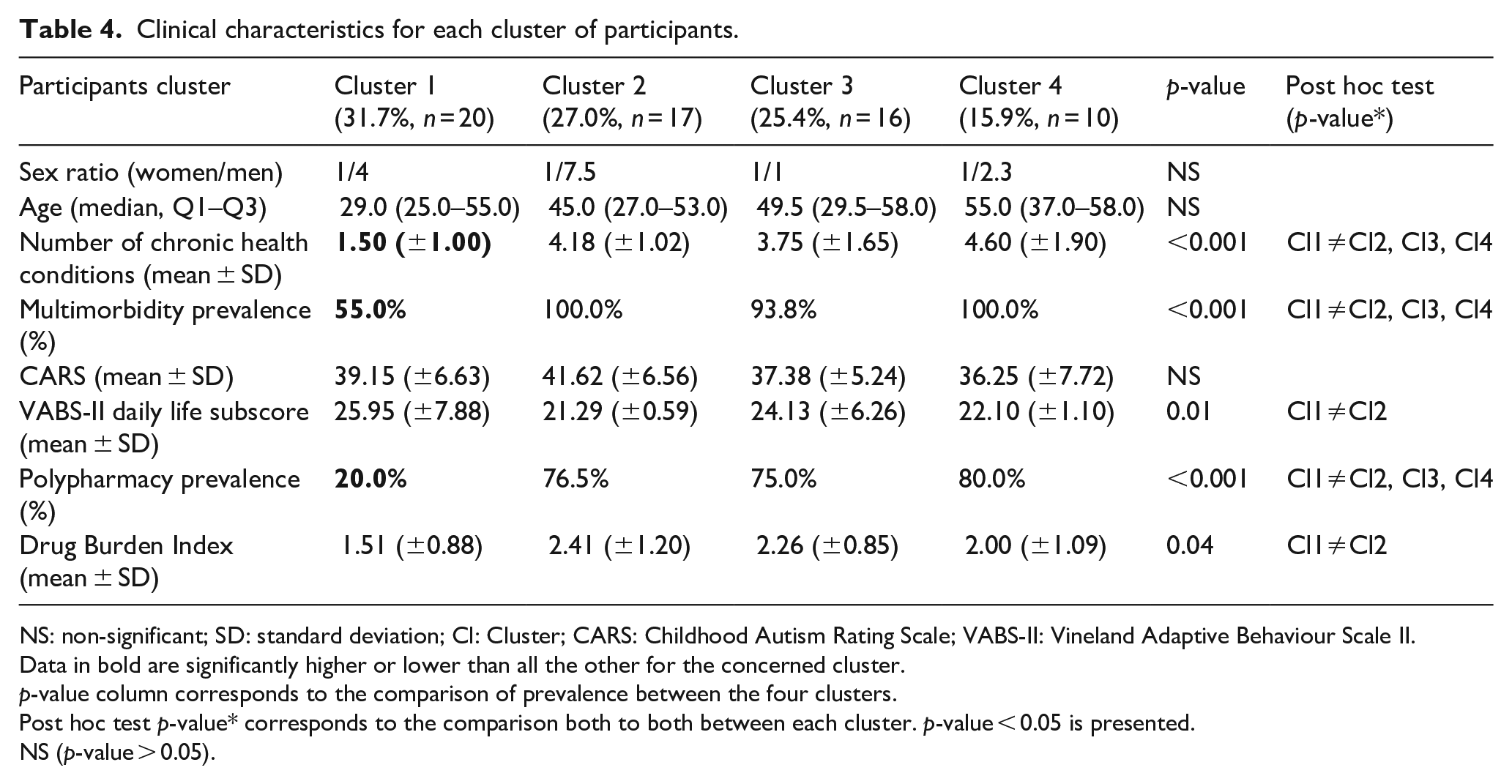
NS: non-significant; SD: standard deviation; Cl: Cluster; CARS: Childhood Autism Rating Scale; VABS-II: Vineland Adaptive Behaviour Scale II.
Data in bold are significantly higher or lower than all the other for the concerned cluster.
p-value column corresponds to the comparison of prevalence between the four clusters.
Post hoc test p-value* corresponds to the comparison both to both between each cluster. p-value < 0.05 is presented.
NS (p-value > 0.05).
Prevalence of chronic health conditions for each cluster of participants.

NS: non-significant.
Percentages are the proportions of affected participants into the cluster. Prevalence in bold are significantly higher or lower than all the other for the concerned cluster.
p-value column corresponds to the comparison of prevalence between the four clusters.
Post hoc test p-value* corresponds to the comparison both to both of prevalence between each cluster. p-value < 0.05 is presented.
NS (p-value > 0.05).
Cluster 1: absence of gastrointestinal disorders and low multimorbidity and polypharmacy
This cluster included 31.7% of participants (n = 20). Approximately one quarter (23.5%) of the women was included in this cluster. Individuals in this subgroup were mostly (60.0%) adults aged under 50 years (median age = 29.0 years, IQR age = (25.0–55.0)), and had the highest daily-life subscore in the VABS-II (25.95 (±7.88)) among the four clusters and a moderate CARS score (39.15 (±6.63)). In addition, they had the lowest rates of polypharmacy (20%) and multimorbidity (55%), and 90.0% of the EFAAR participants without any multimorbidity (n = 10) were grouped in this cluster. Participants had an average of 1.5 (±1.00) associated chronic health conditions, none had gastrointestinal or endocrine disorders, <10.0% had kidney diseases or hypertension, and 20.0% had neurological diseases or mental disorders. Finally, polypharmacy was reported in 20.0% and the DBI scores were the lowest (1.51 (±0.88)) among the four clusters.
Cluster 2: presence of mental disorders, systematic multimorbidity and high polypharmacy
This cluster included 27.0% of participants (n = 17), consisting mostly of adults aged under 50 years (58.8%) and men (88.2%). Approximately 12% (11.8%) of the women were included in this cluster. These participants had the lowest VABS-II daily-life subscore (21.29 (±0.59)) and the highest CARS score (41.62 (±6.56)). All participants showed multimorbidity, with a mean of 4.18 (±1.02) chronic health conditions per individual. All had gastrointestinal disorders and 82.4% had neurological diseases and mental disorders. Few had cardiovascular diseases (5.9%) or hypertension (17.65%). The polypharmacy rate was high (76.0%), and the DBI score was the highest among the four clusters (2.41 (±1.12)).
Cluster 3: presence of endocrine disorders, high multimorbidity and polypharmacy
This cluster included 25.4% of participants (n = 16). Half of them were older adults, and half were women. Almost half (47.1%) of the women were included in this cluster. They had a daily-life VABS-II subscore of 24.13 (±6.26) and a moderate CARS score (37.38 (±5.24)). Multimorbidity was very frequent (94.0%), with endocrine disorders found for 100% of participants, gastrointestinal disorders for 68.8% and kidney diseases for 43.8%. No participants had cardiovascular diseases, one had hypertension, another joint disease and 25.0% neurological disease. Polypharmacy was frequent (76.5%), and the DBI was over 2 (2.26 (±0.85)).
Cluster 4: presence of cardiovascular and kidney diseases, systematic multimorbidity and high polypharmacy
This cluster included 15.9% of participants (n = 10). Approximately 18% (17.6%) of the women were included in this cluster. Participants were mostly older adults, as 70.0% were aged 50 years or older (median age = 55.0 years, IQR = (37.0–58.0)). The VABS-II daily-life subscore was 22.10 (±1.10), and all participants showed multimorbidity. The mean number of chronic health conditions was the highest (4.60 (±1.90)). Most had gastrointestinal disorders (90.0%) or cardiovascular diseases (90.0%). Polypharmacy was frequent (80.0%), even if the DBI score was 2.00 (±1.09).
There were significant differences between these four clusters for the prevalence of gastrointestinal disorders, neurological diseases, mental disorders, endocrine disorders, kidney diseases, cardiovascular diseases, hypertension and joint diseases (p < 0.05) (Table 5) and epilepsy (p = 0.01, data not shown). Moreover, these four participants clusters were significantly different according to the number of associated chronic health conditions (p < 0.001), as well as the VABS daily-life subscore (p = 0.01), polypharmacy (p < 0.001) and DBI score (p = 0.04). There were no significant differences in age, gender or ASD severity between the subgroups (Table 4).
Discussion
Past studies have suggested a putative association between multimorbidity and ASD, in particular, common pathophysiological mechanisms, such as chronic inflammation (Calderon-Larranaga et al., 2019b; Masi et al., 2015) and the subsequent consequences, such as premature mortality (Bishop-Fitzpatrick & Rubenstein, 2019; Gijsen et al., 2001; Hirvikoski et al., 2016; Hwang et al., 2019; Smith DaWalt et al., 2019; Woolfenden et al., 2012).
We found high multimorbidity prevalence rates for ASD + ID adults, increasing in older adults, in particular, affected by epilepsy, kidney and cardiovascular diseases. In our cohort, polypharmacy and autonomy appeared to be critical factors associated with multimorbidity. We also identified a specific multimorbidity pattern related to the gut–brain axis. We observed four clusters according to multimorbidity among our participants. The clusters were characterized by the absence of gastrointestinal disorders in the first, the presence of mental disorders in the second, endocrine disorders in the third, and cardiovascular and kidney diseases in the fourth. These results suggest that chronic health conditions could contribute to define subgroups among ASD + ID patients and could help to predict clinical and outcome trajectories. Two clusters included most of the adults aged under 50 years, one included half of the women, and the last included essentially older adults. These findings highlight several aspects that have an impact on ASD, including ageing trajectories in ASD + ID, the effect of gender on health in ASD and the care needed by ASD + ID adults.
High and early multimorbidity in ASD + ID adults
Prevalence rates of multimorbidity in samples of individuals with only ID aged over 40 years have been reported to range from 53.5% to 79.8% (Cooper et al., 2015; Hermans & Evenhuis, 2014; Hussain et al., 2020; McCarron et al., 2013). The prevalence rate of multimorbidity appears to be higher in our sample of ASD + ID individuals (84.1%). It is known that the number of chronic health conditions increases with age, both in the general population (Barnett et al., 2012) and for people with ID (Hermans & Evenhuis, 2014). Nevertheless, the prevalence rate of 78.8% of multimorbidity in our sample and the number of chronic health conditions per person in the adults aged under 50 years (2.58) are higher than in the general population (Barnett et al., 2012), suggesting higher but also earlier multimorbidity in ASD + ID.
Previous research on samples of individuals with ID has shown the number of chronic health conditions per subject to be 3.6 per individual aged over 40 years (Hussain et al., 2020), and >4 for Down syndrome, severe ID and older age (Hermans & Evenhuis, 2014), whereas participants in our sample aged over 50 years had an average of >4 chronic health conditions. However, the specific impact of ID on multimorbidity in our sample could not be assessed because all participants had profound or severe ID (Miot et al., 2019).
The most common chronic health conditions reported for older adults with ID are arthritis, psychiatric disorders and diabetes, but this is largely dependent on age, gender, aetiology and the severity of the ID (Hermans & Evenhuis, 2014; Hussain et al., 2020; Kinnear et al., 2018; McCarron et al., 2013). Furthermore, it has been suggested that joint diseases, neurocognitive impairment, cardiovascular diseases and strokes occur earlier for autistic older adults than in the general population (Hand et al., 2020). In our sample of ASD + ID adults, gastrointestinal disorders, neurological diseases and mental disorders appeared to occur often, which is common in ASD (McElhanon et al., 2014; Sala et al., 2020). However, we found that the prevalence of these disorders was higher than in autistic children and autistic young adults (Kohane et al., 2012), perhaps related to a higher age in our sample and to the association of ASD with severe ID. Besides, we found more cardiovascular and kidney diseases in older adults than in adults. Although these diseases commonly increase with age in the general population (Barnett et al., 2012), the possibility of greater susceptibility must be considered for ASD + ID individuals. Indeed, poorer cardiovascular health has been reported for autistic people (Bricout et al., 2018), and the hypothesis of a higher cardiovascular risk due to autonomic dysfunction has been put forward (Thapa et al., 2019). In reality, an elevated level of cardiovascular disease is observed in adulthood, affecting approximately half of autistic adults (Bishop-Fitzpatrick & Rubenstein, 2019). Furthermore, we have previously shown that kidney disease was associated with cardiovascular risk factors in our study ASD + ID population (Miot et al., 2019). In addition, several recent studies have highlighted putative genetic vulnerability to kidney disease in ASD as early as in childhood (Clothier & Absoud, 2021), which may be compounded by cardiovascular diseases and ageing itself.
Polypharmacy is closely associated with multimorbidity and has been reported to be 50% for adults with ID and an average age of 55 years (O’Dwyer et al., 2016). Previous studies on ASD + ID adults showed 57% polypharmacy for those with an average age above 30 years (Espadas et al., 2020). In our sample, 58.7% of ASD + ID participants were affected by polypharmacy, as our cohort had an average age of 43 years. This finding suggests that polypharmacy is higher from early adulthood in ASD + ID than in people with isolated ID.
Multimorbidity patterns and the pathophysiology of ASD
Four specific multimorbidity patterns have been reported in the general population: cardiovascular–metabolic diseases, joint–liver–lung–eye diseases, mental–neurological disorders and cancer–gastrointestinal disorders (Kirchberger et al., 2012). For people with ID aged over 50 years, mental–neurological disorders was the only pattern to be identified (McCarron et al., 2013), but this finding was not replicated in another study (Hermans & Evenhuis, 2014).
The most frequent pattern found in this study was the immune dysfunction–gastrointestinal disorders–neurological–joint diseases pattern (pattern D), identified in approximately half of our sample. These findings, obtained in ASD + ID adults, are consistent with the gut–brain axis and immune dysfunction hypotheses for the pathophysiology of ASD (Iglesias-Vazquez et al., 2020; Ye et al., 2021) and potentially ASD + ID. Indeed, intestinal dysbiosis is common in ASD and could contribute to neuroinflammation through systemic chronic low-grade inflammation and impairment of the brain–blood barrier (Yousefi et al., 2022). Furthermore, immune dysfunction has been reported in ASD, as well as in other NDDs (Hsu et al., 2021). Thus, in multimorbidity pattern D, immune dysfunction could be a general condition of NDDs, whereas gastrointestinal disorders and neurological diseases association could be more ASD specific.
This highlights the importance of the involvement of the gut–brain axis in ASD + ID, not only during early development but also during adulthood and ageing. Indeed, the gut–brain axis could be involved in neurodegenerative processes (Yousefi et al., 2022), and inflammageing in chronic health conditions and multimorbidity (Calderon-Larranaga et al., 2019a; Candore et al., 2010; Chung et al., 2009; Pupek et al., 2016). In our sample, the gut–brain axis was over-represented in Cluster 2, which showed a more severe multimorbidity burden, and, potentially, a suspected high risk of premature death (see section ‘Cluster specificities’). Thus, it is possible to speculate that gut–brain axis dysfunction could trigger or enhance the processes of multimorbidity and pathological ageing in ASD and ASD + ID. Impairment of the gut–brain axis could induce or synergise with chronic low-grade inflammation, which contributes to multimorbidity and the development of inflammageing (Calder et al., 2017).
Cluster specificities
We performed cluster analysis to identify subgroups based on multimorbidity of the participants, highlighting certain hypotheses for the heterogeneity of the clinical presentation and outcomes in ASD + ID.
Clusters 1 and 2 were identified primarily among younger adults, and we were able to identify two subgroups of ASD + ID adults: one (Cluster 1) with low multimorbidity and few consequences in terms of autonomy and polypharmacy and the other (Cluster 2) with higher multimorbidity and more negative consequences, such as polypharmacy and reduced autonomy. Polypharmacy among adults with ID is higher than in the general population (O’Dwyer et al., 2016). Moreover, this population suffers from the inappropriate prescription of psychotropic medications (O’Dwyer et al., 2018). In this ID population, polypharmacy is associated with psychiatric disorders and higher use of healthcare (Bratek et al., 2017), and precipitates premature death (Cooper et al., 2020; Schoufour et al., 2018). As in ID, polypharmacy appears to play a key role in the comorbidity burden (Miot et al., 2019) and multimorbidity in our study ASD + ID population. Moreover, polypharmacy is over-represented in Cluster 2, which includes a high DBI, more mental disorders and the lowest level of autonomy. Thus, the management of polypharmacy, particularly that of psychotropic use, may be essential for younger ASD + ID adults with co-occurring mental disorders (Espadas et al., 2020) to improve their autonomy and quality of life. Furthermore, Cluster 2 may be more specifically related to ASD due to typical comorbidities related to the gut–brain axis (Iglesias-Vazquez et al., 2020). Indeed, intestinal dysbiosis is mainly reported for individuals with NDDs, including ASD and attention deficit hyperactivity disorder, but rarely in ID (Jurek et al., 2021). Neurological disorders are also over-represented in Cluster 2 (82.4%), whereas a rate of 19%–36% has been reported for adults with ID only (Hermans et al., 2014; McCarron et al., 2013). This ASD specificity of Cluster 2 could contribute to its higher polypharmacy.
Cluster 3 contained 50% women, indicating a male-to-female ratio of 1, whereas it is generally in the range of 3–4 for autistic adults (Loomes et al., 2017) and 1.91 for ASD + ID adults (Posserud et al., 2021). This cluster included middle-aged individuals with high multimorbidity. Previous studies have also suggested more chronic health problems in women with ID (Kinnear et al., 2018), as for autistic women regardless of age, ethnicity, education, body mass index (BMI) or addictions (Weir et al., 2021). Multimorbidity is two times higher in women than in men with ID at a comparable age and intellectual level (McCarron et al., 2013). Moreover, autistic women have more chronic health conditions than autistic men and women from general population, primarily due to endocrine disorders (Kassee et al., 2020), of which prevalence was significantly higher in our third cluster. However, we did not observed over-representation of cardiovascular or neurological diseases in this Cluster 3, although previously described in autistic women (Amiet et al., 2008; Weir et al., 2021). Furthermore, polypharmacy was high in this group, with a DBI >2, indicating a high prescription rate of psychotropic drugs, even though mental disorders were reported for only about one-third of this cluster. This raises the question of greater iatrogeny, as well as inappropriate prescriptions for ASD + ID women. Moreover, these findings suggest a specific multimorbidity pattern among ASD + ID women and specific medical care needs (Houy-Durand, 2019b) that need to be further studied, especially as they typically have lower access to care and medical follow-up (Ames et al., 2021; Olsen et al., 2021; Woolfenden et al., 2012) and a higher mortality rate than autistic men (Woolfenden et al., 2012). Finally, the over-representation of women in Cluster 3 echoes questions about a specific clinical phenotype of autistic women.
Cluster 4 consisted primarily of the older adults in our sample. This subgroup showed high multimorbidity, with the highest concentration of chronic health conditions relative to the other clusters. Nevertheless, such high multimorbidity appears to be due to the common chronic health conditions seen in ageing: joint disease, hypertension, cardiovascular and kidney diseases (Barnett et al., 2012). Nevertheless, kidney diseases in this cluster could also be specifically related to ASD because this co-occurring disorder is not generally reported in samples with ID alone (Hermans et al., 2014; McCarron et al., 2013), and, as mentioned previously, there are several arguments for a genetic predisposition to kidney diseases in ASD (Clothier & Absoud, 2021). Of note, the frequency of epilepsy was significantly higher in this cluster than in the other three, which is consistent with previous studies reporting a higher prevalence of epilepsy in older autistic adults, especially if they have ID (Bishop-Fitzpatrick & Rubenstein, 2019). Epilepsy appears to be more frequent among people with ID (Kinnear et al., 2018) or severe disability (Van Timmeren et al., 2017) than in the general population, but without any increase with age for adults with ID alone (Kinnear et al., 2018; McCarron et al., 2013). Thus, the observed higher rates of epilepsy in older adults of our ASD + ID cohort could be a specific complication of ageing with ASD. Polypharmacy was also high in this cluster, but with a moderate DBI, suggesting prescriptions driven more by physical than mental disorders, which were indeed less common in this cluster. Unlike the adults of this study aged under 50 years, we did not observe two subgroups of older adults. Our fourth cluster appears to involve older adults with less severe ASD, and, in general, older adults in our cohort had significantly higher communication subscores of the VABS. Thus, it is possible that younger adults with severe ASD + ID, gut–brain axis involvement and polypharmacy (Cluster 2) may have a lower life expectancy because of their high multimorbidity and would, therefore, not be included among the older adults. In addition, Cluster 2 more frequently included individuals with mental disorders and high psychotropic polypharmacy, which are risk factors for higher mortality in autistic (Hwang et al., 2019) or ID population (Cooper et al., 2020; Schoufour et al., 2018). This hypothesis of the loss of the most severe individuals in terms of multimorbidity, dependence or ASD from the ageing ASD + ID population due to a premature death needs to be confirmed on a larger sample with a lifelong follow-up. Here, the management of polypharmacy could once more be key to increasing the healthy life expectancy of ASD + ID adults.
Our results suggest that the observed cluster specificities could be related to the clinical characteristics according to the ASD + ID subtype. We assume that Cluster 2 is likely more specific to ASD, whereas the others represent more an overlap of ASD and ID. The clinical heterogeneity of ASD is insufficiently explained by the clinical characteristics of ASD alone. Indeed, ASD is a condition that affects the entire body. Associated disorders, such as ID, as well as certain somatic or mental disorders, could be helpful in the characterization of subgroups and the prediction of developmental and ageing trajectories in ASD. Thus, our results allow the identification of subgroups according to multimorbidity in ASD + ID adults. On this basis, it is important to search for endophenotypes based on multimorbidity in ASD + ID.
Dedicated continuum of healthcare
Lower access to medical care has been reported for individuals with ID and/or ASD, which may contribute to the frequency of chronic health conditions in this population (Hussain et al., 2020; Weise et al., 2017). Among people with ID, psychiatric disorders and neurological diseases are the most common causes of care seeking from general practitioners, whereas physical health and prevention are under-represented (Weise et al., 2017). In addition, physical health conditions are a risk factor for rehospitalization among adults with ID (Axmon et al., 2019), increasing the annual cost of medical care (Vohra et al., 2017). Given the high multimorbidity and specific needs of our ASD + ID population, it is therefore essential to develop dedicated medical care for the management of their comorbidities and chronic health conditions. The differences between autistic individuals with ID and those without require different care strategies (Gilmore et al., 2021), but, nonetheless, a care strategy that public health policy must take into consideration. To incorporate the complexity of ASD into daily practice (Turcotte & Shea, 2021) and the associated multimorbidity burden, a holistic approach is likely the best adapted to follow-up autistic people, with or without ID (Coury et al., 2014; Kohane et al., 2012). In addition, ASD is a lifelong condition (Houy-Durand, 2019a; Whiteley et al., 2019), and this study shows that multimorbidity is age dependent in ASD + ID adults. Thus, as with adults with ID, those with ASD + ID require early comprehensive geriatric assessment (Cooper et al., 2015) and monitoring of both psychiatric and physical comorbidities (Dunham et al., 2018) performed by trained physicians involved in a dedicated care network that includes an integrated patient pathway.
Strengths and limitations
This study is one of the rare studies to explore multimorbidity and its associated patterns in ASD + ID adults, especially those who are older. Each participant in our sample was assessed in his residence using standardized measures by two investigators in collaboration with the participants’ daily helpers. This reduced misdiagnosis due to behavioural disorders produced by major changes in the participants’ environment, which might have occurred if we had assessed them at hospital. In addition, we performed cluster analysis using multiple methods to identify clinical subgroups in an ASD + ID population as the first step towards identifying endophenotypes (Beauchaine & Constantino, 2017).
However, our findings have to be interpreted in the light of several limitations. First, the size of our sample and that of the clusters were limited. Thus, our findings need to be validated on a larger sample to avoid a risk of over-fitting. Second, the EFAAR study follow-up is currently ongoing and collecting data about falls, hospitalizations and death, which will be useful for exploring ageing trajectories and life expectancy and their association with multimorbidity. These data also need to be confirmed by further long-term and detailed follow-up studies. Finally, our sample included only ASD + ID individuals and, thus, these findings cannot be generalized to every autistic adult without ID. We cannot draw any conclusions on whether our clusters specifically result from ASD, ID or both, because our participants have severe ASD + ID, which are difficult to disconnect. Thus, we cannot rule out the impact of the severity of ASD and/or ID on cluster identification and multimorbidity patterns. Furthermore, the absence of a control group makes it impossible to compare multimorbidity-based clusters and patterns in ASD + ID with those of the general population.
Conclusion and perspectives
The results of this exploratory study provide avenues for improving professional practices in terms of the care of ASD + ID adults, especially those who are older. First, professionals should take into consideration the management of risks related to polypharmacy and mental and neurological disorders in young adults with severe intellectual disabilities. For older adults, they could manage risk prevention and the treatment of epilepsy, kidney and cardiovascular diseases to reduce mortality (Cooper et al., 2020). They should also pay particular attention to the high risk of polypharmacy and the treatment of endocrine disorders in ASD + ID women. Overall, reducing polypharmacy is likely to prolong the healthy life expectancy of ASD + ID people.
In addition, identifying patterns of multimorbidity could facilitate the identification of underlying pathophysiological processes of pathological ageing related to, for example, alterations of the gut–brain axis and inflammageing. Considering multimorbidity provides new insights about the clinical heterogeneity of ASD + ID. Furthermore, it could be a critical aspect in identifying patient groups with specific healthcare and prevention needs.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221121623 – Supplemental material for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study
Supplemental material, sj-docx-1-aut-10.1177_13623613221121623 for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study by Stéphanie Miot, Raphaël Chancel, Marianne Peries, Sophie Crepiat, Sylvie Couderc, Eric Pernon, Marie-Christine Picot, Véronique Gonnier, Claude Jeandel, Hubert Blain and Amaria Baghdadli in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613221121623 – Supplemental material for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study
Supplemental material, sj-docx-2-aut-10.1177_13623613221121623 for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study by Stéphanie Miot, Raphaël Chancel, Marianne Peries, Sophie Crepiat, Sylvie Couderc, Eric Pernon, Marie-Christine Picot, Véronique Gonnier, Claude Jeandel, Hubert Blain and Amaria Baghdadli in Autism
Supplemental Material
sj-docx-3-aut-10.1177_13623613221121623 – Supplemental material for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study
Supplemental material, sj-docx-3-aut-10.1177_13623613221121623 for Multimorbidity patterns and subgroups among autistic adults with intellectual disability: Results from the EFAAR study by Stéphanie Miot, Raphaël Chancel, Marianne Peries, Sophie Crepiat, Sylvie Couderc, Eric Pernon, Marie-Christine Picot, Véronique Gonnier, Claude Jeandel, Hubert Blain and Amaria Baghdadli in Autism
Footnotes
Acknowledgements
The authors sincerely thank participants, their families and institutions for their participation in the EFAAR study. Special thanks to Bill for proofreading and to ERN-ITHACA for its support.
Author contributions
A.B. is the principal investigator of the EFAAR study. A.B., S.M., M.-C.P., E.P. and C.M. designed the study. S.M., S.Cr. and S.Co. collected the data. M.P., and S.M. performed the data analysis. S.M., A.B. and R.C. wrote the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics statement
Authorization for handling personal data was granted by the French Data Protection Authority (CNIL: Commission Nationale de l’Informatique et Libertés). The initial project was approved by the French Ethical Research Committee (Comité de Protection de Personnes (CPP), identification no. 2016-A00166-45) and registered in the International Clinical Trials Register (no. NCT02791321). All subjects or their legal representative gave written informed consent in accordance with the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The EFAAR study was funded by MiRE-DRESS and CNSA through the 2015 IResP grant (2016-025).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.