
Abstract
The illness behavior of patients with medically unexplained physical symptoms (MUS) depends largely on what the patient believes to be the cause of the symptoms. Little data are available on the illness attributions of patients with MUS in China. This cross-sectional study investigated the illness attributions of 96 patients with MUS in the outpatient departments of Psychosomatic Medicine, biomedicine (Neurology, Gynecology), and Traditional Chinese Medicine in Shanghai. Patients completed the Illness Perception Questionnaire (IPQ) for illness attribution, the Screening Questionnaire for Somatoform Symptoms, the Hospital Anxiety and Depression Scale for emotional distress, and questionnaires on clinical and sociodemographic data. The physicians also filled out a questionnaire regarding the cause of the illness (IPQ). In contrast to previous research, both physicians and patients from all three areas of medicine most frequently reported “psychological attributions.” The concordance between the physicians’ and the patients’ illness attributions was low. Emotional distress was an important predictor of psychological attributions. Further research should include large-scale studies among patients from different regions of China and qualitative studies to deepen our understanding of cultural influences on illness attribution.
Keywords
Medically unexplained symptoms (MUS) and functional somatic syndromes (FSS) are terms used to describe the presence of symptoms for which there is no detectable physical illness or for which the intensity and variety of symptoms cannot be adequately explained based on an existing organic disease (Guthrie, 2008; Henningsen, Zipfel, & Herzog, 2007; Peveler, Kilkenny, & Kinmonth, 1997). The terminology used to describe these problems is unsatisfactory. The term MUS is neutral and does not carry a risk of stigmatization of the patient. The term has an advantage in that it does not focus primarily on the patient and his/her physical or mental disease or disorder, but rather describes a problem situation: the dilemma of the physician not being able to sufficiently explain the patient’s symptoms through the usual means of conventional medicine (Kirmayer, Groleau, Looper, & Dao, 2004). In this article, the term MUS is used in accordance with the four core criteria of somatization as defined by Lipowsky (1988): (a) one or more somatic symptoms that (b) lack an adequate medical explanation, (c) cause patient distress, and (d) prompt health care-seeking behavior. This does not presume that the presentation of distressing somatic symptoms is evidence of a psychiatric disorder. However, there is a large overlap between MUS and the diagnostic category of somatoform disorders, anxiety disorders, and depressive disorders.
In primary care in Western countries, up to one third of all symptoms remain medically unexplained even after extensive diagnostic investigations (Kroenke & Mangelsdorff, 1989). In fields such as gynecology, neurology, gastroenterology, and rheumatology, international studies report that no organic cause can be found for symptoms in 30% to 70% of patients (Nimnuan, Hotopf, & Wessely, 2001; Reid, Wessely, Crayford, & Hotopf, 2001). These include common physical symptoms such as dizziness, fatigue, stomach pain, back pain, and headaches. Patients with high levels of these somatic symptoms have been shown to be disproportionately frequent users of health care services (Barsky et al., 2001; Smith, Monson, & Ray, 1986).
International studies have shown that there are no systematic cultural differences regarding the prevalence of somatoform disorders between developing and Western industrialized nations (Gureje, Simon, Ustun, & Goldberg, 1997; Kirmayer & Young, 1998; Simon, von Korff, Piccinelli, Fullerton, & Ormel, 1999). Across all ethno-cultural groups, a quarter of all patients in primary care meet one or more definitions of somatization, functional syndromes, or somatoform disorder (Peveler et al., 1997; Simon et al., 1999). However, specific functional syndromes such as irritable bowel syndrome seem to be more common in Western cultures than in non-Western ones (Chang et al., 2006).
There are clear cultural differences regarding illness behavior and illness perception in MUS (Gureje et al., 1997; Janca, Isaac, Bennett, & Tacchini, 1995; Karasz, Dempsey, & Fallek, 2007). The symptom presentation of depressive complaints seems to especially differ between cultures: several studies have shown that patients in Asia with depression report somatic symptoms significantly more often than psychological symptoms (Karasz et al., 2007; Kleinman, 1982; Parker, Cheah, & Roy, 2001; Ryder et al., 2008) or anxiety (Hoge, Tamrakar, & Kelly, 2006). To date, the reasons for this difference have remained unclear. More widely discussed are the strong stigmatization of mental disorders in China and the resulting tendency to deny psychological symptoms and instead focus primarily on somatic symptoms during physician consultation (Kirmayer & Young, 1998). Newer studies show, however, that Chinese patients are indeed willing to talk about psychosocial distress when appropriate opportunities are offered in the physician–patient consultation (Lee, 1998). A World Health Organization (WHO) study (Simon et al., 1999) showed that patients who had continuous access to a primary care physician were more likely to talk about their psychosocial problems and did not focus as much on somatic symptoms. In a study comparing patients with depression in China and Canada (Ryder et al., 2008), patients reported more somatic symptoms to an unfamiliar research assistant as part of a standardized clinical interview, and less if they privately completed a questionnaire.
Dealing with perceived symptoms depends in large part on the cause to which symptoms are attributed (Dean, 1986; Duddu, Isaac, & Chaturvedi, 2006). In particular, the seeking of health care by MUS patients is influenced by symptom attribution (Barsky et al., 2001; Kirmayer, Young, & Robbins, 1994; Rief & Nanke, 1999; Robbins & Kirmayer, 1991). Symptom attribution itself depends on three major factors (Bishop, 1987; Kelley & Michela, 1980; Shaver, 1975): (a) situational factors such as environmental conditions, lack of sleep, or overexertion; (b) dispositional causes such as physical disease or constitutional weakness; and (c) psychological factors such as emotional distress, e.g., family problems, bad mood, or negative thinking. Moreover, the number of symptoms and the number of physician visits influence the symptom attributions of patients with MUS (Kirmayer et al., 1994; Rief & Sharpe, 2004). The specific presentation of symptoms and the patient’s attribution influence treatment strategies (Greer, Halgin, & Harvey, 2004) and predict whether or not the physician recognizes depressive and anxiety disorders (Kessler, Lloyd, Lewis, & Gray, 1999; Kirmayer, Robbins, Dworkind, & Yaffe, 1993).
Conversely, patients’ presentations of symptoms and illness attribution also depend on the attitude of the treating physicians concerning psychosocial aspects. Three types of presentation have been described (Bridges & Goldberg, 1985; Kirmayer & Robbins, 1991) according to their attribution: (a) “initial somatizers” present exclusively somatic symptoms but, when asked what they think is causing their symptoms, readily attribute them to psychosocial factors; (b) “facultative somatizers” only acknowledge psychosocial causes when they are directly asked about them: “Do you think that emotional distress could have caused your symptoms?”; and (c) “true somatizers” reject every psychosocial explanation even when they are directly asked. Thus, some of these patients clearly seem willing to incorporate psychosomatic attributions, such as stress, family problems, and childhood experiences into their illness concept (Nimnuan et al., 2001).
In a U.S. study, patients with a “chronic psychosomatic illness” reported multicausal explanations, linking their illness to the physical, psychological, and social aspects of their life (Helman, 1985). In a study on 100 primary care patients in Hong Kong with medically unexplained fatigue lasting 6 months or longer, most patients attributed the cause of their illness to psychosocial distress (Lee et al., 2000).
Organic and psychological explanations often exist side by side for one and the same symptoms (Lundh & Wangby, 2002; Rief, Nanke, Emmerich, Bender, & Zech, 2004). Patients with somatoform symptoms with no emotional distress reported more organic attributions and higher “vulnerability,” while patients with depression and anxiety symptoms reported more psychological attributions (Kessler et al., 1999; Kirmayer & Robbins, 1991; Kirmayer et al., 1994; Lundh & Wangby, 2002; Rief et al., 2004).
Organic attribution of somatoform disorders is associated with a worse outcome and persistent somatization (Henningsen, Jakobsen, Schiltenwolf, & Weiss, 2005). In a qualitative study on the illness models of Canadian immigrants with MUS and their physicians, Dao (2006) showed that, similar to the study by Rief et al. (2004), MUS patients who were interviewed did not name one explanation for their symptoms but rather presented numerous explanatory models of varying complexity. These explanations often coexist even though they contradict one another. Moreover, they are sometimes incomplete, not necessarily causal, and are transformed and rejected by the patients during the course of the interviews. For the most part, physicians are not at all familiar with the patients’ complex illness models, and their assessment of whether the patients would accept or reject psychosocial explanations is inaccurate (Dao, 2006).
Physicians’ explanations for medically unexplained symptoms also vary. A Swedish study reported that most general practitioners attribute patients’ MUS to emotional stress, referring to a wide range of contributing factors such as the patient’s psychological fragility, lack of medical knowledge, unrealistic expectations of medicine, traumatic social changes, secondary gain from sick leave, insufficient social support, stressful life events, and dissatisfaction with one’s position in modern society (Woivalin, Krantz, Mantyranta, & Ringsberg, 2004).
Cultural background
Various studies show that symptoms and illness attributions, as well as physicians’ and the patients’ illness categories vary and may be culturally specific (Kirmayer, 2005; Kirmayer & Sartorius, 2007; Kirmayer et al., 1994). Every form of causal explanation of symptoms is embedded in a cultural worldview and way of life. Cultural concepts of the self and the individual are especially important for psychological attributions (Kirmayer et al., 1994). White (1982) emphasizes situation-dependent explanations for emotional distress given by the Chinese over individual-centered explanations from North American patients.
Today, Western culture, Western science, and Western technology affect many aspects of everyday life in China. Nevertheless, certain models from China’s past regarding the human body have been carried over to the present. The lore of the power of ancestral spirits and demons goes back to prehistoric times. This belief that demons cause illness and harm in many other areas of everyday life has survived to the present day in certain segments of China’s population. Similarly old is the belief that illness is caused by the invasion of microorganisms, referred to today as bacteria or viruses (Unschuld, 1985).
Because Traditional Chinese Medicine (TCM) lacks the concept of the psyche as an entity, it also lacks independent psychological illness models. However, psychological concepts have been documented in Chinese medical history and verified in case descriptions. Within the framework of medicine in the educated upper class after the Han Dynasty, which can be considered the forerunner of present-day TCM, various human emotional reactions are conceptually linked to the organs. According to this idea, organ dysfunction manifests itself as an emotional condition (anxiety, rage, sadness, etc.), and by the same token, an excess of emotion damages the respective organ and thus causes the entire organism to break down (Ots, 1990; Scheid, 2002). In addition to the outside (bioclimatic) factors, emotions are considered to be the inner illness-causing factors. Throughout China’s history, however, the assessment and treatment of emotional conditions (i.e., psychology and psychotherapy) took place largely outside of what we call “medicine” today; namely, within the areas of witchcraft, divinatory practices, astrological counsel, and similar rituals. Due to the Westernization and standardization of Chinese medicine within the context of China’s modernization discourse, it is clear from the institutionalization of a large portion of Western biomedicine in medical training that the classical explanatory models of psychological conditions are becoming less relevant (Scheid, 2002). The presentation of physical symptoms in Chinese culture does not imply a somatic attribution of the symptoms. Chinese utilize body-oriented verbal forms of expression in an all-encompassing manner to communicate every aspect of personal or social worries and problems (Tung, 1994).
One somatic syndrome recognized in China is shenjing shuairuo (SJSR), a translation of the term “neurasthenia” which was introduced in the United States by the neurologist George Beard in 1869. Neurasthenia was very popular at the time and included 30 or more symptoms. The diagnostic term spread around the world, and it was referred to as SJSR in China and shinkei suijaku in Japan. The origin of the condition was regarded as organic, but was generally treated with psychological and social therapies (Kleinman, 1982; Lin, 1989; Shixie, 1989; Yan, 1989, 1991).
Patients whose clinical picture included sleep disorders, dizziness, headaches, concentration disorders, rapid exhaustion, and many other similar symptoms very often received this diagnosis (Lee, 1998; Lee & Wong, 1995; Yan, 1989). SJSR is seen as an expression of a high level of stress in individuals who are especially predisposed to it (Lee & Wong, 1995). SJSR includes somatic, cognitive, and emotional symptoms. In contrast to depression, this diagnosis is considered less stigmatizing. Thus, 87 of the 100 patients in Kleinman’s (1982) study fit the diagnosis of major depression, but the term was used on none of the patients. Kleinman described SJSR as a socially and culturally shaped type of somatization (1982) and reported that while patients began their illness narratives with physical symptoms they repeatedly extended their narrative into recollections of past psychosocial distress (Kleinman, 1995).
The concept of SJSR fit well with traditional Chinese ideas about the cause of illness based on disrupted harmony of the vital organs and an imbalance of qi (Cheng, 1989). Today, however, the term is used only by neurologists or general practitioners, and predominantly in rural areas. Psychiatrists orient themselves toward DSM-IV and ICD-10 in diagnoses of depression or somatoform disorders. In 2001, the concept of somatoform disorders was introduced into the Chinese Classification of Mental Disorders (CCMD III). At the same time, hierarchical rules were established permitting the diagnosis of SJSR or neurasthenia only after the exclusion of depressive disorders and anxiety disorders. Neurasthenia received code 43.5 in the CCMD-III and therefore ranked behind other forms of somatoform disorders. As a result, neurasthenia is now rarely diagnosed by Chinese psychiatrists except in neurological and general hospitals outside the major urban centers, where the diagnosis is still in use (Lee & Kleinman, 2007).
Until now there have been only a few studies on the illness perception and illness attribution of patients with MUS in China (Kleinman, 1980, 1982; Lee et al., 2000). Our study is the first to compare the illness attribution of patients as it occurs in psychosomatic medicine, biomedicine, and TCM.
The research questions of our study are as follows:
What explanations do the patients and attending physicians give regarding the cause of the patients’ illness? We expected that patients and physicians would report a combination of physical causes, external contributory factors, and psychosocial causes for somatoform symptoms. Are there differences between psychosomatic medicine, biomedicine, and TCM with regard to the patients’ and the physicians’ explanatory models? We expected that physicians of biomedicine and TCM would report physical causes and external causes significantly more often than the patients do. In psychosomatic medicine clinics, patients and physicians would report psychological causes more often than they do in biomedicine and TCM settings. To what extent do the illness attributions of the physicians concur with those of the patients? We expected to find low concordance between the patients’ and the physicians’ illness attributions. What influence do age, sex, number and severity of symptoms, and emotional distress have on patients’ and physicians’ explanatory models? We expected that younger patients, women, patients with a high number and high severity of somatoform symptoms, and patients with increased emotional distress would report significantly more psychological causes than would older patients, men, patients with a low number and low severity of somatoform symptoms, and those with lower levels of emotional distress.
Method
The study was conducted in the Outpatient Department of the Dong Fang Hospital, which is affiliated with Tongji University Shanghai. The Dong Fang Hospital is a full-service medical facility with approximately 1,000 beds. The study took place in the biomedical Departments of Neurology and Gynecology, the Department of Traditional Chinese Medicine, and the Department of Psychosomatic Medicine. In Chinese general hospitals, the Department of Psychiatry is often called “Department of Psychosomatic Medicine” or “Department of Psychological Medicine” to avoid the stigma associated with the term “psychiatry.” The staff of the Dong Fang Hospital consists of psychiatrists with additional psychotherapeutic training.
Clinical settings
The Psychosomatic Department treats patients with neurotic, psychosomatic, and psychotic conditions. A consultation typically takes 10 to 30 minutes. The Neurology Outpatient Clinic mainly treats stroke and headache patients; consultations last approximately 10 to 20 minutes. The Gynecology and Obstetrics Outpatient Clinic treats the entire spectrum of gynecological illnesses. Consultations in the Gynecology Department are between five and ten minutes long. The TCM Department primarily treats patients with chronic ailments such as chronic pain disorders, e.g., after herniated disc, arthritis, or patients with chronic recurrent infections. All patients in the TCM Department first undergo a biomedical assessment. Direct contact with the physician lasts approximately five minutes, and treatments (e.g., acupuncture) for up to ten minutes.
The study was conducted between May 5 and June 20, 2008. Patients who visited the outpatient clinics in the aforementioned departments were screened at regular time points using the questionnaire for somatoform disorders (see below). The attending physician later clarified whether or not the symptoms were found to be caused by an organic illness based on the available diagnostic examinations. If the physical symptoms could be explained by an organic illness, the patient was excluded from the study. In addition to an organic illness, further exclusion criteria were psychoses, anorexia nervosa, addiction, and mental retardation. Moreover, pregnant patients were excluded from the study, as pregnancy symptoms and somatoform symptoms could not be anamnestically distinguished.
Physicians
Eleven physicians took part in the study: two from the Department of Psychosomatic Medicine, three from neurology, two from gynecology, and four from TCM. All physicians had worked at the hospital for at least 3 years and had completed further specialist training.
Measurements
The following questionnaires were used:
Screening for MUS was carried out with the Screening Questionnaire for Somatoform Symptoms (SOMS; Rief, Hiller, & Heuser, 1997). This questionnaire comprises 53 symptoms and refers to the list of symptoms for somatoform disorders according to DSM-IV. Its validity and reliability are good (Rief et al., 1997). Patients can evaluate the intensity of their symptoms on a 5-point Likert scale from 0 (=not at all) to 4 (=very strong). In addition to the directions on the SOMS, the patients were verbally instructed to include only those symptoms for which the physicians could find no organic explanation. Patients with four or more symptoms for men and six or more symptoms for women over a period of 6 months or longer with a rating of 3 (=strong) or 4 (=very strong) were included in the study (Escobar, Rubio-Stipec, Canino, & Karno, 1989). Furthermore, the duration of symptoms was separated into three different categories: 6 months to 1 year, 1 to 2 years, and over two years. The number of physician visits was categorized into 1 or 2 times, 3 to 6 times, 6 to 12 times, and more than 12 times in the last 12 months. The impairment in well-being and everyday life, e.g., family, work, and leisure activities, was scaled dichotomously (yes/no).
Emotional distress was measured with the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983; Chinese version, Lam, Pan, Chan, Chan, & Munro, 1995; Wang, Chair, Thompson, & Twinn, 2008), which includes two subscales (anxiety and depression) with seven items each that refer to the patient’s condition during the previous week. For both scales, values under 8 are considered unremarkable, values between 8 and 10 marginal, and values over 10 remarkable.
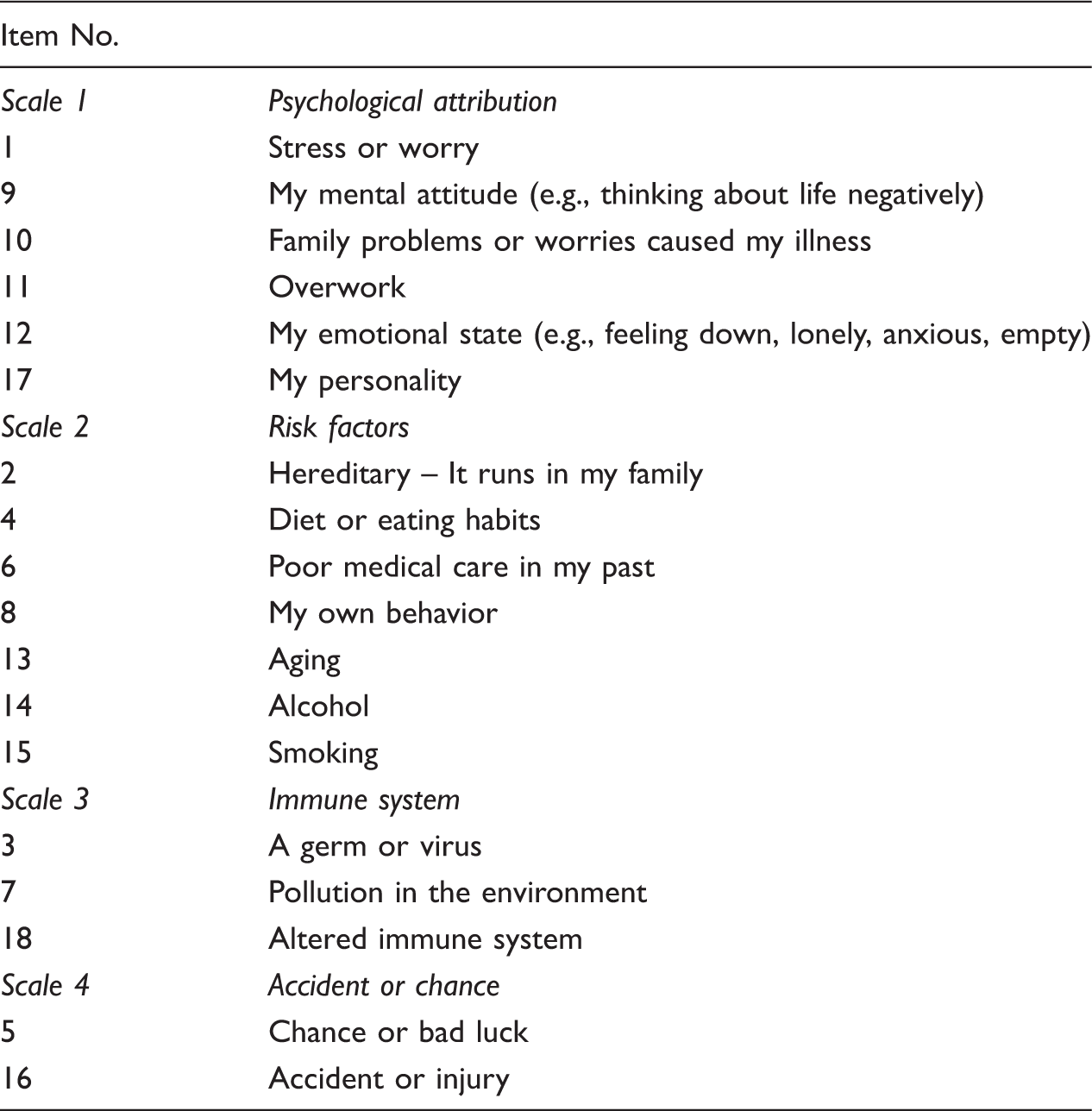
Cognitive representations of illness were measured with Illness Perception Questionnaire (IPQ; Broadbent, Petrie, Main, & Weinman, 2006; Moss-Morris et al., 2002; Weinman, Petrie, Moss-Morris, & Home, 1996) which has good validity and reliability. For the present study, the questionnaire included questions on the suspected causes of illness, with 18 different possible factors influencing illness. Patients used a 5-level Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, strongly agree) to report whether and to what extent the given factors caused their illness. In a subsequent open-ended question, they specified the three most important causes for the emergence of their illness.
Illness Perception Questionnaire (IPQ) scales and items
Translation of the questionnaires
There are previously published translations of the HADS and the IPQ in Mandarin Chinese. We used the HADS version of Lam et al. (1995) and the IPQ-Revised (IPQ-R), which is available on Internet (http://www.uib.no/ipq/pdf/IPQ-R-Chinese.pdf). A psychometric validation of the Chinese version of the IPQ-R has been done by Chen, Tsai, and Lee (2008).
The SOMS (Rief, Hiller, & Heuser, 1997) was translated and back-translated from German into Mandarin Chinese following the guidelines of the International Test Commission (Coyne, 2005; notes to the guidelines in Hambleton, 2005): initially independent translations were done by three native Chinese speakers living in Germany, both of whom were fluent in written and spoken German; one was a psychiatrist and the other a psychologist and educationalist. A translator regularly participated in the project meetings. Translations were discussed within the group, and a final version was agreed upon. Then, back-translation blind to the original into German was carried out, and a comparison of the German original with the translated Chinese and back-translated German versions was done by the working group to create the final version.
An informed consent document explained the aims of the study to the patients, who were informed that participation was voluntary, the data would be evaluated anonymously, and there would be no disadvantages should they choose not to participate in the study. By signing the document, the patients confirmed that they had been properly informed and agreed to the evaluation and processing of the gathered data.
Statistical procedures
The statistical evaluation was done with the SPSS Release 17. Simple descriptive statistics were used to describe the sample and the univariate distribution (mean, standard deviation, frequencies). For the interval scale data, the t test for independent samples was used. Cross tables and chi-square statistics were used for the nominal data. Simple Pearson’s correlation coefficients were calculated to quantify the relationships between continuous variables.
For the multivariate analysis of the causal factors of illness attribution, we dichotomized the IPQ responses into “disagree” (1 and 2) and “agree” (3, 4, 5). The HADS anxiety and depression scores were highly correlated. Because health anxiety is central to MUS/somatoform disorders, we chose HADS anxiety as the primary indicator variable for emotional distress to be entered into the subsequent regression analysis. The list of predictors included HADS anxiety, number and severity of symptoms, age, sex, and department.
The difference in the results was tested according to the usual significance threshold of p < .05. The tables report the exact level of significance. Multiple comparisons of means were used to test for specific differences between the three treatment groups. Using Bonferroni correction, the alpha level was set at p = .008 (Holm, 1979).
Results
A total of 952 patients took part in the screening examination conducted in the waiting areas of the four departments. Patients who screened positive and fulfilled the inclusion and exclusion criteria were asked to fill in further questionnaires before the consultation. In psychosomatic medicine, 57 patients were screened; 31 (54%) showed positive and three were not able to fill out further questionnaires or had incomplete data, resulting in 28 participants. In Gynecology, 681 patients took part in the screening examination; 34 (5%) were positive and eight refused to fill out further questionnaires, had symptoms that could be explained by an organic illness, or provided incomplete data in the questionnaire, resulting in 26 participants. In Neurology, 92 patients took part in the screening examination; 16 (18%) were positive and five were not able to fill out further questionnaires, had symptoms that could be explained by an organic illness, or had incomplete data, resulting in 26 participants. For TCM, 122 patients took part in the screening examination; 38 (31%) were positive and seven were not able to fill out further questionnaires, had symptoms that could be explained by an organic illness, or had incomplete data, resulting in 31 participants.
Sociodemographic characteristics of sample (N = 96)
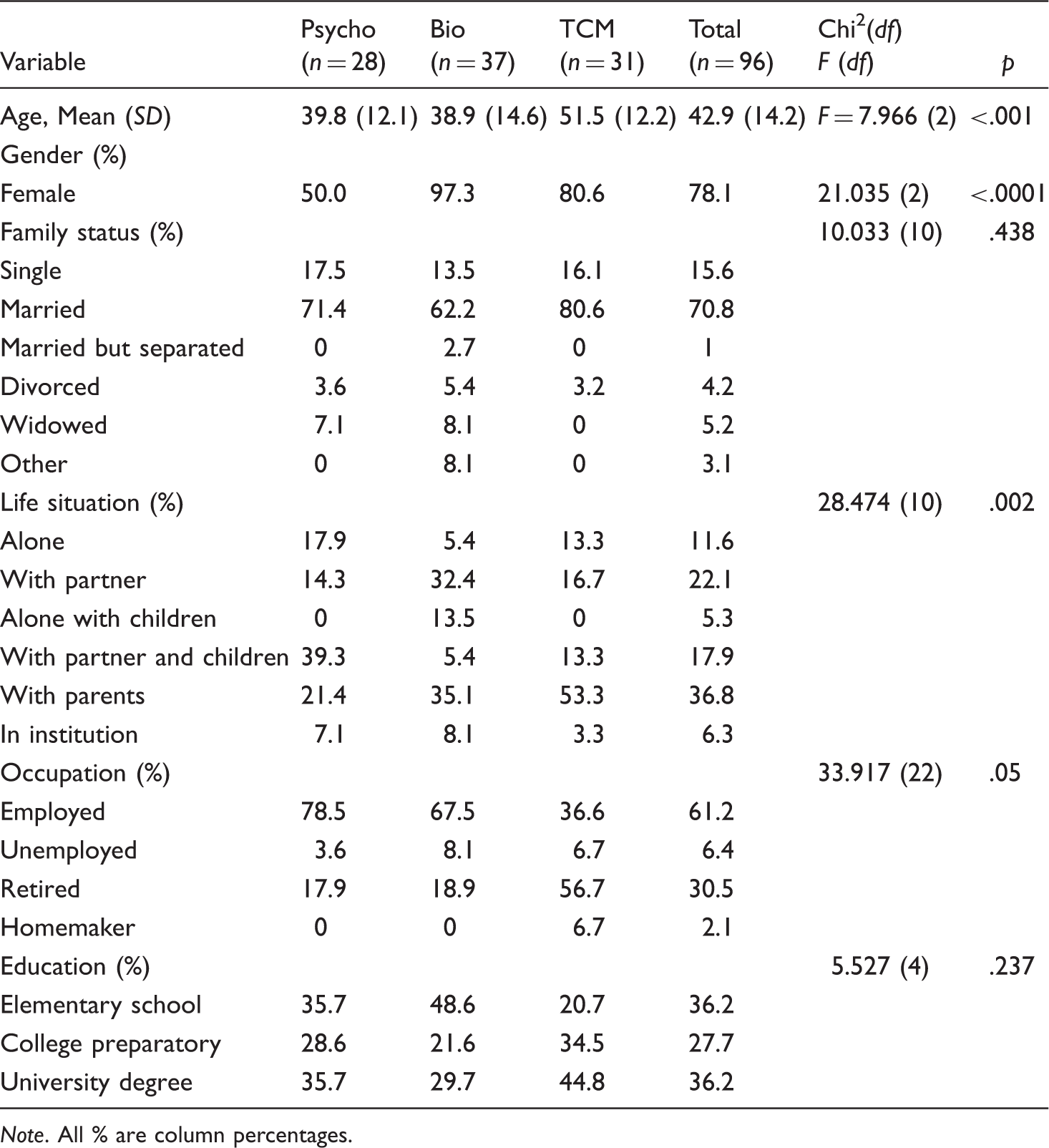
Note. All % are column percentages.
Clinical characteristics of sample (N = 96)
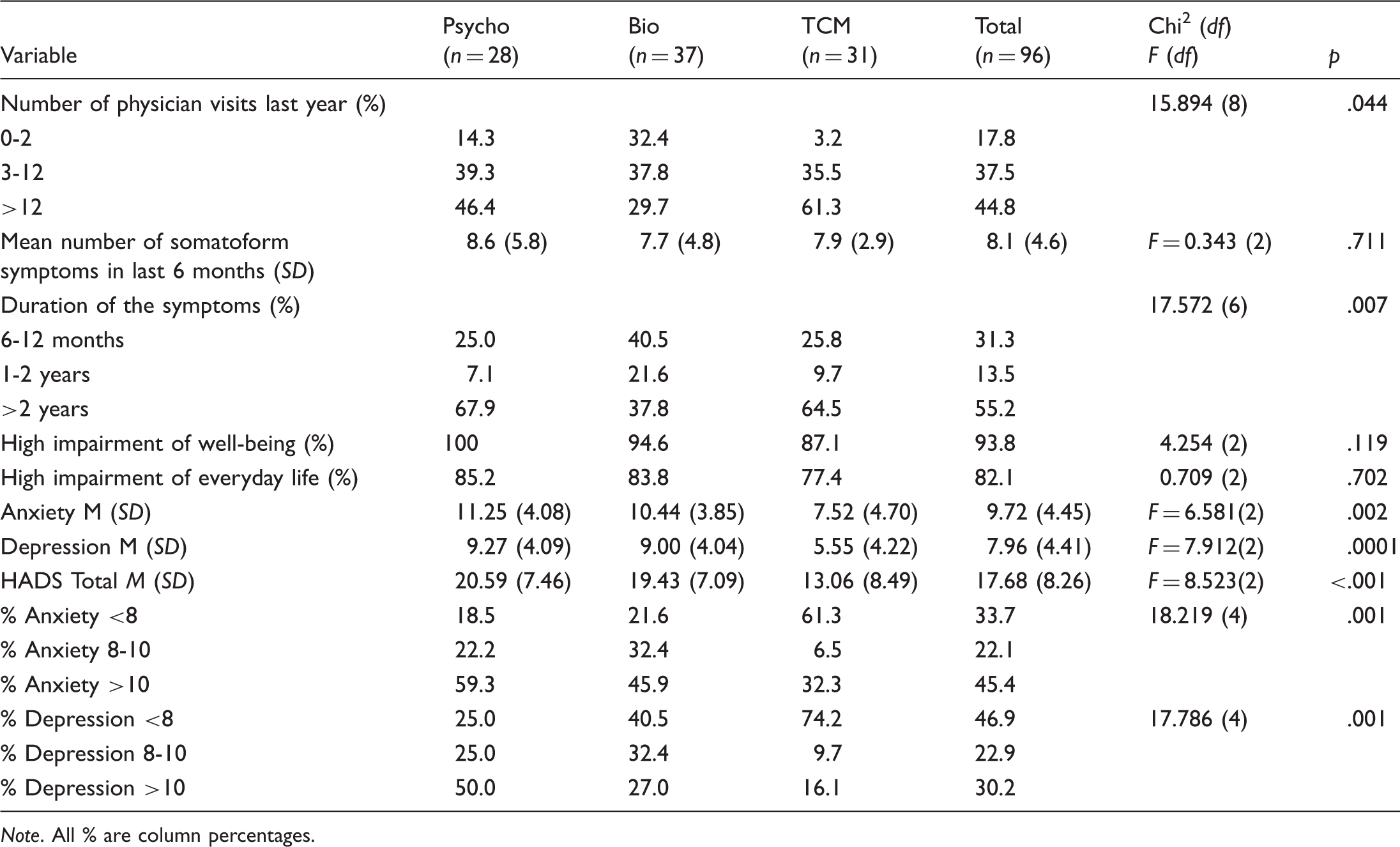
Note. All % are column percentages.
The number of somatoform symptoms with strong or very strong intensity in the last 6 months was 8.1 on average. The most common symptoms in psychosomatic medicine patients were heart palpitations and extrasystoles, a sensation of pressure around the heart, abnormal fatigue with light exertion, sweating, and dry mouth. In biomedicine, the most common symptoms were heart palpitations and extrasystoles, irregular menstruation, abnormal fatigue with light exertion, orofacial pain, and a sensation of pressure around the heart. In TCM, the primary symptoms were back pain, joint pain, arm and leg pain, orofacial pain, and abnormal fatigue with light exertion.
Emotional distress
The mean values for anxiety and depression were considerably high for all patients; 45.4% were suspected to have a clinically significant anxiety disorder, and 22.1% were borderline cases. For 30.2% of patients, there was a strong likelihood of depressive disorder, whereas 22.9% were borderline cases. Patients in TCM had significantly lower HADS total scores compared with those in psychosomatic medicine and biomedicine.
Causes of illness from the patients’ and the physicians’ points of view
Patient and physician symptom attributions* (N = 96)
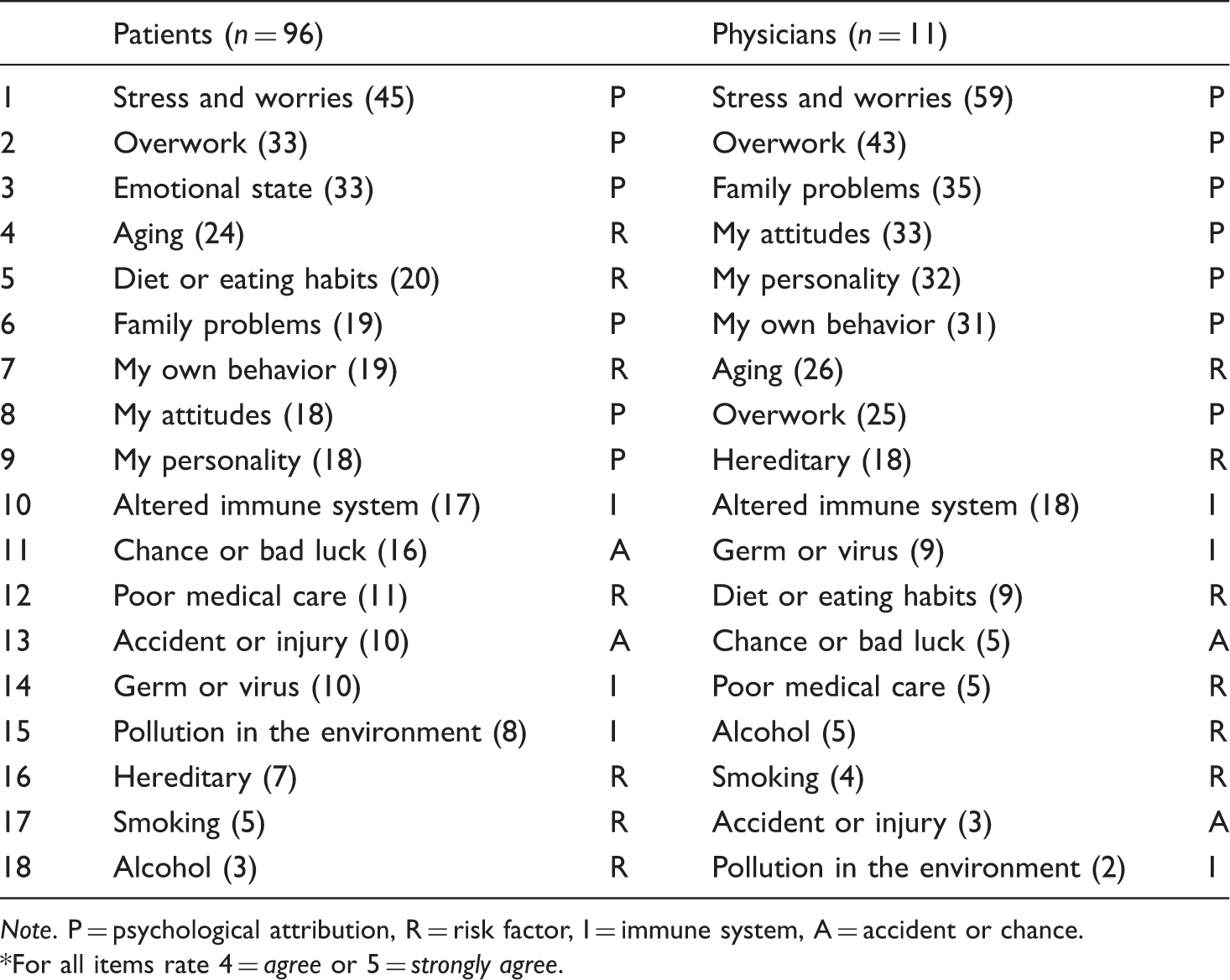
Note. P = psychological attribution, R = risk factor, I = immune system, A = accident or chance.
For all items rate 4 = agree or 5 = strongly agree.
Patient illness attributions by clinic setting (N = 96)
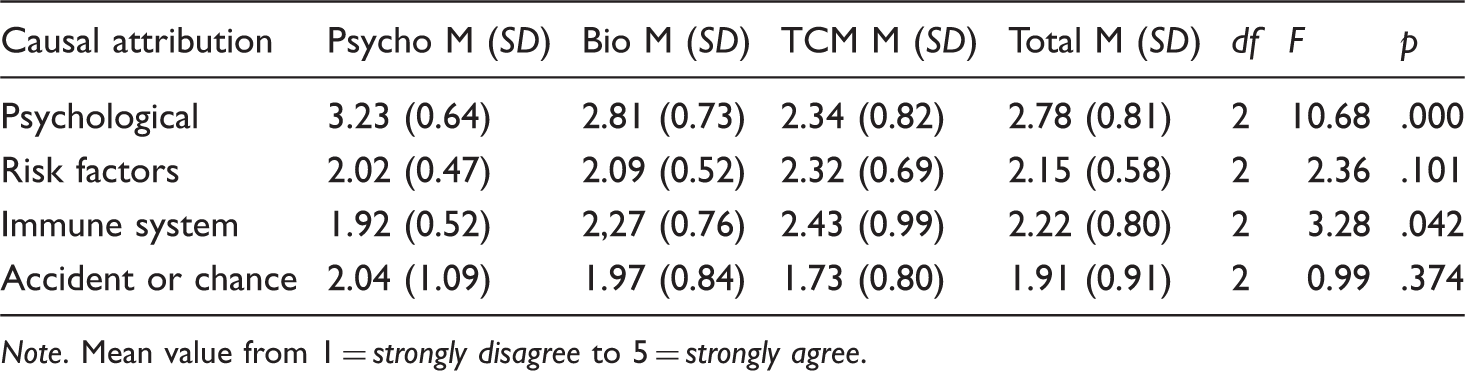
Note. Mean value from 1 = strongly disagree to 5 = strongly agree.
Pearson correlations between the causes of illness from patients’ and physicians’ point of view (N = 11)
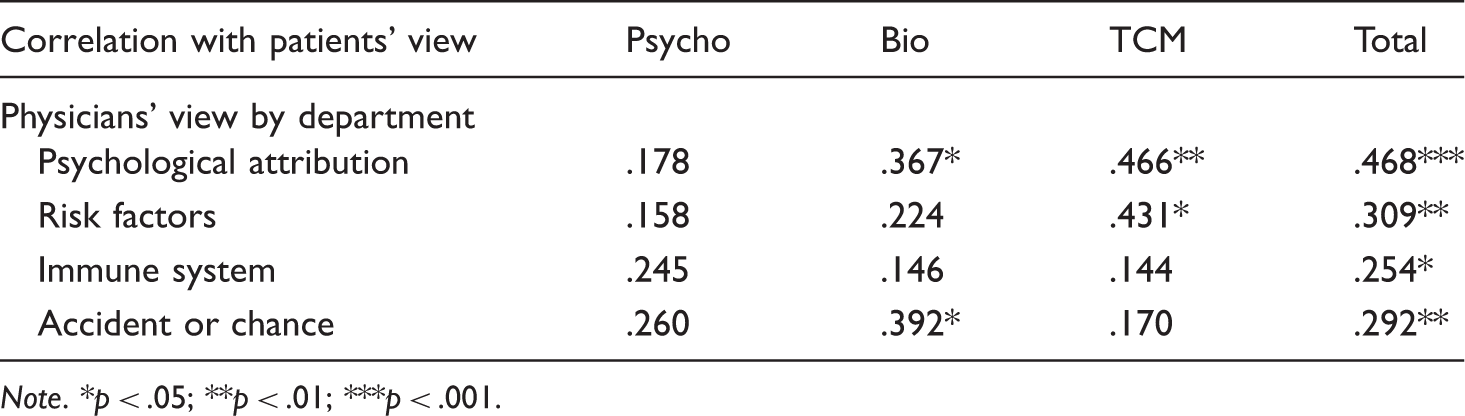
Note. *p < .05; **p < .01; ***p < .001.
From the physicians’ perspective, “psychological attributions” was also the most common cause (mean value from 1 = strongly disagree to 5 = strongly agree: 3.07, SD = 0.94). The other causes were rated as follows: risk factors, M = 2.35 (SD = 0.50); immune system, M = 2.15 (SD = 0.75); and accident or chance, M = 1.88 (SD = 0.63). Because of the limited number of physicians in every department, we did not separate the illness attributions of the physicians according to the three clinical settings.
A comparison of the three areas of medicine at the single-item level reveals the following pattern: psychological attributions such as “my own behavior,” “family problems,” and “my personality” were more frequently given in psychosomatic medicine than in biomedicine and TCM. In contrast, the items “hereditary,” “diet or eating habits,” “pollution,” “aging,” and “altered immune system” were more frequently given in TCM. A similar pattern was found for the cause of the illness from the physicians’ perspective, except that all six items in the psychological attributions scale were given more frequently in psychosomatic medicine; TCM physicians, like the patients, tended to choose the items “hereditary,” “aging,” “diet or eating habits,” and “altered immune system.”
Regarding the three most important causes of illness in the open-ended question, “psychological attributions” was the most common answer in psychosomatic medicine (patients, 78%; physicians, 91%); it showed a similarly high percentage in biomedicine (patients, 51%; physicians, 52%) but a considerably smaller percentage in TCM (patients, 20%; physicians, 27%). While “immunity” played a very marginal role in psychosomatic medicine and biomedicine (under 10%), its percentage in TCM was higher for both physicians and patients (20%). “Risk factors” was the top cause in TCM at 47% for patients and 46% for physicians, compared with approximately 25% in biomedicine and approximately 10% in psychosomatic medicine (from both the physicians’ and the patients’ perspectives). “Accident or chance” did not play a significant role in any of the three areas (less than 5%).
Correlations between causes of illness from the patients’ and physicians’ points of view
The strongest correlations in the causes of the symptoms between the point of view of the patients and the point of view of the physicians were found for the items under “psychological attributions” (see Table 5b). The worst correlation between the patients’ and the physicians’ points of view was in psychosomatic medicine, and the best in TCM. The correlations in the three other scales were low and not significant.
Effect of emotional distress, somatic symptoms, physician visits, age, sex, and department on illness attributions
Clinical anxiety values (≥8 in HADS) were related to higher “psychological attribution” from the patients’ view (df = 1, t = 7.58, p < .0001) and from the physicians’ view (df = 1, t = 5.01, p < 0.001). Clinical depression values (≥8 in HADS) were related to higher “psychological attribution” from the patients’ view (df = 1, t = 6.32, p < .0001) and the physicians’ view (df = 1, t = 4.02, p = .005). The remaining three scales showed no significant correlations with emotional distress.
In multivariate logistic regression analysis, HADS anxiety proved to be a significant predictor of psychological attribution (model parameter: n = 96; Nagelkerke R2 = 0.26; Hosmer-Lemeshow C = 6.3 (df = 7); p > .501; model Chi2 = 20.89 (df = 2); p < .001; significance (HADS anxiety) < .001). Number and severity of symptoms, number of physician visits, age, sex, and department had no significant effect on illness attributions.
Discussion
As expected, both patients and physicians gave a wide range of attributions for illnesses. This confirms that illness attribution is multidimensional in this Chinese sample (Lundh & Wangby, 2002; Rief et al., 2004). What is striking is the high frequency of “excessive labor,” particularly for patients in psychosomatic medicine; this may be the result of high work stress due to the very competitive struggle for jobs. Surprisingly, there were a high number of psychological attributions both in biomedicine and TCM. The hypothesis that Chinese patients tend to attribute somatic symptoms to physical causes was not confirmed by these data. On the contrary, both patients and physicians were very open to psychosocial causal attribution. Our patient group could, for the most part, be described as “initial somatizers” (Bridges & Goldberg, 1985; Kirmayer & Robbins, 1991). In contrast to “true somatizers,” the development of an alternative illness attribution that included not only somatic factors as causes of illness seemed to be possible for a large portion of this patient group. The reattribution model (Fink, Rosendale, & Toft, 2002; Goldberg, Gask, & O’Dowd, 1989) would thus seem to be a promising treatment method for this patient group.
Unlike our results, in 100 patients with neurasthenia (SJSR) at the Psychiatry Outpatient Clinic of the Hunan Medical College, Kleinman (1982) found that 78% of patients held that their disorder was wholly or partially organic, in spite of the fact they were in a psychiatric clinic. Only 22% regarded their problem as principally or wholly psychological. Similar to our results, Kleinman (1982) found the most frequent attribution of cause to be work problems (61%), followed by political problems (25%), separation from work sites (25%), marital and family problems (20%), and exam and school problems (16%). Only a small number of patients thought that their symptoms were due to nutritional problems (9%) or were hereditary (5%). In the follow-up interviews in Kleinman’s (1982) study on “illness meanings,” the patients were very open to psychosocial interpretations: symptoms were seen as an opportunity to express personal or interpersonal distress, or unhappiness (93%), to manipulate interpersonal relations (74%), to take time off from work or other social obligations (72%), and to receive love and care from family and friends (65%). However, the passage of time between Kleinman’s study and the present one might limit the comparison.
Culture-specific explanations were not reported in our study except by the patients and physicians in TCM. The open-ended question often elicited the response “weak immune system (qi)” and “effects of wind, cold, and dampness.”
A comparison of the most common somatic symptoms between our Chinese sample and Western countries is difficult because many sociocultural factors influence symptom presentation. In the United States and the United Kingdom, about half of the symptoms are pain complaints (e.g., headache, chest pain, abdominal pain), a quarter consists of upper respiratory discomfort, and the remainder includes other symptoms such as fatigue and dizziness (Kroenke & Rosmalen, 2006; Reid et al., 2001). The Chinese patients were just as impaired in their well-being and everyday lives, and had consulted their physician about their symptoms in the past year as often as patients in Western countries had (Rief et al., 1997).
The differences in the causes of illness between the three areas of medicine reflect the illness perceptions of the three treatment approaches: For both patients and physicians, “psychological attributions” were most often reported in psychosomatic medicine, while “hereditary,” “diet or eating habits,” “aging,” and “altered immune system” were most often reported in TCM. Patients seen in Biomedicine occupied a middle position.
Regarding the importance of psychosocial factors, there was a significant correlation between the views of physicians and patients. For the other scales, however, the correlation between physicians’ and patients’ explanatory models was low. The biggest differences were found in the effect of the “altered immune system,” “poor medical care in my past,” “pollution in the environment,” and “hereditary.” Physicians considered these items to be much more important than did patients.
Forty-five percent of the patients had an anxiety score of more than 10, and 30% had a depression score of more than 10; this means a high percentage of the sample comprised clinical cases of anxiety and depression. Studies from Western countries show that at least one third of patients with somatoform disorders have comorbid anxiety and depressive disorders, whereas depression and anxiety co-occur up to 50% of the time (Henningsen, Zimmermann, & Sattel, 2003; Toft et al., 2005). The validated psychometric scales for depression, anxiety, and somatization are highly intercorrelated (Bjelland, Dahl, Haug, & Neckelmann, 2002; Simon, Gater, Kisely, & Piccinelli, 1996). Similar to the finding in Western countries, emotional distress was positively related to psychological attributions. Age, sex, and number of somatoform symptoms had no effect in this study.
Generalizability
This study has several limitations. First, the questionnaire on somatoform symptoms and the questionnaire on the causes of the symptoms have not yet been validated for China. They lack both culture-specific symptoms and culture-specific explanations for the symptoms. Second, the study was introduced as a “psychosomatic study.” Thus, patients and physicians might have adjusted to the assumed expectations of the researchers by reporting a high degree of psychosocial attributions. Third, this study used a small sample from three different areas of medicine, and the participants differed significantly with regard to age, sex, life situation, and symptom presentation. Because of the small number of physicians (n = 11, e.g., two physicians from gynecology), the comparisons of the physicians’ illness attributions between the three clinical settings, and the correlation between the causes of the illness from the patients’ and the physicians’ points of view should be interpreted with caution. Patients with less schooling were underrepresented in all three areas. Patients with higher education had fewer difficulties describing and expressing the complexity of their feelings or emotional experiences through language. Fourth, the IPQ lacks both culture-related symptoms and culture-related explanations of the symptoms, e.g., the historical Chinese models of the body and the role of ancestors. The four scales of the IPQ only partially reflect the dimensions of the biopsychosocial model. While psychological and somatic attributions are well represented, the social dimension is not captured in a clear-cut manner. The number of somatoform symptoms, the duration of the symptoms, the high frequency of anxiety and depressive symptoms, and the severe degree of impairment in everyday life show that the patient group is heavily burdened both physically and psychologically. In this respect, Chinese and European MUS patients are similar.
Conclusion
This pilot study is the first systematic comparison of the illness attributions of patients with medically unexplained physical symptoms in psychosomatic medicine, biomedicine, and TCM in China. Due to the small and heterogeneous sample group, conclusions should be drawn very carefully. Despite the higher proportion of somatic presentations of Chinese patients described in the literature, patients and physicians are extremely willing to accept psychosocial causes for symptoms. This is an important prerequisite for successful clinical assessment, treatment negotiation, and intervention. The distribution patterns of illness attributions reflect the illness perceptions of the physicians and the patients who seek care in those respective departments.
To deepen our understanding of patient and physician illness attributions and the everyday and professional notions behind them, quantitative studies need to be supplemented with interviews, such as the McGill Illness Narrative Interview (Groleau, Young, & Kirmayer, 2006). In this way, we can better understand culture-specific symptoms and explanatory models.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements
We thank Dr. Wu (psychosomatic medicine), Dr. Zhang (Traditional Chinese Medicine), Dr. Huang (gynecology and obstetrics), and Dr. Huang (Neurology) of the Dong Fang Hospital, and Stephanie Kern (Freiburg) for their support in data collection. Many thanks to our physician candidate Zhao Ruoyao for the translation of the questionnaires, and to Chinese medical students Yuanzhe Li and Sun Hui for help in interpretation. We thank Mathias Nübling and Armin Hartmann for their advice in statistics.