
Abstract
Little is known about the extent to which the healthcare needs of autistic older adults with intellectual disability differ from autistic older adults without intellectual disability. We conducted a cross-sectional retrospective cohort study of Medicare claims data from 2016 to 2017 to compare the prevalence of physical and mental health conditions among autistic older adults (age 65+ years) with intellectual disability (N = 2054) to autistic older adults without intellectual disability (N = 2631). Medicare claims data consisted of records from inpatient hospitalizations and institutional outpatient visits (i.e. visits to hospital outpatient departments, rural health clinics, renal dialysis facilities, outpatient rehabilitation facilities, Federally Qualified Health Centers, and community mental health centers). Examination of the largest between-group differences revealed that autistic older adults with intellectual disability had 350% greater odds of epilepsy (odds ratio = 4.5, 95% confidence interval = 3.9–5.2), 170% greater odds of osteoporosis (odds ratio = 2.7, 95% confidence interval = 2.3–3.2), and 100% greater odds of gastrointestinal conditions (odds ratio = 2.0, 95% confidence interval = 1.8–2.2) but 80% lower odds of attention deficit disorders (odds ratio = 0.2, 95% confidence interval = 0.1–0.3), 70% lower odds of substance use disorders (odds ratio = 0.3, 95% confidence interval = 0.2–0.4), and 60% lower odds of suicidal ideation or intentional self-injury (odds ratio = 0.4, 95% confidence interval = 0.3–0.6). These findings highlight the importance of developing tailored health management strategies for the autistic older adult population as a function of intellectual disability status.
Lay abstract
Little is known about the extent to which the healthcare needs of autistic older adults with intellectual disability differ from autistic older adults without intellectual disability. Our study is the first, to our knowledge, to use US national data to compare physical and mental health conditions among autistic older adults with and without intellectual disability. The data analyzed in this study consisted of records from inpatient hospitalizations as well as “institutional outpatient” healthcare visits, which include visits to hospital outpatient departments, rural health clinics, renal dialysis facilities, outpatient rehabilitation facilities, Federally Qualified Health Centers, and community mental health centers. Autistic older adults with intellectual disability were significantly more likely to have thyroid disorders, epilepsy, respiratory infections, gastrointestinal conditions, osteoporosis, cognitive disorders, and schizophrenia/psychotic disorders. In contrast, autistic older adults without intellectual disability were significantly more likely to have obesity, diabetes, high blood pressure, cerebrovascular disease, chronic obstructive pulmonary disease, arthritis, back conditions, attention deficit disorders, substance use disorders, and suicidal ideation or intentional self-injury. These findings highlight the importance of developing distinct, tailored health management strategies for the autistic older adults with and without intellectual disability.
Keywords
Introduction
Relatively little is known about the health status of autistic adults over the age of 65 years. Much of what is known about this population comes from self-report studies, which exclude individuals for whom surveys are inaccessible (van Heijst & Geurts, 2015), or studies with limited generalizability due to restriction to a single geographic region (Bishop-Fitzpatrick & Rubenstein, 2019; Lever & Geurts, 2016). Other studies combine data from autistic adults over the age of 65 years together with younger age groups, which makes it challenging to distinguish the unique needs of this older population (Bishop-Fitzpatrick & Rubenstein, 2019; de Winter et al., 2012). The lack of studies in this area creates a great deal of uncertainty for autistic adults, their loved ones, and healthcare systems concerning how best to anticipate and meet this population’s needs as they age (Bishop-Fitzpatrick & Rubenstein, 2019; Kats et al., 2013; Piven & Rabins, 2011).
To help address this gap in knowledge, US national data were used in a recent study to compare the prevalence of physical and mental health conditions among autistic older adults (age 65+ years) to a population comparison group (Hand et al., 2020). Results revealed that autistic older adults were more likely than the population comparison group to be diagnosed with almost all physical and mental health conditions examined. However, the extent to which the physical and mental health conditions for which older autistic adults require care differs based on intellectual disability (ID) remains unclear.
Studies of younger populations of autistic individuals have found that the healthcare needs of those with and without co-occurring ID tend to differ. For example, some studies have found autistic individuals without co-occurring ID are more likely to have mental health conditions like depression, anxiety, and suicidal ideation than autistic individuals with ID (Camm-Crosbie et al., 2018; Hand et al., 2019; Strang et al., 2012). Other studies have found that autistic individuals with ID are more likely than those without ID to have epilepsy (Berg & Plioplys, 2012) or obesity (Rimmer et al., 2010). In addition, there is some evidence to suggest that autistic adults with ID over the age of 40 years may be more likely than same-aged autistic adults without ID to have neurologic and gastrointestinal disorders (Bishop-Fitzpatrick & Rubenstein, 2019).
Further research is critical for understanding the specific needs of older autistic adults with and without co-occurring ID to inform autism community members, policy makers, healthcare delivery systems, and healthcare providers. The purpose of this study, therefore, was to compare the prevalence of physical and mental health conditions among a national sample of older autistic adults with and without co-occurring ID. We hypothesized that autistic adults with and without co-occurring ID would significantly differ on the prevalence of mental and physical health conditions. Specifically, based on prior literature, we hypothesized that mental health conditions would be more common among autistic older adults without ID, while autistic older adults with ID would be more likely to have physical health conditions like epilepsy, gastrointestinal conditions, and obesity.
Methods
Data source
We analyzed beneficiary-level inpatient and outpatient healthcare claims data from Medicare Standard Analytic Files (SAF), which include Limited Data Set information on 100% of Medicare beneficiaries for the years 2016–2017. One unique benefit of this data source is that it allows us to study a large, national sample of individuals without the need for prospective data collection. The SAF outpatient records contained medical billing claims from institutional outpatient providers (i.e. hospital outpatient departments, rural health clinics, renal dialysis facilities, outpatient rehabilitation facilities, Federally Qualified Health Centers, and community mental health centers) but did not include professional service claims from non-institutional professional providers such as physicians, physician assistants, clinical social workers, or nurse practitioners.
Study population
Autistic adults were included in this study if they (1) were aged 65 years or older, (2) were enrolled in Medicare Fee for Service for at least 6 consecutive months in 2016 or 2017, and (3) had at least one inpatient or outpatient encounter with an autism spectrum disorder (ASD) diagnosis at any time during 1 January 2016 to 31 December 2017. Requiring only one ASD diagnosis has been shown to be appropriate for identifying autistic individuals in Medicare claims (Benevides et al., 2019) and has been used in prior studies of healthcare claims data (e.g. Benevides et al., 2020; Hand et al., 2020; Leslie & Martin, 2007; Maddox et al., 2018). ASD diagnoses were identified using International Classification of Diseases, 10th edition (ICD-10) codes F84.0, F84.1, F84.5, or F84.9.
We excluded beneficiaries enrolled in Medicare Advantage Plans due to concerns regarding the availability of accurate, complete data (Demiralp et al., 2019; Lankiewicz et al., 2018; Mahr et al., 2018). We also excluded Medicare-enrolled autistic adults under the age of 65 years. Although recent expert-opinions suggest that autistic individuals should be considered older adults at the age of 50 years (Roestorf et al., 2019), we chose to keep the more conventional cut-off of 65 years of age due to Medicare eligibility rules. Most Medicare beneficiaries are entitled to coverage based on their age (i.e. any US citizen or permanent resident over the age of 65 years). In contrast, individuals under the age of 65 years can also qualify for Medicare, but only with a formal disability ruling by the Social Security Administration. As Medicare beneficiaries under the age of 65 years may differ in meaningful ways from individuals who qualify for Medicare on the basis of age, we made the methodologic choice that would result in the most homogeneous study sample.
After identifying all eligible autistic older adults, we classified the beneficiaries into two groups: (1) autistic older adults with a co-occurring ID diagnosis and (2) autistic older adults without a co-occurring ID diagnosis. ID was identified based on at least one medical encounter with an ICD-10 code of F70–F79.
Measures
We identified mental and physical health conditions using the Healthcare Cost and Utilization Project (HCUP) Beta Multilevel Clinical Classification Software (CCS) for ICD-10 (HCUP, 2016). HCUP Beta CCS groups diagnostic codes from the medical billing record into a smaller number of clinically meaningful categories. We also identified some mental and physical health conditions, including obesity, menopausal disorders, Parkinson’s disease, multiple sclerosis, sleep disorders, and attention-deficit hyperactivity disorders, based on the presence of specific ICD-10 codes. We provided a list of the physical and mental health conditions we examined and how each was defined in Supplementary Table 1.
Statistical analysis
Demographic characteristics were summarized descriptively. To maintain beneficiary confidentiality, frequency counts were only provided if >10 for all sub-groups. Separate logistic regression models were performed to compare older autistic adults with and without co-occurring ID on the odds of each condition while controlling for sex, race/ethnicity, age, rural residence, estimated household income, and duration (months) of observation. Race and ethnicity were categorized as white non-Hispanic, Black non-Hispanic, Hispanic, and other/unknown. Rural residence was defined by living in a non-metropolitan statistical area. Household incomes were estimated for each beneficiary using the median per capita household income during 2017, among individuals over 65 years of age, for the beneficiary’s county of residence. Duration of observation was defined as the number of months during 2016 and 2017 that the individual was enrolled in Medicare. Odds ratios (ORs) were interpreted according to Agresti (2013). In addition, we performed a sensitivity analysis to determine the extent to which our results were influenced by our inclusion criteria (i.e. inclusion of autistic adults with at least one inpatient or one outpatient encounter with a diagnosis of autism). To examine this, we replicated our analyses with only the subset of beneficiaries who met a more stringent inclusion criteria of at least one inpatient or two outpatient encounters with a diagnosis code for autism. We used SAS statistical software, version 9.4 for all analyses.
Ethical approval
The Institutional Review Board (IRB) of the Ohio State University reviewed this study and determined it to be IRB-exempt due to the use of limited datasets.
Results
A total of 4685 autistic older adults met the inclusion criteria for this analysis. Demographic information for included beneficiaries is provided in Table 1. Most beneficiaries were male, aged 65–69 years, and white. Approximately 19% of autistic older adults with an ID and 21% of those without ID resided in rural areas. Most beneficiaries resided in the Southern or Northeastern United States.
Demographic characteristics of autistic older adult Medicare beneficiaries with and without co-occurring intellectual disability.
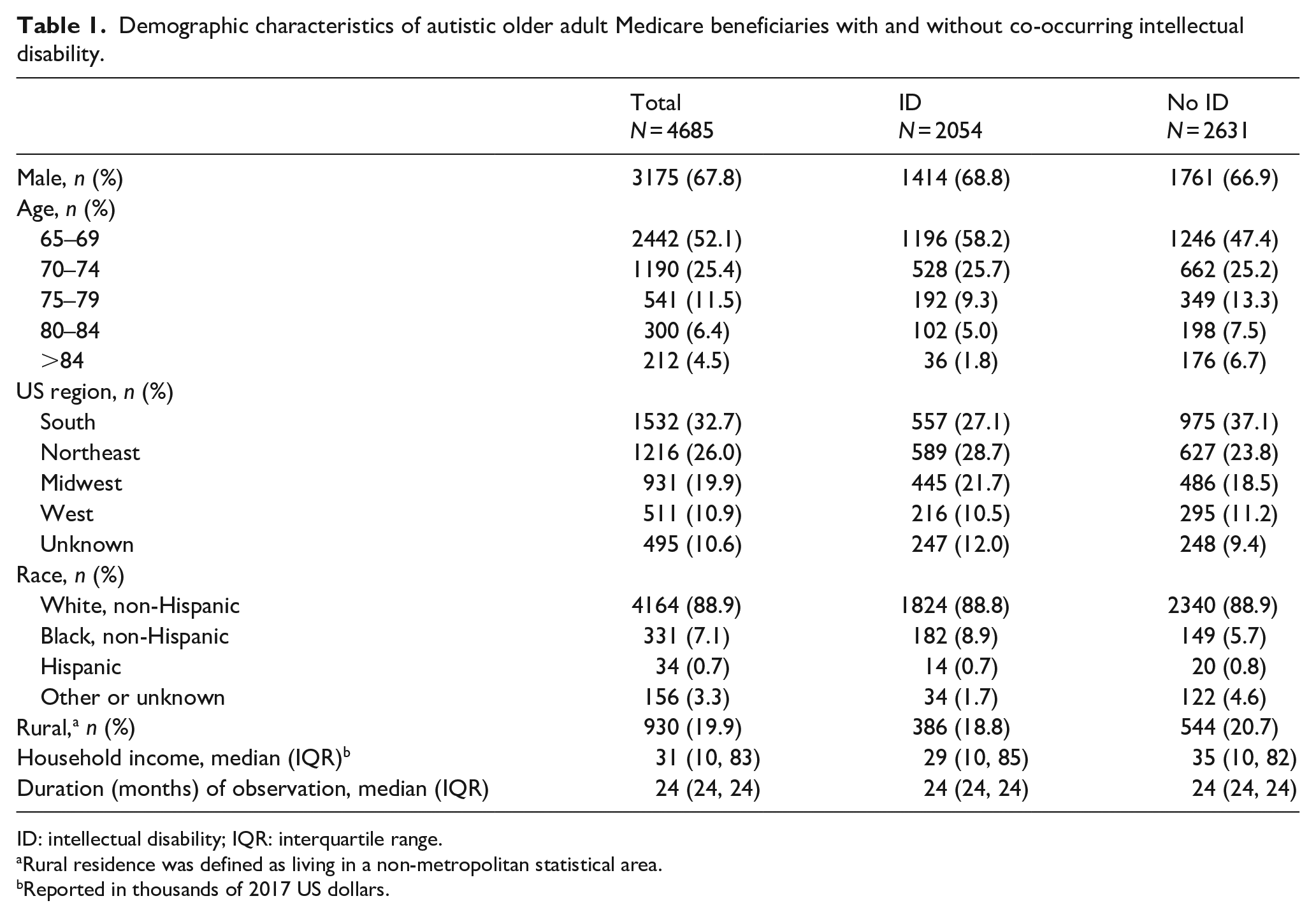
ID: intellectual disability; IQR: interquartile range.
Rural residence was defined as living in a non-metropolitan statistical area.
Reported in thousands of 2017 US dollars.
Table 2 provides information on the prevalence of physical and mental health conditions among autistic older adults with and without co-occurring ID. After adjusting for sex, age, race/ethnicity, rural residence, and estimated household income, significant differences between groups were observed in the odds of having most physical and mental health conditions. Specifically, relative to autistic older adults without ID, those with co-occurring ID had 350% greater odds of epilepsy (OR = 4.5, 95% confidence interval (CI) = 3.9–5.2), 170% greater odds of osteoporosis (OR = 2.7, 95% CI = 2.3–3.2), 100% greater odds of other gastrointestinal disorders (OR = 2.0, 95% CI = 1.8–2.2), 80% greater odds of respiratory infections (OR = 1.8, 95% CI = 1.6–2.1), 50% greater odds of thyroid disorders (OR = 1.5, 95% CI = 1.3–1.7), 50% greater odds of upper or lower gastrointestinal disorders (OR = 1.5, 95% CI = 1.3–1.7), 40% greater odds of cognitive disorders (OR = 1.4, 95% CI = 1.2–1.6), and 30% greater odds of schizophrenia/psychotic disorders (OR = 1.3, 95% CI = 1.1–1.6).
Prevalence of physical and mental health conditions among autistic older adults with and without co-occurring intellectual disability.
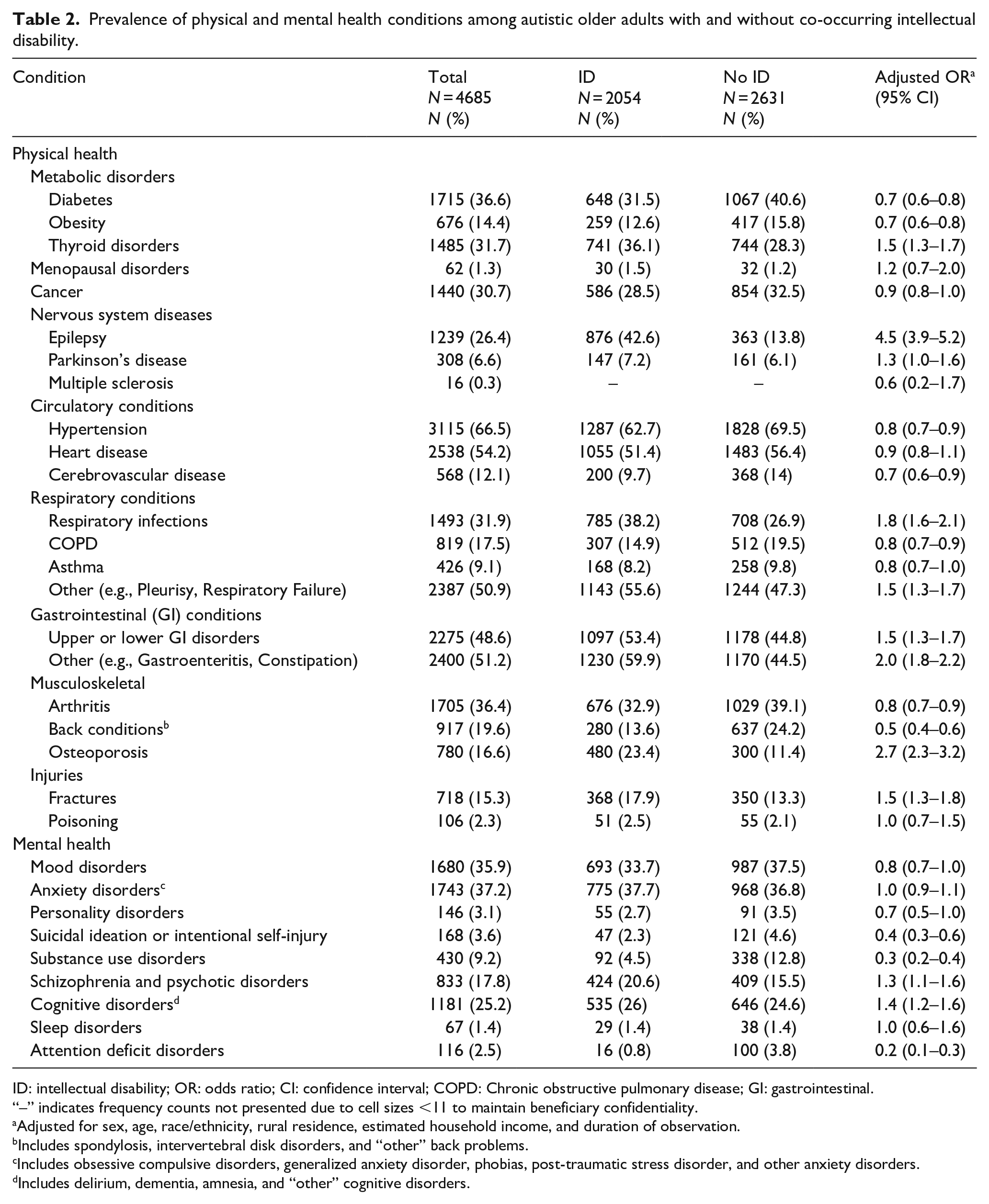
ID: intellectual disability; OR: odds ratio; CI: confidence interval; COPD: Chronic obstructive pulmonary disease; GI: gastrointestinal.
“–” indicates frequency counts not presented due to cell sizes <11 to maintain beneficiary confidentiality.
Adjusted for sex, age, race/ethnicity, rural residence, estimated household income, and duration of observation.
Includes spondylosis, intervertebral disk disorders, and “other” back problems.
Includes obsessive compulsive disorders, generalized anxiety disorder, phobias, post-traumatic stress disorder, and other anxiety disorders.
Includes delirium, dementia, amnesia, and “other” cognitive disorders.
However, autistic older adults with ID had significantly lower odds of attention deficit disorders (ADD; 80% lower odds; OR = 0.2, 95% CI = 0.1–0.3), substance use disorders (70% lower odds; OR = 0.3, 95% CI = 0.2–0.4), suicidal ideation or intentional self-injury (60% lower odds; OR = 0.4, 95% CI = 0.3–0.6), back conditions (50% lower odds; OR = 0.5, 95% CI = 0.4–0.6), obesity (30% lower odds; OR = 0.7, 95% CI = 0.6–0.8), diabetes (30% lower odds; OR = 0.7, 95% CI = 0.6–0.8), cerebrovascular disease (30% lower odds; OR = 0.7, 95% CI = 0.6–0.9), high blood pressure (20% lower odds; OR = 0.8, 95% CI = 0.7–0.9), chronic obstructive pulmonary disease (20% lower odds; OR = 0.8, 95% CI = 0.7–0.9), and arthritis (20% lower odds; OR = 0.8, 95% CI = 0.7–0.9).
Sensitivity analysis
Supplementary Table 2 summarizes demographic information about the subset of beneficiaries who were included in our sensitivity analyses. A total of 3388 beneficiaries (N = 1594 with co-occurring ID; N = 1,794 without co-occurring ID) met the more stringent inclusion criteria, requiring at least one inpatient or two outpatient encounters with an autism diagnosis. Supplementary Table 3 provides information on the prevalence of physical and mental health conditions among this subset of beneficiaries. Overall, logistic regression results comparing the odds of physical and mental health conditions among the subsets of autistic older adults with and without ID were consistent with those presented in Table 2. One exception is that, in this sensitivity analysis, autistic older adults with and without co-occurring ID did not significantly differ in the odds of diabetes (OR = 1.1; 95% CI = 0.6–2.0).
Discussion
The present study constitutes the first US nation-wide analysis of the prevalence of health conditions among autistic adults over 65 years of age, stratified by ID. Results of this study suggest that autistic older adults with and without ID significantly differ on the prevalence of many physical and mental health conditions. The findings of this work have important implications for healthcare providers, healthcare systems, and policy makers. For example, these findings speak to the need to develop tailored health management strategies for autistic older adults as a function of co-occurring ID due to differences in the prevalence of many conditions. In addition, by characterizing the healthcare needs of autistic adults as they age using a large national sample, this study addresses a priority area identified by the Interagency Autism Coordinating Committee’s (2017) 2016–2017 strategic plan, which is used to inform funding priorities for federal activities related to autism. Our results can help inform future funding priorities to develop innovative, patient-centered solutions to better meet the healthcare needs autistic older adults with and without ID.
When interpreting our findings, it is important to acknowledge that beneficiaries included in this study were selected based on medical billing records from inpatient hospitalizations or institutional outpatient visits. Institutional outpatient visits include visits to hospital outpatient departments, rural health clinics, community health centers, renal dialysis facilities, and outpatient rehabilitation facilities. These settings likely did not capture all eligible autistic older adults, as individuals may have received outpatient care in non-institutional settings from professional providers such as physicians, physician assistants, clinical social workers, and nurse practitioners. As a result, it is possible that some Medicare-enrolled autistic older adults were not included in this study. In addition, it is possible that the autistic older adults who were included in this study visited non-institutional outpatient facilities for mental or physical healthcare, which indicates that our findings likely represent a conservative estimate of the prevalence of mental and physical health conditions in this population.
It is also important to acknowledge that the results of this study apply only to those autistic adults who are currently 65 years of age or older and may not be predictive of the health needs of future generations of autistic older adults. For example, our inclusion of only individuals who lived past 65 years introduces survivorship bias, particularly as autistic adults may be at elevated risk for premature mortality (Hirvikoski et al., 2016). As such, our findings generalize only to those autistic adults who live past the age of 65 years, a population that may be meaningfully different from those autistic adults who do not live past the age of 65 years. In addition, all Medicare beneficiaries included in this study were born before the year 1950, which was before autism was an official diagnosis (1980) in the Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III) and revisions were made to the diagnostic criteria for autism in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; 1994) and Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). These beneficiaries also did not have the protections afforded to subsequent generations by the Americans with Disabilities Act (1990) and the Individuals with Disabilities Education Act (1990) during their formative years. As such, this sample likely includes autistic individuals with different health-related needs than current pediatric or younger adult samples. Nevertheless, the findings of this study have important implications for the healthcare of autistic older adults living in the United States today.
Indeed, comparing our findings to those of prior studies suggests that autistic older adults represent a unique subgroup with healthcare needs that are distinct from younger populations of autistic adults or older adults with ID. In examining the prevalence of physical and mental health conditions among our total sample, the autistic older adults in this study had a higher prevalence of most health conditions than have been found in prior studies of autistic adults (Croen et al., 2015) or adults with ID (Cooper et al., 2015; Hussain et al., 2020; McCarron et al., 2017). For example, the prevalence of rates diabetes and hypertension in our sample were 36.6% and 66.5%, while Croen et al. (2015) found prevalence rates among autistic adults of 7.6% and 25.6%, respectively. This higher prevalence is likely explained by the older age of individuals included in our sample, as Croen et al.’s (2015) study comprised almost exclusively of individuals aged 18–64 years. However, our sample did have a lower prevalence of a select few health conditions compared to that of Croen et al. (2015) such as obesity (14.4% vs 33.9%), asthma (9.1% vs 12.5%), ADD (2.5% vs 12.0%), and sleep disorders (1.4% vs 17.6%). Relative to prior studies on the prevalence of conditions among adults with ID aged 60+ years (Hussain et al., 2020), our sample of autistic older adults had a higher prevalence of a number of conditions including diabetes (36.6% vs 25.6%), heart disease (54.2% vs 14.9%), hypertension (66.5% vs 8.7%), and anxiety (37.2% vs 22.0%) but lower prevalence of other conditions such as asthma (9.1% vs 16.1%) and arthritis (36.4% vs 40.4%).
Several of our findings, however, are consistent with the broader literature about the physical and mental health of younger populations of autistic individuals. For example, co-occurring ID is significantly associated with gastrointestinal conditions among autistic individuals aged 1–53 years (Penzol et al., 2019) and osteoporosis among autistic individuals over the age of 40 years (Bishop-Fitzpatrick & Rubenstein, 2019). In addition, the link between autism, ID, and epilepsy has been well-documented in pediatric samples (Anand & Jauhari, 2019; Berg & Plioplys, 2012). While the mechanisms that link these conditions are not well-understood, literature points to likely factors such as shared genetic underpinnings and similar biological processes (Lee et al., 2015). In part, the common co-occurrence of autism, ID, and epilepsy may explain our finding of increased prevalence of osteoporosis among autistic older adults with ID, as anti-seizure medications are a known risk factor for osteoporosis (Srikanth et al., 2011).
Similar to other published studies, we also found that ADD was more common among autistic adults without ID (Bishop-Fitzpatrick & Rubenstein, 2019). One possible explanation for this finding may be that, among those with ID, ADDs may be more difficult to diagnose due to diagnostic overshadowing (Al-Khudairi et al., 2019). The higher prevalence of ADDs among autistic older adults without ID may also explain the increased risk of substance use disorders among this group, as prior studies have shown that substance use disorders are most common among autistic adults who have a co-occurring ADD diagnosis (Butwicka et al., 2017).
Finally, our results echo the need for better methods of detecting of suicidality among autistic individuals. Autistic older adults have 15 times greater odds of suicidal ideation and intentional self-injury, and autistic adults have 5 times greater odds of suicide attempts than general older adult and adult populations, respectively (Croen et al., 2015; Hand et al., 2020). In this study, autistic older adults without co-occurring ID were significantly more likely to have a medical encounter for suicidal ideation or intentional self-inflicted injury than those with a co-occurring ID. This finding may be related to evidence that absence of an ID is associated with higher rates of depression among autistic individuals (Buck et al., 2014; Greenlee et al., 2016), and depression is a well-established risk factor for suicidal ideation (Mayes et al., 2013; Stewart et al., 2017; Taliaferro & Muehlenkamp, 2014). Our findings, therefore, add to a growing body of literature on factors associated with increased risk of suicidality among autistic individuals (e.g. Cassidy et al., 2018; Hand et al., 2019; Kirby et al., 2019).
Methodologic considerations and future directions
Several additional methodologic factors are crucial to acknowledge for this study and should be considered when interpreting our results. First, we identified autistic adults based on the presence of at least one inpatient or outpatient encounter with an autism diagnosis for our primary analyses. Although this approach is supported by research evidence (Benevides et al., 2019) and precedent (e.g. Benevides et al., 2020; Hand et al., 2020; Leslie & Martin, 2007; Maddox et al., 2018), we also conducted a sensitivity analysis to determine the extent to which using more stringent criteria to identify autistic adults (at least one inpatient or two outpatient encounters) may have altered our findings. Of the 22 physical health conditions and nine mental health conditions examined, the results of our sensitivity analysis differed from our primary analysis for only one condition, diabetes. This indicates a high degree of consistency between our primary and sensitivity analyses. The lack of a significant difference between autistic older adults with and without co-occurring ID on the odds of diabetes in our sensitivity analysis may have been due to a non-existent association between co-occurring ID and diabetes, or due to type II error given the large number of analyses completed.
Other methodologic considerations include our inability to control for variables such as socioeconomic status, social support, and perceived met/unmet healthcare needs, and these may be strongly associated with the prevalence of the conditions that we examined. In addition, the diagnostic codes found in the medical claims data that we used for this study carry with them possible bias; accurate diagnoses can be challenging for providers to obtain for patients who have barriers to communication, and providers themselves may have their own biases that influence their diagnostic decision making. This study did not examine longitudinal change in the occurrence of physical and mental health conditions, but this will be important to examine in future work. Finally, eligible autistic older adults who did not seek treatment for physical and mental health conditions or who were undiagnosed were also not captured in this study. Despite these methodological factors, this work provides an impactful contribution to the literature and may aid clinicians in provision of informed healthcare for autistic older adults with and without ID.
Conclusion
This research offers valuable insight into the distinct physical and mental health conditions for which Medicare-enrolled autistic older adults with and without ID require care. Further research is warranted to understand change in condition prevalence over time and the underlying mechanisms that contribute to differences in the prevalence of physical and mental health conditions between autistic older adults with and without ID. The findings of this work further support the need for comprehensive, patient-centered healthcare for this population to best meet their needs.
Supplemental Material
Supplemental_Table_2_1 – Supplemental material for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims
Supplemental material, Supplemental_Table_2_1 for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims by Daniel Gilmore, Lauren Harris, Anne Longo and Brittany N Hand in Autism
Supplemental Material
Supplemental_Table_3_1 – Supplemental material for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims
Supplemental material, Supplemental_Table_3_1 for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims by Daniel Gilmore, Lauren Harris, Anne Longo and Brittany N Hand in Autism
Supplemental Material
Supplementary_Table_1_1 – Supplemental material for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims
Supplemental material, Supplementary_Table_1_1 for Health status of Medicare-enrolled autistic older adults with and without co-occurring intellectual disability: An analysis of inpatient and institutional outpatient medical claims by Daniel Gilmore, Lauren Harris, Anne Longo and Brittany N Hand in Autism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.