
Abstract
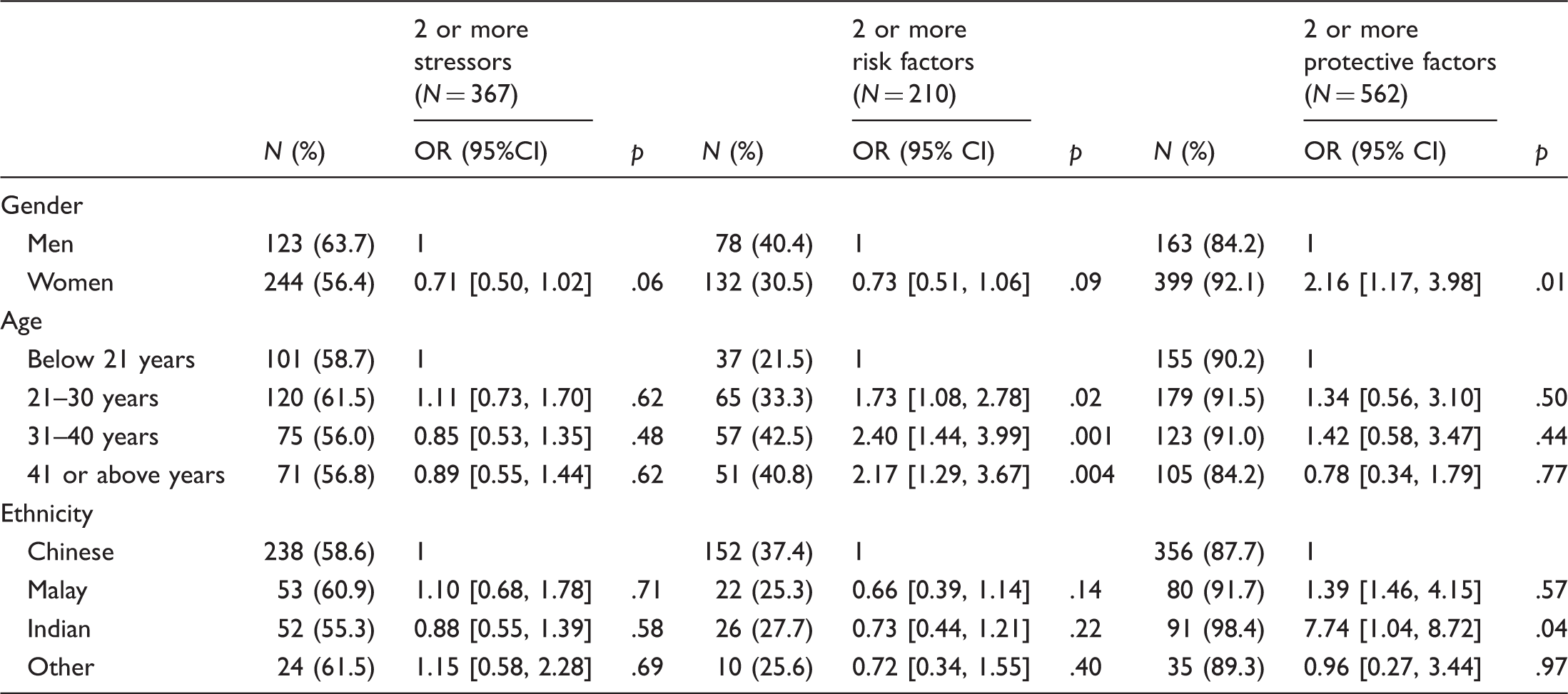
This study examined the ethnic differences in stressors, risk, and protective factors among people who attempted suicide in Singapore. A retrospective chart review of 626 attempted suicide cases at a hospital in Singapore between 2004 and 2006 collected information on diagnosis according to DSM-IV-TR criteria. Chi-square tests was used to compare the sociodemographic characteristics, stressors, risk factors, and protective factors among Chinese, Malay, Indian, and other ethnic groups. Logistic regression was used to determine the odds ratios of having two or more stressors, risk factors, or protective factors for the four ethnic groups. Women were more likely than men to attempt suicide, although they also were more likely to have two or more suicide protective factors than men. In general, older people were more likely to have two or more suicide risk factors than the younger groups. Ethnic differences were found in history of psychiatric illnesses and unemployment among the risk factors, and for most of the protective factors, but none of the stressors. Indians were more likely to have two or more protective factors than were Chinese (OR of 7.74, 95% CI [1.04, 8.72]. Future suicide prevention programs should target young adults and strengthen the protective factors among different ethnic groups.
Introduction
Suicide is a complex behavior that has substantial social, economic, and public health impact. It is estimated by the World Health Organization (WHO) that 873,000 people commit suicide worldwide each year, representing 1.4% of the global burden of diseases (World Health Organization, 2004). Suicide rates vary across countries (Liu et al., 2011), owing to differences in ethnicity, culture, religion, medical care, and social support (Chia, Chia, & Tai, 2008; Levi et al., 2003). Asian countries account for about 60% of the estimated total deaths by suicide in the world, with Japan, South Korea, and Sri Lanka ranking among the highest (Hendin, Vijayuakumar, & Bertolote, 2008). The epidemiological profiles of suicides in Asia differ significantly from the Western societies (Hendin et al., 2008). In the West, suicide rates for males are about 3–4 times higher than females, but smaller gender differences are found in Asian countries (Chen, Wu, Yousuf, & Yip, 2012). Acute life stress also appears to play a more important role in Asia than in Western countries (Wei & Chua, 2008). Furthermore, the methods of suicide vary with the West commonly using firearms, hanging, drug overdose, and gassing, while in Asia ingestion of pesticides in rural areas and drug overdose and jumping from heights in more urban settings predominate. However, research on socioeconomic, cultural, and religious factors contributing to the pattern of suicide in Asia is still limited.
Singapore is a major commercial centre in South East Asia and has a population of about 5.1 million with major ethnic groups including Chinese (74.1%), Malay (13.4%), Indian (9.2%) and other ethnicities (3.3%) distributed across all parts of the island. This multiethnic population offers a unique opportunity for studying cultural and social differences in suicide behaviors. The suicide rate in Singapore is about 13 per 100,000, ranking in the middle among other countries in the West and is comparable to most developed countries (La Vecchia, Lucchini, & Levi, 1994). Previous studies in Singapore have found suicide rates increase with age, have a lower male:female ratio compared to other countries, and are correlated with unemployment (Loh et al., 2007). Like many other countries, there are variations in suicide rates across ethnic groups within the community. A study in the early 1970s found similar suicide rates between Chinese (12.4 per 100,000 in males and 8.90 per 100,000 in females) and Indians (10.9 per 100,000 in males and 8.70 per 100,000 in females; Chia & Tsoi, 1972). Other studies reported the highest suicide rate among Indians with 13.7 per 100,000 in 1980 (Tsoi & Kok, 1982) and 20.3 per 100,000 in 1986 (Peng & Choo, 1990). A study of the elderly conducted in the late 1980s found a higher suicide rate in Chinese (59.3 per 100,000) compared to Indians (33.9 per 100,000) and Malays (3.0 per 100,000; Ko & Kua, 1995). Later studies, continued to find that Chinese had the highest suicide rates, followed by Indians and Malays (Chia, Chia, Yee, & Choo, 2010; Loh et al., 2007). A study of 251 cases of completed suicide conducted by Murty and colleagues in Malaysia, a country that has close geographical connection to Singapore and shares similar ethnic groups (Malays, Chinese, and Indians) and cultures, found a distribution on the order of 48% Chinese, 35% Indian, 6% Malay, and 11% other ethnic groups (Murty et al., 2008). Another Malaysian study also found that Chinese were more likely than Malays to report suicide plans and that Malays had consistently lower rates of suicide attempts than Chinese and Indians (Foo, Mohd Alwi, Ismail, Ibrahim, & Jamil Osman, 2014).
Religion can influence individuals’ attitudes toward the meaning of life and death, and end-of-life decisions. Religion can also contribute to the differences in how various ethnic groups tolerate and accept suicide as a way of life. Religiosity has been shown to be associated with reduced risk of suicidality (Lizardi et al., 2007). This effect is due to several factors. Most religions have sanctions against suicide and this may inhibit suicide behavior in individuals with strong religious commitments. Religious individuals are also more likely to be involved in activities organized by their religion, which provide opportunities to develop an extended support network. Furthermore, religiosity has been shown to be associated with lower levels of aggression and hostility, perhaps reflecting religious teachings (Koenig, McCullough, & Larson, 2001). Nevertheless, for members of certain religions that may be ambivalent and permissive about suicide, it may become a negative coping method (Pargament, 1997).
For Islam, suicide is strictly a forbidden act that is considered sinful and unforgivable. Islam also forbids the use of alcohol and drugs, which are well-known risk factors for suicide. Thus, national suicide rates are generally lower in predominantly Islamic countries (Lester, 2006). However, many researchers have expressed concerns that these figures may be inaccurate because families may conceal suicidal acts to preserve family reputation and social status within the community, leading to underreporting of suicides (Pritchard & Amanullah, 2007). Buddhism, Hinduism, and Christianity are more ambivalent about suicide. Although Buddhism does not condone suicide, the belief in the cycle of karma, reincarnation, and the afterlife may lead some to resort to suicide to end their suffering with the conviction that the next life will be better. Perhaps as a result, some Buddhist countries such as Japan and Sri Lanka have reported relatively high suicide rates of 25.3 and 23.9 per 100,000, respectively (Vijayakumar et al., 2008). An exception is Thailand which has a relatively low suicide rate of 6.3 per 100,000; suicide in Thailand is generally regarded as an unacceptable action which condemns the individual to hell for 500 lifetimes (Vijayakumar et al., 2008). In Hinduism, suicide for religious or social reasons may be tolerated and sometimes even encouraged. For instance, “sati” is a Hindu custom in India whereby the widow demonstrates her devotion to the dead husband by burning herself into ashes over his funeral pyre. Christianity generally forbids suicide, regarding it as contrary to God’s plan. Nevertheless, Christian doctrines do not explicitly deny suicide victims from entering Heaven as long as they have faith in God and there are several examples of individuals committing suicide appearing in the Bible, such as Judas and Samson (Maris, Berman, & Silverman, 2000). Views of the morality of suicide vary among different Christian groups. In Protestantism, man’s salvation is by God’s grace alone and not by any merit of man’s own work, whereas for Catholicism God’s judgment is affected by man’s deeds and sins. As a consequence, committing suicide forgoes heaven for Catholics but not for Protestants. This is probably one of the reasons why there have been reports of higher suicide rates among Protestants compared to Catholics (Gearing & Lizardi, 2009).
In the multiethnic context of Singapore, there are many religions coexisting together, and this may have an impact on suicidality. The major religions practiced in Singapore are Islam, Hinduism, Buddhism, Taoism, and Christianity (Census of Population, Singapore, 2010). Most local Chinese are followers of Buddhism and Taoism, although there has been a shift in religious affiliations in the recent census. The proportion of Chinese who reported themselves as Buddhists or Taoists decreased from 64% in 2000 to 57% in 2010. In addition, there was an increase in the proportion of Christians (from 17% to 20%) and atheists (from 19% to 22%) among the local Chinese. Among Malays, Islam remained the major (about 99%) religion during the period of 2000 to 2010. Among the local Indians, Hinduism (59%) and Muslim (22%) were the major groups with only 13% reported to be Christian in 2010. We conjecture that the increasing religious and cultural heterogeneity within ethnic groups may affect the various ethnic groups’ perception and acceptance of suicide.
There have been rapid changes in the social, cultural, and economic landscape over the last few years brought about by globalization and this is likely to influence the suicide pattern in Asia (Milner, McClure, Sun, & De Leo, 2011). Stressors related to suicide have been investigated in Singaporean children and adolescents (Ang, Chia, & Fung, 2006), but not in adults. Most studies of suicide among adults in Singapore have not investigated how ethnic differences could influence stressors, risk factors, and protective factors at the same time. Nevertheless, there is evidence from studies in the West that suicide risk varies across ethnic groups. For example, a study in the United Kingdom found that suicide ideation, hostility, and emotional distress were less common among black Africans, black Caribbeans, and South Asians, while hopelessness and depression were more common among South Asians (Bhui & McKenzie, 2008). Therefore, this study aims to provide a profile of the demographic, ethnic, and religious characteristics of adults hospitalized for suicide attempts and the related ethnic and religious differences in a Singapore general hospital.
Methods
This study is based on an archival retrospective review of consecutive cases of attempted suicide admitted to the adult medical ward at the National University Hospital, Singapore, between January 2004 and December 2006. The hospital was selected as two of the authors worked there during the time that a comprehensive suicide risk assessment checklist form was implemented. Patients who had attempted suicide were referred from the medical ward to the psychiatric team for assessment and the interview took approximately 30 minutes. This assessment was part of the standard clinical protocol for patients admitted following a suicide attempt. The interview was based on a semistructured checklist. At the time of the evaluation, the psychiatrist made a formal diagnosis based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV-TR; American Psychiatric Association, 2000).
The stressors assessed were work-related issues, family-related issues, relationships, financial problems, and medical illnesses. Risk factors of suicide assessed were history of psychiatric illnesses, family history of psychiatric illnesses, living alone, alcohol or substance misuse, ongoing interpersonal problems, lack of confidantes, serious physical illnesses, poor coping skills, severe financial problems, and unemployment. The protective factors included faith in a religion, resolution of precipitants, receiving support from dependents, expression of regret, positive plans for the future, willingness to seek help, and good emotional support. All these factors mentioned were listed in the suicide risk assessment checklist form, which was created by a team of psychiatrists in the department based on known common risk factors of suicide. The main function of the checklist form was to serve as a clinical tool to enable the assessing psychiatrist to not miss common possible stressors and risk/protective factors. The assessing psychiatrist would go through the list of factors for each patient and record information according to what the patient and family members reported. Most of the risk and protective factors were straightforward, for example, “history of psychiatric illness” and “willingness to seek help,” which could be verified from the family and medical records from hospitals/private clinics. However, there were some factors such as “coping skills,” “interpersonal problems,” and “emotional support” that could be subjective, as they were based mainly on the patient’s and family’s perceptions. Therefore, in an attempt to standardize the assessment, all psychiatrists were briefed and trained on the individual factors so that they reach a common understanding of the terms and what they encompass prior to using the form. All available medical records from hospitals and private clinics were traced and included to ensure accuracy of the information provided. Archival data were extracted from multiple databases and sources, including the suicide risk assessment checklist forms, risk assessment records, as well as psychiatric reports, inpatient records, and electronic notes completed by medical officers.
All reports were anonymized and identified by unique identification numbers. This project was approved by the hospital ethics committee.
In the main analysis, chi-square tests were used to compare the sociodemographic characteristics (gender and age), stressors, risk factors, and protective factors among Chinese, Malay, Indian, and other ethnic groups. Logistic regression was used to determine the odds ratios of having two or more stressors, risk factors, or protective factors for each ethnic group with adjustment for demographic factors.
Results
Basic characteristics and factors of people who attempted suicide by ethnic groups.

The top three psychiatric diagnoses across all ethnic groups for those who attempted suicide were acute stress reaction, adjustment disorder, and depressive disorder, with “acute stress reaction” being the most common. Malays had higher rates of being diagnosed with acute stress reaction as compared to Chinese (40.2% vs. 25.7%; p = .006). More Chinese were diagnosed with depressive disorder as compared to other ethnic groups (17.3% Chinese, 5.7% Malay, 9.7% Indians, 5.1% others; p = .005). A similar percentage of people across all ethnic groups who attempted suicide did not have a psychiatric diagnosis (15.3% Chinese, 12.6% Malay, 12.9% Indian, 15.4% others).
About half or more of the people who attempted suicide in all ethnic groups regarded relationship issues as one of the main stressors for suicide. Having ongoing interpersonal problems was the most common risk factor for all ethnic groups, while poor coping skills came in second place for all except the “other ethnic” group. Chinese who attempted suicide were more likely to have history of psychiatric illnesses as compared to Malays or Indians and this was statistically significant (p < .001). In terms of protective factors, expression of regret and good emotional support were the most common factors in all ethnic groups. Malays (62.1%) and Indians (44.7%) were more likely to regard faith in religion as a protective factor as compared to Chinese (24.4%; p < .001). Relatively more Malays found receiving support from dependents helped in preventing suicide than did Chinese (p = .001). More Malays and Indians than Chinese viewed the resolution of precipitants as a protective factor against suicide.
Odds ratios of having two or more stressors, and risk factors and protective factors of suicidal behaviors for different ethnic groups.
Discussion
Among the patients in our study who attempted suicide, Chinese appeared to be slightly underrepresented while Indians and Malays were overrepresented compared to their proportion in the general population. Regarding methods of suicide, previous studies have reported poisoning to be the most common suicide method used by Malays (Murty et al., 2008) and Indians (National Crime Records Bureau & Ministry of Home Affairs, Government of India, 2005), while jumping from a height was most common among Chinese in Singapore (Lester, 2008). Our study found that the most frequent methods of attempted suicide were drug or substance overdose and there was no difference among the ethnic groups. This could be due to the fact that it is easy to obtain certain drugs such as paracetamol over the counter and the accessibility of suicide means is an important determinant of method irrespective of ethnicity. Furthermore, the patients in this study were cases of attempted suicide rather than completed suicide, thus the use of less lethal or violent means of suicide might be more frequent.
Risk and protective factors
Women were found in our study to have a relatively higher likelihood of having two or more protective factors of suicides as compared to men, although their actual attempt rates were higher in the present findings. This suggests that the conventionally recognized protective factors may not be sufficient to alleviate the risk of suicide attempts among women in Singapore. Further research is needed to delineate risk and protective factors specific in women.
The odds of having two or more risk factors for suicide were found to increase in the age group above 21 years, with higher risk between 31 and 40 years. These ages are the times when adults encounter greater stress as they take on various roles and responsibilities in society, with problems ranging from relationship issues (setting up families, broadening social networks), work (competing with others to advance up the ranks), and financial matters (buying a house, paying bills). These problems can often evoke feelings of hopelessness and worthlessness to cope with everyday life. Suicide may therefore present itself as an escape route from one’s problems or be the result of impulsivity or as a way to demonstrate unmet needs (Rudnicka-Drozak, Makara-Studzinska, & Skorzynska, 2002).
Psychological autopsy studies conducted in Asian countries have identified the major risk factors for suicide including mental disorders, misuse of alcohol/drugs, previous history of suicide attempt, and presence of an acute life event. In Asia, the causal role of depression or other mental disorders appears to be less pronounced than in the West (Vijayakumar, 2005). Within Asia, while the role of acute life stresses such as job loss and work-related factors were important precipitants of suicide for men, family conflicts was a major risk factor for women (Chen et al., 2012).
In our study, relationship issues were the most common stressor precipitating suicide in all ethnic groups, with family-related issues in the second place. Interpersonal problems and poor coping skills were identified as the top two risk factors whereas expression of regret and good emotional support were the top two protective factors for all ethnic groups. These stressors, and risk and protective factors were closely related with a common theme of interpersonal difficulty. Failure to resolve conflicts occurring at various levels of interaction (at work, among friends, within families, etc.) may increase one’s risks of suicide. With the rapidly changing society and increased pace of life, the time one spends on interaction with others decreases and there may be disintegration of relationships with lesser emotional support.
In our results, Chinese people who attempted suicide were more likely to have a history of psychiatric illness as compared to other ethnic groups. This was consistent with the results of a local population survey which estimated prevalence of minor psychiatric morbidity to be highest for Chinese, followed by Indians and Malays (Fones, Kua, Ng, & Ko, 1998). However, another recent population survey in Singapore found that Indians had a higher lifetime risk of at least one mental disorder as compared to Chinese, while Malays had the lowest risk (Chong et al., 2012). In general, local Chinese and Indian people may be more competitive and lead fast-paced lifestyles, which may dispose them to psychiatric morbidities.
The top three psychiatric diagnoses made for all ethnic groups were acute stress reaction, adjustment disorder, and depression, which are closely related to acute life stressors, reiterating the importance these stressors may play in attempted suicide in the local context. Malays had more frequent diagnoses of acute stress reaction but a lower rate of depression compared to Chinese. This could reflect some protective effect of close-knit families and social support that appears common among Malays, which might help them overcome stressors, and prevent acute stress reaction from progressing to depression.
Religion was noted as a protective factor more commonly among Malays and Indians compared to Chinese. This may be due to Malays and Indians placing more emphasis on religion than Chinese, who have a higher percentage of atheists (Census of Population 2010 Statistical Release 1, Singapore, 2010). Receiving support from dependents was noted to be a protective factor more often for Malays. A local study tracing suicide cases from 1955 to 1984 found an association between social bonding and suicidal behaviors in Indians, but not in Chinese or Malays (Lester, 1998).
Limitations
Our study has important limitations. Our sample comprised mainly younger adults who were admitted to the medical wards of a university hospital but not those who were certified dead at the suicide scene and the elderly. Therefore, our results may not be generalizable to other age groups of people who attempted suicide and those who did not seek medical help after their suicide attempt. Furthermore, this is a single-centre study and may not be representative of the entire Singapore population. The measures and indices of the suicide assessment checklist form were based on clinician judgement and the interrater reliability was not established. Nevertheless, the form was originally designed as a clinical tool and it has been used in the hospital for almost 10 years. Recall bias was also inevitable in this archival retrospective study. Future research should involve more hospitals, nonclinical samples, and having a broader range of age groups, so as to provide a more complete picture to the suicide scene. There is a need to conduct further studies with validated measures canvassing a wider array of variables.
Conclusion
Our study has documented some differences in the characteristics of patients in Singapore from different ethnic groups hospitalized for suicide attempts. Each ethnic group has one unique risk and protective factors or suicide due to sociocultural background.
Suicide is a complex and multifacetted problem that requires multidisciplinary efforts for prevention. In view of the distinctive profiles of suicide in Asia, there is a need to design interventions that are sensitive to the specific socioeconomic, cultural, and religious context. Social support is an important protective factor against suicidal behavior. The use of community-based suicide intervention programmes involving various resources such as family, religious groups, community centers, and organizations can enhance the connectivity of individuals in the community. Involvement of religion in suicide prevention may be more useful among Malays and Indians.
In Singapore, rates of suicide are higher among adults 31–40 years of age compared to other age groups. Increased public education, access to self-help, and antisuicide campaigns targeted at individuals in this age group are needed, because they face high levels of stress as they transition to taking on more social roles and responsibilities. Workplace programmes may be an effective way to deliver mental health promotion. The prominent role that acute stressors play in suicides in this region accentuates the importance of increasing accessibility of counseling services such as setting up more 24-hour crisis telephone helplines and social service centers, and improving impulse control through teaching of problem-solving/coping skills to at-risk individuals. In addition, given that interpersonal conflicts were identified as significant stressors in our study, the focus of suicide prevention on effective communication, managing of relationships, and emotion regulation may contribute to a reduction in suicide rates. Suicide prevention needs to consider cultural and religious factors to be most effective in a multiethnic country such as Singapore.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None for all authors.
Acknowledgements
We gratefully acknowledge the support of the Department of Psychological Medicine, National University of Singapore. We also thank all who have helped out with the research.