
Abstract
The COVID-19 pandemic disrupted a range of health services for children across the United States. Autistic children have well-documented deficits in health-related services compared to nonautistic children. Parents of autistic children reported an increase in mental health and behavior problems with the onset of the pandemic, increasing the need for supportive services. The current study used data from the National Survey of Children’s Health from 2019 and 2020 to conduct logistic regressions predicting the likelihood of having unmet service needs before and after the onset of the pandemic. Results suggested that autistic children were more likely to have unmet medical, dental, and mental health service needs across years compared to nonautistic children, but there were no interactions by year. All children experienced an increased likelihood of having unmet needs from pre- to post-pandemic. Results suggest that although the pandemic disrupted services across the board, autistic children lacked health services regardless of the pandemic, pointing to persisting disparities in service receipt. A discussion of ongoing barriers to services and issues related to virtual services is included. Future research should further investigate the feasibility of virtual services as well as ways of reducing barriers to all services for autistic children.
Lay abstract
The COVID-19 pandemic disrupted doctor’s and dental visits, mental health treatments, and other special therapies for children across the United States. Prior research has found that autistic children were more likely to lack these services even before the pandemic, but they experienced more mental health and behavior problems with the onset of the pandemic, increasing the need for these services. This study analyzed data from before (2019) and after (2020) the onset of the pandemic to determine whether autistic children had even more severe disruptions in services after the pandemic started compared to nonautistic children. We found that autistic children were more likely to have unmet medical, dental, and mental health needs in both 2019 and 2020. Overall, children experienced increased disruptions from 2019 to 2020, but this did not differ by diagnosis. Our results suggest that there are persisting gaps in autistic children’s healthcare regardless of the pandemic. We discuss issues surrounding barriers to services for autistic children and issues surrounding virtual services, such as teletherapy. Future research should further explore how to reduce barriers to services for autistic children, including virtual and in-person services.
During the spring of 2020, as the COVID-19 pandemic caused the widespread closure of schools, workplaces, and storefronts in the United States, many healthcare services, including medical, dental, behavioral, and mental health services were restricted or suspended to mitigate the spread of COVID-19. The Centers for Medicare & Medicaid Services (CMS) reported a large drop in vaccinations, screenings, dental, and mental health visits between the spring of 2019 and the spring of 2020 among children in Medicaid and Children’s Health Insurance Program (McMorrow et al., 2020). Prior to the pandemic, autistic children were more likely than nonautistic children to have unmet preventive, specialty, and therapeutic care needs (Chiri & Warfield, 2012). One study by Cummings and colleagues (2016) found that among children aged 10–17, autistic children were less likely to receive a well-child visit compared to nonautistic children. In addition, autistic children aged 3–9 were less likely to have received a vaccination in the prior year compared to nonautistic children.
More broadly, autistic children have well-documented barriers to accessing health-related services. For example, many areas in the United States have a severe shortage of specialists who can diagnose and provide specialty services for autistic children (Malik-Soni et al., 2022). Relatedly, primary care physicians often lack the expertise and skills to treat autistic children, especially children with more impairing symptoms who require special accommodations for communication differences, sensory challenges, and challenging behavior (Malik-Soni et al., 2022). Parents’ lack of knowledge of autism and available services has also been found to predict lower service utilization, particularly among families of lower socioeconomic status (SES) and those who live in more rural areas (Antezana et al., 2017; Pickard & Ingersoll, 2016). Stigma within the healthcare system continues to be another barrier to families seeking health and related services, even more so for families of color and immigrant families (Khanlou et al., 2017; Kinnear et al., 2016). Finally, financial and logistic barriers such as work schedules and a lack of transportation are further barriers to services, especially for families with lower SES (Pickard & Ingersoll, 2016).
With the onset of the pandemic, parents of autistic children reported significant disruptions in services, including medical, special education, speech-language pathology, physical and occupational therapy, applied behavior analysis, early intervention, and mental health services (Bhat, 2021; L. C. White, Law, et al., 2021). A study by L. C. White, Law and colleagues (2021) found that younger children were more likely to be affected by disruptions in services, presumably because younger children have more difficulty with attending virtual services compared to older children. Given that earlier intervention is associated with more positive outcomes, disruptions in services for younger children are especially alarming. In addition, missed well-child visits have the potential to delay developmental screening for children with increased likelihood of autism, leading to delayed diagnosis and intervention (Bellomo et al., 2020). In addition to disruptions in needed medical and behavioral health services, autistic children experienced increased mental health and behavior problems with the onset of the pandemic (Colizzi et al., 2020; Mutluer et al., 2020; Vasa et al., 2021). One study found that communication challenges, stereotypy, and hypersensitivity worsened along with behavior problems and sleep difficulties from pre- to postpandemic among autistic children and young adults (Mutluer et al., 2020). In addition, parental anxiety was significantly correlated with children’s irritability, hyperactivity, and inappropriate speech during the pandemic but not before the pandemic (Mutluer et al., 2020). Within 2 months of the onset of the pandemic, 59% of parents of autistic children in an autism center registry reported that their child had experienced either worsening of prepandemic psychiatric symptoms or the development of new symptoms, including ADHD, anxiety, depression, behavior problems, irritability, and sleep problems (Vasa et al., 2021).
During the pandemic, many services transitioned from traditional in-person visits to telemedicine. Utilization of telehealth as a tool to continue care delivery while reducing the risk of COVID-19 exposure offered new opportunities and improved access to services by reducing barriers associated with cost, transportation, taking time away from work, and coordinating childcare (Annaswamy et al., 2020; Kryszak et al., 2022). However, the shift to virtual services also posed many unique challenges and logistical barriers for certain populations in accessing care. For example, high-speed Internet and connectivity are not accessible in certain rural or low-income communities (Ramtekkar et al., 2020). In addition, many platforms used for delivering telehealth do not have sufficient features to adequately support communication for individuals who are deaf, blind, or who have intellectual disabilities (Annaswamy et al., 2020). Specifically, a mixed methods investigation of practitioner and client perspectives found that, despite numerous benefits, teletherapy may be especially challenging for clients with English as a second language, or who have significant mental health concerns or intellectual disabilities and do not live with a person who can provide support in navigating telehealth (Johnsson & Bulkeley, 2021). Some parents of autistic children have reported that telehealth services were difficult for children with communication challenges or specific learning styles, while others noted that their child simply did not feel satisfied with virtual services (S. W. White, Stoppelbein, et al., 2021). Thus, the availability of virtual services may not have been able to compensate for the loss of in-person services, particularly for autistic children.
The loss of daily routines caused by the pandemic, including being kept home from school, isolation from peers and/or loved ones, and more time spent inside likely contributed significantly to worsening mental and behavioral health for all children. This may have been particularly distressing for autistic children, who often rely heavily on routines and predictability. Autistic children needed services more during the pandemic than ever before but experienced severe disruptions. However, the extent to which the pandemic contributed to unmet needs among autistic children relative to those without autism has not been examined. The current study aims to investigate patterns of unmet service needs for autistic and nonautistic children in the United States before and after the onset of the COVID-19 pandemic within a large, nationally distributed sample.
Methods
Participants
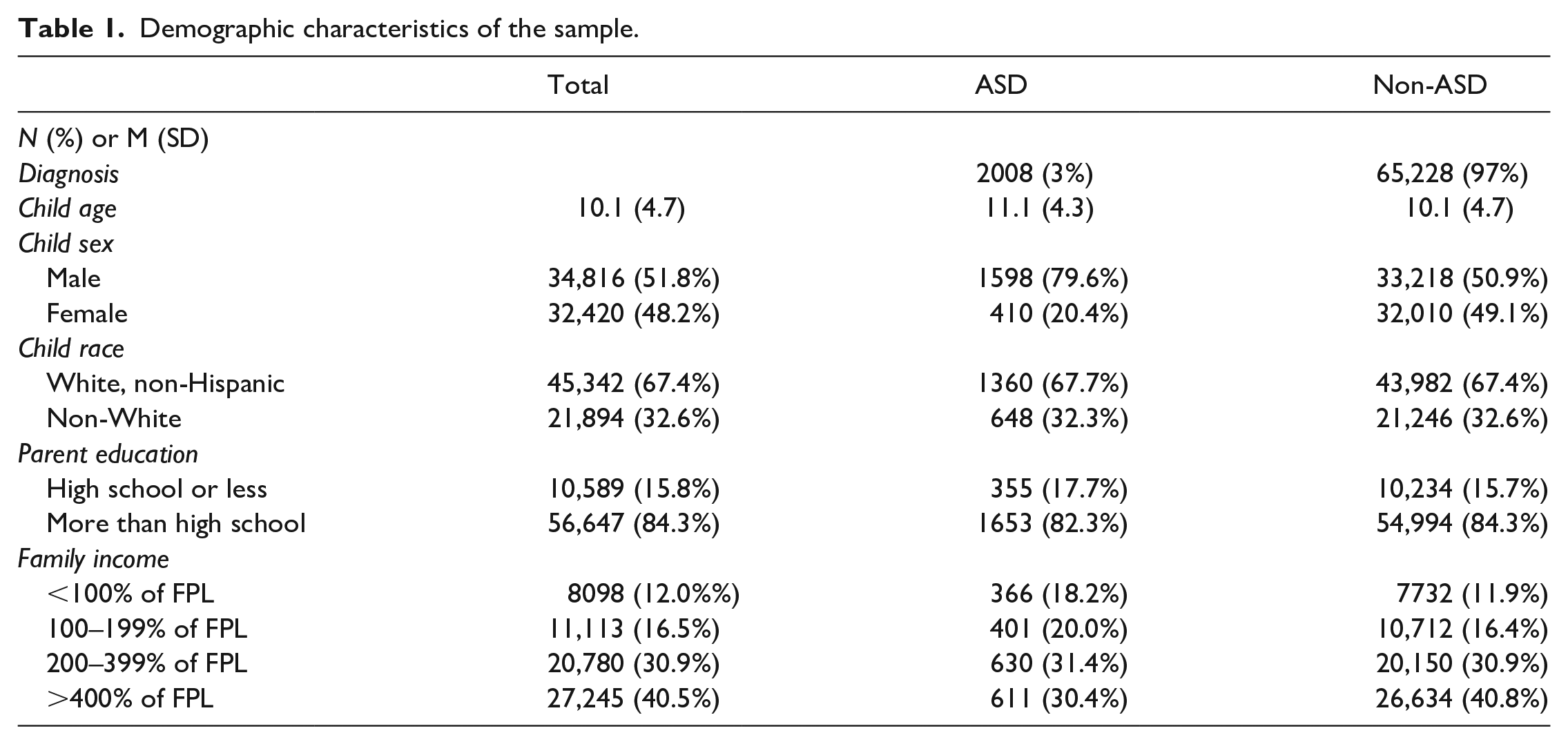
The sample consisted of 34,816 male (51.8%) and 32,420 female (48.2%) children aged 2–17 years (M = 10.1) whose parents completed the National Survey of Children’s Health (NSCH), a questionnaire that examines the mental and physical health of children across the United States. Invitations to complete the questionnaire were sent to randomly selected households across the United States with options to complete the survey online or on paper. Children younger than the age of 2 years were excluded due to the low probability of having an ASD diagnosis. Prepandemic respondents (surveyed in 2019) comprised 40.8% of the sample, while 59.2% responded during the pandemic (surveyed between July 2020 and January 2021). The demographic characteristics of the families that participated are reported in Table 1. The majority of participants were White, non-Hispanic (67.4%) with at least one college-educated parent (61.2%) whose family income was above 200% of the federal poverty level (FPL) (71.4%). The FPL refers to the income threshold set by the US Census Bureau at which an individual or family is considered to be living in poverty, depending on the number of people in the household.
Demographic characteristics of the sample.
Measures
Demographic variables of interest were child age, sex, race (non-White vs White, non-Hispanic), and the family’s income converted to percentage of the federal poverty level (FPL).
ASD diagnosis
Parents were asked if their child had ever been diagnosed with an autism spectrum disorder, including Asperger’s Disorder and Pervasive Developmental Disorder (PDD), and whether their child currently met criteria for the disorder (1 = current ASD, 0 = no current ASD).
Year responding
Participants who responded as part of the 2019 survey were included in the prepandemic group, coded 0, while participants who responded in 2020 were included in the pandemic group, coded 1.
Unmet health service needs
Parents were asked if there was a time in the past year that their child had a care need that went unmet, including medical, dental, and mental health. Having any unmet care need was the first outcome of interest; additionally, medical, dental, and mental health care needs were included as separate outcomes of interest.
Data analysis
A series of logistic regressions were conducted, each of which included demographic covariates, autism diagnosis, year, and the interaction between autism diagnosis and year as predictors of the binary outcome of whether the child had not received a needed health service in the prior year (for medical, dental, mental health, or any health service). Odds ratios are reported in lieu of coefficients for ease of interpretation.
There was no community involvement to report in the current study.
Results
Table 2 summarizes the results of the logistic regressions. Controlling for covariates and year responding, autistic children were nearly four times more likely to have any unmet health need than nonautistic children (OR = 3.86, p < 0.001). Unsurprisingly, controlling for covariates and autism diagnosis, children were 1.3 times more likely to have had an unmet health need during 2020 than 2019 (OR = 1.28, p < 0.001). The interaction between autism diagnosis and year was not significant (OR = 1.05, p = 0.77), suggesting that autistic children did not experience a disproportionate loss of services compared to nonautistic children (Figure 1).
Results of the logistic regressions predicting likelihood of having an unmet service need within the prior year.
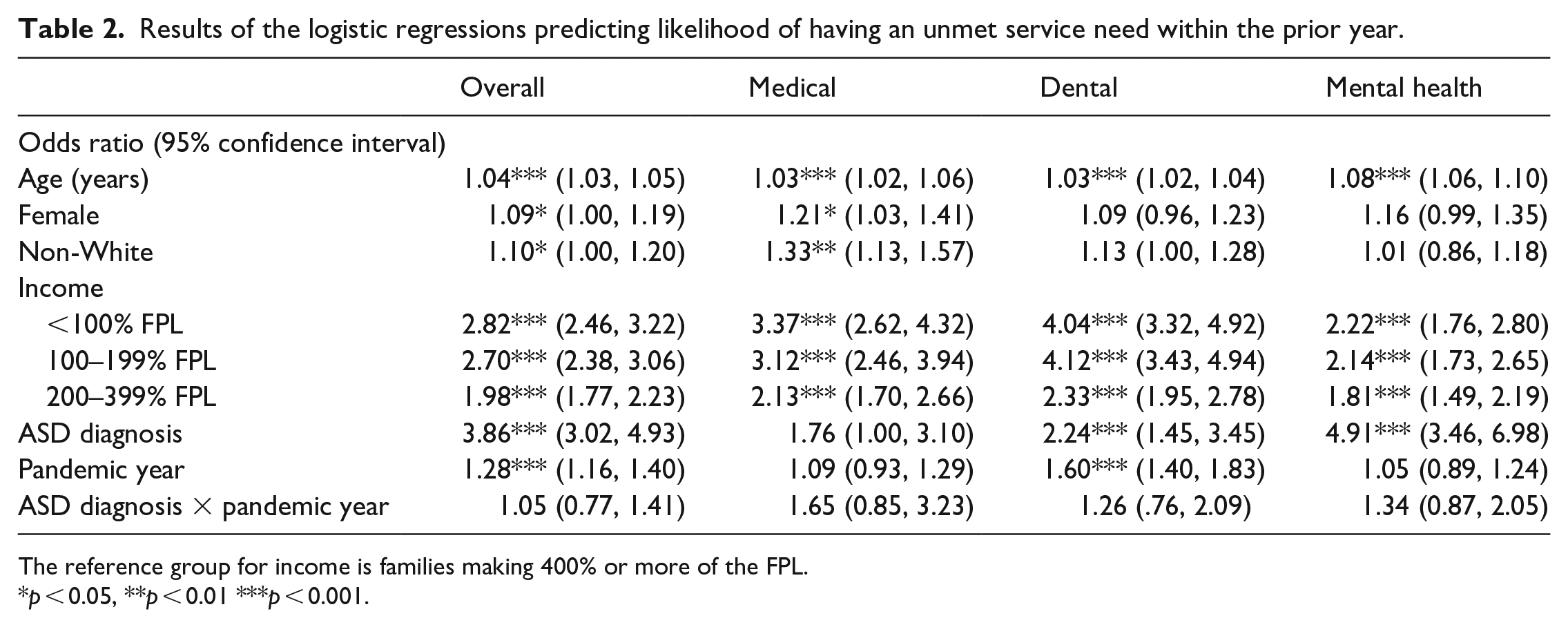
The reference group for income is families making 400% or more of the FPL.
p < 0.05, **p < 0.01 ***p < 0.001.

Estimated marginal means of having unmet service needs by year and diagnostic group.
With respect to separate healthcare services, autistic children were significantly more likely to have unmet dental (OR = 2.24, p < 0.001) and mental health (OR = 4.91, p < 0.001) needs across years, and were marginally more likely to have unmet medical needs (OR = 1.76, p = 0.05). A main effect of pandemic year was observed for dental care (OR = 1.60, p < 0.001), but not for medical or mental health. The interaction between autism diagnosis and year was not significant for any of the three outcomes.
Unsurprisingly, families from lower income brackets were significantly more likely to report unmet needs across all outcomes compared to families making 400% or more of the FPL (p < 0.001 for all analyses). In addition, for each 1-year increase in age, there was a significant increase in the likelihood of having an unmet need across all outcomes (p < 0.001 for all analyses). Finally, females and non-White children were more likely to have an unmet medical need and an unmet healthcare need more broadly. However, given that these odds ratios are small and the confidence intervals approach 1, it is likely that the large sample size allowed detection of very small effects which may not necessarily reflect clinical or practical significance.
Discussion
Results suggest that autistic children were nearly four times more likely to have an unmet healthcare need than nonautistic children across years, regardless of pandemic interference. This pattern largely held true when examining medical, dental, and mental health needs separately. This is consistent with previous findings of health disparities among autistic children (Chiri & Warfield, 2012; Cummings et al., 2016). This is likely a result of a variety of barriers to accessing services that are common among autistic children, including stigma, communication, sensory, and behavior challenges, and a lack of available providers with sufficient expertise (Malik-Soni et al., 2022).
While the pandemic did not have a disproportionate effect on autistic children’s access to services, it did disrupt health services overall, with more parents reporting an unmet healthcare need in 2020 compared to 2019. However, when examining individual services, only dental care was significantly impacted by the onset of the pandemic, while medical and mental health care were not. One explanation for the nonsignificant effect for medical care is that it may be regarded as more medically necessary than dental care and thus prioritized even during a global pandemic. However, it is unclear whether parents considered well-child or preventive care visits as “medical care,” or whether they interpreted medical care to mean services procured as a result of illness or injury. In addition, the pandemic may have actually reduced barriers to mental health services as many providers began offering teletherapy (Pinkerton et al., 2022), which was found to be acceptable by children and their parents (Meininger et al., 2022). Finally, telehealth services may be feasible for certain services, such as mental health therapy, while it is not feasible for addressing most medical or dental care needs.
It is also likely that children missed out on certain therapies that were not feasible or difficult to administer virtually or that the children more generally had difficulty attending to virtual services (Bellomo et al., 2020). For example, certain components of occupational or behavioral therapies are challenging to implement virtually given the emphasis on behavior observation, modeling, and utilization of shared materials while being in close contact (Baweja et al., 2021). Prior research found that caregivers of autistic children often need to have active involvement in their child’s virtual therapy to support their engagement given attention difficulties, frustration, or overstimulation (Pellicano et al., 2020; L. C. White, Law, et al., 2021), but this may not be feasible to implement in all home environments. In addition, some caregivers reported that telehealth may be incompatible with their child’s learning, communication, or processing styles (e.g. visual learners, nonverbal communication, or literal processors; (Pellicano et al., 2020; S. W. White, Stoppelbein, et al., 2021). Overall, the efficacy of virtual services for autistic children is an emerging area of research, with some studies suggesting that virtual services can be both effective and convenient (Sutherland et al., 2018), while others highlight the variability in telehealth experiences among autistic children (S. W. White, Stoppelbein, et al., 2021).
The availability of telehealth for certain needs, such as mental health services, may increase the likelihood that some autistic children receive needed services because it addresses some barriers to receiving services in person (Solomon & Soares, 2020) as long as it is found to be acceptable to the individual. However, virtual service delivery is difficult or impossible for many other kinds of services, including medical, dental, and behavioral health services. Future research should not only investigate the acceptability of telehealth for different types of health services among autistic children and their families but should also continue to work toward improving access to in-person services where telehealth is not a feasible option. For example, Project ECHO Autism has achieved success in training primary care physicians and community mental health providers in evidence-based care for autistic children, helping to reduce barriers to these services caused by lack of access to specialists (Dreiling et al., 2022; Mazurek et al., 2017). With this model, community providers are supported in meeting the specific needs of autistic children, which is particularly important in areas where specialty providers are scarce and/or waitlists for services are long.
Results were also consistent with previous findings of disparities in health services among lower-income families (Oberg et al., 2016). Children from lower-income families were significantly more likely to have unmet health needs, despite 95% of the sample reporting health insurance coverage. This suggests that despite the availability of public health insurance programs, there are additional barriers to receiving needed health services that should be examined. Although we did not examine whether low-income families had more access to services during the pandemic due to the availability of telehealth, this may have been the case for some families for whom transportation, time, and childcare constraints posed significant barriers to in-person services. However, there are still barriers to telehealth services among some low-income families, such as lack of a reliable Internet connection or a device capable of telehealth video calls (Ramtekkar et al., 2020).
The current study presents a high-level overview of how the pandemic disrupted services for autistic and nonautistic children. Although autistic children did not experience disruptions in services that were disproportionate to the general population, the pandemic exacerbated an already existing problem among this community, and there are mixed findings on the acceptability of virtually delivered services among autistic children. Future research should further investigate whether the quality of virtual services is comparable to that of in-person services.
The current study has several limitations. Although the NSCH strives for a nationally representative sample, the sample was skewed toward higher-income, college-educated families. The study excludes parents who were unable or unwilling to complete a lengthy, in-depth survey about their child’s health and development, and the self-report nature of the survey does not guarantee accuracy. As such, the data likely underestimate the loss of services in the general population. In addition, because of the nature of the survey, we did not have detailed data on the family’s service needs or experiences navigating healthcare systems. Future research should consider other family and systemic factors that contribute to these significant disparities in service receipt among autistic children, such as family structure, parent’s mental health and social support, and the availability of specialty providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The National Survey of Children’s Health (NSCH) is conducted by the U.S. Census Bureau for the U.S. Department of Health and Human Services’ (HHS) Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB). All data are available on the U.S. Census Bureau website: ![]() .
.