
Abstract
This article seeks to understand to what extent cultural engagement and substance use risk factors influence families’ decisions to participate, and ultimately complete, a culturally grounded substance use prevention program. Using data from a 14-week culturally oriented family-based substance use prevention program, we examine predictors of successful recruitment and retention of American Indian youth and their caregivers. Guided by the theoretical model for developing culturally specific preventions, the community-based approach to recruitment resulted in 85.6% of eligible families from two American Indian communities agreeing to participate in the randomized controlled trial. After completion of baseline surveys, 57.3% of the intervention selected families initiated participation in the program sessions and 67.8% of these families completed participation in the program. We used logistic regression to analyze two different models: one that predicted whether invited families chose to participate and whether participating families attended eight or more sessions. Important predictors of participation in the intervention program included single-caregiver households, youth Indigenous language and cultural identity, youth early substance use initiation, and household substance use exposure. Overall, results from this study highlight the importance of fully engaged community research partnerships for multi-session family-based interventions, while identifying potential challenges to program recruitment and participation.
Introduction
Substance use and abuse is a serious public health concern for American Indian tribes. American Indian youth have high prevalence of substance use (Stanley & Swaim, 2015; Whitbeck et al., 2014; Whitesell et al., 2014), which increases the risk for long-term substance abuse and related health issues. Swaim and Stanley (2018) found that American Indian youth in the eighth grade had significantly higher rates of alcohol and drug usage compared to a nationally representative sample of U.S. youth. In addition, American Indian and Alaskan Native (AI/AN) adults had the highest rates of death due to drug poisoning and alcohol compared to all other race/ethnicities (Shiels et al., 2020). There is a clear need for intervention prevention programs to protect American Indian youth from the early initiation of substance use.
The development of a substance use prevention program among diverse American Indian communities presents unique challenges (Lowe et al., 2016; Whitesell et al., 2012). Historical traumas such as colonialization and systemic discrimination leave a legacy of mistrust with researchers and institutions (Pacheco et al., 2013). In addition, strong cultural norms of sharing and inclusion are at odds with standard research methods such as randomized trials. In fact, many researchers have recommended that AI/AN prevention programs incorporate aspects of cultural values or beliefs into program curriculum (Walsh & Baldwin, 2015).
Culturally adapted, family-based, prevention programs appear to hold the most promise (Ivanich et al., 2020; Lowe et al., 2016). However, to achieve their promise, the programs need to be designed and implemented to overcome both structural barriers encountered in obtaining broad-based program participation such as access to childcare, transportation, time demands, as well as attitudinal barriers related to perceived treatment and beliefs about the providers or researchers (Mendez et al., 2009; Spoth et al., 1996).
Previous research has identified multiple barriers associated with recruitment and retention of participants in prevention programs such as efficacy, cultural alignment, motivations, and community support (Barrera et al., 2013; Michalopoulos et al., 2015; Supplee et al., 2018). In particular, programs that require the involvement of both an adult caregiver and the child, as well as involvement in multiple sessions, present challenges for engagement and completion (Spoth et al., 1996). These barriers may be exacerbated if the prevention content is not culturally relevant and appropriate.
The goal of this study is to examine factors that may affect program engagement and completion of a multi-session, family-based, and culturally adapted American Indian youth substance abuse prevention program. Specifically, we were interested in how youth and adult cultural engagement may influence a family's decision to participate in and complete the program. Likewise, we were curious to see to what degree youth and adults’ substance use might affect whether families engaged with the program. Using data from the randomized controlled trial (RCT) of the Bii-Zin-Da-De-Dah (BZDDD: Listening to One Another) intervention program, we used logistic regression models to examine factors associated with program recruitment and retention. BZDDD is an American Indian youth substance use prevention program with a history of sustained use and development in collaboration with American Indian and Canadian First Nation tribes. This culturally adapted, multi-session, family-based program provides an ideal context for systematically assessing the complex mix of factors that predict active participation and program completion.
Prior research
Family-based intervention programs
The effectiveness of substance use prevention and intervention programs is contingent on successful recruitment and retention of the target population. Recruitment and retention challenges are especially pronounced when the programs are family-based, requiring time commitments from multiple family members (Snell-Johns et al., 2004; Spoth et al., 2000). Research on recruitment and attendance rates in family-focused intervention and prevention programs addressing public health issues reveal that participation rates have often been low (Ingoldsby, 2010; Spoth et al., 1997; Williams et al., 2010). Low recruitment and completion rates can greatly diminish the potential impact of an intervention (LoBraico et al., 2021; Nix et al., 2009).
Examinations of various logistical and socioeconomic barriers to participation in intervention and prevention programs provide insight into factors that need to be addressed to ensure higher levels of engagement. Logistical barriers include difficulties in scheduling around parental work, transportation, and finding childcare for children not in the program (Garvey et al., 2006; Gul & Ali, 2010). These types of barriers are more commonly encountered by low income families and are often exacerbated in rural communities (Redmond et al., 2004; Smokowski et al., 2018). For example, LoBraico et al. (2021) identified key factors that contributed to declining attendance rates in a universal family-based preventive intervention program including low-income status, low school engagement, and engagement with deviant peers.
Another set of factors influencing recruitment and attendance rates are tied to the attitudes and beliefs of the families (Benish et al., 2011; Griner & Smith, 2006; Hodge, 2012). For example, Mendez et al. (2009) note that one of the barriers to participation in family-based services involves attitudinal beliefs about service providers or researchers, who may be perceived as judgmental or non-empathetic, and whether the goals and activities of the program are perceived as relevant to their own needs (Ingoldsby, 2010). Specifically, families are more likely to engage in an intervention when they (a) perceive a need to participate in a treatment program, (b) believe that participation will result in positive outcomes, and (c) have confidence in their ability to create positive change in their lives (Bamberger et al., 2014; Berkel et al., 2011; Kazdin et al., 1997). Strategies for increasing family engagement in prevention programs highlight the importance of understanding the underlying motivating factors for family involvement (LoBraico et al., 2021; Spoth et al., 2000).
Demographic factors have consistently been shown to be associated with participation in intervention programs. For example, youth, and particularly youth of color, from low income families are less likely to be recruited and retained in research compared to peers from middle and upper middle class communities (Ingoldsby, 2010; Mendelson et al., 2021; Prado & Pantin, 2011; Zand et al., 2006). In addition, single-parent status is consistently associated with lower participation rates and increased likelihood of not completing the program, likely due in part to limited economic resources (Baker et al., 2011; Garvey et al., 2006; Snell-Johns et al., 2004). Furthermore, low levels of parental educational attainment have also been shown to be associated with lower levels of participation in family-based prevention (Diaz et al., 2006; Spoth et al., 1997).
Culturally adapted intervention programs
New challenges to recruitment and retention emerge when researchers are working with communities that require greater attention to cultural sensitivity (George et al., 2014; Rathod et al., 2017). Studies have frequently noted that there are additional barriers related to both enrollment and retention of racial/ethnic minority families in prevention and intervention programs (Snell-Johns et al., 2004). For example, scholars have identified additional barriers such as mistrust of researchers and/or providers (Brannon et al., 2013; Kennedy et al., 2010), perceived differences in cultural backgrounds including language barriers (Cooney et al., 2007), and perceived racism or stigmatization (L. Robinson et al., 2016; Winslow et al., 2009). Families are more likely to participate in intervention programs when they successfully address such issues in a culturally appropriate manner (Guerrero, 2013; Nueces et al., 2012; Yancey et al., 2006).
The most appropriate approach to intervention and prevention programs developed for American Indian communities is the need to incorporate their cultural values and beliefs such as reciprocity and equity (Wallerstein & Duran, 2010), resilience (Kahn et al., 2016; Stumblingbear-Riddle & Romans, 2012), and the importance of tribal identity and tribal Elders (Brown et al., 2016; Ivanich et al., 2020; Smokowski et al., 2014). This requires a collaborative research partnership with the communities (Brown et al., 2012; Donovan et al., 2015; Whitbeck, 2006). Fully engaged community-based participatory partnerships between American Indian communities and university researchers provide the foundation required for successful research collaborations and community interest in participating in prevention programs (Gone, 2009; Walls et al., 2007; Whitbeck et al., 2012).
Part of developing trust with Indigenous communities is the recognition and consideration of the history of American Indian communities as subjects of exploitative research for decades (Buchwald et al., 2006; Whitbeck, 2006; Whitesell et al., 2012). Factors shown to have been associated with American Indian community distrust of researchers include Western medical model treatments, not sharing results of the study with the community, failing to provide benefits associated with participating in the research, and racial trauma that has both historical and contemporary consequences (Hodge, 2012; Skewes & Blume, 2019; Skewes et al., 2020). Based upon these types of historical experiences, tribal governments have become more restrictive in their approval of research projects involving outside researchers and have developed their own tribal review boards for research protocols and ethics (Brugge & Missaghian, 2006; Indian Health Services, 2022; Kuhn et al., 2020; Norton & Manson, 1996).
Another important aspect regarding cultural adaptation is learning about the unique strengths and challenges of the local communities. For example, working with communities to ensure local practices are incorporated not only honors local traditions but may also increase program participation (Ivanich et al., 2020; Schmidt et al., 2022). In addition, it is critical to make sure that local needs are addressed in order to effectively support the community. For example, much of the research with American Indian communities is often based on tribal reservations where there are structural disadvantages that exacerbate health disparities and other inequities, such as underfunded and understaffed health services, lack of available access to health treatment facilities, and underfunded educational systems (Gone & Trimble, 2012; Whitesell et al., 2018). Addressing frequently experienced issues such as transportation, distance and expense for traveling to the intervention site, as well as childcare challenges is necessary to improve recruitment and retention (Adams et al., 2008; Hodge et al., 2000).
Designing a responsive intervention
The research literature is clear regarding the multiple challenges faced in developing and delivering a family-based intervention program in cooperation with Indigenous communities. A fundamental research question is whether this unique combination of challenges and barriers can be navigated in a manner that leads to the kind of broad and inclusive participation needed for the interventions to produce maximum benefits for the community. The present study examines this question in the context of a multi-site randomized control trial of a family-based intervention designed to reduce substance use among American Indian pre-adolescent youth aged 8–10. This study was developed as part of the National Institutes of Health's initiative to support Intervention Research to Improve Native American Health (IRINAH) and was approved by the University of Nebraska's Institutional Review Board (IRB #20140214158FB).
The Bii-Zin-Da-De-Dah (BZDDD, Ojibwe for Listening to One Another) program is a 14-week culturally oriented family-based substance use prevention program designed to reduce substance use among youth. The program was delivered in collaboration with two different American Indian tribal communities that share a common culture and language. The initial prevention elements were based upon an adaptation of the Iowa Strengthening Families Program (Spoth & Redmond, 2002). The foundation of the BZDDD program is based upon Whitbeck's (2006) theoretical model for the development of culturally specific prevention research that emphasizes the importance of adapting culturally key constructs of risk and resilience into the program. It also requires that prevention scientists recognize the independent effects of culturally specific risk and protective factors that are not part of Eurocentric prevention programs. The partnerships formed on this foundation, with fully engaged community-based participatory research, have resulted in a sustained collaboration for developing, revising, and sustaining BZDDD (Whitbeck et al., 2014).
The BZDDD program, from its initial development, has been based upon the standards established for ethical research with American Indians (Baldwin, 1998; Beauvais, 2018; Harding et al., 2012; Kovach, 2015; Norton & Manson, 1996). The research team worked with the community to obtain approval from the tribal governments for each reservation. Tribal approved Advisory Boards were established on each reservation and provided oversight for the project including advising on personnel matters, input on prevention program components, conducting reviews and making recommendations on questionnaires, approving family recruitment procedures, and pre-reviewing papers and reports to ensure cultural sensitivity. The Tribal Resolutions, and the data sharing plans on the funding proposals, specify that the tribes will maintain control over the intervention materials and research data. Combined with established commitment to hire and train Tribal residents to work on the research and intervention team, these efforts have contributed to the acceptance and sustainability of the BZDDD intervention.
In addition to the community-based research design and implementation, the BZDDD project addressed many of the considerations that have been shown to impact broad-based community participation and completion of multi-session family programs (Coday et al., 2005; K. A. Robinson et al., 2007). For example, practices for requesting participation were designed and implemented with particular consideration given to the cultural importance of community ties (Ivanich et al., 2020). Flexibility was designed into the sessions, by offering a second round in case circumstances arose that kept the family from making it to a session. Korfmacher et al. (2008) have reported that a flexible program structure that is responsive to difficulties encountered in lower-resource areas is likely to increase family engagement. Other design elements incorporated extrinsic rewards such as food and celebrations that are consistent with increased recruitment and participation rates and are examples of cultural norms of reciprocity (Ivanich et al., 2020; Skewes et al., 2020; Staudt, 2007). Finally, scholars note the importance of collaborative processes in recruitment, participation, and retention in research such that communities are equal stakeholders (Hodge, 2012; Skewes & Blume, 2019). Equity includes translation and dissemination of research findings through discourse that is culturally appropriate, integrating cultural beliefs and values into the program (Christopher et al., 2011; Hodge, 2012; Wallerstein & Duran, 2010).
The BZDDD project was designed to get the community engaged in conversations about cultural strengths and the well-being of children and families. One notable effort in this aspect involved tribal community leaders, service providers, and Elders in videos that were made for the project curriculum and which validate the expertise and experiences of the community (Ivanich et al., 2020). Additionally, the BZDDD project integrated traditional values and provided enhanced opportunities for youth to interact with Elders through activities such as talking circles and learning to offer traditional tobacco to Elders.
This combination of culturally sensitive design, development, and implementation is expected to produce strong enrollment and participation rates. Given the required time commitment for families experiencing challenges with limited resources, another key outcome is whether the program is successful in recruiting and retaining youth who are at greater risk. We anticipate that, as developed and delivered, the BZDDD program will be successful in engaging families and youth who have high risk profiles. Finally, we expect that strong cultural orientation and building upon tribal traditions and strengths will increase participation from families and youth with higher levels of enculturation compared to prevention programs designed from a westernized perspective.
Methods
BZDDD was designed as a multi-site randomized control trial for American Indian pre-adolescent youth aged 8–10 (for more details on the cultural adaptation, see Ivanich et al., 2020). This age range was selected in an effort to reach the youth prior to the initiation of substance use which typically occurs around 12–14 years of age, with early onset starting as young as 11 years old (Hautala et al., 2019; Sittner et al., 2021; Whitbeck & Armenta, 2015). The program was administered in two different American Indian communities that share a common language, culture, and history. Local recruiters made traditionally respectful home visits to families designated to be eligible by each community, where they introduced themselves and spent time informally chatting with families prior to discussing the program. For a family to be considered eligible there had to be a youth living in the home between the ages of 8–10 and an adult caregiver willing to consider participation. Families were informed that all families and youth would be provided the opportunity to participate in the intervention program, either as the assigned intervention group or a wait-list control group. Families that declined enrollment, moved, or were unreachable after the initial visit were excluded from program enrollment. For additional details about the recruitment strategy, please see Habecker and Ivanich (2020).
The intervention consisted of 14 weekly family sessions that were held in a reservation community building selected with the guidance of the Prevention Research Council (PRC). Local program facilitators received two days of extensive training on the BZDDD curriculum, program materials, and general facilitation techniques. The first four sessions focused on elements of Anishinaabe history and culture such as values and beliefs of the Anishinaabe people, increasing family communication by using Talking Circles, and characteristics of a “good way of life” (Bimaadiziwin). The other 10 sessions covered potential risks for and development of protective factors against substance use. For example, weeks 5 through 8 addressed how to identify feelings and manage negative feelings in a positive way. Weeks 9 through 13 concentrated on outside influences and building positive support systems. The 14th session was a celebration ceremony to honor the families’ participation and community support.
Sample characteristics
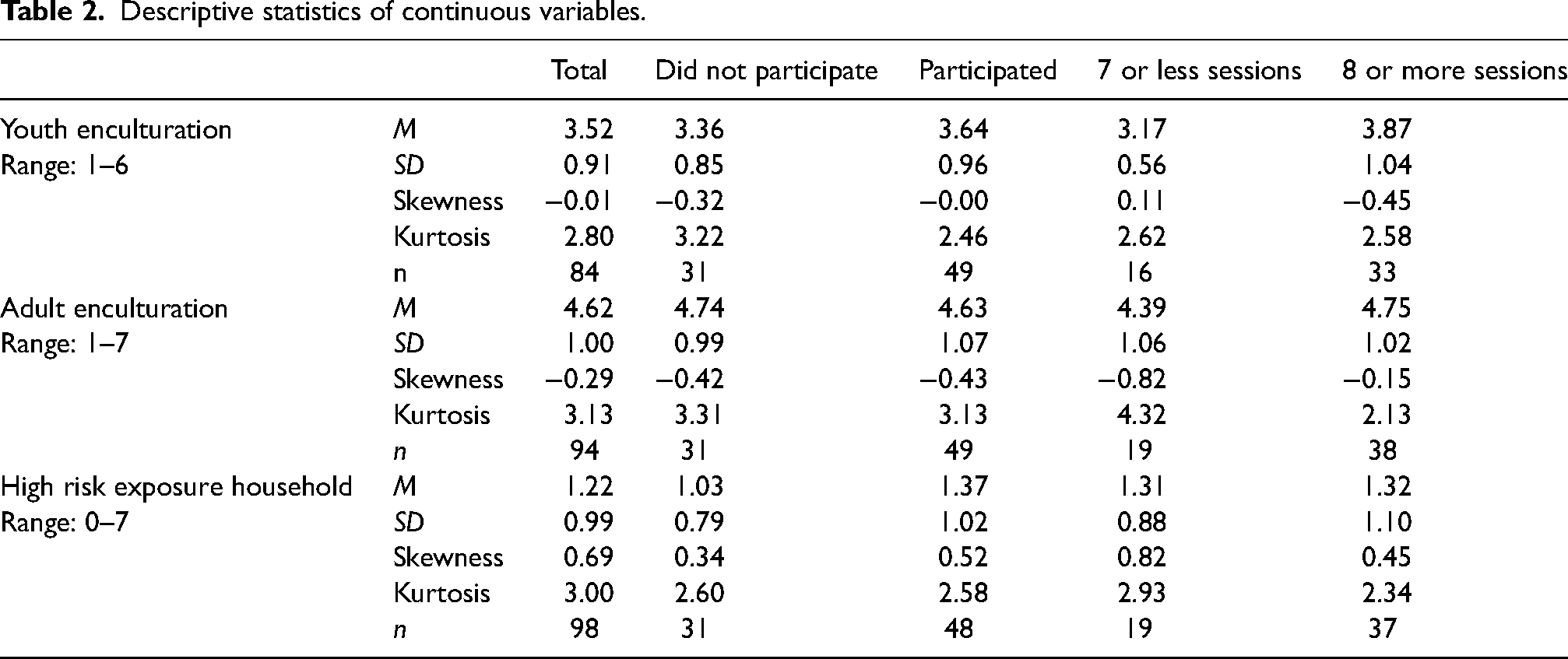
The initial process resulted in the identification of 243 eligible families who completed a short interest form indicating they wanted to learn more about the program. The baseline interviews began in May 2017 and concluded in April 2018, resulting in successfully conducted interviews with 208 families. Thus, the preliminary recruitment rate was 85.6%, supporting the expectation that the culturally specific, community-based, approach would increase engagement compared to generic intervention programs (Kumpfer et al., 2002). For example, the first iteration of BZDDD hosted in 1996 had a recruitment rate of 79.4%, which was a significant improvement over the original program it was adapted from (SFP) and which had recruitment rates ranging from 51% to 68% across various implementations (Spoth & Redmond, 2002; Whitbeck et al., 2014). Participants were fairly evenly distributed across the two communities with 56.7% from community A and 43.3% from community B. Tables 1 and 2 include the descriptive statistics of the total sample, along with a breakout by participation and completion groups. Additional information on enrollment and recruitment can be found in the CONSORT flow diagram in Figure 1.
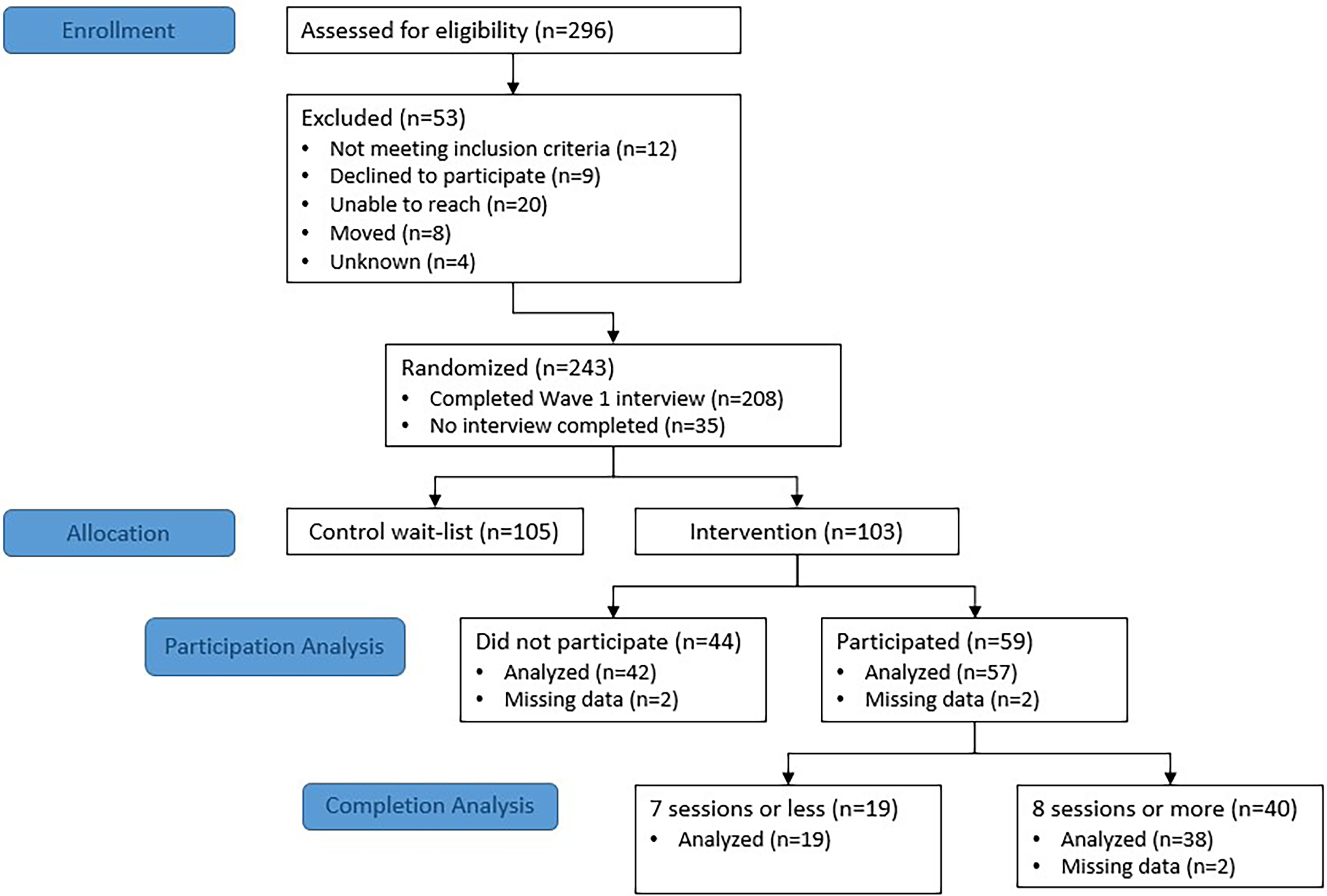
CONSORT flow diagram.
Descriptive Statistics of Categorical Variables.

Descriptive statistics of continuous variables.
Measures
To measure recruitment, we created a binary variable to indicate whether invited families actively participated in the program. Recruitment was defined as a family that attended one or more sessions (code = 1). Invited families that did not attend any sessions were coded as 0. Of the 103 families invited to attend, 59 (57.3%) attended one or more sessions while 44 (42.7%) attended none. Another outcome of interest was program completion. Since it is unrealistic to expect all families to attend all of the sessions, we selected completing over half of the sessions (eight or more) as the cut point based upon the work of Spoth et al. (1999), who found dosage-related effects for youth who attended more than half of the SFP intervention sessions. Of the 59 families that attended one or more sessions, 40 (68%) attended eight or more sessions while 19 (32%) attended seven sessions or less.
Youth alcohol and drug use was based on whether the youth had ever consumed alcohol, smoked a cigarette, used marijuana, prescription pills, or any other substance to get high. A binary measure was created with never having used any substance coded as 0 and having used any of these substances was coded as 1. Just over 1 in every 10 youth (13.4%) had initiated some substance use. We included this measure because we believed that families of youth who had not yet initiated substance use may see less need for the program and be less likely to participate (Salas-Wright et al., 2019).
A measure of household substance use exposure was created to assess proximity of the youth to substance use, independent of their own initiation. This measure is a seven-item scale, reported by the adult caregiver, tapping exposure to cigarette, alcohol, and marijuana use by adults living in the same household as the youth. The seven indicators were dichotomous yes or no responses summed to create a 0–7 scale (M = 1.22). Households where children are exposed to substances, whether by handling those items for family members or by seeing family members use them, may be less likely to participate in a substance use prevention program due to potential stigmatization (Schomerus, 2014).
Youth culture consists of a measure of cultural/ethnic identity and native language skills. Youth cultural/ethnic identification was measured using a modified version of the Multicomponent Measure of In-group Identification scale (Leach et al., 2008). The measure consists of six items with a scale of Strongly Disagree (1) to Strongly Agree (4). The questions asked about the importance of and identifying as Anishinaabe, in addition to feeling a connection to, being proud of, and being committed to the Anishinaabe people. Youths’ familiarity with the Ojibwe language was measured using five items that asked about the ability to speak some words or carry on a conversation in Ojibwe, and knowing someone who can carry on a conversation in Ojibwe (0 = no, 1 = yes). Youth were also asked how often Ojibwe is spoken in their home with four response options ranging from every day to never that were then dichotomized into categories of “Never or only on special occasions” = 0 and “Some of the time or every day” = 1. Finally, youth were asked if they understood Ojibwe when it is spoken. Responses were dichotomized into “No or some words” = 0 and “Most or all words” = 1. The ethnic/cultural identification scale measures were converted into a scale ranging from 0–1 and then added to the language scale items. The ethnic/cultural identification and language items were equally weighted and summed together (range 0–6, mean 3.52). The combined scale has a Cronbach's alpha reliability score of .731.
Adult ethnic/cultural identification was measured using a modified version of the Multicomponent Measure of In-group Identification scale (Leach et al., 2008). The questions asked about their connection, pride, commitment, happiness, knowledge, and self-identity associated with being Anishinaabe. The measure consisted of eight items on a scale of Strongly Disagree (1) to Strongly Agree (4). These item responses were then recoded so that each question response ranged from 0–1. Adults’ familiarity with the Ojibwe language was measured using five items where adults were asked if they speak some Ojibwe beyond a few common words, if they can carry on a conversation in Ojibwe, and if they know anyone who speaks Ojibwe fluently (0 = no, 1 = yes). Respondents were also asked how frequently Ojibwe is spoken in their home with four response options ranging from never to everyday. Reponses were dichotomized into “Never or on special occasions” = 0 and “Some of the time or everyday” = 1. Finally, adults were asked if they understand what is being said when they hear Ojibwe with four response options ranging from none to all. Responses were dichotomized into “None or some words” = 0 and “Most words or all” = 1. The ethnic/cultural identification and language items were equally weighted and summed together (range 0–7, mean 4.63). The combined scale has a Cronbach's alpha reliability score of .763.
The following demographic variables were included as controls: youth gender (0 = male, 1 = female), parental education (0 = high school education or less, 1 = greater than high school education), whether the participant lived on the reservation (0 = no, 1 = yes), and the caregiver structure of the youth's household (0 = two caregivers, 1 = single caregiver). The distributions of these variables are available in Table 1.
Data analysis
For the analysis, we were interested in how various factors affected successful recruitment and retention. There were two types of models analyzed, those that looked at factors associated with whether invited families chose to attend the program (participation models) and whether families completed eight or more sessions of the program (completion models). The first participation model included only the demographic variables and included 99 families as those missing basic demographic data were removed from the analysis (n = 4). For the second recruitment model, we added measures of youth culture and adult culture to the model. Observations with missing data on the culture measures were dropped from the model (n = 19). The last recruitment model added a measure of youth substance use and household substance use exposure. Observations missing data on these measures were also dropped (n = 2).
The structure of the completion models was the same, although the outcome variable was whether the family completed eight or more sessions. A total of 59 families attended at least one or more sessions of the program. For the first model with only demographic variables, families with missing data were dropped from the analysis (n = 2). The youth and adult culture measures with missing data were dropped from the next model (n = 8). In the third model, youth substance use was not included due to the small sample size and how few youths had used substances at Wave 1. The household substance use exposure measure was added and families with missing data dropped (n = 1).
Since both outcome variables are binary (attended one or more sessions or did not attend; attended eight or more sessions or not) the data were analyzed using logistic regression models in Stata 15.
Results
Active participation in BZDDD
We wanted to identify factors that may be associated with families’ decision to actively participate in BZDDD. Note that we define active participation as attending one or more sessions of BZDDD. Of the 99 families invited to attend BZDDD first (the intervention group), a total of 57 (57.6%) actively participated. For most comparisons, there was not a significant difference between families that did not attend and those that actively participated. Mean differences and frequency distributions can be found in Table 1. In one case, the distributions did significantly differ between the families. Of families that chose not to attend, more youth had already initiated some substance use (21.4%) compared to youth in families that actively attended (7.3%).
The first logistic regression model analyzed predictors’ effects on the probability that a family chose to participate versus not to participate in the BZDDD program (Table 3). The first model showed no substantial effect sizes nor significant effects for the gender of the youth, parental education, community, or reservation residency. The model did show a substantive effect size for caregiver composition, with single-caregiver households nearly twice as likely to participate in the program (OR =1.959, p = .109). Given the small sample size this effect does not reach the level of statistical significance.
Logistic regression predicting recruitment into the intervention.
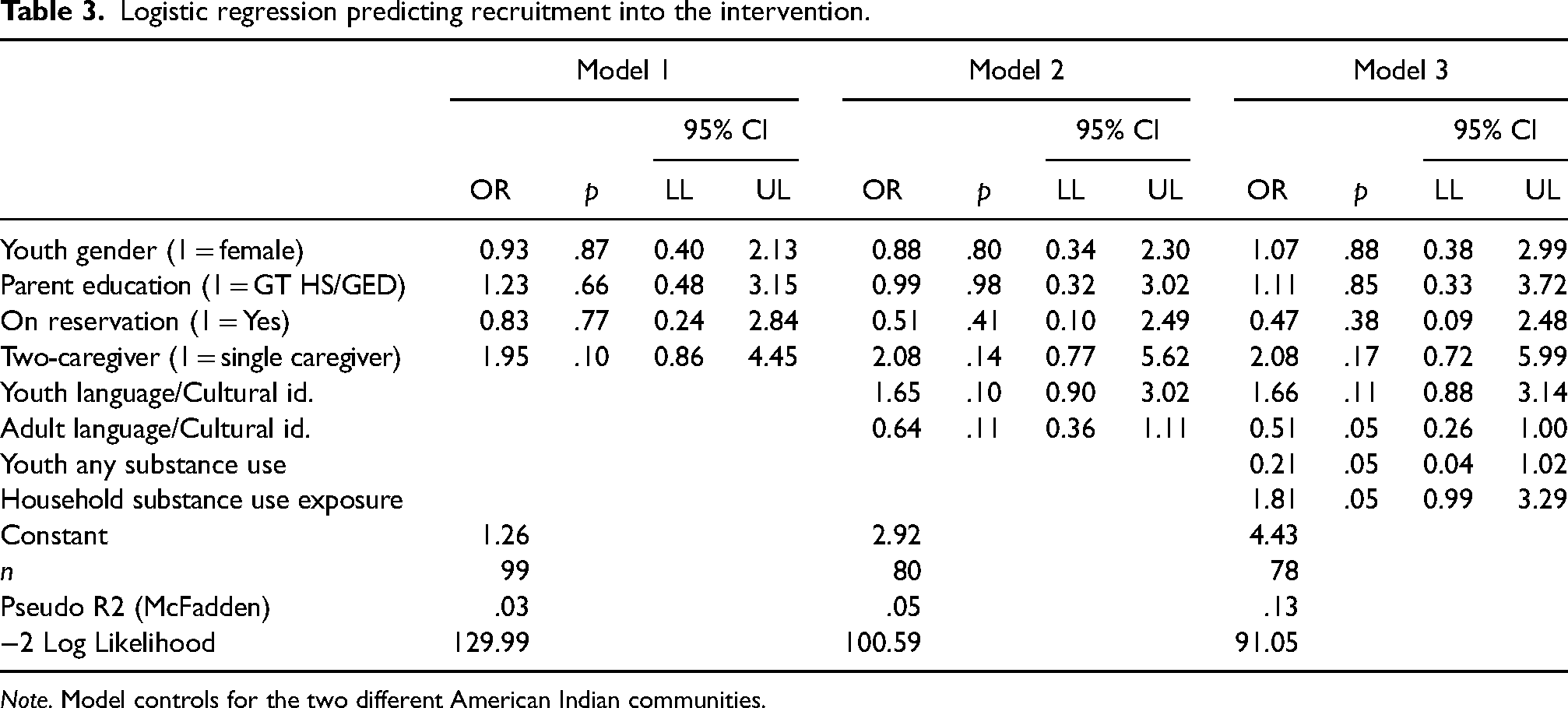
Note. Model controls for the two different American Indian communities.
The measures of youth and adult cultural scores were added in the second model. Judging solely on statistical significance, just one of the effects reaches the .10 level set for these small sample data. Each one-unit increment in the level of youth language and cultural identity is associated with a one and two-thirds increase in the odds of participation (OR = 1.657, p = .101). As with the first step, there is a large effect size, but not quite reaching statistical significance for household structure. Single-caregiver households were twice as likely to participate in contrast with two-caregiver households (OR = 2.086, p = .146). Another non-significant substantive effect is found for parent's language and cultural identity. Each unit increase in this identity measure is associated with a 0.64 times decrease in participation (OR = 0.641, p = .116).
In the final step, youth substance use and household substance use exposure were added to the model. The substance use and exposure measures are both significantly related to program participation. Youth who had already engaged in some form of substance use were less likely to participate in the intervention program (OR = 0.213, p = .053). In addition, exposure to adult substance use was significant, with a 1.8 times increase in odds of program participation with each unit increase in adult substance use (OR = 1.810, p = .053). With these substance use measures in the model, the adult's language and cultural identity is significantly associated with an approximate 50% decrease in the odds for program participation (OR = 0.519, p = .050). Youth language and cultural identity demonstrate a similar pattern for odds of participation as in the prior model (OR = 1.665, p = .116). Similarly, the observed pattern for single-caregiver households was sustained (OR = 2.088, p = .172).
Program completion
The second set of models examined program completion among the families who participated in the intervention. For this model, the dependent variable is program completion, which is defined as attending more than one-half the sessions. Of the 59 families that participated, 40 families (67.8%) attended eight or more sessions (Table 4).
Logistic regression predicting program completion (8 + sessions).
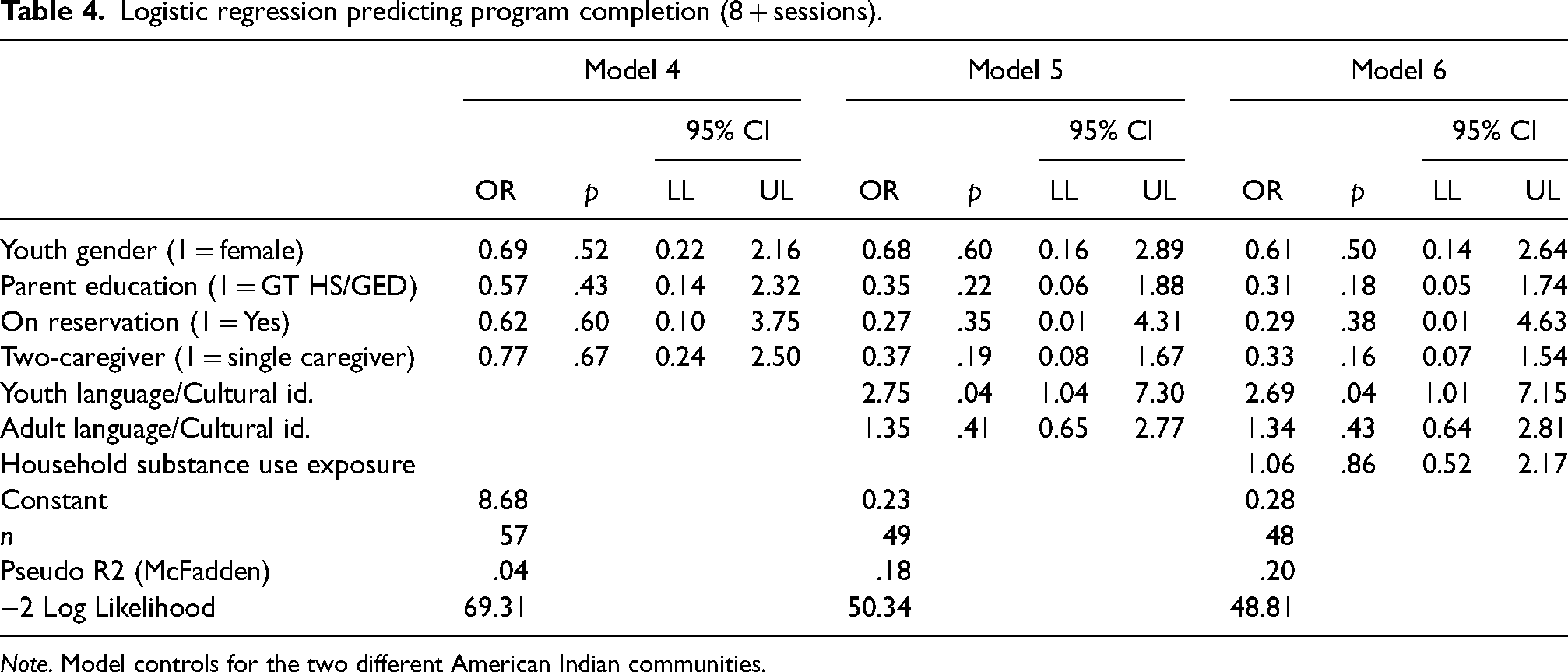
Note. Model controls for the two different American Indian communities.
The first logistic regression model includes the same demographic measures as examined in the participation model; youth gender, parent's education, living on or off the reservation, two-caregiver household, and community. None of these demographic measures had significant effects on program completion. The second model added in the measures of youth and adult cultural engagement and showed results similar to model 1 (OR = 2.758, p = .041). Each unit increase in the youth's cultural score is associated with a 2.76 times increase in the odds of completing the program. The adult cultural score was not a significant predictor.
Household substance use exposure was added to the model in the final step. Youth substance use was not included due to the very small number of youths who had previously used a substance prior to attending the program. Household substance use exposure was not a significant predictor. However, youths’ cultural scores retained their effect size and continued to be significant (OR = 2.690, p = .047).
Summary and discussion
The strong initial level of interest and completion rates among participating families all point to the strengths of the culturally adapted approach that is designed as a research partnership between the participating tribes and the university research team. The preliminary recruitment, a rate of 85.6%, is exceptional when taking into consideration the required elements of both caregiver and child program participation, in addition to the commitment to multiple waves of assessment for both the treatment and wait-list groups. While we do not have specific data on why people chose to participate, the culturally specific community-based approach to recruitment is clearly an important factor for an increased level of engagement in both reservation communities as has been demonstrated in previous research (Lowe et al., 2016; Okamoto et al., 2014; Skewes et al., 2020).
Culturally adapted recruitment methods were used to describe the requirements of the intervention program and gain consent of the families to participate. While preliminary recruitment in the program was high (85.6%), the rate of actively participating in the program was lower (57.3%). The length of the program may have been a deterrent for some families. While the number of sessions was necessary to fully incorporate the communities’ desire for more cultural content, the duration of the program may have prevented some families from participating. Such recruitment challenges are not unique to BZDDD (Lowe et al., 2016; Whitesell et al., 2012) and highlight the ongoing need to evaluate dosage effects in order to arrive at an optimal program length that incorporates cultural content with substance use prevention outcomes.
Another challenging aspect of the program was to get families to completion without dropping out (LoBraico et al., 2021; Spoth et al., 1997). Among families that attended one or more sessions, the BZDDD program had a completion rate of 67.8%. This may be due in part to addressing the types of barriers faced by many of the families. For example, family availability could be limited due to local practices such as hunting or subsistence leave, school events, weather, or financial issues. To alleviate the burden of attending a higher number of sessions, the BZDDD team offered second opportunity sessions for families who encountered unanticipated difficulties in attending the initial sessions. While this type of adjustment is guided by the theoretical model for developing culturally specific preventions (Whitbeck, 2006) and is essential to the successful implementation of the intervention program, the opportunity to further increase participation remains.
Considering these challenges, we examined how recruitment and retention may be affected by youth and adult cultural engagement. The level of the youth's cultural identity and native language awareness was associated with substantively higher levels of family participation in the program. The positive association can be an advantage for culturally adapted programs by engaging with youth in a way that honors their culture. It is important to note that our operationalization of youth and adult enculturation is limited to measures of cultural identity and tribal language, which excludes engagement in several types of diverse cultural practices. We made this decision because we believe that cultural identity, which can be developed through cultural practices, was the best overall measure to use given the limited sample size. We included the Ojibwe language measures because of how important incorporating Ojibwe into the program was to the tribal communities. Clearly this is one of many ways to measure how cultural elements may impact program recruitment and retention. Results may change if other measures were used in addition to these measures.
While not surprising, households where youth had already initiated some substance use were less likely to participate in the program, although it is difficult to say if that is more attributable to the youth or the adult. For example, of the 13 youth who indicated they had tried some type of substance, only three of the adults indicated they knew the youth had tried a substance. Out of those three families where both the youth and adult acknowledged youth substance use, only one of the families attended the program. Overall, in families where the youth had initiated some form of substance use, the likelihood of participation was approximately 20% less than non-substance initiated youth. These findings highlight the importance of connecting youth and their families with substance use prevention programs prior to the youth engaging in substance use.
Another impact of substance use was found for household substance use exposure. For each one unit increase in exposure, the odds of participating in the program increased by a 1.8 times. In other words, while controlling for youth substance use initiation, families had a significantly increasing likelihood of participation in the program with increasing levels of adult use. This may be due in part to the community-based efforts to increase awareness of substance use among youth, which may have been successful in raising awareness and overcoming resistance that might be associated with households where there is more adult engagement in substance use.
A particularly encouraging finding from this study is the high level of participation from single caregivers, a segment of the population that is often difficult to successfully engage in multi-session family-based intervention programs as they may be more likely to experience the logistical barriers that often hinder participation (Garvey et al., 2006; Gul & Ali, 2010). Single caregivers participated at a rate of 58.0%, which is significantly higher than two-caregiver households (42%). In the logistic regression model, single caregiver households were nearly twice as likely to participate in the program while controlling for other factors. However, the caregiver measure did not significantly predict program completion. It may be the case that after recruiting single caregiver households to participate, they could face the biggest challenges in meeting the logistical demands of attending multiple sessions.
The challenge in interpreting the findings associated with the effect of single and two-caregiver families highlights an important limitation for the present study. Overall, the small sample size places some constraints on our ability to rely solely on traditional significance level testing. With our limited sample size, we use p < .10 as a starting point for examining associations. We supplement this with a consideration of the associated effect sizes that convey the magnitude of the effect (Durlak, 2009). There are portions of these analyses where the effect sizes point to potential substantive differences. While limited, this approach permits the consideration of unexpected patterns and helps set the stage for important new questions and hypotheses in future studies.
Increasing the sample size is an obvious recommendation for further investigating the patterns identified in this study and an important consideration in research designed to replicate and expand the findings from this study. One particular challenge to this effort is the relatively small population sizes on American Indian reservations that is then exacerbated by limiting the research to families with children in the program delivery age range (Whitbeck et al., 2012). It is possible to address the small reservation population challenge by developing randomized controlled trials for intervention programs across multiple reservations. However, that then introduces new statistical analysis challenges associated with the nested sample design. Clearly, we need to be able to develop, deliver, and evaluate substance use intervention programs in the context of small rural American Indian reservations. The findings from this study point to important risk and resilience factors that are likely to be, in some respects, unique to this context.
Future studies may strongly benefit from a mixed-methods approach by employing semi-structured interviews with youth and caregivers, providing greater insight into their individual and shared motivations for participating in the program and continuing to attend sessions. Qualitative data could reveal important information for communities and researchers to better understand and address community interest in the program, while working to remove barriers to participation.
This study demonstrates the importance of fully engaged community research partnerships for multi-session family-based interventions. The most significant key to community engagement was ownership of the prevention program. Community leaders supported the program and various agencies facilitated recruitment. All the cultural content originated from Anishinaabe communities including activities, values, and language. Also, all program recruiters and facilitators were community members. The very high preliminary participation rate and the strong program completion rate among those who actively participated, each demonstrate the benefits of building and sustaining community engaged participatory research. There is clear evidence that the traditional cultural engagement of the youth enhances program participation and completion. This reinforces the significance of participating tribes’ efforts to increase youth exposure to traditional cultural values, practices, and language. This study reinforced the importance of engaging youth and their families in preventive interventions at ages early enough to be prior to initiation of youth substance use. Families with youth who had initiated substance use were much less likely to participate in the program. Finally, the single caregiver findings point to very important considerations as we move to the next stage of interventions. The high participation rate for single caregiver households demonstrates that these caregivers want to seek help in preventing youth substance use. However, the lower program completion rates for single caregiver households indicates that we need to develop more comprehensive support to make it possible for these families to fully benefit from these programs.
Footnotes
Author note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the University of Nebraska.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute on Drug Abuse of the National Institutes of Health [R01DA037177], Les B. Whitbeck, Principal Investigator. Additional support was provided by the National Institute of General Medical Sciences of the National Institutes of Health [P20GM130461] and the Rural Drug Addiction Research Center at the University of Nebraska–Lincoln.