
Abstract
The COVID-19 pandemic prompted a large-scale move to remote delivery of healthcare services. However, little research has directly explored telehealth experiences of autistic adults, a population strongly affected by health inequalities and care access barriers. This study sought telehealth experiences of 11 autistic adults (aged 27–67 years), seven family members/carers (aged 44–75) reporting about autistic people and six service providers. In-depth qualitative interviews were conducted with all participants, which were then thematically analysed. Two over-arching themes identified were technology aids communication and access – except when it doesn’t, and in/flexibility, with a number of sub-themes. The themes, on one hand, highlighted positives of telehealth delivery, including easing some aspects of communication and decreased stress and, on the other hand, negatives, such as increased rigidity of the healthcare system, amplifying pre-existing barriers. Considering autistic people experience barriers to accessing healthcare, this study highlights such barriers could be, in some instances, addressed via remote delivery, as well as possible limitations of telehealth for some autistic adults.
Lay abstract
The COVID-19 pandemic meant that a lot of healthcare services had to move online, such as to video-calls, or to telephone. However, not many studies have looked at how autistic adults feel about this kind of service delivery. It is important to know this, as autistic people may have poorer health than non-autistic people, and they may also struggle to access services more than non-autistic people. This study asked 11 autistic adults (aged 27–67 years), seven family members/carers (aged 44–75) reporting about autistic adults and six service providers about their experiences of accessing or providing a telehealth service. These experiences were collected through interviews, which were then analysed through thematic analysis. Two main themes were: technology aids communication and access – except when it doesn’t, and in/flexibility. The themes pointed out some positive aspects of telehealth delivery, including improved communication and decreased stress. The themes also pointed out negative aspects of telehealth, such as increased rigidity of the healthcare system, amplifying pre-existing barriers. Because autistic people have many barriers to accessing healthcare, this study encourages researchers and healthcare providers to think about how such barriers could be addressed through telehealth, and about the possible limitations of telehealth for some autistic people.
The COVID-19 pandemic resulted in extensive global disruption to healthcare services and a rapid increase in the use of telehealth methods and technologies (Thomas et al., 2022; Torous & Wykes, 2020; Wong et al., 2021). Definitions of telehealth vary, but there is consensus that telehealth involves transferring medical or health information between people and groups using computers and phones to communicate via media that include e-mails, videoconferencing and audio calls (Kruse et al., 2017).
Research exploring telehealth delivery for autistic people began before the onset of the COVID-19 pandemic. One motivating factor in these efforts was to determine whether telehealth could contribute towards reducing the healthcare inequalities faced by autistic people (Croen et al., 2015). Autistic children and adults report higher rates of mental health difficulties (Cashin et al., 2018; Kinnear et al., 2020) and physical illness (Lai et al., 2019) than their non-autistic peers. In addition, autistic adults have highlighted multiple barriers when accessing healthcare, including sensory difficulties affecting appointment attendance (Mason et al., 2019), and social communication differences that may lead to misunderstandings between clinician and patient (Babb et al., 2021; Howard & Sedgewick, 2021). Some autistic adults struggle to manage the practicalities of attending appointments, due to executive functioning difficulties (Mason et al., 2019). Telehealth may prove useful in addressing some of these challenges (Alfuraydan et al., 2020; Harris et al., 2021).
Research to date suggests some success with telehealth delivery for autistic children, particularly in the areas of remote diagnosis and remote intervention delivery. For example, Dahiya et al. (2020) demonstrated some clinicians felt confident using a remote child diagnostic assessment tool, while a high degree of agreement between remote and face-to-face assessment methods was reported in a scoping review (Alfuraydan et al., 2020). Parents of autistic children have also reported satisfaction and positive outcomes of interventions delivered through telehealth (Sutherland et al., 2018). However, a systematic review of remote delivery of behavioural interventions for children suggested that the quality of evidence for telehealth interventions is still low (Ferguson et al., 2019). There is limited research into the impact of telehealth service delivery for autistic adults, and very few studies include the perspectives of autistic people themselves.
In addition, telehealth may improve delivering care to people in remote areas and areas without specialist services, as well as reducing costs for patients (Burke et al., 2015). Reducing costs may be of particular importance for the autistic population, who face higher levels of unemployment (Knapp et al., 2009; Mavranezouli et al., 2014), with only 21.7% of autistic adults employed (Office for National Statistics, 2021) and high proportions being homeless (Churchard et al., 2019; Stone, 2018). Yet, it remains possible that some barriers experienced in face-to-face services may sometimes be exacerbated rather than ameliorated when delivered using telehealth methods, including increased social communication difficulties (Bundy et al., 2021; White et al., 2021); processing ability; and sensory sensitivities negatively affected, for example, due to background noise in video-calls, and other environmental distractions (Harris et al., 2021; Pellicano et al., 2022). Despite the importance of this area for service providers, and emerging research with children, there has been little research investigating remote delivery of physical and mental health services for autistic adults in the United Kingdom.
Given these gaps in the research literature and the unique opportunity afforded by the COVID-19-triggered shift to widespread adoption of telehealth methods, the present study aimed to describe the telehealth experiences of UK-based autistic adults. The perspectives of autistic adults, family members or carers of autistic adults and those providing services to autistic people were sought. Through in-depth interviews, we sought to establish perspectives on (1) the nature of the shift to telehealth during the COVID-19 pandemic and (2) the barriers and facilitators to accessing and receiving support via telehealth.
Methods
Procedures
Autistic adults, close family members or carers of autistic adults and service providers working with autistic people, were all invited to take part in in-depth interviews. Service providers were also invited via researchers’ own personal networks. Due to the pandemic restrictions, all interviews were conducted remotely, via e-mail, Zoom chat, telephone or videoconferencing. All interviews were conducted in a 4-week period in early 2021, during the COVID-19 pandemic. Ethical approval was obtained from the UCL Research Ethics committee (reference number: 7475.005).
Participants
Participants were 11 autistic adults (aged 26–67 years); seven family members or carers (aged 44–75 years) reporting about autistic adults; and six healthcare professionals or service providers. When quoting participants, we have used the code ‘AUT’ for autistic participants, ‘FAM’ for family members or carers and ‘CLIN’ for all service providers. See Tables 1 and 2 for reported participant information. To be eligible, all participants were over 18 years old, and able to answer questions in English, through speech or writing. Autistic participants reported to be all formally diagnosed and accessing telehealth service since the beginning of the pandemic. Family members or carers had to have a close relationship with the autistic person (e.g. parents or siblings) and had to be supporting the autistic person in their day-to-day life during the pandemic. Service providers had to be working with autistic people since the beginning of COVID-19.
Demographic characteristics of participants.
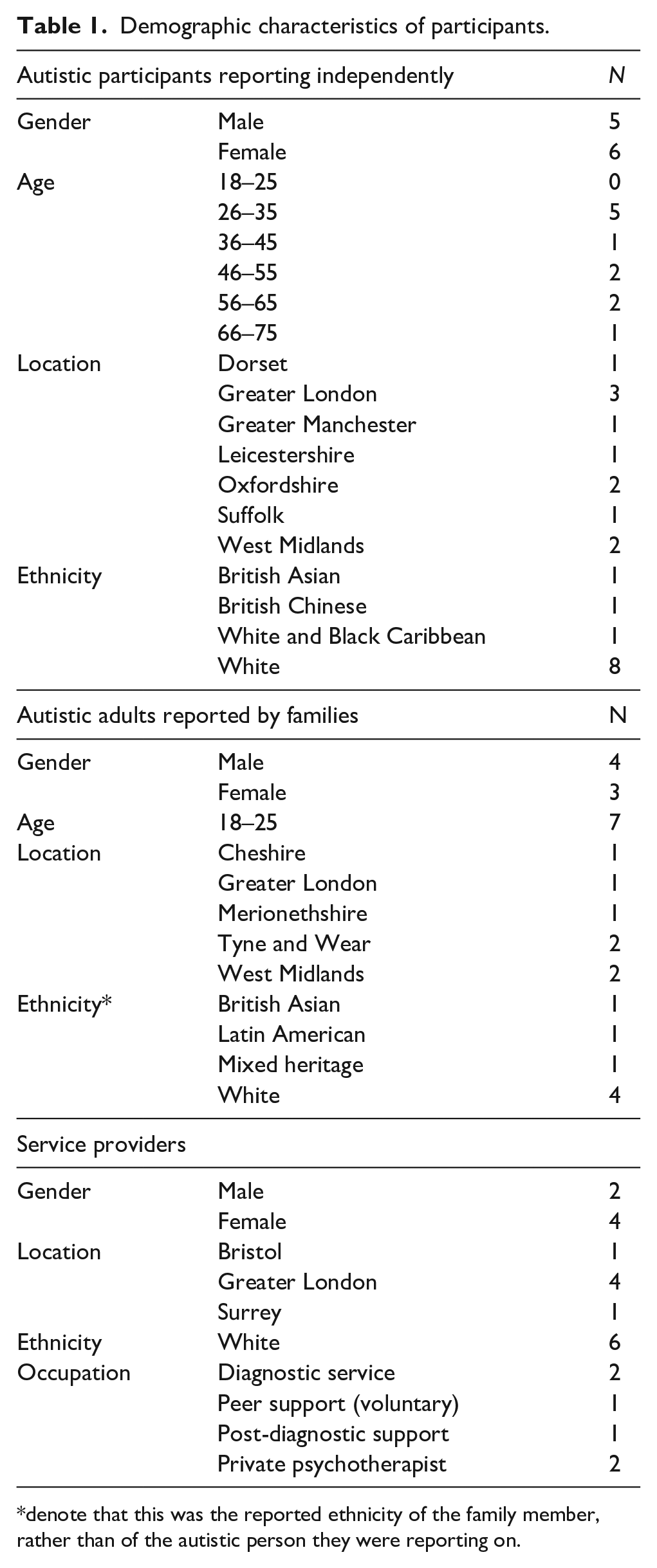
denote that this was the reported ethnicity of the family member, rather than of the autistic person they were reporting on.
Number of participants reporting medical diagnoses.
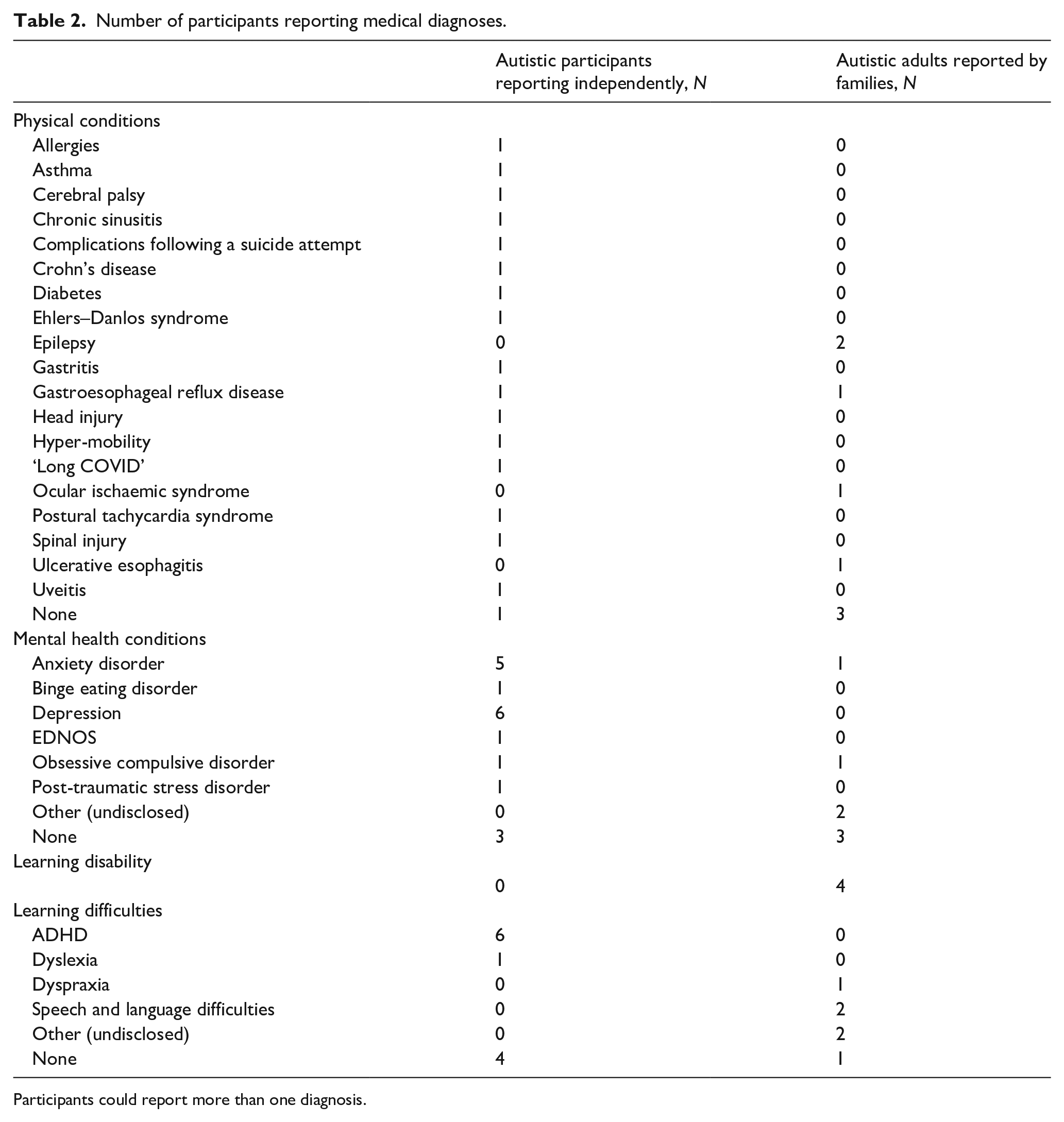
Participants could report more than one diagnosis.
A study advertisement was sent by e-mail to members of the Autistica Network and prospective participants expressed interest in participating to the researchers. There was some overlap between categories: one parent was also autistic; one autistic person was also a clinician and one parent was a healthcare practitioner. In these cases, the participants’ overlapping experiences were included, and the participant was grouped in all the categories in which they felt they belonged.
Materials
See supplementary materials, Figures 1–3, for the complete interview schedule. Interview questions were informed by a literature review of telehealth delivery with autistic adults. Demographic questions were asked at the beginning of the interview. These focussed on participants’ gender, age and ethnicity (for autistic participants and reporting family members – family members disclosed information about the autistic person, as they felt comfortable), and type of services accessed or delivered now and in the past. The interview covered the following topics: (1) change to professional services received since the beginning of the pandemic; (2) accessing new services since the start of the pandemic; (3) information given about a telehealth service accessed; (4) struggles surrounding accessing/receiving a telehealth service; (5) positive aspects about accessing/receiving a telehealth service; (6) telehealth and own communication; (7) telehealth and communication of service providers; (8) improving unhelpful aspects of telehealth; (9) keeping helpful aspects of telehealth and (10) additional thoughts. The way in which these topics were discussed was adapted appropriately for family members and providers. At the end of the interview, participants were asked how they found the questions, and if there was anything else they thought was important to ask other people about telehealth. The interviews were dynamically refined throughout the interview process, incorporating participant feedback (McGrath et al., 2019).
Data analysis
The data were thematically analysed, according to Braun and Clarke (2006, 2021) by DA. Thematic analysis was chosen for its flexibility and ability to capture in-depth patterns in the data (Nowell et al., 2017). Coding was conducted on the entirety of the interview transcripts, in Microsoft Word. Analysis was a dynamic and inductive (i.e. data-driven) process, with themes identified at the primarily semantic (i.e. explicit), as opposed to the latent (i.e. interpretative) level. To establish trustworthiness (Nowell et al., 2017), DA made notes during and after the interviews, with impressions and thoughts about emerging codes and themes. Notes were made also throughout the coding process. Emerging themes were discussed throughout the analytical process with all members of the research team to mitigate existing biases, encourage reflexivity and to make sure the themes were consistent with the data (Darawsheh, 2014; McNair et al., 2008; Probst, 2015).
Community involvement and positionality
The research team included autistic and non-autistic researchers, all of whom view autism through a biopsychosocial lens, considering the important interaction between a person and their environment. As a team, we believed in the importance of taking positionality and reflexivity seriously. Throughout every point of our process, we reflected on, and where appropriate discussed and made sensible changes, on how our backgrounds and experiences shaped our interpretations, and conclusions.
Results
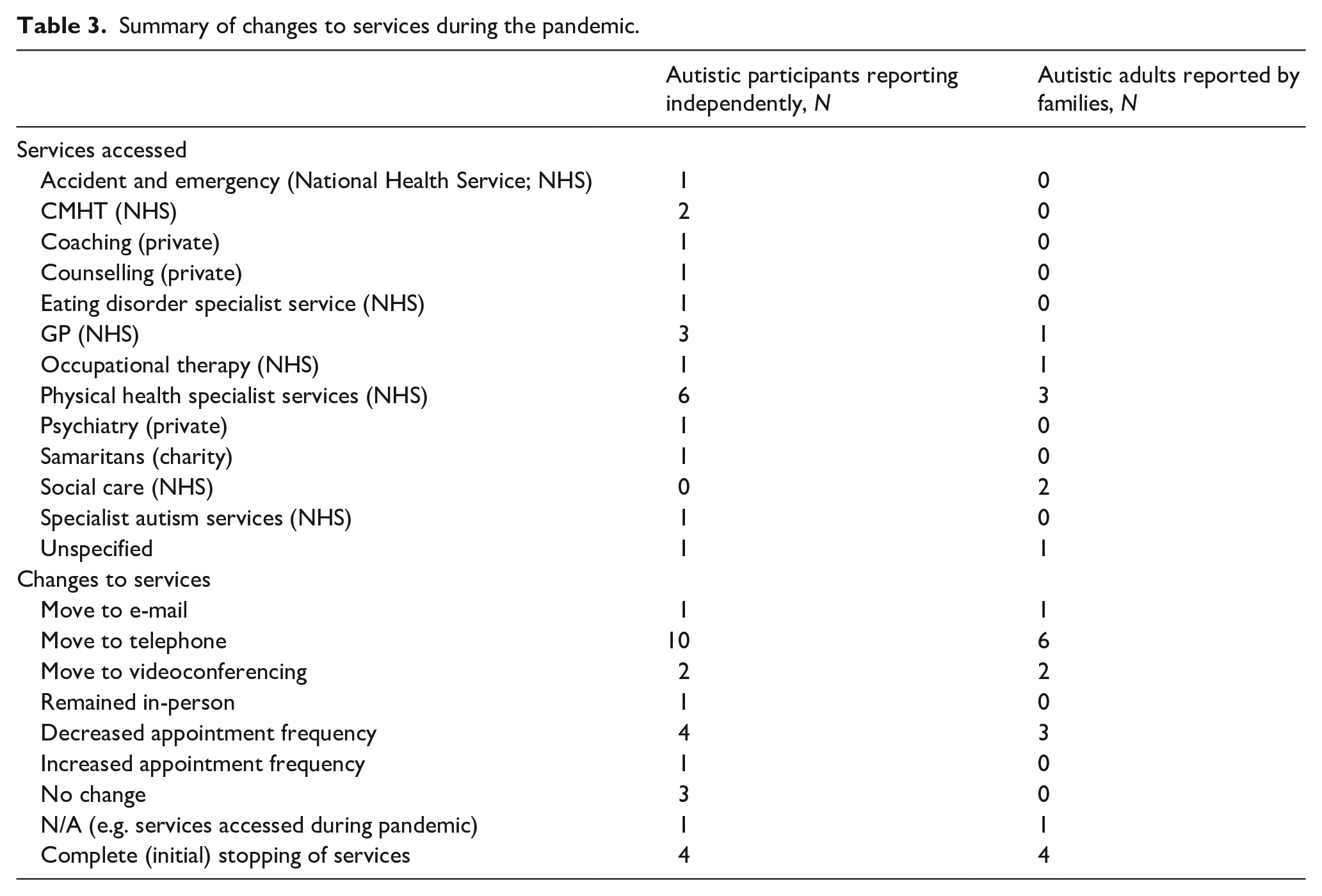
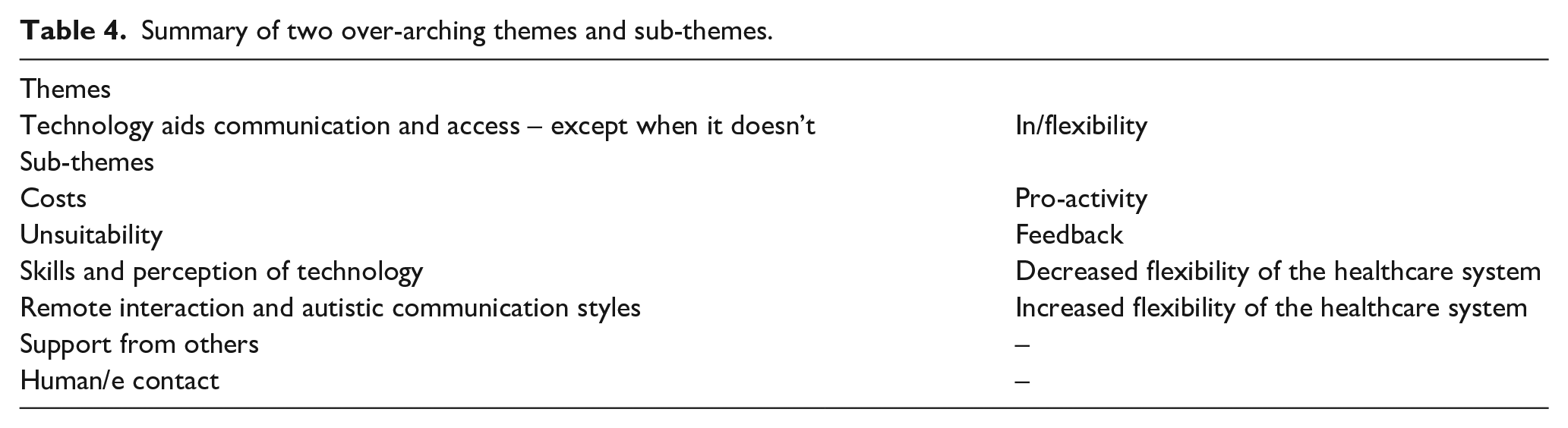
See Table 3 for types of services accessed. The experiences of all three participant groups were organised into two over-arching themes: technology aids communication and access – except when it doesn’t; and in/flexibility. These were organised into further sub-themes. See Table 4 for the overview of the themes and sub-themes.
Summary of changes to services during the pandemic.
Summary of two over-arching themes and sub-themes.
Technology aids communication and access – except when it doesn’t
This theme captures positive and negative factors that participants experienced linked to technology, when accessing a remote service. It focuses primarily on individual-level interactions and captures the two-way relationship between technology and communication/access.
Costs
A few participants, particularly service providers, indicated that some groups of autistic people may be partially or completely cut off from accessing services delivered via telehealth due to digital poverty, a term covering situations where people cannot afford mobile or broadband data to meet their needs. Hence, there is a complete cut-off in communication. This was primarily expressed by service providers, perhaps because our study, conducted remotely, selected for patients who did have access to a telephone, a computer and/or the Internet. Providers attributed this to lacking sufficient hardware or reliable Internet connections:
First of all access to computers for some people – there is such thing as ‘digital poverty’ – some people might not have laptops. But, luckily, a lot of people did. Some didn’t. And it was really interesting because it opened it up to people who’ve never came to our service. And then people who have been in our service for a long time didn’t. (CLIN006)
However, some participants indicated that accessing their appointments via telehealth technologies meant they could save money, for example, by not having to pay for parking or train tickets, or not having to take time off work, as they were able to fit their appointments more flexibly into their working day. This also served to reduce stress, as one autistic participant explained:
I’m very much in the freelance industry, and so, me taking time off means I lose money, which is obviously going to be a source of anxiety anyway. But also, it just means that logistics – for me, if I was at work and I needed an appointment, I wouldn’t have my car and then I’d have to sort out or change my routine, and, as an autistic person, it’s a huge change to my routine that I don’t like, I don’t want to deal with. It kind of removes that stress. (AUT008)
Unsuitability
Autistic participants, family members and providers agreed there were some services and situations where in-person contact was more appropriate than telehealth. Several participants thought that for highly distressed people, such as those experiencing suicidal thoughts, in-person contact was essential, as one clinician put it, ‘Just the idea that someone’s talking about having suicidal thoughts and then the whole connection drops- It really needs to be very reliable, because otherwise you’re just left hanging there, thinking: “What on earth is going on?”’ (CLIN001).
This linked to other mental distress-related emergencies, such as self-injury, as an autistic participant described: ‘Where there’s things like self-harm involved – I think somebody needs to see it, you can’t describe it’ (AUT008).
Indeed, remote communication had the potential to make judging and communicating distress harder. Although anxiety was reduced for some participants if they did not have to come into the clinic, possibly leading to better communication, some participants felt that telehealth made identification of true levels of need more difficult, as compared to in-person interactions:
It caused less anxiety because you’re in your own home and you can just relax, without all the environments being so chaotic and it being in a new place. But then, sometimes, it’s hard because they don’t really see the true you. Because you kind of zone into your space. When you’re in person, they actually see the true you. (AUT002)
This was relevant to both therapeutic and diagnostic services. Within the latter, service providers mentioned reduced ability to observe behaviours perceived as helpful for the diagnostic process: ‘We lost a lot of information, and we just had no sense of what it felt like to be with that person in the room’ (CLIN003). However, upsides were also acknowledged, such as finding home environments a novel part of the assessment: ‘Some people’s bedrooms were really revealing, but that was relatively rare’ (CLIN003).
The fragility of the interaction over telehealth was a prominent concern. For some participants, there was a sustained background awareness the clinical interaction could cut off at any point. Both the potential and the reality of this increased distress, illustrated by an autistic participant: ‘If there’s a critical point, you can’t respond back via telephone. You’re cut off, and you can’t phone them back because they literally cut you off’ (AUT003).
Linked to medical emergencies was the unsuitability of telehealth for some aspects of physical healthcare. Several participants suggested that primary care appointments crucially required in-person care for autistic people because, for example, general practitioners (GPs) were able to visually gage difficulties the patients themselves may not have been aware of, which could be more difficult, if not impossible, via telehealth.
Several family members highlighted that the people they supported who had additional needs, such as an intellectual disability, were entirely unable to access any form of remote communication. Therefore, this form of service delivery was inappropriate for the autistic person’s access needs:
I know that my sister would not be able to communicate her needs fully so this type of service is not really a viable option . . . My sister always finds it hard to communicate her needs in a comprehensive manner and can talk around subjects she does not want discuss, such as pain. (FAM005)
Finally, delivery via digital technology was thought to be sometimes inappropriate for cultural, religious or social reasons, pointed out by a clinician: ‘There are cultural barriers to the use of technology. We have a very large [Orthodox] Jewish community in the borough, and they don’t use any technology at all, so obviously they can’t engage on that kind of platform’ (CLIN004).
Skills and perception of technology
Some participants were apprehensive accessing or delivering services via telehealth. Some autistic participants highlighted unease with accessing unfamiliar platforms, facing too many unknown steps, and needing support to do this. One family member described this:
The fact that he knows that it’s not just a case of phoning up and making an appointment, it’s the case of phoning up to make an appointment and then having another phone-call. There have been times when he hasn’t felt great, but he’s just gone, ‘I’ll be fine’. And I know it’s because of having that thought of having another telephone conversation. It’s just put him off. (FAM004)
Healthcare professionals were also reported to struggle with aspects of technology. This acted as a barrier to contact with the patient, as the focus ended up being on getting technology to work, rather than on developing rapport via a different method:
The person [i.e., clinician] who I was trying to speak to wasn’t very tech savvy and couldn’t get the meeting to work . . . They seemed to fiddle around, trying to sort it out and their focus was very much on the technology, rather than the problem. (AUT010)
Service providers sometimes felt they/their colleagues held negative assumptions about what delivering services via telehealth to autistic people would be like:
We had assumptions. So, we kind of thought: how are we going to do this?! You know when the pandemic started. How is this going to happen? . . . But it was actually so much better than we thought. (CLIN006)
Others pointed out physical contact and being able to see visual cues was vitally missing and that this reduced the quality of the interaction between client and clinician, as one private psychotherapist described:
Actually they miss being in front of me. And I think there’s something, I don’t think we have a word for it in our language, but there’s something about being together in a space, where we co-create, that doesn’t happen online. (CLIN001).
Autistic participants also highlighted concerns around privacy, online security and data protection. One participant pointed out that they were unable to engage in video-calls, having to choose telephone contact instead, because they lived with their parents and had no privacy inside the house. A few participants were concerned how their data would be used, concerned that they could be filmed or very sensitive data shared with others: ‘Imagine breaking down and crying to a therapist via Zoom. I would have to end that call, rather than be filmed in distress’ (AUT009).
Remote interaction and autistic communication styles
Several elements reported by participants, related specifically to communication as autistic individuals. For some autistic participants, the loss of visual social cues was reported as a negative development, making communication more difficult, as one participant described: ‘Socially, I can use some visual cues, and the phone takes that away’ (AUT001). Another participant commented, ‘It comes down to audio processing disorder. My memory around speech is near zero. I usually lip read’ (AUT003). Yet others found the loss of visual cues via telephone a positive, such as not having to cope with eye contact, and, as one participant described, ‘I never think I look appropriate for how they want me to look. At least on the phone I don’t have the ‘Oh my God, I don’t look like I’m in enough pain . . .’. At least it’s just about how I sound’ (AUT007).
This links to many autistic participants indicating a continual concern and self-consciousness of their behaviours and speech, in terms of being misperceived or misunderstood in telehealth interactions. Some worried about stronger emotions being misperceived as aggression, and there was an overall sense of mistrust and fear of services and clinicians. One of the participants compared this mistrust to that experienced by LGBTQ + people within the healthcare system in the recent past:
There is a fear of doctors because doctors are trouble. . . .Because they’ll often have declared you to be bad, or you’ve got a problem or whatever. It’s not unlike – I mean, I am gay – it’s not unlike the way it used to be, I think, for gay people and doctors. It was like: don’t go near doctors. Because you can’t trust them. (AUT011)
Support from others
Prior to the pandemic, some autistic people, through self-report and family member report, relied on formal and informal support from family members, social workers, friends and partners, to access or prepare for appointments. For some, parents were fully in charge of the autistic person’s communication, for example, due to the person’s intellectual disability. Others gave consent for a parent to be in charge. Rehearsing what one would say in an appointment and finding the presence of a loved one reassuring were other reasons mentioned. For some of the participants, this need for support heightened over telehealth delivery, with one autistic person completely disengaging:
It put up more of a barrier between [participant’s son] and the healthcare provision. So, because I was the one that did all of that, and he just completely backed out of it, he didn’t even want to be co-consulting or anything, it was just me doing it. (FAM002)
Others found it more difficult to provide this support while aware it was much needed, as one parent described: ‘I’m with him when the conversation takes place, and, therefore, I can prompt him, and I can open up different parts in the conversation. But you can’t do that over the phone’ (FAM003).
Yet, others became sole communicators for their autistic family members, with services relying on their reports, in terms of both symptoms and situations, such as formal safeguarding assessments. This left some family members feeling concerned about the responsibility they had: ‘The responsibility was huge in terms of [communicating daughter’s needs to the doctor]. And, for me, English is a second language as well. Describing things accurately, the fear of making a mistake . . .’ (FAM001).
Human(e) contact
Across the board, autistic participants and family members supporting autistic adults, emphasised the value of human(e) contact. This involved two main elements. First, a few participants highlighted that remote delivery reduced the personal and reassuring aspects of support and made them feel less able to share themselves: ‘I am getting used to it, but it does lose a bit of the informality. It is more difficult to talk about some things’ (AUT004).
Second, kindness, patience and willingness to learn were highly valued when encountered, and, for some participants, these ways of engaging and behaving were what made telehealth delivery either effective or ineffective, as one autistic person highlighted:
I think what it really comes down to is the kindness and patience and empathy shown by individual staff members, whether they are medical, or administrative. Allowing people to feel comfortable, so they can say things, maybe they never said to anybody. . . But that’s more of a cultural attitude thing, rather than something you can just put into place. (AUT007)
This was supported by a carer of an autistic person:
If you’re going to do remote calling, you need to establish empathy . . . If you’ve got people who are in any way authoritarian or have some kind of inspector mode to their personality, there is no way they can work with anybody who’s autistic. The key to this is not so much the technology. It’s the individual who is using the technology, in my view. (FAM006)
In/flexibility
This theme reflects how technology and, in turn, its impact on communication, affected existing healthcare systems, positively and negatively. This theme is more focussed on systemic-level impacts.
Pro-activity
Most autistic participants and family members indicated that to access or engage with any telehealth-delivered service, autistic people and in applicable circumstances their families, had to be proactive in their communication, pointed out by one family member, ‘. . . the well-being of autistic young people very much depended on the strength of advocacy of their carers. There was very little proactive checking-in by services’ (FAM001). This included calling services multiple times; inquiring about test results; and, during interactions, actively offering up information as clinicians did not ask questions that would elucidate these answers.
Across participant groups, this need to be proactive was seen as a significant barrier to healthcare and support. Reasons for this included being already in high distress or highly anxious and finding it difficult to self-advocate for one’s needs; not knowing what was required to obtain a service; and autistic communication differences:
I think one of the things that struck me is that is that it requires a certain element of pro-activity to actually get involved with services. If he’d been more proactive maybe he would have rung up the social worker and said, actually what support can I get? You know, that’s not on his radar. (FAM003).
Feedback
The quality of communication between clients and services was frequently cited as important. It was highlighted that it was essential to elicit, listen to, and attempt to implement autistic people and family members’ feedback in service design and delivery, as urged by one family member:
I think the services themselves could or would be wise to seek feedback from the users; we’re never asked or rarely asked ‘how was the service for you?’ So, both at the point of setting up any form of consultation/communication, if there is a possibility, they could ask what the best way for everybody would be, including for them. (FAM001)
In relation to this, one service provider described the value of peer mentors:
We’ve got peer mentors, so people who are autistic and they facilitate groups with us, together. And they’re amazing. Their feedback is really important to us. (CLIN006)
Decreased flexibility of the healthcare system
The use of telehealth saw an exacerbation of barriers that were already present in the system. Some participants highlighted that the already over-burdened system increased in its rigidity, and fracture. Given most autistic participants had multiple health conditions, they reported there was lack of communication between the various services they were accessing, as pointed out by one autistic person: ‘The professionals, they don’t communicate with each other, either by letter or phone call. It’s not happening and, since COVID, it’s just gone off a cliff’ (AUT003).
The health system was also perceived as goal-oriented, and rigid, rather than holistic. This linked to the criticism by some autistic people and family members, that the services felt automated and impersonal: ‘It’s focused on specific tasks, and it doesn’t give an overview of the whole person. It’s very focused on one particular problem. Most people have got multiple problems’ (AUT010).
Some autistic people and parents also felt unable to voice their preferences and concerns, as there was a perception that either there was no time for this, or that it would be perceived negatively, as non-compliance:
I just get the sense that it would be a problem. It would be trouble . . . You know, we don’t run the [general practice] for your convenience, basically. We run it for the doctor’s convenience. So, there was kind of a sense that asserting a need to see a doctor at a particular time was not something you could do. (AUT011)
Increased flexibility of the healthcare system
Although there were some exacerbations of pre-existing issues, some elements of telehealth digital delivery were seen in a positive light. This included well-run online (booking) systems, which increased flexibility of access, allowing patients to manage their appointments, test results and medical documents, and being able to communicate via writing, such as by e-mail. Considering many autistic participants struggled with telephone contact, for some, this addressed the difficulty.
In addition, the increased use and acceptance of online digital communication aspects, such as the sharing and creating photographs, videos, recordings and applications (e.g. for measuring blood pressure), made some participants feel they could communicate more flexibly, effectively and accurately, than just by verbal language alone. An autistic participant, for example, explained: ‘I was asked about my blood sugar readings. I have an app which makes a spreadsheet, so I just e-mail it to my specialist nurse. This is more precise than just saying if they are good or bad’ (AUT001).
Discussion
This study investigated the use of telehealth in the UK services during the COVID-19 pandemic, as reported by autistic participants, family members or carers of autistic adults, and service providers working with autistic populations. Two key interconnected themes, with positive and negative features for the delivery of services, were identified: technology aids communication and access – except when it doesn’t, and in/flexibility. The factors are discussed in relation to existing literature, and future questions for research, policy and practice.
Participants pointed out access via digital technology had both cost advantages (e.g. not having to pay for travel) and disadvantages (e.g. lacking access to reliable technology). This is consistent with research highlighting, on one hand, cost-effectiveness of geographically wide-reaching implementation of telehealth (Alfuraydan et al., 2020; Baweja et al., 2022; Little et al., 2018) and, on the other hand, the impact on communities without reliable access to technologies and broadband to benefit from these innovations (Ramirez et al., 2021; Valdez et al., 2020). Given that autism-related studies evaluating telehealth interventions often provide equipment or exclude those that do not have the technology (Baweja et al., 2022), it is difficult to gauge the extent of digital poverty within autistic communities. However, in the United States, the disabled community, as compared to the general population, has lower access to broadband and technologies that allow telehealth use (Anderson & Perrin, 2017).
Future studies should ask questions about digital access overtly, and/or document the participants that are supported in taking part. In terms of policy and practice, services could explore resources and providing equipment. For example, not having enough data or a fast-enough connection on a mobile plan can be solved by conducting sessions via phone. If video is needed, clients could be provided with a SIM card with data; being posted a tablet with a SIM card or by making it possible for them to have access to a private room with a stable Internet connection in their own community (e.g. community health centre).
Telehealth was considered to be inappropriate for high distress, physical examinations, and for some people with intellectual disabilities. To the authors’ knowledge, little research exists on how high distress, self-injury and suicidality are impacted by remote delivery in autistic populations. Only one study to date has explored self-injury, in the context of a remote behavioural intervention in three autistic adults, citing reduction in self-injurious behaviours (Singh et al., 2021). Given the diverse responses to telehealth by different autistic individuals, for example, increased communication difficulties for some, while improved communication for others, it may be speculated some highly distressed autistic people will be better supported remotely, whereas others in-person. It is therefore a priority for future studies to ask nuanced questions, and to determine how workable decisions can best be made in practice. Likewise, considering the high rates of physical health conditions in the autistic population, communication differences, and, for some, alexithymia (Oakley et al., 2020), questions related to assessing physical wellbeing via telehealth need to be urgently asked. Arguably, telehealth may be valuable for initial triaging with more specialist support conducted in-person. However, it is unclear how this triaging can be done in a helpful and accurate way that leads to satisfactory investigation of the issues experienced.
Finally, in terms of telehealth delivery and intellectual disability, little research explores this area. Studies concerning those who have an intellectual disability are mostly behavioural, suggesting valued outcomes (e.g. Pellegrino & Reed, 2020). Rothman (2021) described a dance therapy intervention, with an autistic client that had an intellectual disability and Down syndrome, judged to have been meaningful, despite several telehealth-related challenges, each of which was worked through between the client and therapist. Though valuable, there are limitations to experimental, behavioural, and case studies, including low participant numbers, and more general ethical concerns (Bottema-Beutel & Crowley, 2021). It is imperative to explore telehealth within different service types, and autistic people with a range of support needs to understand the benefits and consequences.
Autistic participants and healthcare providers held pre-conceptions about telehealth in the context of autism, and competencies in remote access and delivery were varying. Both client and clinician technology literacy play a role in a satisfying outcome, and absence of these competencies from either side may be a barrier (Malliaras et al., 2021; Triana et al., 2020). Several organisations, including the British Psychological Society (BPS)( 2020), the British Association for Counselling and Psychotherapy (BACP) (2019) and the British Medical Association (BMA) (2021) created competency frameworks and advice guidelines for remote service provision, including advice surrounding technology, privacy and confidentiality. Therefore, a provider lacking technical skills or confidence can improve these via training and support. If the client feels they lack these skills or confidence, increased flexibility from the healthcare professional, who is, for example, equally happy to use Zoom, Teams or another platform, could partially address the difficulty.
In addition, autistic participants felt distrustful of healthcare providers and services, including uncertainty around privacy while using telehealth. It may be that the existing atmosphere of distress attached to services, combined with the discussed barriers faced when accessing telehealth, exasperate pre-existing distrust, which should be explored further. It is important for practitioners to be aware of the distrust many autistic people may generally have towards accessing care, considering trust is a key elements of meaningful clinical relationships (Gilburt et al., 2008; S. D. Pearson & Raeke, 2000; Rowe & Calnan, 2006). The highlighted issue of privacy and Internet security has been discussed by others, for instance, Spain et al. (2021) mention clinicians’ anxiety over losing control of their clients’ privacy. Future solutions and guidelines for data security have been proposed (e.g. Shachar et al., 2020). As highlighted by some participants, future studies should ask how frequent anxiety about online privacy is. Services should understand this concern as a barrier, and provide helpful information, such as how online privacy and security is ensured within their practice – and what the limitations to it are. It should not be taken for granted that this information is known, or not valuable.
The consequences of telehealth for the interpretation of observable behaviour are an open question for future studies. It was suggested by participants that communication could improve within remote appointments: if a person feels comfortable within their home environment, they may behave in a more relaxed way (Mason, 2021). However, if a person is in a safe, non-stressful environment, the healthcare provider cannot observe how the autistic person copes more challenging contexts, making it difficult to behaviourally gage every-day distress, as discussed by Adamou et al. (2021). This may be likewise relevant to diagnostic assessments, mental health services and physical health appointments, albeit for different reasons. Within practice, asking key questions, and having trust in the client’s communication of internal experiences even if they may not be observably or ‘typically’ upset or in pain, may be most helpful. Clear communication and the clinician’s curiosity in the patient’s experience, could also alleviate some autistic people’s worries about being misperceived and misunderstood.
The removal of non-verbal social cues in some remote methods was an impediment to communication for some but made communication easier to navigate for others. Bundy et al. (2021) further highlighted some participants perceived videoconferencing as heightening reliance on non-verbal communication, increasing distress. These different perceptions highlight the need to hold the autistic population with nuance. The introduction of non-verbal tools, such as the sharing of photographs, images and digital applications, such as for graphs, had a positive impact for several participants, as it allowed autistic people to communicate their needs with more precision than by language alone. In addition, some participants welcomed the increased use of e-mail, finding it easier to communicate in a written format than via speech. This is consistent with Howard and Sedgewick’s (2021) participants who found telephone contact particularly difficult. Considering its potential usefulness, healthcare providers could explore balancing the clients’ needs with the resources of the service in seeing how such tools can be incorporated as useful aids.
Most of the autistic participants and family members pointed out getting involved with a healthcare service required a high level of pro-activity and flexibility. The discussed issues – including distrust of services, higher likelihood of complex interactions of physical and mental health (increasing exhaustion, stress and burnout), and communication differences – are likely contributors to some autistic people being more strongly affected by the need for pro-activity and the struggle to attain it. In current practice, it may be useful for services to attach a ‘reach out’ note to autistic people’s records, making clinicians aware of this barrier. Furthermore, this point did not seem to be relevant to only telehealth interaction, but also accessing healthcare in general. In terms of future research, it is important to continue exploring what different autistic populations feel they need from various services, for them to be accessible. Indeed, the importance of actively seeking feedback from clients was highlighted.
Furthermore, participants pointed out that they often relied on the support of family members, friends, and partners, when accessing healthcare services. Some studies have highlighted that autistic participants rely on practicing general conversations (Miller et al., 2021), as well as the extensive role of family support in life management (Papadopoulos et al., 2019). The importance of involving and accommodating families, and other intimate acquaintances, is crucial. As one family member noted, although they were anxious about the increased medical responsibility because of the move to telehealth, they welcomed being more involved in their daughter’s epilepsy care.
Important characteristics mentioned by the autistic participants and family members were the professional and personal qualities of the healthcare staff. These included kindness, compassion, patience and willingness to listen and learn. These open and respectful attitudes were, by some participants, cited as being the most crucial elements in delivery of a service, whether remote or in-person. This is consistent with a recent qualitative study, where autistic adults judged clinicians’ patience and willingness to listen as deeply valued (Mason et al., 2021). From the general patterns within the interviews, it could be argued that a lack of these attributes was felt strongly in remote communication, perhaps due to the fragility of the connection, and possible technological issues requiring the management and balancing of a great amount of emotional and practical elements. Some clinicians feel uncomfortable or unsupported working with autistic populations (Corden et al., 2021; Maddox et al., 2020; Unigwe et al., 2017), while healthcare environments have historically been fast-paced and under-resourced. The transition to telehealth may have exacerbated these issues (Spain et al., 2021), meaning important professional and personal qualities may become strained or lost on an individual level. It is therefore paramount to continue addressing these systemic issues, as well as understanding how they (will) impact on telehealth delivery. In addition, in current practice and clinical training, it is important to continue overtly highlighting that the positive impacts of humanity in healthcare, particularly for people with long-term difficulties and poor service experiences, cannot be underestimated.
This study included a variety of services, and patterns across provisions were described. One limitation is that we did not separately compare responses related to physical health, mental health, or diagnostic services, although all three were referred to by participants. Some aspects of autistic people’s experiences with telehealth may be particularly relevant to one type of service, and this should be explored in greater detail in future research. In particular, autistic people’s engagement with mental health services should be specifically explored, for example, to examine the impact on the therapeutic relationship and engagement. Further, some of the comments made by participants were not necessarily specific to experiences of telehealth (rather, healthcare systems, or care, in general), nor solely to autistic adults (rather, to the broader population as a whole). Although this may, on one hand, be a limitation given the focus of the study, on the other hand, it may point towards at least two lessons: that telehealth and in-person contact share some overlapping characteristics of helpfulness/unhelpfulness, and that what works for autistic adults has a much broader application. As such, we included themes which may not be unique to autistic people or telehealth, as these may be the most relevant to services seeking to improve their practice more generally. However, future research would benefit from exploring characteristics that specifically impact autistic people, especially in the context of autism-specific services, such as diagnosis.
Finally, only participants who had adequate technologies could access the interviews; including the views of those who cannot use telehealth at all would partially address the recruitment bias in this study. The present study excluded the perspectives of autistic children and/or young people, therefore, future research would benefit from including a broader range of autistic people from across the lifespan and with varying levels of additional need.
Following the rapid move to remote service provision, this project conducted in-depth interviews with autistic adults, families/carers of autistic individuals and service providers working with autistic populations, based in the United Kingdom, to explore this transition, and to identify patterns and impacts on autistic communities. Barriers and facilitators to healthcare were identified. These included both positives and negative impacts of two interconnected factors. Future studies should look to recruit larger participant numbers and focus on specific services, particularly those providing mental healthcare to autistic people, whether specialist or general. Autistic communities and their wider support networks should be engaged to form and/or discuss the most relevant questions that should be addressed around telehealth. Importantly, rather than creating a prescriptive approach, this research instead points to and should inform person-centred choices.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221108010 – Supplemental material for ‘The key to this is not so much the technology. It’s the individual who is using the technology’: Perspectives on telehealth delivery for autistic adults during the COVID-19 pandemic
Supplemental material, sj-docx-1-aut-10.1177_13623613221108010 for ‘The key to this is not so much the technology. It’s the individual who is using the technology’: Perspectives on telehealth delivery for autistic adults during the COVID-19 pandemic by Dorota Ali, Sarah O’Brien, Laura Hull, Lorcan Kenny and Will Mandy in Autism
Footnotes
Author contributions
The study was co-designed by all the authors. DA ran and transcribed the interviews, performed initial analyses, and wrote the first draft of the paper. All authors reviewed and contributed to the editing of the later versions of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research presented in this paper was funded by Autistica (grant ID: 7281). The views expressed are those of the author(s) and not necessarily those of Autistica. They would like to thank members of the Autistica Network who took part in this research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.