
Abstract
This mixed-methods study examined providers’ experiences using a structured developmentally sensitive tool to assess transition readiness for youth with special health-care needs moving from pediatric to adult care. Twenty-eight health-care providers from three pediatric specialty clinics reported their experiences using the tool by surveys and semistructured telephone interviews. Qualitative data were analyzed using thematic analysis. Most (96%) believed routine practice should include a structured tool; 65.7% incorporated information from the tool into patient care plans. Salient themes pertained to practice behavior changes and implementation barriers. Integrating structured tools into standard clinical practice has the potential to optimize transition and improve patient care.
Introduction
Pediatric to adult health-care transition is an important topic of widespread interest in the United States and internationally (Schwartz et al., 2014; Stinson et al., 2014; Zhang et al., 2014). New technologies and treatments have dramatically changed the outlook and prognosis for youth with special health-care needs (YSHCNs) (Elias and Murphy, 2012). As YSHCNs are increasingly living longer and facing adolescent and adult challenges, new responsibilities have been placed on the health-care system to care for these patients and to respond to the medical, developmental, and psychosocial needs of this vulnerable population as they transition from child-oriented to adult-oriented health care (American Academy of Pediatrics (AAP) et al., 2011). More recently, the AAP (2017) provided guidelines suggesting avoidance of arbitrary age limits and creation of very individualized plans. This recommendation places more responsibility on providers to first fully understand a patient’s development and potential barriers to self-management and subsequently provide guidance for successful transition and transfer. Proactive identification by the interdisciplinary health-care team of both the patient’s developmentally appropriate knowledge and skill mastery thus provides a starting point for ensuring medical independence in adulthood, which we define as the capacity of an individual to manage one’s own health-care needs and associated care decisions. Assessment of a patient’s current capacity for skill management and provision of family education are integral components of transition counseling and care for YSHCN (Osterkamp et al., 2013).
The process of transition encompasses the development of medical autonomy and self-care behaviors for all youth. Kieckhefer and Trahms (2000) outline a model that incorporates developmental milestones as well as a ‘planned and systemic leadership transition’ in which the patient becomes the ‘CEO’ of his/her own care. Adolescents and young adults who have not incorporated the necessary skillset to master these self-efficacy behaviors may be at increased risk for nonadherence to treatment and loss of follow-up care, potentially resulting in poor health outcomes (Department of Health/Child Health and Maternity Services Branch, 2006). In addition, providers who are aware of a patient’s psychosocial stressors may be able to address those factors, which might otherwise interfere with learning, skill mastery, and the ability to achieve medical independence (Pai and Ostendorf, 2011; Shanske et al., 2012; Viner, 2008).
Although there is emerging awareness that this process should begin early (Lewis, 2013; Swanson, 2010), there is no consensus of what ‘early’ is. Based on the authors’ clinical experience and accepted developmental expectations (Hagan et al., 2017), the authors identified milestones as they related to medical skill mastery, acknowledging that young children can be active participants in their care. For example, a three-year-old patient can use language to name their condition (‘bedes’ for diabetes) and be able to describe symptoms or discomfort (‘belly hurts’).
Existing validated transition tools generally begin in early adolescence (Schwartz et al., 2014). Although some are also generalizable across diseases (Ferris et al., 2012), the unique feature of our tool is that it is not only generalizable but also starts as early as birth. Most tools also rely exclusively on parent or patient self-report and lack outcome measures (Burke et al., 2018; Ferris et al., 2012); our tool requires providers to assess using direct observation and interaction. Although patients and families seem to rely on guidance from providers, many young adults report that they have not received health-care transition counseling (Dwyer-Matzky et al., 2017; Sawicki et al., 2011). The lack of validated developmental assessment tools for use by providers may inhibit such counseling.
The authors contend that achieving medical independence is an important stepping stone to eventual successful transition from pediatric to adult care and that health-care providers, when adequately prepared, can facilitate the developmentally appropriate skill mastery required. In addition, the authors maintain both that psychosocial stressors may interfere with effective skill acquisition and that it is helpful to begin assessing transition readiness and preparing for transition—and ultimate transfer—as early as possible. The aim of this study was to pilot test a structured developmentally sensitive transition readiness tool for providers to use with YSHCN to examine its feasibility and utility. Designed to address medical independence and transition readiness, the tool can be utilized at the time of diagnosis (as early as birth), employs both observational and interactional assessment mechanisms, and includes assessment of psychosocial factors.
Methods
This multiphase mixed-methods study employed a concurrent triangulation design, wherein qualitative and quantitative data are collected concurrently. This method was selected intentionally to allow the investigators to cross-validate and corroborate findings from unique qualitative and quantitative data collection methods.
Tool development
Developed by a team of pediatric hospital social workers specializing in YSHCN populations, the tool is comprised of a series of developmentally sensitive assessment instruments for providers to use with patients ages birth to 21 years of age. The assessments, intended to be generalizable to all chronic illnesses, can help determine the proficiency of YSHCN in domains of knowledge acquisition and skill mastery required for medical independence. Age ranges were selected based on clinical experience as well as generally accepted developmental guidelines (Hagan et al., 2017). The tool incorporates observational measures across disciplines with a goal of getting the provider to focus directly on the patient. As such, each skill level is based on reasonable assumptions of appropriate developmental tasks for the age and encompasses physical, emotional, and cognitive development. Because parents are expected to learn health management tasks during infancy and toddlerhood, the authors purposely outlined observable patient behavior skills starting with the three- to four-year-old range. Twenty-four to thirty-six month age ranges for each tool were chosen to align with current child development literature recommendations (Hagen et al., 2017). The authors chose the end point of 21 years because it aligns with the hospital access policy ensuring care to all patients through age 21.
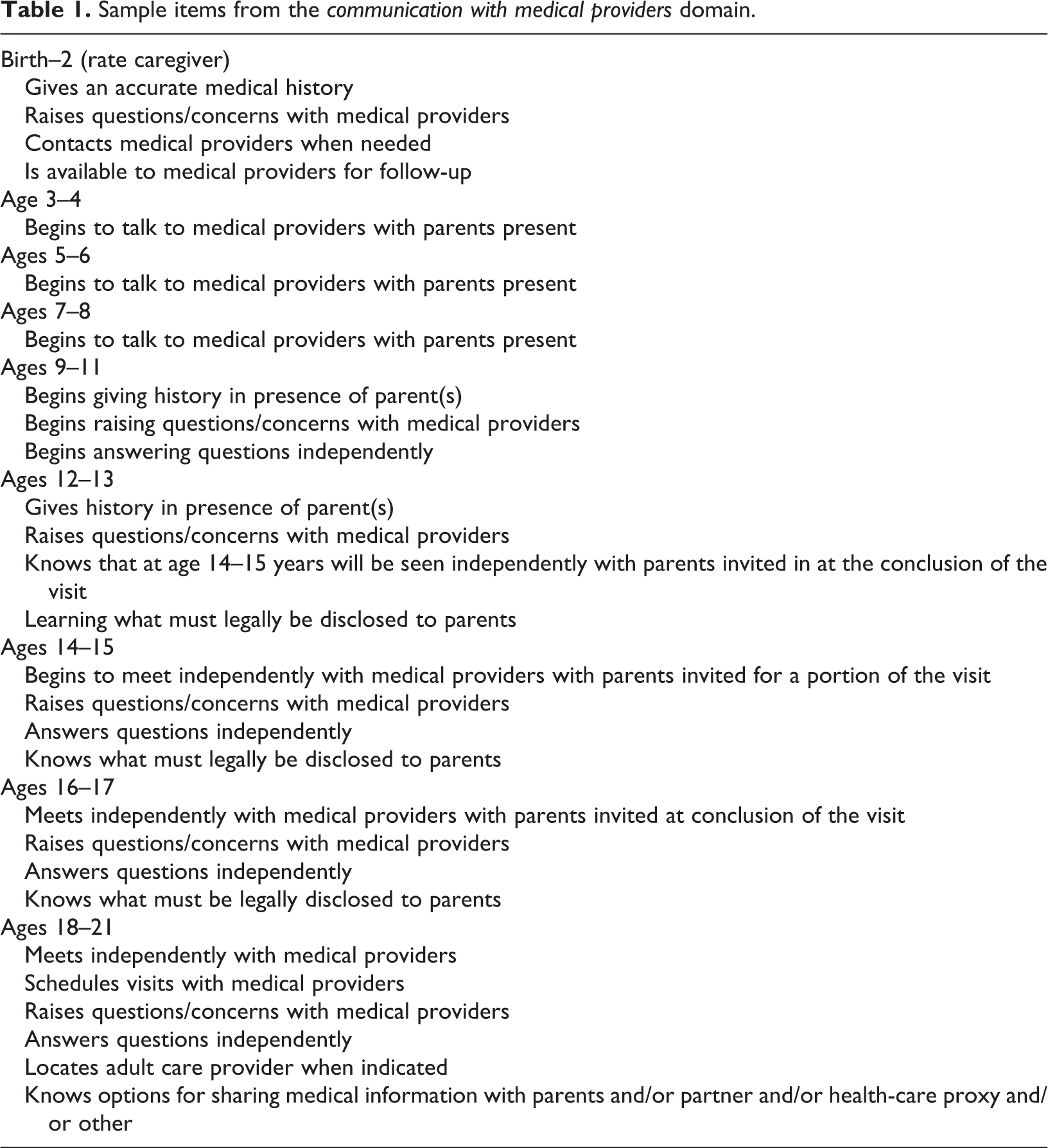
The tool also includes an assessment of psychosocial factors that may present barriers to medical independence. Tool content is based on widely accepted normative developmental milestones for specific age groups (Dosman et al., 2012; Hagan et al., 2017); it is designed for use with typically developing children diagnosed with chronic illnesses but is not appropriate for children with developmental or intellectual disabilities. The tool contains common elements required for medical independence across chronic medical illness populations. These elements are described in Table 1.
Sample items from the communication with medical providers domain.
Tool content and structure
Given that children and adolescents typically acquire new and different skills within a two- to three-year period (Decker, 2016, Hagan et al., 2017), each age-specific instrument spans a period of 24–36 months. The tool was devised for use with patients starting at birth or point of diagnosis to maximize patients’ ability over time to acquire increasingly more complex knowledge of their condition and self-management skills. The tool was designed so that providers can determine by inquiry and observation, rather than by self- or parent-report, the patients’ competency in demonstrating skills necessary for medical independence at each developmental stage. Only the first of the nine aged-based instruments focuses exclusively on the mastery of skills for parents/caregivers, as infants/young children ages birth–24 months are not expected to demonstrate independent skills. The remaining eight instruments focus only on the patient’s mastery of skills. Each measure assesses developmentally appropriate skills in five domains: health assessment, communication with medical providers, use of medication/medical equipment, access to insurance/medical records, and management of lifestyle choices.
Domains are comprised of three to six items, each of which is rated on a five-point rating scale: proficient, limited skills, no skills, not applicable, or indication that the provider ‘did not know’ based on observation and developmentally appropriate inquiry. Items are intentionally nondisease specific, thereby enabling clinicians to adapt items for more disease-specific inquiries as appropriate. Table 1 contains example items of skill mastery content for all developmental stages in the communication with medical providers domain. Tables 2 and 3 provide examples of 12- to 13-year-old patient responses in the health assessment domain. Two examples are given under the item ‘Learning names/purposes of medical tests/procedures’: one for gastroenterology and one for hematology. An additional example is given under the item ‘Learning symptoms and risk factors associated with medical condition’ using an endocrine condition. During the in-person trainings, comparable disease specific examples were given to help providers formulate questions they would use to assess patients in their clinical areas.
Example ratings from the training on tool use.a

a The below ratings are from 12- to 13-year-old developmental stage in response to the following topic in the health assessment domain: Learning names/purposes of medical tests/procedures.
Example ratings from the training on tool use.a
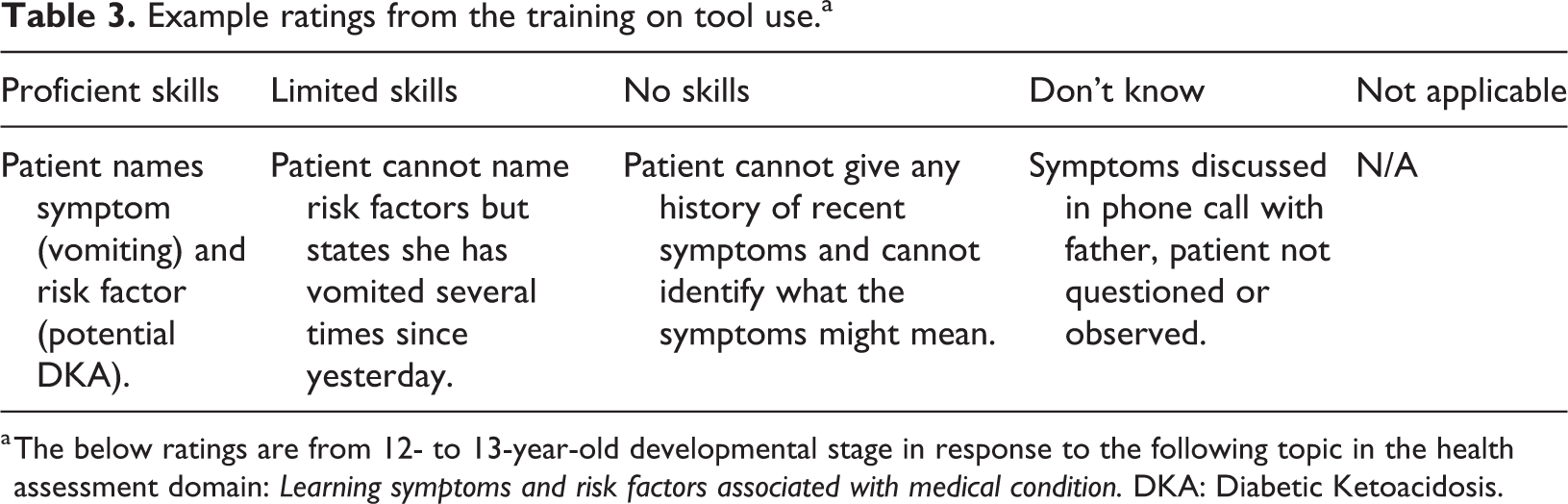
a The below ratings are from 12- to 13-year-old developmental stage in response to the following topic in the health assessment domain: Learning symptoms and risk factors associated with medical condition. DKA: Diabetic Ketoacidosis.
Another feature of the tool is the inclusion of psychosocial factors or circumstances that can potentially affect transition skill mastery. Six psychosocial categories are identified: learning issues, psychological functioning, family relationships, safety concerns, financial stressors, and social context (i.e. language, religious, and cultural factors). Each category encompasses the patient and family psychosocial circumstance and is rated on a four-point Likert-type scale: zero to three, ranging from no challenges to severe challenges.
Procedures
After initial protocol review, the host hospital’s Institutional Review Board (IRB) determined that the study did not require IRB approval due to the nature of the study and participant sample. Outreach was then made to leadership of several medical divisions to determine interest and obtain approval. To avoid internal bias, leadership in divisions with which the tool developers were affiliated were not approached. Three clinics agreed to participate and providers in each were subsequently solicited on a volunteer basis via snowball sampling. None of the three participating specialty divisions had created a formal transition policy or transition program; however, each division had staff who were working to create standards for such practice. Participants attended a one-hour training session facilitated by the study team that included specific instruction on tool administration and case vignettes. Trainings were tailored to the specific chronic illness population served by each specialty clinic but were not evaluated in this study. Participating providers also received an instruction manual that included examples of common verbal and behavioral responses corresponding to the various rating categories for each item across the five domains (see Tables 2 and 3).
During 10-month pilot period, participants were asked to administer the tool during routine follow-up (not urgent) clinic visits with patients who met criteria as established for the pilot study: prior diagnosis of at least one chronic illness, absence of intellectual or developmental disability, English speaking, and not currently in custody of a state agency. After each appointment in which the tool was administered, providers completed a survey to rate items pertaining to the use of the tool during that visit. Questions solicited provider perspectives on the tool’s usefulness, ease of integration, clinic time used, and impact on care delivery. At the end of the 10-month pilot period, a masters-level independent consultant conducted semistructured telephone interviews with each provider about his/her experiences using the tool. Research consultation was available through an institution-based grant, with a survey methodologist providing technical support in question development and subsequent analyses. A description of the questions is located in the Results section and in Table 4.
Provider responses to the survey examining experiences of using the tool by discipline (n = 28).

Analyses
For quantitative data, means, standard deviations, and proportions were computed. All qualitative interviews were analyzed using thematic analysis (Braun and Clarke, 2006). Specifically, each interview was coded line-by-line to facilitate the identification and the exploration of themes emerging from the data (Charmaz, 2006). After all interview data had been coded initially, the research team categorized the data according to two areas of inquiry: practice experiences and implementation challenges. Conceptually, clustered matrices were used to facilitate comparisons within and across participants (Miles and Huberman, 1994). Qualitative analyses were conducted by two of the tool developers in conjunction with an independent qualitative data analyst. The independent qualitative data analyst was not involved in tool development, data collection, or pilot testing.
Results
Twenty-eight pediatric health-care providers completed a total of 108 tools. Providers included 15 physicians (53.6%), six nurses (21.4%; registered nurses and nurse practitioners), and seven Masters of Social Work (MSW)-level social workers (25.0%). On average, each provider completed 3.9 (SD = 2.1) tools, with a range of 1–10. Of the 28 providers, 27 completed semistructured telephone interviews with an independent consultant. The distribution of providers who participated was relatively equal across the three chronic illness divisions (endocrinology, n = 11; gastroenterology, n = 8; and hematology, n = 9).
The self-report survey included questions about the length of time required to complete the tool, whether or not the length of the visit was extended when the tool was administered and whether findings from the tool were incorporated into the plan of care. Questions about ease of using the tool and usefulness of incorporating a tool into clinical practice were assessed using Likert-type scales ranging from 1 (not at all/very difficult) to 10 (very much/very easy). During the semistructured qualitative telephone interviews, the consultant asked each participant about their experiences using the tool and any challenges or barriers to implementation. Eighty-nine percentage of respondents noted that using the tool increased both their awareness and knowledge about developmental milestones associated with medical independence (M = 7.6; SD = 2.1). The ease of use of the tool had an overall mean rating of 7.3 (SD = 2.1) on a scale of 1–10; 87.5% (n = 21) of respondents reported that administration of the tool became easier with repeated use. Ninety-two percent (n = 23) of participating providers reported that it was feasible to incorporate the tool into general clinical practice. Overall, providers reported that the information gleaned from the tool was incorporated into the plan of care 65.7% of the time. Almost all (96.0%; n = 26) respondents reported that a structured developmental assessment tool should be incorporated into standard clinical practice. A little over one-third (34.3%; n = 10) of providers reported that administering the tool increased the length of the patient’s routine clinic visit; on average, the time it took to administer the tool completion was 8.1(SD = 4.5) minutes. In terms of incorporating information from the assessment into the patient’s plan of care, almost half of physicians did so (47.1%; n = 7), followed by nurses (72.0%; n = 4) and social workers (SW) (85.7%; n = 6; Table 4).
A total of six themes emerged from the semistructured telephone interviews. Themes spanned two areas of inquiry: practice behavior changes and implementation barriers. Themes related to practice behavior changes were (1) thinking developmentally, (2) focusing on the patient, and (3) structuring the approach. Themes related to barriers using the tool consisted of (1) clinic visit time constraints, (2) tool length, and (3) discipline-specific challenges related to the psychosocial assessment component.
The first practice behavior change theme was ‘thinking developmentally’. Providers indicated that the tool helped them enhance their understanding of what to expect at various ages and stages of development, thus providing a framework for working on medical skill mastery with each patient. Providers noted that the tool augmented their capacity to facilitate skills needed for medical independence at developmentally appropriate levels. In addition, providers commented that their skill-building education with patients was enhanced using the tool to formulate patients’ plans of care that identified gaps in learning and resources needed to support skill mastery. Some noted that while this was not new information, it reinforced and validated the need to think about skill mastery from a developmental perspective. Specific mention was made about increased awareness regarding setting expectations for younger patients and how these patients might participate in their own care. Providers commented that it was helpful to have specific skills and behaviors identified to address in teaching. One social worker said that using the tool: got me thinking about what the expectations are for each age group—do they know the name of their illness, do they know how their body works? It made me much more aware of the younger children in particular and how much they know. That was eye opening. (Social Worker, Endocrinology)
The second practice behavior change theme was ‘focusing on the patient’. In an effort to be family centered, pediatric providers often include the entire family during routine visits. Frequently, providers interact with parents/caregivers who answer on behalf of the child, thus directing education to the parents/caregivers rather than to the patient. Providers noticed that as they used the tool, they began to shift attention from parents/caregivers to the patient, most notably with younger patients. One physician noted that using a structured developmental readiness assessment tool ‘moved me to focus more on what the child was thinking, rather than just the parents’ (MD, Endocrinology). Similarly, a nurse noted that ‘with younger kids, we take for granted that their caretakers answer for them. With this tool [which requires direct interaction with the patient and skill demonstration], we get a handle on how much the kids understand’ (Registered Nurse [RN], Gastroenterology). Many providers noted that focusing on the patient increased their understanding of what the patient knows and can demonstrate. A social worker noted that ‘it is really empowering for the kids to see “I can do this.” Kids were very excited to see what they could do. Particularly with the younger children, it was interesting to see how they incorporated their illness into their life’ (SW, Endocrinology).
Providers noted that focusing on the patients encouraged more active participation by the patients in their own health care and educated parents/caregivers about skill mastery expectations. Across disciplines, providers agreed that focusing on the patient increased their understanding of what the patient knows and can demonstrate, fostering increased patient comfort and competence. This broader perspective allowed for the development of a care plan created jointly with patients, caregivers, and providers that focuses on the patient’s specific skills and needs.
The third practice behavior change theme of the pilot study, ‘structuring the approach’, focused on changes providers noted in their own practice after using the tool. Many providers noted that their experiences of using the tool led them, over time, to systematically structure their approaches during routine clinic visits. One social worker said she ‘started being aware and raising the issue with younger patients to encourage more active participation in their healthcare. Raising the questions in front of the family was also good’ (SW, Gastroenterology). Many providers noticed a marked shift in the way they prepared for and conducted clinic visits. For example, a nurse practitioner noted that the experience ‘made me think about what was needed before a patient would be ready for transition to adult care. I use [the tool] as part of my assessment to see where each developmental group should be’ (NP, Gastroenterology). A social worker said that ‘because of the tool, I was primed to think about next steps to be achieved—not just focus on what has been achieved already’ (SW, Gastroenterology). Providers emphasized how the tool helped them understand the importance of educating patients and their parents/caregivers about age-appropriate transition readiness skill mastery. One nurse noted that ‘it does make you think about teaching so that a patient is competent about their disease’ (Nurse Practitioner [NP], Hematology), and a social worker said that ‘it gave me the sense that we [providers] need to build in more time for education at each visit’ (SW, Hematology).
Providers commented that a structured framework for formulating questions was particularly useful. A physician said that ‘exposure to the tool helped operationalize my approach. It solidified what I already did, but in a more systematic way’ (MD, Endocrinology). Many noted that, in addition to the structure, the specific prompts and domain areas minimized the possibility of omitting key information. A nurse said ‘The tool gave me some really good ideas about what I should ask. This made [the visit] more concrete and standardized. It ensures that I don’t forget any area’ (RN, Hematology). Similarly, a physician noted that ‘it gave me a framework of what specifically to ask. It puts the issues down concretely and highlights the milestones that I might not otherwise have known’ (MD, Endocrinology).
Providers reported that the structure and prompts were helpful and that they liked having a ‘script’ of what to ask. Overall, providers recognized the need to conduct age-specific education with patients and to adjust the care plan accordingly. They expressed feeling reassured about not missing key issues and clarity in formulating the care plan. Many attributed the changes in approach to the tool itself, indicating that having a roadmap ensured that they were more effective in addressing patient self-care management issues.
Finally, while results indicated overwhelmingly that a structured developmental transition readiness assessment tool was useful in practice, there were a number of barriers that made it challenging to implement. Comments from providers about the barriers to implementation focused on the length of time it took to complete the tool, the length of the tool itself, discipline-specific challenges related to completing the psychosocial component, and the challenge of conducting additional inquiry during clinic visits given competing institutional demands. A physician noted, ‘We have so many things to do in a visit’ (MD, Gastroenterology). Some providers commented that the length of the instrument itself could function as a barrier. One physician reflected that the idea of administering a structured developmental readiness assessment focused on medical independence ‘is very useful conceptually, but realistically difficult to do. Time/length is an issue’ (MD, Hematology). Similarly, another noted, ‘I found it really cumbersome. It’s too long. It would have to be significantly shorter—less than a page’ (MD, Gastroenterology). Finally, comfort with integrating psychosocial components was noted to be a barrier. A physician commented that the psychosocial components are ‘familiar to social work or psychiatry, but very foreign to MDs’ (MD, Gastroenterology).
Ideally, incorporating a structured tool into standard clinical practice should enhance the quality of the visit and the patient experience without increasing the length of the visit significantly. Although on average, the pilot tool extended clinic visits by 8.1 minutes, it was noted by many that they became more proficient in using the tool with repetition, suggesting that a shorter, more concise version of the tool could be done more efficiently and in less time. Of note, some providers, mainly physicians, noted that they did not feel ‘equipped’ to adequately assess psychosocial factors as identified on the tool. Future revisions of the tool might incorporate binary screening or early detection questions—as opposed to severity rating scales—that raise awareness of the presence of psychosocial issues and trigger referrals to additional disciplines, such as social work.
Discussion
Results of the pilot of a transition readiness assessment tool for providers illustrated that it is both feasible and useful to incorporate a structured transition readiness tool into standard practice in the ambulatory setting. Past research related to providers’ perspectives highlights their experience of feeling ill-prepared to conduct transition counseling given lack of standardized tools to measure developmental progress (Fernandes et al., 2011). Providers in this pilot noted that they appreciated having a developmental frame or “roadmap” that defined expectations for skill mastery at each age of development starting at diagnosis and throughout childhood into emerging adulthood. Importantly, and differing from most tools which are self-report or parent report (Schwartz et al., 2014), qualitative provider feedback indicated the benefit to providers of being able to identify skills to be demonstrated by the patient so that the provider could recognize challenges to mastery that require remediation for the patient and address barriers or education needs in the plan of care, which they reported doing 65.7% of the time.
Although there is significant literature addressing the need to ‘start early’, including policy statements related to transition readiness (AAP et al., 2011; AAP, 2017), the timing to begin this process is generally noted to be early adolescence. The piloted tool is unique as it begins at age of diagnosis and incorporates observational measures to assess cross-illness milestones associated with medical independence so that common elements of skill mastery can be generalizable to any condition and consistent expectations can be set across specialties and across disciplines. Studies indicate that patients want to be involved in treatment related discussions (Carpenter et al., 2014) and that interventions may be required to help patients and providers engage more successfully (Bray et al., 2017). Research also indicates that patients want education on the various transition- and transfer-related changes in care as well as support in self-management (Coyne et al., 2017). The piloted structured tool facilitates discussion between providers and patients and helps providers to assist patients from an early age in maximizing autonomy and building skills, with most providers (89%) noting that using a tool increased both their awareness and knowledge about developmental milestones associated with medical independence. Results also revealed that the tool assisted providers in shifting the focus to address the patient at younger ages, rather than counting only on parent report. Although parent perspectives were not measured in this study, it is possible that parents and caregivers may also benefit from this tool as they observe providers model patient-focused behavior that encourages self-management.
Identifying psychosocial circumstances that could be potential barriers to skill acquisition was an additional unique feature of the tool, providing the context as providers developed a plan of care. The literature specifically states that psychosocial factors often act as barriers to successful transition and transfer (Lotstein et al., 2010; Viner, 2008). Research findings speak to the impact of psychosocial factors in accessing health care and on adult health outcomes (Conroy et al., 2010) and to psychological factors such as increased feelings of self-efficacy regarding care management that may likewise impact transition (Sawicki et al., 2014). The tool developers, all social workers, based the tool in the ecological approach, which stresses the person in their environment (Hare, 2004), with the assumption that patients are learning skills of medical independence in the context of variable levels of challenging psychosocial circumstances. Social workers and nurses were more likely than physicians to report incorporating information gleaned from the tool into patient care plans, perhaps suggesting possible differences in the ways disciplines assess, formulate, and document patients’ plans of care. While results in this pilot did not explicitly measure the potential impact of psychosocial factors upon skill attainment, qualitative data indicating the need for additional education for patients may be attributed to the understanding gleaned using the tool, which did provide the psychosocial context. It is possible that the plans of care developed the majority of the time (65.7%) did take these factors into account; this was not explicitly asked in the pilot study and could be the subject of future research.
Limitations
Several limitations to this pilot study should be noted. Participants included a convenience sample of volunteer providers with variability in familiarity with transition-related concepts. Sample size limitations prohibited the use of statistical analyses. Provider knowledge about developmental milestones, developmentally appropriate skill mastery, and practice behaviors during routine clinic visits with YSCHN were not assessed prior to attending the in-person trainings; moreover, the in-person trainings were not assessed. Future studies might include measures of provider awareness and knowledge of developmentally specific skills necessary for medical independence prior to and following implementation of a tool into their practice and employ larger sample sizes. Tool use was not mandatory with every patient; thus, providers may have chosen to use the tool with less complex patients. Data were collected via self-report only. Inter-rater reliability was not assessed in the interest of minimizing patient and provider burden; validity and reliability can be addressed in a future study. It is also possible that qualitative data may have been susceptible to some degree of biased interpretation, as two of the tool developers were involved in data analysis and interpretation. Although the research team did include a third independent coder who was not involved in earlier phases of the research study, inclusion of developers in the analytic phase may have influenced interpretation of results to some degree. Finally, the assessment of the presence and the quality of other transitional care arrangements were beyond the scope of the current study; future research should assess whether and how provider use of a transition readiness assessment tool can inform collateral service use by patients and their families.
Conclusion
Findings from this pilot study indicate that a developmentally sensitive transition readiness assessment tool could be incorporated into standard practice. Feedback from providers underscored the value of having a structured tool that defines developmentally based expectations for what patients should know and be able to demonstrate at each age and helps formulate what questions providers should be asking to guide patient education. Results suggest the importance of focusing on the patient versus directing questions, concerns, and teaching exclusively to parents or caregivers and starting medical independence preparedness early. Additional research is needed to evaluate whether utilization of a developmental transition readiness assessment tool affects the patient’s acquisition of self-efficacy skills and the process of transferring from pediatric to adult care. Next steps include validation of the content of the measure itself to ensure that the developmental expectations for medical independence skills set for each stage are aligned with current understanding of child, adolescent, and emerging adult capabilities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received funding from the Program for Patient Safety and Quality (PPSQ) at Boston Children's Hospital for this study.