
Abstract
This study estimated the prevalence of autism spectrum disorder in a 5-year inpatient cohort of children and adolescents diagnosed with first-episode psychosis in two Hong Kong teaching hospitals, and explored the clinical characteristics predicting first-episode psychosis–autism spectrum disorder comorbidity. The autism spectrum disorder diagnoses of 103 patients with first-episode psychosis were confirmed by Autism Diagnostic Interview–Revised. Based on the (1) Diagnostic and Statistical Manual of Mental Disorders (5th ed.) diagnostic checklist and (2) Autism Diagnostic Interview–Revised, three major observations were reported: (1) the prevalence of autism spectrum disorder among children and adolescents with first-episode psychosis was 28.2% (95% confidence interval = (19.7%, 37.9%)); (2) after administering the Autism Diagnostic Interview–Revised, an additional 31.0% of first-episode psychosis patients met the clinical diagnostic cut-off for autism spectrum disorder; and (3) multivariate binary logistic regression analysis showed that first-episode psychosis patients with a comorbid autism spectrum disorder diagnosis were more likely to be a male than a female (adjusted odds ratio = 3.57, 95% confidence interval = (1.29, 9.86), p = 0.014). Adding to the current literature, this study examined first-episode psychosis–autism spectrum disorder comorbidity with a large Chinese, inpatient sample with first-episode psychosis. Consistent with studies conducted overseas, we show that autism spectrum disorder is a common comorbidity among Chinese first-episode psychosis patients. A comprehensive autism spectrum disorder assessment that incorporates both observation-based and parent-report diagnostic tools is warranted for children and adolescents, especially boys, with psychosis.
Lay abstract
Autistic features are commonly observed in children and adolescents with first-episode psychosis, but they are sometimes overlooked by clinicians and caregivers. By comprehensively examining the clinical profiles of 103 children and adolescents (below 18 years old) with first-episode psychosis and conducting the Autism Diagnostic Interview–Revised (the ‘gold standard’ autism diagnostic tool) with their primary caregivers, we showed that around 28% of patients with first-episode psychosis had a comorbid autism diagnosis, and boys were 3.57 times more likely to have first-episode psychosis–autism spectrum disorder comorbidity than girls. After administering the Autism Diagnostic Interview–Revised, we also observed that an additional 30% of patients with first-episode psychosis met the autism spectrum disorder diagnostic cut-off; their autism spectrum disorder symptoms were probably overshadowed by prodromal psychotic symptoms and left undetected before this study. The co-occurrence of autism and first-episode psychosis might be more common than we previously thought. Careful autism screening and assessment is highly recommended for clinicians working with patients with psychosis.
Introduction
Acute psychosis, defined as the manifestation of florid psychotic symptoms encompassing delusion, hallucination, disorganized thinking, grossly disorganized or abnormal motor behaviour, and negative symptoms (American Psychiatric Association [APA], 2013), is the most disabling mental condition associated with significant socioeconomic burden (GBD Mental Disorders Collaborators, 2022). In accordance with the early detection and intervention principle (Birchwood et al., 1998), many works have been done to improve the outcomes associated with the onset of first-episode psychosis (FEP), yet, after decades of research, the outcome improvement is minimal (Fusar-Poli et al., 2017). Of note, converging evidence shows that FEP patients with poorer premorbid social functioning, including those with a comorbid diagnosis of autism spectrum disorder (ASD; Larson et al., 2017; Strålin & Hetta, 2019), are associated with worse functional outcomes (Chisholm et al., 2019; Hollis, 2000; Wunderink et al., 2013; Zheng et al., 2021). Improving our understanding about this subgroup may enhance overall FEP illness outcome, although these patients, particularly those with FEP-ASD comorbidity, are currently underrepresented.
Diagnosing comorbid ASD in patients with FEP is particularly challenging (Ribolsi et al., 2022), because there is substantial overlap in symptomatology between psychosis and autism (Chisholm et al., 2015; Sampson et al., 2021; Vaquerizo-Serrano et al., 2022); some researchers suggest that ASD is probably underdiagnosed among people with psychosis (Kincaid et al., 2017). Our understanding about FEP-ASD comorbidity is further complicated by the use of different ASD assessment tools for discerning autistic features from psychotic symptoms in patients with FEP, as currently no single standardized tool is designed for this purpose. For instance, self-report autistic trait screening tools are sometimes adopted (Zheng et al., 2021), although some researchers noted that the use of screening tools alone might not be adequate for delineating the overlapping symptoms of psychosis and autism (Schalbroeck et al., 2023). Meanwhile, others may adopt observation-based ASD diagnostic tools (Treise et al., 2021; Trevisan et al., 2020), although observation-based tools primarily measure current, but not childhood-onset, autistic-like features (Schalbroeck et al., 2023), which could be overshadowed by active psychotic symptoms (Trevisan et al., 2020), and some evidence even suggests that solely using observation-based ASD diagnostic tools may lead to overdiagnosis of ASD in patients with psychosis (Maddox et al., 2017).
To acquire information regarding both current and childhood-onset autistic-like features in patients with FEP, semi-structured interviews appear to be the most suitable choice, one of which is the Autism Diagnostic Interview–Revised (ADI-R; Falkmer et al., 2013; Lord et al., 1994), a ‘gold standard’ ASD diagnostic tool. Indeed, ADI-R has been adopted in several studies for confirming ASD diagnosis in patients with psychosis (Davidson et al., 2014; Mandell et al., 2012; Sunwoo et al., 2020; Waris et al., 2013). These studies were mainly conducted in western countries with heterogeneous samples, with the reported prevalence rates of FEP-ASD comorbidity varying between 3.6% (Davidson et al., 2014) and 52% (Waris et al., 2013). Such variability in findings is likely influenced by sample diversities across studies, for example, participants’ age, psychiatric comorbidities and nationalities (M.-C. Lai et al., 2019). The prevalence of FEP-ASD has not been formally investigated in any Chinese population, not to mention the clinical characteristics of these individuals.
This study aimed to add to the literature on the FEP-ASD comorbidity of the Chinese child and adolescent population. By conducting a cross-sectional cohort study (Hudson et al., 2005) with a large Chinese inpatient sample with FEP, we documented the prevalence and clinical characteristics of FEP-ASD of a 5-year FEP patient cohort in two Hong Kong teaching hospitals that serve approximately 18% (i.e. 1.3 million) of the local population (Hospital Authority, 2021). Of note, both the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnostic checklist for ASD (APA, 2013) and the ADI-R Cantonese Version (K. Y. Lai et al., 2022), performed by child psychiatrists, were used to guide diagnostic decisions. The socioeconomic and clinical characteristics predicting FEP-ASD comorbidity were also explored.
Methods
Participants
Participants under the age of 18 with FEP (with or without a prior clinical diagnosis of ASD) admitted to the Child and Adolescent Psychiatric Inpatient Wards in two teaching hospitals of the Chinese University of Hong Kong, Alice Ho Miu Ling Nethersole Hospital (AHNH) or Tai Po Hospital (TPH), between May 2017 and April 2022 were included in this study. In these two hospitals, psychiatric diagnoses and/or diagnoses of neurodevelopmental disorders were given after multidisciplinary clinical evaluation made during hospitalization by an expert panel led by consultant child psychiatrists (K.Y.C.L., F.Y.M.M., S.-F.H., C.K.S.S.), according to the DSM-5 (APA, 2013). Specifically, every day during hospitalization, inpatients were individually seen by the child psychiatrists/clinical psychologists; they also participated in several group sessions, of which their social and communicative behaviours, as well as sensory issues, were observed by speech pathologists, occupational therapists or mental health nurse practitioners. As a requirement of AHNH and TPH, clinical observations made by these professionals were routinely documented after each patient contact. This 5-year cohort was selected because detailed patient histories and multidisciplinary clinical observation notes that informed inpatient diagnostic decisions were available, which were thoroughly documented in multiple systems including the (1) Hong Kong Hospital Authority Clinical Management System (CMS), (2) Hong Kong Hospital Authority Clinical Data Analysis and Reporting System (CDARS), and (3) paper-based patient records.
Patients were defined to have first-episode psychosis if they showed no evidence of receiving treatment for psychosis before their hospitalization during May 2017 to April 2022. We excluded FEP patients with the following comorbidities: (1) significant medical illnesses affecting the central nervous system (e.g. epilepsy and organic brain damage), (2) substance abuse or dependence, and (3) moderate/severe/profound intellectual disability (ID; full-scale intelligence quotient (IQ) < 50; APA, 2000). Of note, we excluded patients with moderate/severe/profound ID because the lack of reliable self-report of psychotic symptoms from these patients may contribute to reduced validity of psychosis diagnosis (Hatton et al., 2005). However, given current evidence suggests that psychosis could be reliably diagnosed (Hatton et al., 2005) in patients with mild ID (50 ⩽ full-scale IQ < 69; APA, 2000), we included FEP patients comorbid with mild ID, who also demonstrated adequate abilities to comprehend verbal instructions (Resnik & Ness, 2012) and express personal psychotic experience.
Procedures
To identify potential participants, a two-step procedure was performed by the first author (T.T.Y.K.) who was supervised by the corresponding author (C.K.S.S.). First, AHNH and TPH Child and Adolescent Psychiatric Inpatient Ward consecutive admission lists (period: 1 May 2017 to 30 April 2022), with age, sex and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) principal diagnosis codes (at discharge) for this admission for all patients (represented by a unique hospital number) admitted during this period, were retrieved from the CDARS; patients with the ICD-9-CM principal diagnosis codes 295-298 were included in the next stage of screening. Then, the clinical profiles of these patients were retrieved and screened in the CMS to include potential participants who had their first treatment contact for FEP in this admission and without (1) other neurological disorders, (2) histories of substance abuse and (3) moderate/severe/profound ID.
All potential participants were reached and informed about this study. Informed consents were sought from both patients and their parents/primary caregivers in person when they attended post-hospitalization outpatient psychiatry follow-up. If both parties consented to participate in the study, a three-step procedure would be administered. First, a consultation session would be arranged for the patient, during which T.T.Y.K. would conduct a clinical interview and examine the participant’s current ASD and psychotic symptoms according to DSM-5 diagnostic criteria. Second, the parents/primary caregivers of the patient were invited to visit AHNH for (1) attending the ADI-R diagnostic interview (duration: 60–120 min) and (2) completing a questionnaire that gathered information about sociodemographic status of the patient’s family (i.e. parental age, sex, education, living arrangement, household income), first-degree family histories of mental illnesses, and participants’ birth and medical histories, which took around 30–60 min to complete. Third, the participant’s inpatient multidisciplinary clinical observation notes that documented their social and communicative behaviours during inpatient hospitalization and other clinical information (i.e. clinical presentation of psychosis, comorbid mental illness, aggression and suicidal risks at admission, duration of hospitalization, medication regime and dosage upon discharge) were obtained from CDARS, CMS and paper-based patient records. Missing or unclear data and information were clarified with patients and parents or primary caregivers upon interview. Note that the DSM-5 diagnostic checklist and ADI-R were administered to all parents/primary caregivers of the participants even if the participants had already diagnosed with ASD before this study.
Measures
ASD diagnoses for all participants were made based on the (1) DSM-5 diagnostic checklist for ASD (APA, 2013) and (2) ADI-R Cantonese Version (K. Y. Lai et al., 2022). These assessments were conducted by a child psychiatrist (T.T.Y.K.) with all decisions being discussed with the corresponding author (C.K.S.S.), one of the consultant psychiatrists from the expert panel responsible for inpatient diagnostic decisions.
Although incorporating standardized observation-based ASD diagnostic tools, for example, the Autism Diagnostic Observation Schedule, Second edition (ADOS-2; Lord et al., 2012), Diagnostic Interview for Social and Communication Disorders–11th edition (DISCO-11; Wing et al., 2002) and Developmental, Dimensional and Diagnostic Interview (3di; Skuse et al., 2004), would allow us to perform ASD-specific clinical observations and might further strengthen our study design, these tools were not used because (1) previous research suggested that none of these tools comprehensively represents DSM-5 diagnostic criteria for ASD (Evers et al., 2021) and (2) some of these tools were shown to have a high false-positive rate (e.g. 30% when ADOS-2 was used; Maddox et al., 2017) in identifying autistic features among people with psychosis. To obtain a more comprehensive picture regarding participants’ ASD symptom manifestation (such that ASD diagnosis was not made based on just a single patient contact), the DSM-5 diagnostic checklist was applied by T.T.Y.K. to assess patients’ (1) current ASD symptomatology during patient consultation session and (2) ASD symptomatology during hospitalization based on detailed retrospective reviews of clinical observation notes regarding participants’ social and communicative behaviours.
To obtain ADI-R scores, T.T.Y.K. scored primary caregivers’ descriptions of the child’s behaviours according to the ADI-R diagnostic algorithms. ADI-R is a standardized, investigator-based tool with 93 items that assess 4 domains of dysfunction – (1) language/communication, (2) reciprocal social interactions, (3) restricted and repetitive, stereotyped behaviours and interests and (4) abnormality of development evident at or before 36 months – of patients with mental ages from 2 years old and above (Hus & Lord, 2013). Participants scored above cut-off for all four domains indicated a diagnosis of ASD. The Cantonese version of ADI-R was shown to have high sensitivity and specificity within the DSM-5 framework in Chinese children (K. Y. Lai et al., 2022).
Participants’ aggression and suicidal risks at admission were measured by Nurses’ Global Assessment of Suicide Risk (NGSAR; Cutcliffe & Barker, 2004) and Dynamic Appraisal of Situational Aggression (DASA; Ogloff & Daffern, 2006), respectively. Detailed psychometric properties of ADI-R, as well as the descriptions of NGSAR and DASA, are reported in Table S1.
Data analysis
To estimate the proportion of FEP patients with a comorbid diagnosis of ASD within this 5-year FEP patient cohort (i.e. FEP-ASD prevalence), the number of patients with a diagnosis of ASD was divided by the total number of FEP patients within this cohort, with 95% confidence interval (CI) estimated using the exact binomial test. Based on the findings from a previous systematic review (Kincaid et al., 2017), we anticipated that a small proportion of previously undiagnosed ASD cases would meet clinical diagnostic cut-off on the ADI-R (i.e. missed ASD diagnosis). To explore the possible explanations for missed ASD diagnosis, we planned to compare the ASD (reflected by ADI-R subdomain scores) and FEP (reflected by the presence of affective symptoms/delusion/hallucination/thought disorder/disorganized behaviours/negative symptoms) symptomatology between FEP participants with a missed ASD diagnosis and those who were diagnosed with ASD before this study using chi-square test/Fisher’s exact test (for categorical data) or Welch’s t-test (for continuous data). Given the exploratory nature of this analysis, a significant difference between the two groups was indicated by p < 0.05 (uncorrected).
To explore the socioeconomic and clinical characteristics predicting FEP-ASD comorbidity, a multivariate binary logistic regression (enter method, two-tailed, alpha level = 0.05) was conducted. Candidate variables included in the regression model survived (1) the threshold of p ⩽ 0.1 (uncorrected) in the univariate analyses (i.e. chi-square test/Fisher’s exact test for categorical data, independent-samples t-test/Mann–Whitney U test for continuous data) that tested the differences in all sociodemographic and clinical variables in FEP patients with and without a diagnosis of ASD, (2) Box-Tidwell tests for linearity of logit and (3) bivariate analyses for correlations between independent variables. The Hosmer and Lemeshow goodness-of-fit test was used to examine the fitness of the logistic regression model. Adjusted odds ratios (ORs) with 95% CI were calculated. Statistical Package for the Social Sciences (SPSS) version 28 was used for statistical analyses (SPSS Inc., Chicago, IL, USA).
Community involvement
This investigation is part of a prospective cohort study that examines the clinical profile and prognosis of patients with comorbid ASD and FEP. Participants involved in this investigation (i.e. hospital-based sample), as well as FEP-ASD participants we recruited from the community, are being followed up for 5 years, during the follow-up period they receive regular psychiatric consultations, and are offered continuous multidisciplinary support. A multidisciplinary autism research team involving psychiatrists (T.T.Y.K., C.K.S.S., F.Y.M.M., S.-F.H., K.Y.C.L.), clinical psychologist (P.W.L.L.) and researcher (M.M.Y.C.) is responsible for the study conception and design, results interpretation, and dissemination of findings.
Results
There were 1160 admission entries (AHNH: 676; TPH: 484) documented between 1 May 2017 and 30 April 2022, with 226 entries (19.48%) bearing a principal diagnosis (at discharge) of psychotic disorders (ICD-9-CM code: 295 and 298; 88 entries) or mood/bipolar disorders with psychotic features (ICD-9-CM code: 296; 138 entries). See Table S2 of the supplementary material for a list of the principal diagnoses (at discharge) for all included and excluded patients. A total of 125 participants were contacted and invited to participate in the study, and finally, 103 FEP participants (mean age: 14.71 years, SD = 1.86 years; male-to-female ratio = 35:68) were recruited in this study (see Figure 1 for the recruitment process). All primary caregivers of 103 participants completed the ADI-R, with 29 patients scored above cut-off for all 4 ADI-R domains, which translated to a prevalence rate of 28.2% (95% CI = (19.7%, 37.9%)) for FEP-ASD comorbidity within this FEP patient cohort. Notably, 9 of these 29 patients, that is, 31.03% (95% CI = (15.28%, 50.83%)) did not have a prior clinical diagnosis of ASD. A closer look into the ASD and FEP symptomatology between the 9 participants (male-to-female ratio = 4:5) with missed ASD diagnosis and the 20 participants (male-to-female ratio = 13:7) with a prior ASD diagnosis (Table 1) revealed that these two subgroups differed in the number of patients who experienced hallucination (χ2(2) = 3.99, p = 0.046); they also showed a trendwise difference in ADI-R social interaction sub-score. Specifically, all but one of FEP patients (88.9%) with missed ASD diagnosis experienced hallucination, but only half of the FEP patients with a prior ASD diagnosis experienced hallucination (50.0%); FEP patients with missed ASD diagnosis had a lower ADI-R social interaction sub-score (M = 14.78; SD = 2.05) than those with a prior ASD diagnosis (M = 16.40; SD = 2.89).
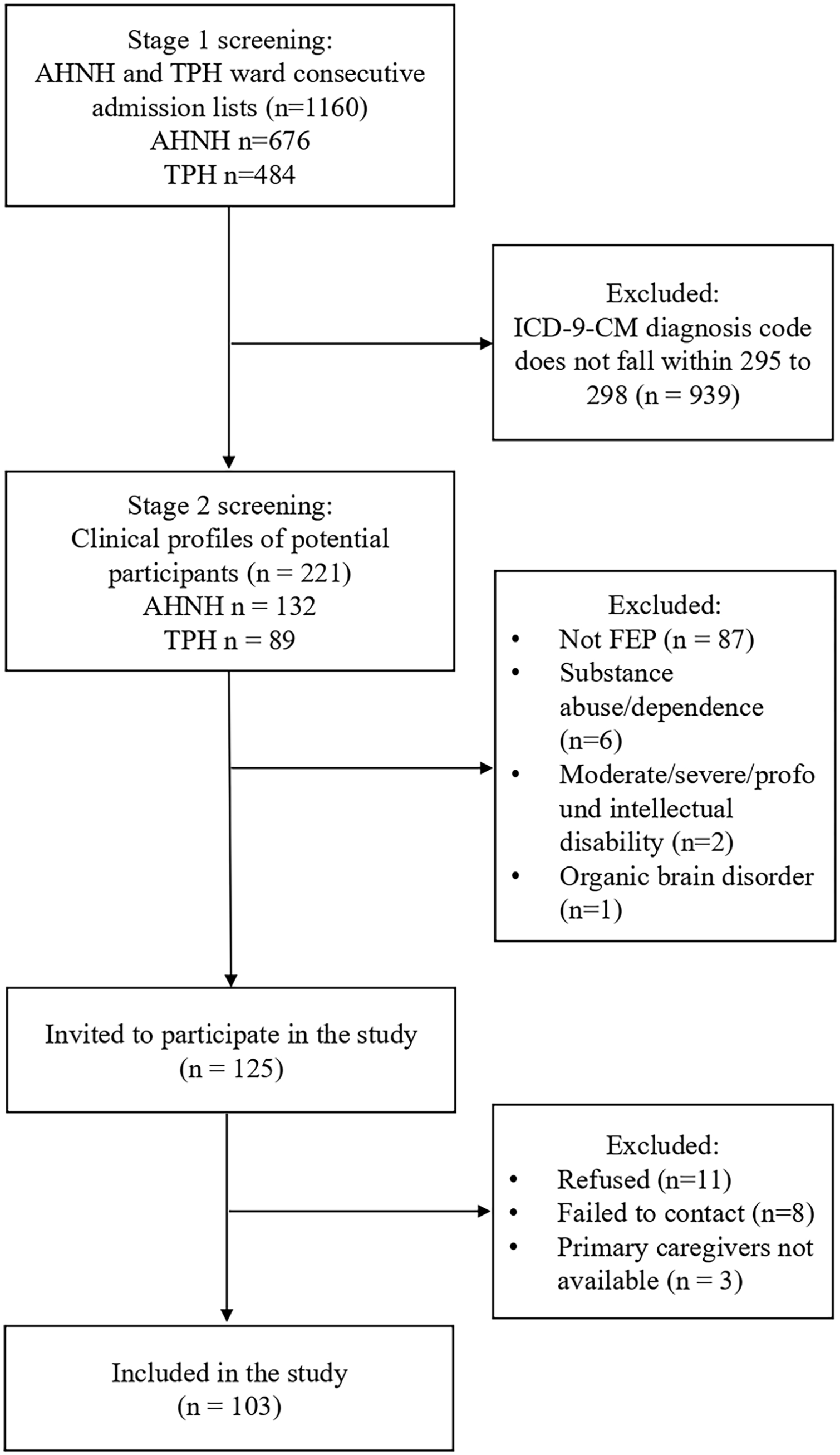
A flowchart showing the participant recruitment process.
Comparison of ASD and FEP symptom manifestation between FEP patients with missed ASD diagnosis and those with prior ASD diagnosis.
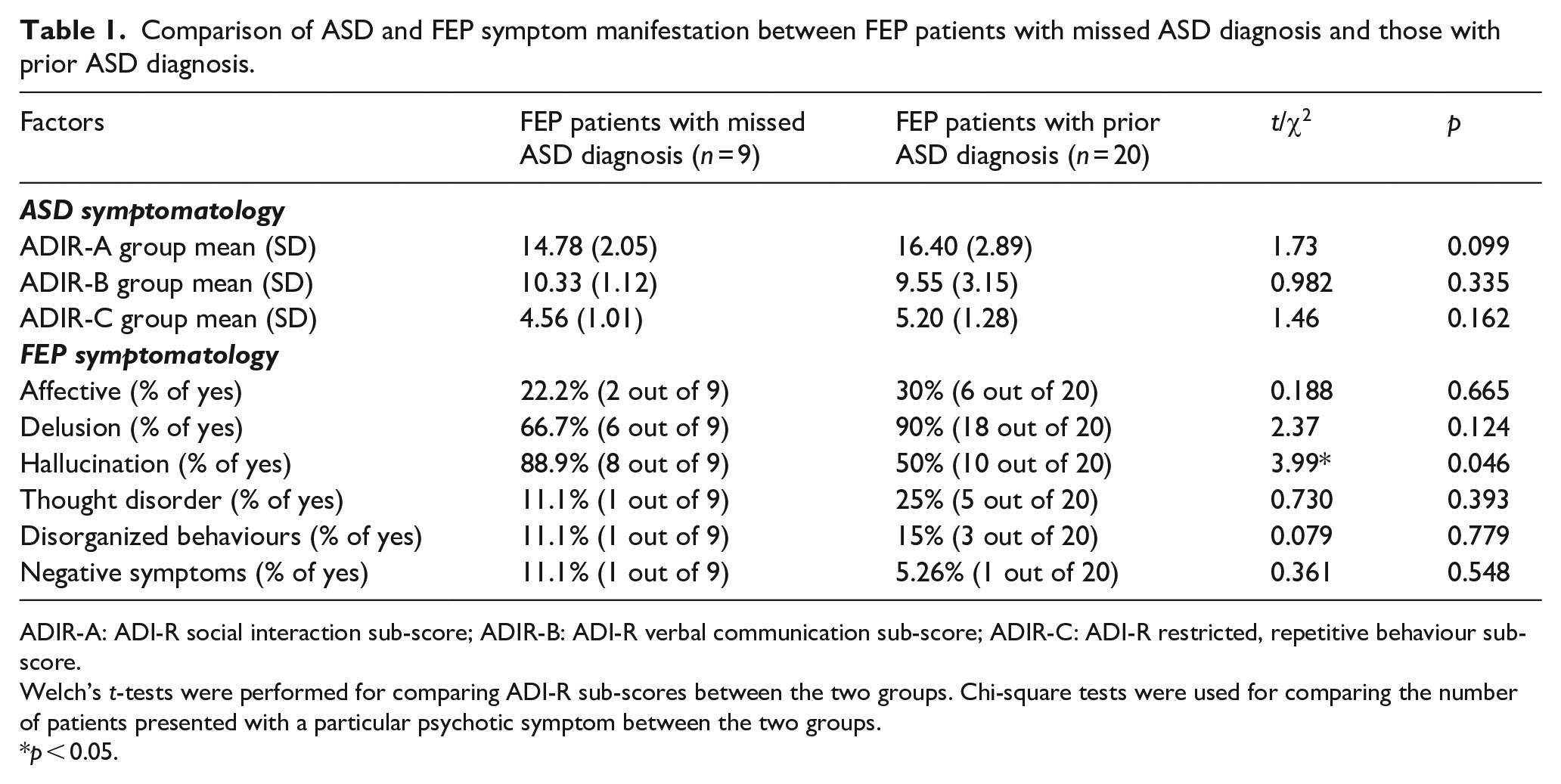
ADIR-A: ADI-R social interaction sub-score; ADIR-B: ADI-R verbal communication sub-score; ADIR-C: ADI-R restricted, repetitive behaviour sub-score.
Welch’s t-tests were performed for comparing ADI-R sub-scores between the two groups. Chi-square tests were used for comparing the number of patients presented with a particular psychotic symptom between the two groups.
p < 0.05.
The sociodemographic data and clinical characteristics of FEP patients with and without ASD are reported in Table 2. Univariate analyses revealed significant differences between the subgroups in (1) sex (p < 0.001), (2) presence of comorbid mental illness (p = 0.017), (3) diagnosis of psychosis (p = 0.029) and trendwise significant differences in (4) first-degree family history of ASD (p = 0.067) and (5) suicidal risk at admission (p = 0.085). These five variables were included in the multivariate logistic regression. Multivariate logistic regression showed that FEP patients with a comorbid ASD diagnosis were more likely to be a male than a female (adjusted OR = 3.57, 95% CI = (1.29, 9.86), p = 0.014). Other variables did not survive the statistical threshold of p = 0.05 (Table S3). Hosmer and Lemeshow goodness-of-fit test indicated that this model achieved a good fit: χ2 (2) = 4.414, p = 0.818.
Sociodemographic data and clinical characteristics of the current sample.
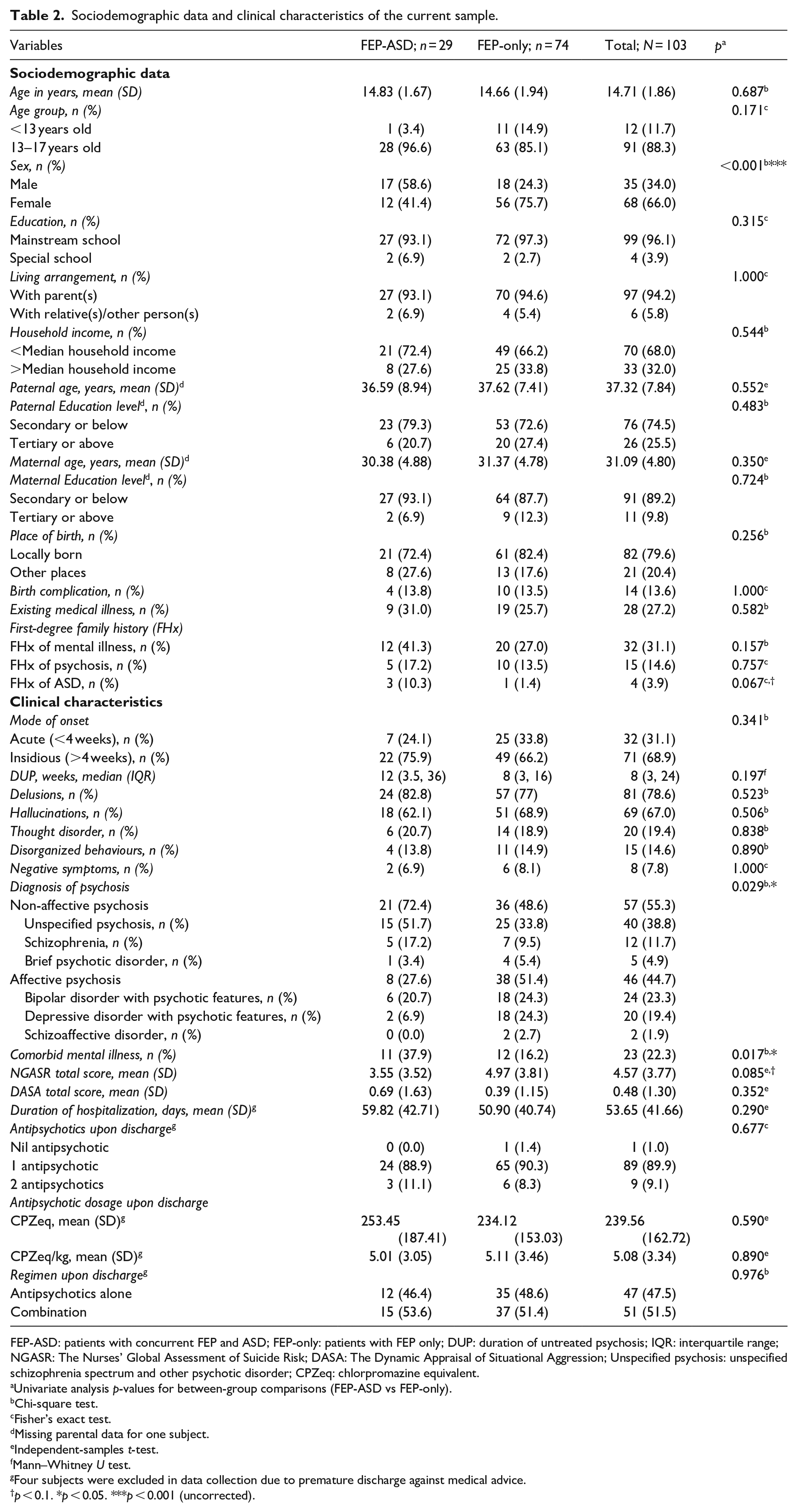
FEP-ASD: patients with concurrent FEP and ASD; FEP-only: patients with FEP only; DUP: duration of untreated psychosis; IQR: interquartile range; NGASR: The Nurses’ Global Assessment of Suicide Risk; DASA: The Dynamic Appraisal of Situational Aggression; Unspecified psychosis: unspecified schizophrenia spectrum and other psychotic disorder; CPZeq: chlorpromazine equivalent.
Univariate analysis p-values for between-group comparisons (FEP-ASD vs FEP-only).
Chi-square test.
Fisher’s exact test.
Missing parental data for one subject.
Independent-samples t-test.
Mann–Whitney U test.
Four subjects were excluded in data collection due to premature discharge against medical advice.
p < 0.1. *p < 0.05. ***p < 0.001 (uncorrected).
Discussion
This study estimated the prevalence of ASD in a 5-year inpatient cohort of children and adolescents diagnosed with FEP in two Hong Kong teaching hospitals and explored the clinical characteristics predicting FEP-ASD comorbidity. ASD diagnoses were made based on (1) clinical consultation that assessed current ASD symptoms based on DSM-5 diagnostic criteria; (2) retrospective review, based on the DSM-5 diagnostic checklist for ASD, of multidisciplinary clinical notes that documented participants’ social and communicative behaviours during their inpatient hospital stay; and (3) the ADI-R. Three main results were reported: (1) the prevalence rate of FEP-ASD comorbidity within a 5-year FEP inpatient cohort of two Hong Kong teaching hospitals is 28.2%; (2) among the 29 patients with FEP-ASD, 31.03% of patients did not have a prior ASD diagnosis, implying that their autistic features might have been overlooked by clinicians; and (3) within this female-dominated FEP cohort, boys were 3.57 times more likely to have FEP-ASD comorbidity than girls.
With a stringent diagnostic method, our study concludes that the prevalence of ASD in Hong Kong children and adolescents suffering from FEP is high, which echoes the results from existing overseas studies (Hallerbäck et al., 2012; Mandell et al., 2012; Waris et al., 2013). The exact mechanisms underlying the high prevalence of FEP-ASD comorbidity is unknown; further studies on this topic are warranted. To improve overall FEP outcome, proper identification of FEP patients comorbid with ASD is of utmost importance as people with ASD often require long-term care and support services beyond acute psychosis management (Larson et al., 2017). However, after administering the ADI-R, we discovered nine additional participants who met the clinical diagnostic cut-off, which implies that solely conducting non-standardized multidisciplinary clinical observations and making clinical judgement based on the DSM-5 diagnostic checklist for ASD might not be adequate for detecting FEP patients comorbid with ASD. Among FEP patients with a missed ASD diagnosis (n = 9), most of them (90%) experience active hallucination, while only 50% of the FEP participants with a prior ASD diagnosis (n = 20) experienced active hallucination during their inpatient stays. This could perhaps explain why ASD diagnoses were missed in some patients during their hospital stay, or even before FEP manifested – autistic traits might be overshadowed by active/prodromal psychotic symptoms, especially for those with less severe social and communicative deficits. To improve the overall diagnostic sensitivity, ASD-specific observation-based and/or parent-report assessments for all patients suffering from FEP are warranted. Nevertheless, as psychotic and ASD symptoms heavily overlap, potential recall bias could exist and affect parent-report assessment (e.g. ADI-R) results. Thus, to make a more accurate ASD diagnosis among patients with psychosis, incorporating both standardized clinical observation tools and parent-report semi-structured interviews (e.g. ADI-R) into routine multidisciplinary clinical observations could be very helpful.
We identify more girls than boys in our cohort of FEP children and adolescents, with 66% of them being female. The observation is consistent with an overseas (Talonen et al., 2017) and a local study (Lee et al., 2016). Despite the predominance of girls in this sample, the number of boys diagnosed with ASD is still higher than girls, with almost half of the boys having a concurrent ASD diagnosis. FEP participants comorbid with ASD are 3.57 times more likely to be male than female. The result aligns with the imbalanced male-to-female ratio of ASD observed in a community adolescent sample (aged 12–17) in Hong Kong (male-to-female ratio = 7.64 to 1; The Chinese University of Hong Kong, 2023) and is consistent with previous studies on the demographic characteristics of the ASD cohorts comorbid with psychosis (Larson et al., 2017; Supekar et al., 2017). However, it should be noted that this finding might be subjected to measurement bias, as current instruments that aid ASD diagnosis were developed with predominantly male samples, which might not capture a more nuanced autistic presentation, especially in females and gender-diverse individuals (Burrows et al., 2022). Nevertheless, based on our current results, we advise that clinicians should prioritize the identification of possible autistic features in male patients suffering from psychosis.
This study added significant value to the current literature by systematically investigating FEP-ASD comorbidity in an inpatient sample of Chinese children and adolescents (below 18 years old) with FEP using (1) the ADI-R (a ‘gold standard’ ASD diagnostic tool), combined with (2) clinical consultation assessing current ASD symptomatology and (3) retrospective review of multidisciplinary clinical observation notes based on the DSM-5 diagnostic checklist for ASD. However, several limitations should be noted, and careful interpretation of results is warranted. First, the high prevalence rate of FEP-ASD comorbidity could be overestimated due to recruitment bias, as it is possible that the caregivers of the participants might already have some suspicion about their children having autism/participants with a prior ASD diagnosis were more willing to participate. Second, as the ASD diagnoses were partly based on retrospective clinical notes review based on DSM-5 diagnostic criteria, this could subject to possible confirmation bias (e.g. looking for evidence from the clinical notes that aligned with current ASD symptomatology and caregivers’ answers to ADI-R questions). Third, the inclusion of only an inpatient sample with FEP might limit the generalizability of results. Nevertheless, we believe that these preliminary results can inspire clinicians to pay special attention to the subtle autistic features that could be overshadowed by psychotic symptoms and possibly incorporate ASD diagnostic tools into daily clinical practice. Last but not least, future studies with a prospective study design and a larger/broader sample (e.g. outpatient/private setting, involvement of other local hospitals) can provide a more generalized and less biased representation of FEP-ASD comorbidity in Hong Kong.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241259062 – Supplemental material for Prevalence of autism in first-episode psychosis in two Hong Kong teaching hospitals
Supplemental material, sj-docx-1-aut-10.1177_13623613241259062 for Prevalence of autism in first-episode psychosis in two Hong Kong teaching hospitals by Terence TY Kwok, Melody MY Chan, Flora YM Mo, Se-Fong Hung, Patrick WL Leung, Kelly YC Lai and Caroline KS Shea in Autism
Footnotes
Acknowledgements
The authors would like to thank all the patients and their families who participated in the study and Mr Tung Siu Ming for his assistance with the extraction of patient admission lists. Data would be available upon reasonable request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Joint Chinese University of Hong Kong–New Territories East Cluster Clinical Research Ethics Committee (Ref no. CRE-2021.439).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.