
Abstract
Transition-age youth and young adults with autism spectrum disorder have complex healthcare needs, yet the current healthcare system is not equipped to adequately meet the needs of this growing population. Primary care providers lack training and confidence in caring for youth and young adults with autism spectrum disorder. The current study developed and tested an adaptation of the Extension for Community Healthcare Outcomes model to train and mentor primary care providers (n = 16) in best-practice care for transition-age youth and young adults with autism spectrum disorder. The Extension for Community Healthcare Outcomes Autism Transition program consisted of 12 weekly 1-h sessions connecting primary care providers to an interdisciplinary expert team via multipoint videoconferencing. Sessions included brief didactics, case-based learning, and guided practice. Measures of primary care provider self-efficacy, knowledge, and practice were administered pre- and post-training. Participants demonstrated significant improvements in self-efficacy regarding caring for youth/young adults with autism spectrum disorder and reported high satisfaction and changes in practice as a result of participation. By contrast, no significant improvements in knowledge or perceived barriers were observed. Overall, the results indicate that the model holds promise for improving primary care providers’ confidence and interest in working with transition-age youth and young adults with autism spectrum disorder. However, further refinements may be helpful for enhancing scope and impact on practice.
The increasing prevalence of autism spectrum disorder (ASD; Baio et al., 2018; Nevison, Blaxill, & Zahorodny, 2018) has been accompanied by a growing population of adolescents and young adults with ASD who need access to healthcare. However, the current healthcare system is not equipped to adequately meet the needs of this special population (Bruder, Kerins, Mazzarella, Sims, & Stein, 2012; Nicolaidis et al., 2013; Rast, Shattuck, Roux, Anderson, & Kuo, 2018; Roux, Shattuck, Rast, & Anderson, 2017; Roux, Shattuck, Rast, Rava, & Anderson, 2015; Warfield, Crossman, Delahaye, Der Weerd, & Kuhlthau, 2015; Zerbo, Massolo, Qian, & Croen, 2015). Youth and young adults with ASD face complex developmental, medical, and psychiatric challenges, and they need support across a range of domains (American Psychiatric Association, 2013; Croen, Najjar, Ray, Lotspeich, & Bernal, 2006), yet the availability of ASD services and community supports declines sharply as individuals age out of the child and adolescent services system (Mauch, Pfefferle, Booker, Pustell, & Levin, 2011).
The psychosocial challenges inherent in transitioning to adulthood are often accompanied by complex healthcare needs for individuals with ASD (Croen et al., 2006). Youth and adults with ASD are at high risk for significant co-occurring medical and psychiatric conditions, including anxiety disorders, depression, behavior disorders, seizures, gastrointestinal problems, sleep disorders, immune conditions, and obesity (Davignon, Qian, Massolo, & Croen, 2018; de Bruin, Ferdinand, Meester, de Nijs, & Verheij, 2007; Levy et al., 2010; Simonoff et al., 2008; Soke, Maenner, Christensen, Kurzius-Spencer, & Schieve, 2018). These conditions rarely exist in isolation, and many appear to be interrelated (Aldinger, Lane, Veenstra-VanderWeele, & Levitt, 2015; Doshi-Velez, Ge, & Kohane, 2014; Kohane et al., 2012; Mazurek et al., 2013). In a recent large-scale study of Kaiser Permanente Northern California members between the ages of 14 and 25, those with ASD were found to be at significantly greater risk for all psychiatric conditions examined and most medical conditions, as compared to a typical control group, with a nearly fourfold increased risk for suicide and self-injury. Nearly all these conditions increased with age among individuals with ASD (Davignon et al., 2018). Psychiatric symptoms, in particular, have frequent onset and worsening during adolescence and adulthood for individuals with ASD (Billstedt, Gillberg, & Gillberg, 2005; Seltzer, Shattuck, Abbeduto, & Greenberg, 2004; Taylor & Seltzer, 2010). Healthcare use and expenditures for individuals with ASD also increase with age, particularly for long-term care, psychiatric medications, and both inpatient and outpatient psychiatric hospitalization (Cidav, Lawer, Marcus, & Mandell, 2013; Shea et al., 2018). As such, individuals with ASD have considerable healthcare needs that appear to increase in complexity as they transition from adolescence into adulthood.
Despite the need for comprehensive and coordinated healthcare, the availability of healthcare specialists with expertise in ASD is limited (Bisgaier, Levinson, Cutts, & Rhodes, 2011; Krauss, Gulley, Sciegaj, & Wells, 2003). Children and adolescents with ASD have more unmet healthcare needs, higher healthcare costs, and worse access to medical homes and specialty care than those with other special healthcare needs (Croen et al., 2006; Kogan et al., 2008; Krauss et al., 2003; Liptak, Stuart, & Auinger, 2006; Sheldrick & Perrin, 2010). These challenges persist and worsen for individuals with ASD over time, and the transition from pediatric to adult healthcare can be fraught with difficulties (Kuhlthau et al., 2016). The results from the 2009–2010 National Survey of Children with Special Healthcare Needs indicated that youth with ASD were much less likely to receive healthcare transition services than those with other special healthcare needs (Rast et al., 2018). Healthcare transition services typically refer to the process of supporting youth in progressing from a pediatric to an adult model of healthcare (White, Cooley, American Academy of Pediatrics, & American Academy of Family Physicians, 2018). In a survey of caregivers of youth with ASD, 40% had not received any type of transition services (Kuhlthau et al., 2016). This may be due to several different factors, including both provider-level and systems-level (Nehring, Betz, & Lobo, 2015; White et al., 2018).
Many youth with ASD do not have access to a medical home (a model of care that is accessible, continuous, family centered, compassionate, coordinated, and culturally competent (Medical Home Initiative for Children with Special Needs Project Advisory Committee, American Academy of Pediatrics, 2002), which means that they may not be receiving comprehensive or coordinated healthcare even before the transition to adulthood (Brachlow, Ness, McPheeters, & Gurney, 2007). In fact, prior research has shown that youth with ASD were more likely to receive healthcare transition services if they had a medical home (Rast et al., 2018). However, many pediatric providers struggle to successfully transition their patients with ASD due, in part, to a lack of adult healthcare providers with adequate training or comfort in caring for patients with ASD (Kuhlthau, Warfield, Hurson, Delahaye, & Crossman, 2015). A recent large-scale study of healthcare utilization found that youth with ASD received significantly less outpatient healthcare services over time from adolescence into adulthood, while the use of emergency department services remained stable (Nathenson & Zablotsky, 2017). Not surprisingly, adults with ASD and their families experience significant unmet healthcare needs (Nicolaidis et al., 2013). Together, these findings indicate significant gaps in healthcare delivery for youth and young adults with ASD.
Barriers to healthcare for youth and young adults with ASD
There are a number of factors that may interfere with healthcare access and quality for youth and young adults with ASD. Caregivers of youth with ASD report a number of barriers to accessing care during the transition period. In a survey of 183 caregivers, most (51%) lacked information about the healthcare transition process, and almost one-third reported difficulty finding an adult primary care provider (PCP) with knowledge of ASD and who would be willing to accept their child as a patient. An additional 20% reported lack of coordination and communication between the pediatrician and adult PCP (Kuhlthau et al., 2016). Similar themes were reported by young adults with ASD and their caregivers during a qualitative study of healthcare transition, including lack of preparation for transition and a lack of education and sensitivity about autism among adult providers (Cheak-Zamora & Teti, 2015).
Adults with ASD report additional barriers related to both healthcare access and healthcare delivery. In a survey of 40 adults with ASD, the majority reported not knowing where to find healthcare services and feeling too overwhelmed by the steps to seek services. An additional 47% reported having had negative experiences with healthcare professionals in the past. Those who had co-occurring mental health and medical conditions reported significantly less satisfaction with their healthcare services (Vogan, Lake, Tint, Weiss, & Lunsky, 2017). In a 2013 study, adults with ASD reported significantly less overall satisfaction with their healthcare providers as compared to those without ASD. Notably, only 57% reported that their healthcare providers understood what they were trying to communicate and 40% reported feeling that they could not trust their healthcare provider to take care of their healthcare needs (Nicolaidis et al., 2013). In a more recent 2017 study, the most common healthcare barriers reported by adults with ASD included fear or anxiety, trouble processing information quickly, concerns about costs, sensory issues, and difficulty communicating with providers (Raymaker et al., 2017). Similarly, adults with ASD participating in a focus group reported that their most significant healthcare barriers included sensory sensitivity and stress, anxiety due to waiting, and difficulties with communication and trust in the physician (Saqr, Braun, Porter, Barnette, & Hanks, 2018).
As noted above, there are very few healthcare providers with expertise in caring for patients with ASD, and even fewer who are able to provide adult healthcare services. Regarding provider perspectives, only 40% of 376 adult PCPs surveyed had any patients with ASD and very few had any training in caring for patients with ASD (Bruder et al., 2012). In a more recent study of 922 providers, 77% described their knowledge and skill at providing care to patients with ASD as being “poor” or “fair,” and only 13% felt that they had adequate tools, referral resources, or practice models to accommodate patients with ASD. Follow-up interviews with a subsample of providers revealed a perceived need for training, resources, and specific accommodations to enhance communication and comfort during clinic visits (Zerbo et al., 2015). Similar results were found in a qualitative study of 10 PCPs, including lack of education and training in ASD. Systems-level challenges to providing care for adults with ASD included a lack of available services, supports, and healthcare providers. Providers also reported challenges related to communication and the patients’ comfort with the clinic environment (Warfield et al., 2015).
Overall, there is considerable evidence that youth and adults with ASD face significant healthcare disparities. Although PCPs are well-placed to provide timely and responsive healthcare services, a general lack of knowledge about caring for patients with ASD appears to be a key barrier to high-quality healthcare throughout the transition from adolescence to adulthood. Thus, training PCPs in best-practice approaches to transition and autism-specific healthcare delivery may improve both healthcare access and quality for youth and young adults with ASD.
A novel technology-enabled framework for provider training
The Extension for Community Healthcare Outcomes (Project ECHO) model represents a particularly innovative framework that leverages technology to provide both training and ongoing mentorship to community-based PCPs (Arora et al., 2010). Project ECHO was originally developed to improve healthcare for patients with hepatitis C by training and mentoring PCPs in rural communities using videoconferencing technology (Arora et al., 2010; Arora et al., 2011). The model was recently adapted to improve care of children with ASD by training PCPs in best-practice approaches for screening, diagnosis, and management of ASD and common co-occurring conditions (Mazurek, Brown, Curran, & Sohl, 2017; Mazurek, Curran, Burnette, & Sohl, 2019). The ECHO Autism model uses videoconferencing to connect local PCPs (“spokes”) to an interdisciplinary team of experts (“hub”) during bimonthly ECHO Autism clinics. Each clinic consisted of a brief didactic presentation, case-based learning, and collaborative guided practice. During each clinic, PCPs present their own cases for discussion, recommendations, and guided practice. The model has demonstrated success in improving PCP self-efficacy and use of autism screening tools and resources for children with ASD (Mazurek et al., 2017; Mazurek et al., 2019).
The purpose of this pilot study was to develop and test an adapted version of the ECHO Autism model, focused specifically on training PCPs in best-practice care for transition-age youth and young adults with ASD (ECHO Autism Transition). Our goals were to evaluate the feasibility of the adapted model and to examine the effects of participation in ECHO Autism Transition on PCP self-efficacy, knowledge, and experiences in providing care for youth and young adults with ASD.
Methods
Participants
PCPs from across the United States were recruited for participation in the ECHO Autism Transition pilot project. A combination of recruitment strategies were used including word-of-mouth recruitment through professional networks of study team members, and sending flyers to distribution lists of national healthcare professional organizations (e.g. the American Academy of Pediatrics and the American Academy of Developmental Medicine and Dentistry). Eligibility criteria included current practice as a PCP, including pediatrics, family medicine, internal medicine, or advance practice nursing (i.e. nurse practitioner or physician assistant), and an active medical license in the state of practice. Trainees (e.g. medical student, intern, resident, or pre-professional trainee) and subspecialists (e.g. psychiatrists, neurologists, and developmental and behavioral pediatricians) were not eligible to participate.
A total of 16 participants initially enrolled in the study. Of those, one attended only one session and was later determined to be ineligible (due to subspecialist status as a developmental and behavioral pediatrician), two discontinued participation due to changes in clinic schedule (after attending two sessions), and one participant relocated across the state as a result of a family emergency after attending nine sessions. One participant completed the program but did not complete all pre-training measures. This resulted in a sample of 12 who completed the ECHO Autism Transition program, 11 of whom completed both pre- and post-training assessments. Participants were provided with a monetary incentive for survey completion at each time point.
ECHO Autism Transition model
ECHO Autism Transition clinics were held for 1 h every week for 3 months (from October 2018 to January 2019). Each clinic provided training and mentorship in best-practice care for youth and young adults with ASD, and consisted of brief didactics, case-based learning, and guided practice. During each clinic, all PCP participants (“spokes”) were connected to one another and to an interdisciplinary team of experts (“hub”) via secure multipoint videoconferencing technology. All members of the expert hub team had specific expertise in ASD, and included an adult neurologist, an internal medicine-pediatrics physician, a clinical psychologist, a neurologist/sleep specialist, a parent advocate/transition specialist, and a young adult self-advocate with ASD.
The ECHO Autism Transition curriculum focused on understanding ASD in youth and young adults, supporting individuals and families throughout the transition process, and providing evidence-based care. Content was based on the current available evidence and best-practice approaches for healthcare for youth and adults with ASD (e.g. Azad, Singh, Kalb, Pinkett-Davis, & Landa, 2019; Baghdadli et al., 2018; Holmes, Strassberg, & Himle, 2019; Lee, Heerwagen, & Loftin, 2019; Nicolaidis, Kripke, & Raymaker, 2014; Roux et al., 2015; Sala, Hooley, Attwood, Mesibov, & Stokes, 2019; Saqr et al., 2018; Seltzer et al., 2004; Walter, Johnson, & Schomberg, 2009). Didactic topics included the following: What is Autism?, Psychiatric Co-occurring Conditions, Medical Co-occurring Conditions, Behavior Management in Primary Care, Supporting Families through Transition to Adulthood, Healthcare Transition Planning (Role of the PCP), Life Skills Development, Supporting the Self-Advocate, Guardianship, Special Education Transition to ADA, Housing and Community Supports for Adults with Autism, and Relationships and Sexuality in Autism. Evidence-based autism and transition resources, toolkits, and community-based options for treatment, education and support were integrated throughout each ECHO Autism Transition clinic.
Each ECHO Autism Transition clinic also included a de-identified case presented by one of the PCP participants for discussion, providing opportunities for shared learning, peer support, and mentoring. The expert hub team also provided verbal and written feedback and recommendations for each case presented, supporting PCPs as they maintained responsibility for care of their patients. Resources and toolkits were shared and stored through a secure online portal/shared folder.
Measures
Participants completed questionnaires at pre-training (prior to attending the first ECHO Autism Transition session) and post-training (after completion of the 3-month program). Pre- and post- data were linked using participant-generated ID codes. Questionnaires were completed online using a web-based data collection system (REDCap). De-identified case presentation forms were also examined.
Demographic information
A demographic survey was administered at pre-training to obtain information about participants’ age, race, ethnicity, sex, provider type, practice setting, and current and previous ASD experience.
Practice patterns
Additional survey questions at both pre- and post-training assessed practice patterns, patient population, and perceptions of providing care to youth and young adults with ASD. Participants were also asked to respond to a 10-item checklist of possible barriers faced when treating adolescents and young adults with autism in their practices. Participants were instructed to check all items that apply. Checklist items included the following: lack of time, lack of support from administration, inadequate reimbursement, difficulty communicating with patients with autism and/or caregivers, lack of knowledge about autism, lack of confidence in (the provider’s) ability to work with patients with autism, lack of access to autism specialists, lack of providers with expertise in caring for young adults with autism, and other. At post-training only, additional open- and closed-ended questions were included to assess participants’ perceptions of the ECHO Autism Transition program, perceived changes in practice and changes in relationships and interactions with patients with autism and their families.
Self-efficacy
Self-efficacy was assessed at both pre- and post-training using an adapted version of the Primary Care Autism Self-Efficacy (PCASE) Survey (Mazurek et al., 2017). For the current study, item content was adapted for transition-age youth and young adults. Participants rated their degree of confidence in their ability to provide effective care across 56 items, ranging from 1 (no confidence) to 6 (highly confident/expert). Item scores are totaled to yield a total score and the following subscale scores: (a) Autism Understanding (7 items), (b) Referral and Resources (10 items), (c) Healthcare Transition (9 items), (d) Managing Medical Comorbidities (10 items), (e) Managing Psychiatric Symptoms (10 items), and (f) Additional Aspects of Care for Autism (7 items).
Knowledge test
Knowledge about caring for youth and young adults with autism was assessed at pre- and post-training using a 29-item test developed specifically for the current study. Content areas included autism identification, psychiatric comorbidities, medical comorbidities, healthcare transition, and management of additional autism-specific needs.
Satisfaction
At post-training only, participants completed a 10-item Satisfaction Survey to assess overall satisfaction with ECHO Autism Transition program (each item was rated on a 5-point scale, with higher scores indicating greater satisfaction).
Data analysis plan
Descriptive statistics (i.e. mean, standard deviation, and percentage) were conducted to characterize variables of interest. Due to the small sample size and lack of normal distribution of the data, pre- to post-training changes in PCP self-efficacy, knowledge, and number of perceived barriers were examined using a non-parametric approach, the Wilcoxon signed-ranks test. Open-ended text-based responses to the questions about changes in practice and patient and family relationships were examined using qualitative methods. Two authors reviewed all the written responses and formulated initial impressions of the data. A constant comparative method was used (Boeije, 2002), in which each additional response was compared with previous categories until saturation was reached. Initial impressions of thematic categories were discussed by both the authors until consensus was reached on the final categories and codes.
Results
Provider and practice characteristics
Provider characteristics are shown in Table 1. Although 37% were pediatricians, the majority of providers (75%) cared for adults (18 years and older) in their practices. Most (56.3%) reported having had at least some previous training on autism.
Participant characteristics.
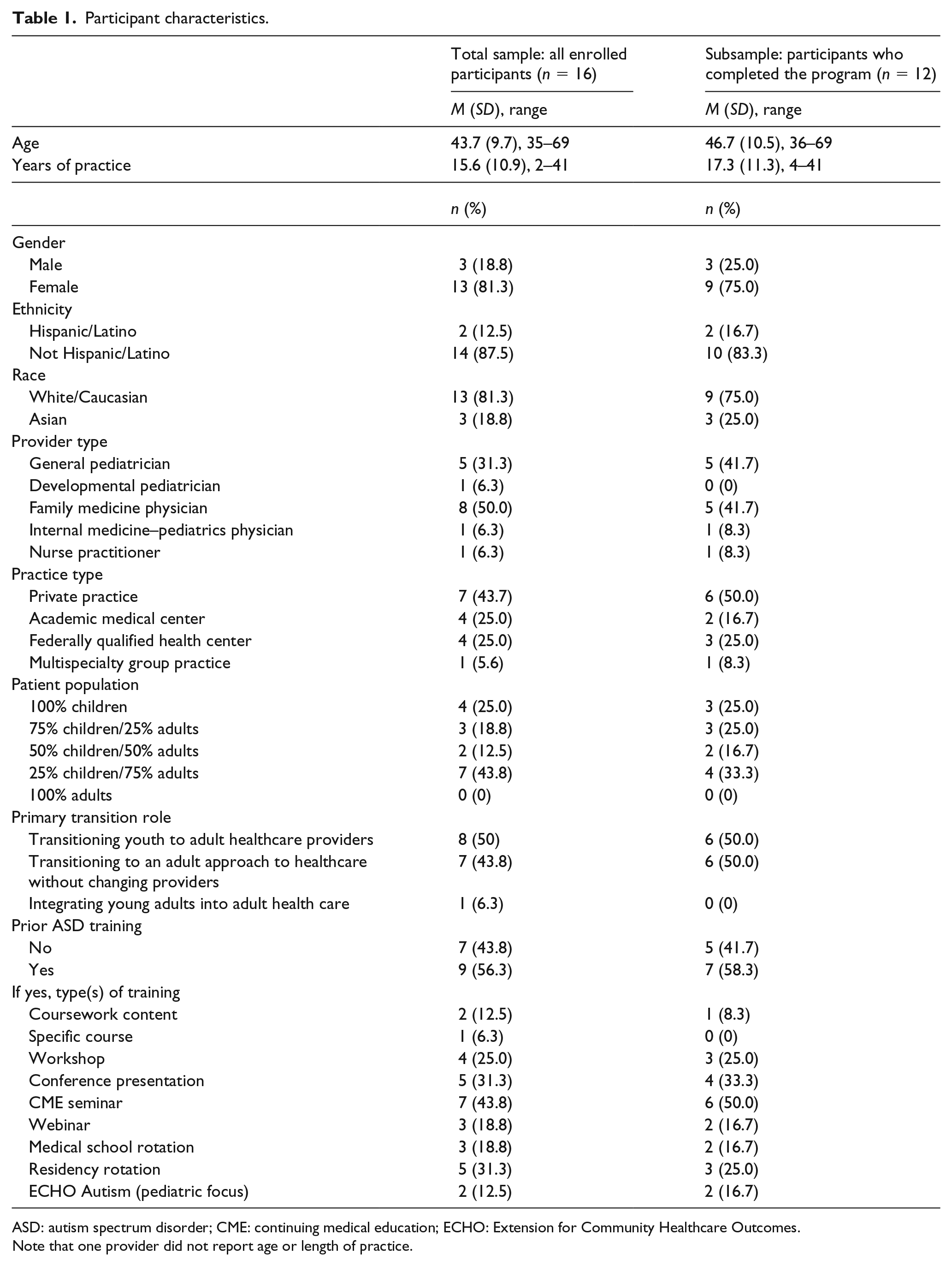
ASD: autism spectrum disorder; CME: continuing medical education; ECHO: Extension for Community Healthcare Outcomes.
Note that one provider did not report age or length of practice.
Cases presented
A total of 11 de-identified cases were presented by participants for discussion during the pilot program, providing additional information about the specific types of patients for whom PCPs needed additional support and guidance. The cases were mostly male (54.5%), ranging in age from 15 to 31 years (M = 19.9, SD = 5.2). All cases (100%) were accompanied to their appointment by a caregiver (81.8% mother), and 100% were living at home with parent(s)/caregiver(s). A total of 27% of cases were nonverbal, 45.4% had some language, and 27.3% were verbally fluent. The chief presenting concerns included planning for the future (63.6%), mental and behavioral health (36%), medication management (18%), physical health (18%), family coping (9%), and romantic relationships (9%).
Self-efficacy, knowledge, and perceptions of practice change
Regarding improvements in PCP self-efficacy in caring for patients with ASD, the Total Self-Efficacy raw scores improved significantly from pre-training (M = 181.9, SD = 54.0) to post-training (M = 210.5, SD = 38.9; Z = −2.93, p = 0.003), as did scores in almost all subdomains, including Referral and Resources (Z = −2.13, p = 0.033), Healthcare Transition (Z = −2.94, p = 0.003), Managing Medical Comorbidities (Z = −2.08, p = 0.038), Managing Psychiatric Symptoms (Z = −2.07, p = 0.038), and Additional (Z = −2.76, p = 0.006). Improvements were also noted in the Autism Understanding domain, but this difference did not reach statistical significance (Z = −1.91, p = 0.057) (see Figure 1).

Improvement in self-efficacy subscale scores.
Participants demonstrated slight, but not statistically significant, improvements in overall knowledge (as assessed by the Knowledge Quiz) from pre-training (M = 67.3%, SD = 11.5%) to post-training (M = 71.9%, SD = 12.6%; Z = −1.79, p = 0.074).
The total number of perceived barriers to caring for youth/young adults with ASD did not change significantly from pre-training (M = 4.2, SD = 1.9) to post-training (M = 3.7, SD = 1.6; Z = −1.25, p = 0.212). Figure 2 depicts the number of providers reporting specific types of barriers at both pre- and post-training.
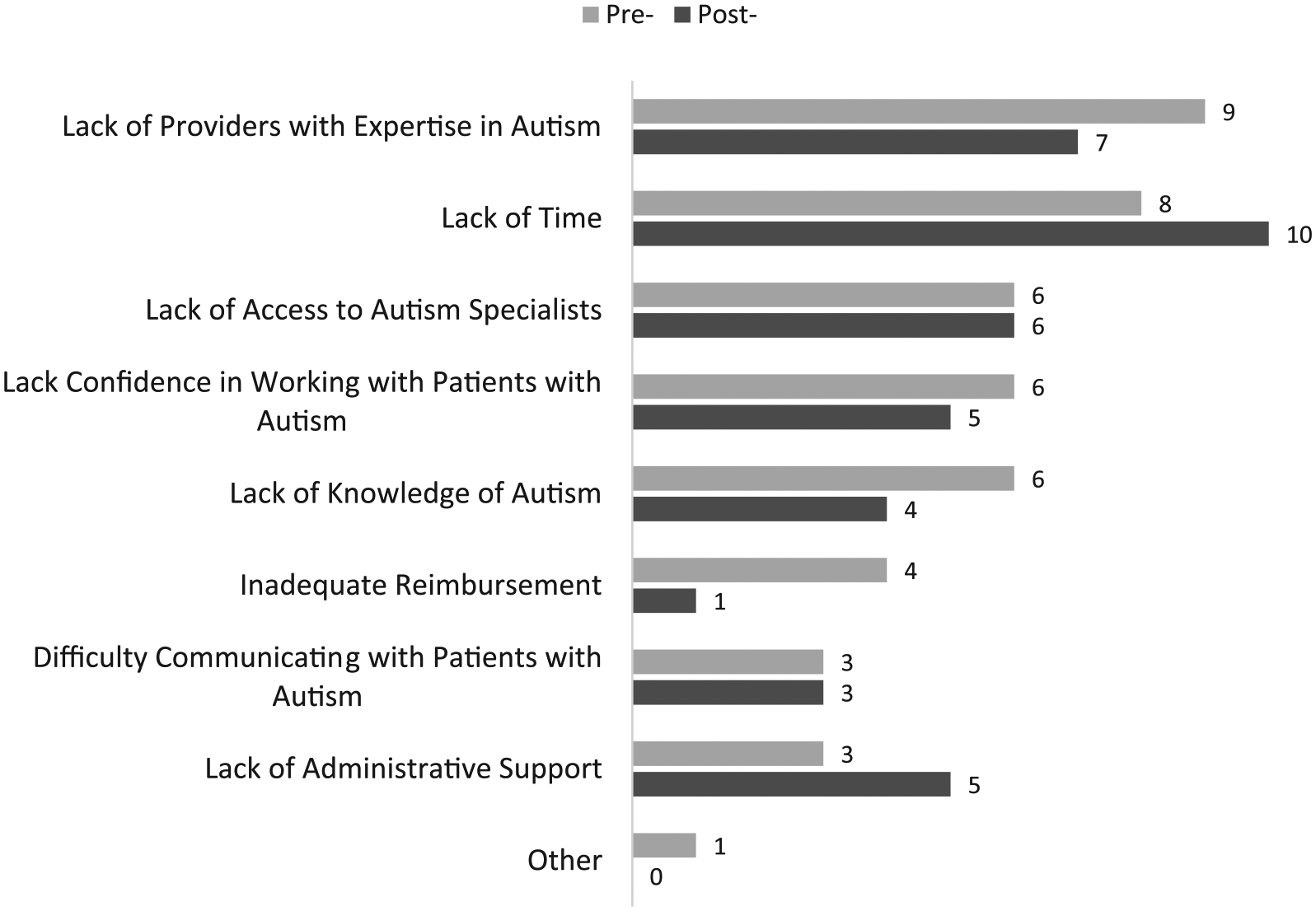
Perceived barriers to caring for patients with autism at pre- and post-training (number of providers reporting each type of barrier among those with complete data, n = 11).
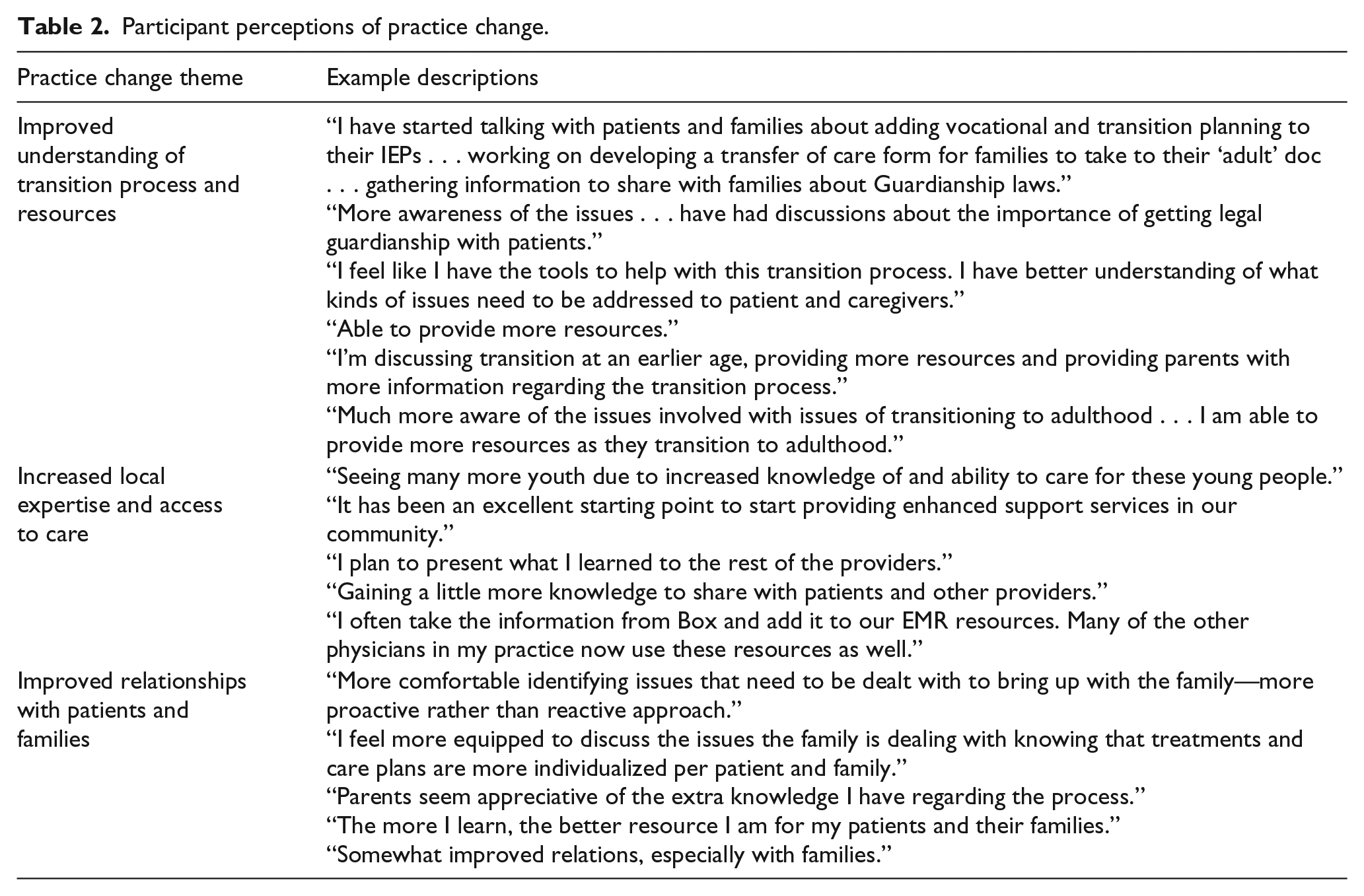
Most (75%) of the participants reported that they had changed their practice as a result of participation in the program, 67% reported changes in relationships and interactions with patients and autism and their families, and 100% reported that they would be interested in working with youth/young adults with autism in the future and that the program had a positive impact on their communities. In addition, 67% reported feeling less professionally isolated as a result of participation in the program. Qualitative responses to the questions about changes in practice and patient and family relationships are presented in Table 2.
Participant perceptions of practice change.
Satisfaction with the program
Participants reported high satisfaction with ECHO Autism, with an average rating of 1.37 (SD = 0.55) across all questions, with “1” indicating the highest satisfaction (see Table 3).
Participant satisfaction with the ECHO Autism Transition program (n = 12).
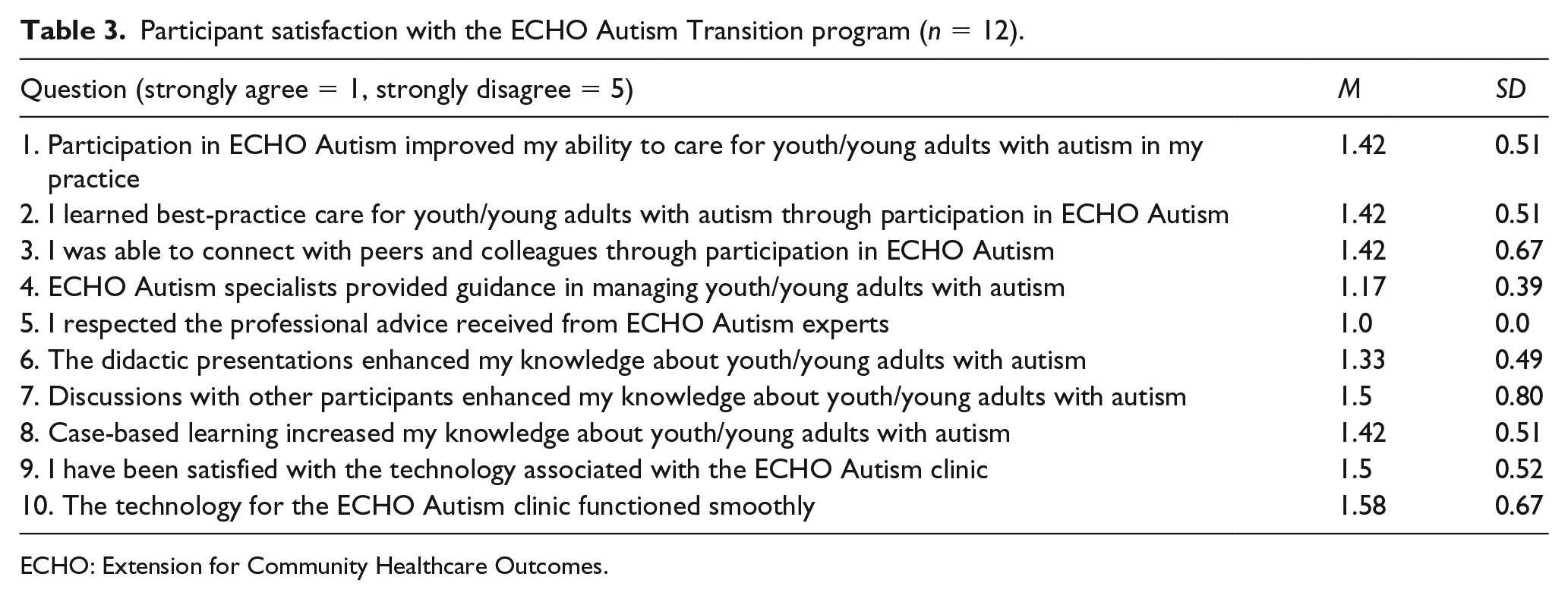
ECHO: Extension for Community Healthcare Outcomes.
Discussion
Youth and young adults with ASD experience significant unmet healthcare needs during the transition to adulthood (Brachlow et al., 2007; Kuhlthau et al., 2016; Nathenson & Zablotsky, 2017) and PCPs lack training and confidence in their ability to care for patients with ASD (Bruder et al., 2012; Zerbo et al., 2015). Equipping PCPs with additional support and resources to provide best-practice care for youth and young adults with ASD has the potential to improve overall health and quality of life during this critically important period. The results of this pilot study indicate that the ECHO Autism Transition program may represent a feasible approach for enhancing healthcare for transition-age youth and young adults with ASD.
Overall, PCPs participating in the program demonstrated improvements in their self-efficacy regarding providing effective care for youth and young adults with ASD in their practices. Importantly, PCPs felt significantly better equipped to help their patients with ASD navigate the transition process, manage co-occurring medical and mental health conditions, and access available resources. Most PCP participants also reported direct changes in their practice and changes in interactions with patients with ASD and their families as a result of the program. An examination of responses to open-ended questions indicated that PCPs observed particular improvements in their understanding of the transition process, their knowledge of appropriate resources, and their ability to serve as a local expert for patients with ASD and their families.
All reported an interest in working with patients with autism in the future, highlighting the potential of this program for increasing local access to care.
These findings are important, given the growing population of transition-age youth and young adults with ASD, and the complex medical and mental health challenges they face (Croen et al., 2006; Davignon et al., 2018; de Bruin et al., 2007; Levy et al., 2010; Simonoff et al., 2008; Soke et al., 2018). A review of the de-identified cases presented by PCPs to the ECHO Autism Transition team reflects these challenges. The majority of cases (i.e. youth and young adults with ASD; 63%) needed help with future planning. Mental and behavioral health represented the second most common presenting concern, followed by physical health and medication management. Equipping PCPs with resources and knowledge to more effectively manage these issues may significantly improve overall health and quality of life among youth and young adults with ASD.
Despite significant improvements in PCP self-efficacy and perceived changes to practice, we did not observe significant improvements in knowledge. The knowledge quiz was developed specifically for this study prior to the implementation of the pilot program, and was based on the planned didactic schedule and anticipated discussion topics. As such, it covered a wide range of topics relevant to understanding ASD and providing care for a range of common medical, mental health, and transition-related needs. One possible reason for lack of knowledge improvement may have been that the ECHO Autism Transition program was too brief to provide thorough training on all these topics. Another alternative is that the content covered had a slightly different emphasis than originally planned when the knowledge test was designed. Since much of the learning within the ECHO model is case-based, meaning that it occurs within the context of case discussions, the emphasis may have been driven by the needs of the community rather than the pre-planned curriculum. Finally, many participants (56%) reported having some prior training in ASD prior to participation in the program, as compared to only 36% of PCPs in previous research (Bruder et al., 2012). As such, it is possible that the participants in the current study demonstrated relatively higher levels of baseline knowledge (and less room for growth) than the larger population of PCPs. Future studies of the ECHO Autism Transition model should carefully evaluate key areas of knowledge to continue to examine the effectiveness of the model in participants with and without prior training in ASD. Further refinement of the curriculum may also be helpful to maximize learning and mastery of key concepts.
Participation in ECHO Autism Transition did not appear to reduce the overall number of perceived barriers to caring for youth/young adults with ASD. However, a closer examination of specific barriers indicates that fewer PCPs reported barriers related to lack of knowledge or expertise in autism at post-training. On the other hand, by the end of the program, more PCPs reported that a lack of time and lack of administrative support were barriers to caring for patients with ASD. While this may seem counterintuitive, this finding may actually reflect an increased understanding of the complex challenges faced by transition-age youth and young adults inside and outside of healthcare settings, as well as a greater appreciation for the need for more comprehensive and individualized medical care. Because providing best-practice care for this population may require longer office visits, special accommodations within the clinic environment, and coordination of various services, it is not surprising that PCPs may encounter new administrative challenges as they begin to implement practice change. These findings also underscore that PCP education alone may not be sufficient to overcome all barriers to healthcare for individuals with ASD, and suggest that additional efforts may be required to enhance the broader healthcare system. For example, reimbursement and administrative models that support the additional time required for management of complex patients would be helpful. Building the workforce of professionals across disciplines with expertise in ASD would also help to improve access to comprehensive and coordinated care, community resources, and other needed supports. Given the prevalence and complexity of mental health concerns among youth and adults with ASD (Croen et al., 2015; Davignon et al., 2018), efforts to improve the mental health system and to equip mental health providers with additional knowledge and skills to support individuals with ASD are critically important.
Limitations and future directions
The current pilot study was limited by a small sample of participants, a lack of control or comparison group, and reliance on self-report measures rather than direct assessments of practice change. In addition, the sample may not be representative of the larger population of PCPs, as participants demonstrated enough interest in ASD to voluntarily participate in the training program. Most had at least some previous training in ASD. Further evaluation of the ECHO Autism Transition program is needed to directly evaluate its efficacy and effectiveness in improving care for youth/young adults with ASD. Larger and more representative samples, direct assessments, and examination of patient outcomes (including perspectives of patients and families), would be particularly informative.
Despite these limitations, these preliminary results indicate that the ECHO Autism Transition model is feasible and holds promise for improving PCP confidence and interest in working with youth and young adults with ASD. However, further refinements and evaluation of the model may be helpful for enhancing the scope and impact on practice.
Footnotes
Acknowledgements
The authors are extremely grateful to all the primary care providers who participated in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under cooperative agreement UA3 MC11054—Autism Intervention Research Network on Physical Health. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government. This work was conducted through the Autism Speaks Autism Treatment Network serving as the Autism Intervention Research Network on Physical Health.