
Abstract
Objective
To explore the preoperative predictive efficacy of multimodal ultrasound based on microflow imaging(MFI) in Glypican-3(GPC-3) in hepatocellular carcinoma(HCC).
Methods
The general data and ultrasonographic data of patients with HCC confirmed by histopathology and hepatectomy from January 2019 to June 2023 were analyzed retrospectively. According to the gold standard of postoperative pathology, the patients were divided into GPC-3 positive group and GPC-3 negative group. Through analyze the correlation between multimodal ultrasound features and GPC-3, to determine the independent predictors of GPC-3, and to further analyze the preoperative predictive efficiency of Two-dimensional ultrasound(2D-US), contrast-enhanced ultrasound(CEUS) and microflow imaging(MFI) for GPC-3 of HCC.
Results
A total of 102 patients were enrolled in this study, including 60 GPC-3 positive patients(58.8%) and 42 GPC-3 negative patients(41.2%). Through univariate and multivariate analysis, it was found that there were significant differences in diameter(95%CI: 1.080–7.741, P = 0.034), start washout time(95%CI: 0.105–0.694, P = 0.007) and CEUS-MFI(95%CI: 1.180–4.553, P = 0.015) between the two groups, which were independent predictors of GPC-3 positive occurrence. The prediction efficiency of multimodal ultrasound combined with GPC-3 for HCC is better than that of single mode(P<0.05).
Conclusion
The feasibility of multimodal ultrasound in predicting GPC-3 of HCC before operation is confirmed.
Keywords
Primary liver cancer is the common malignant tumor, of which hepatocellular carcinoma(HCC) accounts for the vast majority. 1 Even though the morbidity and mortality of liver cancer are declining, it is still a serious threat to people's life and health. 2 At present, the mode of diagnosis and treatment of HCC shows the characteristics of multi-disciplinary participation and multi-methods.3–6 However, even after active treatment, including radical surgery and non-surgical treatment, the recurrence rate and long-term survival rate of patients with HCC are still low. 7 With the understanding and in-depth study of the mechanism of tumor occurrence and development, the concept of tumor treatment is constantly updated and developed to micro and precision medicine. Therefore, precision medicine such as biomarker-driven and site-specific therapy has been paid more and more attention and accepted. 8
Glypican-3(GPC-3) is a member of heparan sulfate proteoglycan family and is anchored to the cell surface by glycosylphosphatidylinositol on the cell membrane. It is an effective biomarker for the diagnosis of HCC. GPC-3 is not expressed in normal liver tissues, but it is overexpressed in more than 70% of HCC tissues. The overexpression of GPC-3 also indicates a poor prognosis in patients with HCC.9,10 In recent years, GPC-3 has been considered as one of the targets of tumor specific immunotherapy. Therefore, GPC-3 is an important marker for the diagnosis, treatment and prognosis of HCC. 11
Recently, some scholars are studying the relationship between GPC-3 and enhanced MRI or 18F-FDGPET/CT.12–14 Although they have obtained good prediction ability by using preoperative radiological imaging to make prediction models, the use of these techniques is limited by problems such as cost and radiation exposure. 15 As far as we know, only a few scholars have studied the correlation between ultrasound features and GPC-3 of HCC, 16 especially in contrast-enhanced ultrasound(CEUS) and MFI features. CEUS has the advantages of low cost, no radiation exposure and no limitation of liver and kidney function, so it has been widely used in clinic as one of the clinical diagnostic tools for localized liver nodules. 17 As a new ultrasonic imaging technique, microflow imaging(MFI) is more effective than color Doppler flow imaging in microvascular visualization. 18 And this technique is widely used in the diagnosis of breast, joint, vascular and kidney diseases19–22; As far as we know, there are no scholars to explore the relationship between MFI and GPC-3 in HCC. It has been confirmed that CEUS and MFI have a certain predictive value in evaluating the poor prognosis and invasiveness of HCC.23,24
The purpose of this study was to retrospectively analyze the correlation between Two-dimensional ultrasound(2D-US), CEUS, MFI and GPC-3 of HCC, and to evaluate the predictive value of multimodal ultrasound in judging the positive expression of GPC-3 in HCC, so as to provide reference for patients to make individualized treatment plan.
Methods
Study patients
The general data and ultrasonographic data of patients with HCC a confirmed by histopathology in from January 2019 to June 2023 were analyzed retrospectively. Inclusion criteria: (1) The patients does not receive any treatment before hepatectomy. (2) 2D-US, CEUS and MFI are performed within 1–2 weeks before operation, and the imaging data were complete. (3) After hepatectomy, the histopathology confirme that it is HCC, and the pathological data are complete. (4) There is no allergic reaction to ultrasound contrast agent.
Our retrospective study has been approved by the institutional ethics committee, and all patients have signed informed consent before CEUS[2022128]. A total of 102 patients are enrolled in this study, and their clinical data(including sex, age, liver disease history), pathological data(GPC-3 positive or negative) and ultrasound data(2D-US, CEUS, MFI) are collected.
Process of ultrasonic examination
The ultrasound instruments are EPIQ 7 (Philips Medical Systems, Amsterdam, Netherlands) with 1.0- to 5.0-MHz phased convex probe for all the patients. The mechanical index(MI) is set to 0.06 for CEUS examination, and all patients are performed with MFI software. The contrast medium is SonoVue(Bracco, Milan, Italy) sulfur hexafluoride microbubble contrast agent.
The patient takes supine position or left lateral supine position. The nodules in the hepatic parenchyma are observed by 2D-US, and then the maximum diameter section of the nodules is selected to open the two-dimensional microflow imaging(2D-MFI). The 2D-MFI is used to observe the internal blood flow of the tumor. Then CEUS mode is opened in the maximum diameter section of the lesion, and MFI mode was started in the state of CEUS(contrast-enhanced ultrasound-microflow imaging, CEUS-MFI). The ultrasound contrast agent SonoVue is added to 5.0 ml normal saline to make microbubble suspension, then 1.2 ml is extracted and injected into the median elbow vein, and then saline 5 ml is injected into the catheter. At the same time, the dynamic perfusion and washout of the focus are observed continuously, and the imaging trajectory of ultrasound contrast agent microbubbles in the microvessels in the lesion is observed in real time.
Ultrasonic image judgment and analysis
All ultrasound images are independently analyzed and diagnosed by two ultrasound doctors with more than 5 years of diagnostic experience. When there is a disagreement, the third doctor analyzes the case and makes a final diagnostic decision through discussion.
The observation contents of 2D-US are as follows: the number of nodules (1, 2, ≥3), the diameter of nodules (<3 cm, ≥3 cm), the edge of nodules(clear, unclear), the form of nodules(regular, irregular), the echo of nodules (hypoechoic, isoechoic, hyperechoic). The blood flow in 2D-MFI images is analyzed according to Alder-score quantitative evaluation method. 25
The observation contents in CEUS are as follows: (a) Enhancement range extension(yes/no), defined as an increase in the maximum diameter of the nodule in the enhancement range compared with that measured by 2D-US. (b) Enhancement mode in arterial phase(uniform/non-uniform). (c) Nodule shape in arterial phase(regular/irregular). (d) Time of start washing out(<45 s, ≥45 s). (e) Degree of wash out(no-mild/significant), significant regression is defined as complete removal of Tumor with hypoechoic within 2 min after injection of contrast medium; mild regression is defined as the degree of enhancement of the lesion is lower than that of the hepatic parenchyma but not completely removed (there is still some enhancement in the lesion). (f) CEUS-MFI (Type I, Type II, Type III), Type I is defined as only punctate blood flow signal in the nodule, Type II is defined as small branched blood flow signal in the nodule, Type III is defined as cluttered, thick and irregular blood flow signal in the nodule.
Statistical analysis
All the statistical data in this study are analyzed by SPSS26.0. Univariate analysis is used to investigate the relationship between all data (classified variables, continuous variables) and GPC-3, and then the indicators with significant statistical significance are included in the binary Logistic regression analysis to determine the independent predictors of GPC-3. The ability of multimodal ultrasound to predict the GPC-3 of HCC is predicted by making the receiver working characteristic(ROC) curve and calculating the area under the curve(AUC). P<0.05 indicates that the difference is statistically significant.
Results
General data of patients
A total of 102 patients were divided into two groups according to the pathological results after hepatectomy, including GPC-3 positive patients (60/102, 58.8%) and GPC-3 negative patients (42/102, 41.2%). Among all patients, 68.6% (70/102) were males and 31.4% (32/102) were females. The mean age of all patients (53, 66). Patients with a history of liver disease (80/102, 78.4%) and patients without a history of liver disease (22/102, 21.6%). There was no significant difference in age, sex and liver history between the two groups (P>0.05). As shown in Table 1.
Univariate analysis and Logistic regression analysis of 2D-US and 2D-MFI in patients.
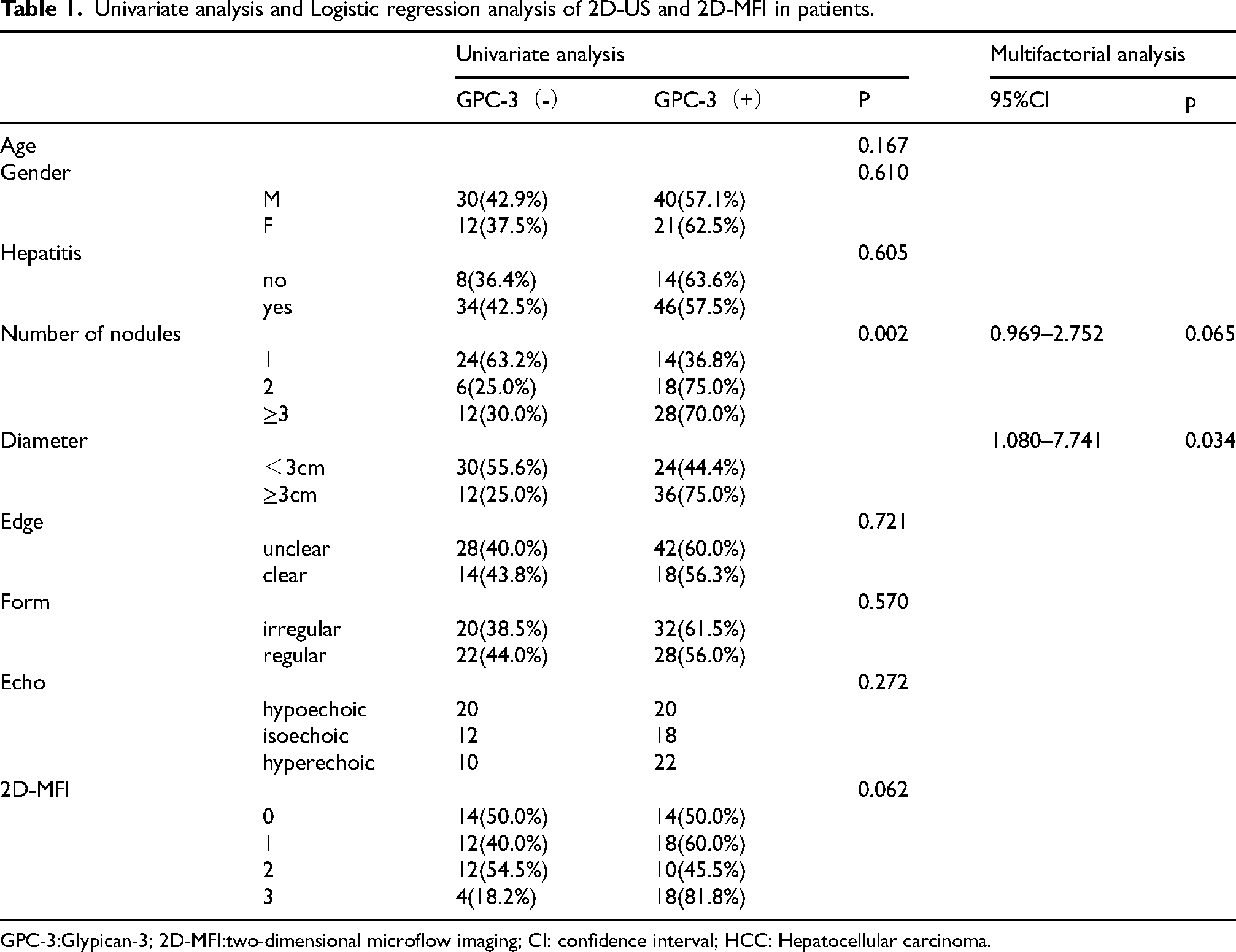
GPC-3:Glypican-3; 2D-MFI:two-dimensional microflow imaging; CI: confidence interval; HCC: Hepatocellular carcinoma.
Results of univariate analysis and Logistic regression analysis of 2D-US and 2D-MFI in patients
Univariate analysis showed that the edge, shape and echo of nodules had significant statistical significance between the two groups, and the number and diameter of nodules had significant statistical significance between the two groups(P < 0.05). Multivariate Logistic regression analysis showed that only the diameter had significant statistical significance(P = 0.034). In GPC-3 positive patients, 60.0% of nodules(36/60) with diameter ≥3 cm were significantly higher than 40.0%of nodules(24/60) with diameter <3 cm. As shown in Table 1.
Results of univariate analysis and Logistic regression analysis of CEUS and CEUS-MFI in patients
We studied the difference of CEUS and CEUS-MFI between GPC-3 positive group and GPC-3 negative group. The results of univariate analysis showed that there were significant differences between the two groups in whether enhancement range extension (P = 0.008), enhancement mode in arterial phase(P = 0.036), time of start washing out(P = 0.002) and CEUS-MFI(P = 0.007). After multivariate analysis, there were significant differences in After multivariate analysis, there were significant differences in the time of start washing out(95%CI:0.105–0.694, P = 0.007) and CEUS-MFI(95%CI:1.180–4.553, P = 0.015) between GPC-3 positive and negative groups, which indicated that the time of start washing out and CEUS-MFI was an independent predictor of GPC-3 in HCC. As shown in Table 2 and Figure 1.
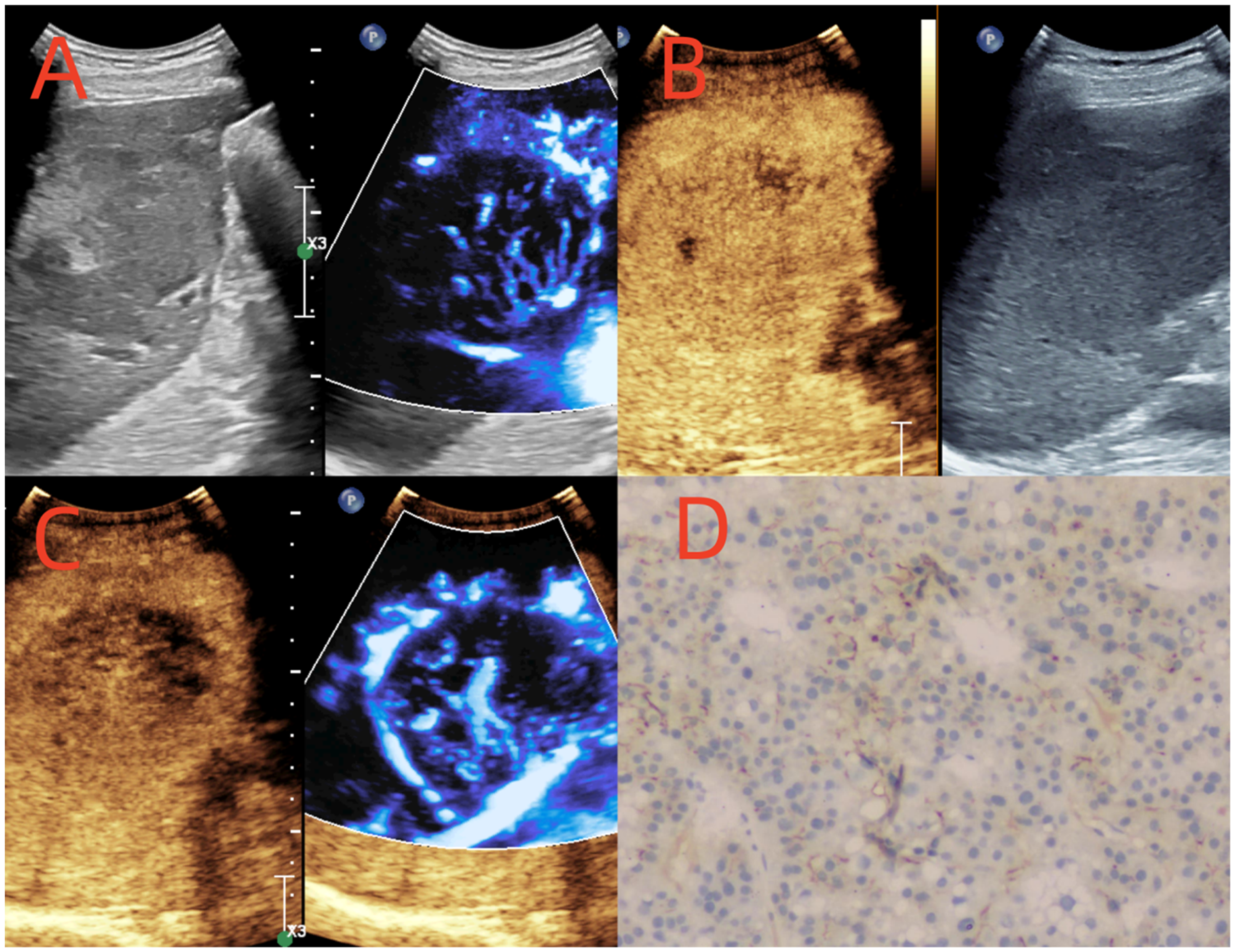
A 69-year-old man with hepatocellular carcinoma. A: 2D-US showed the isoechoic nodule with unclear edges in the right lobe of liver, and its diameter were 75 mm. B: CEUS showed that the nodule showed inhomogeneous hyperenhancement in the arterial phase, and it began to clear in 43 s. C: CEUS-MFI showed disordered, thick and irregular blood flow signals in the nodule. D: The pathological result showed that the GPC-3 of the lesion was positive (×100).
Univariate analysis and Logistic regression analysis of CEUS and CEUS-MFI in patients.
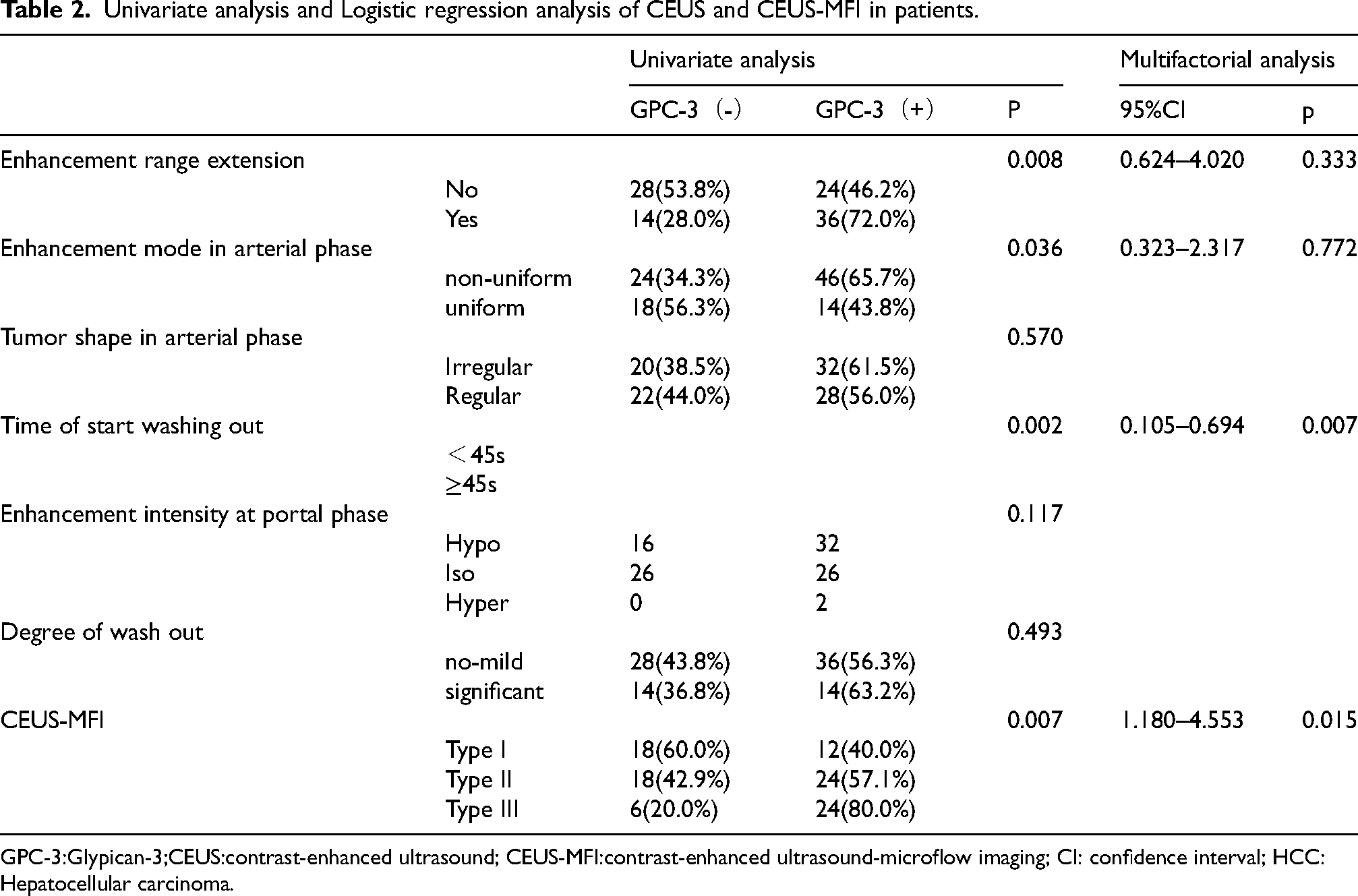
GPC-3:Glypican-3;CEUS:contrast-enhanced ultrasound; CEUS-MFI:contrast-enhanced ultrasound-microflow imaging; CI: confidence interval; HCC: Hepatocellular carcinoma.
The predictive efficacy of the combination of monomodal and multimodal ultrasound in predicting GPC-3 of HCC
The results of ROC curve showed that the AUC value, sensitivity and specificity of 2D-US for GPC-3 of HCC were 0.657, 0.600, 0.714. The sensitivity, specificity and accuracy of CEUS in for GPC-3 of HCC were 0.733, 0.700, 0.571. The AUC value, sensitivity, specificity and accuracy of multimodal ultrasound (2D-US, CEUS, CEUS-MFI) for GPC-3 of HCC were 0.761, 0.767, 0.571. As shown in Table 3 and Figure 2.
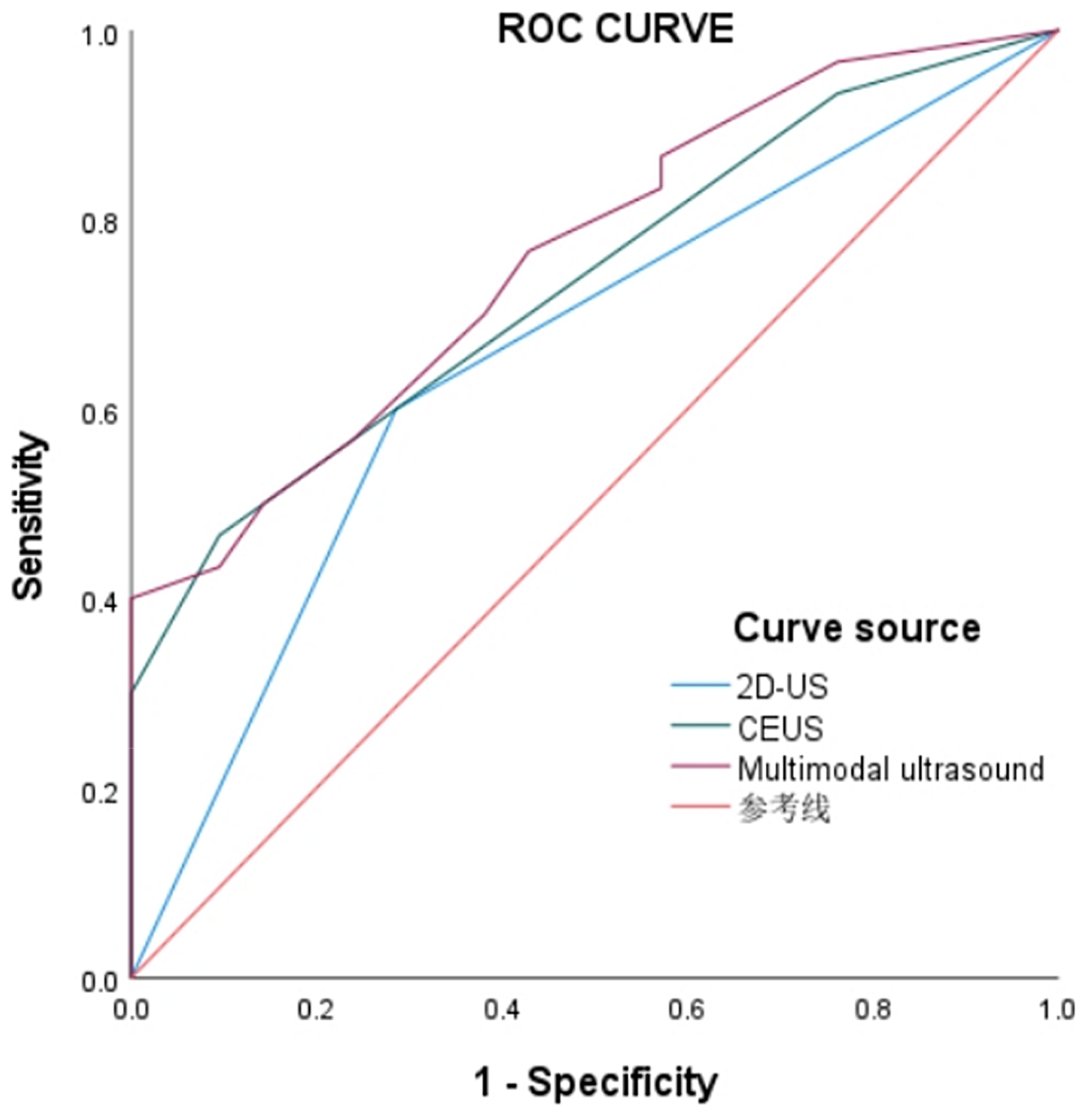
Prediction of GPC-3-positive ROC curve by single-mode and multimode ultrasound.
Predictive efficacy of the combination of monomodal and multimodal ultrasound in predicting GPC-3 of HCC.

2D-US: two-dimensional ultrasound, CEUS: contrast-enhanced ultrasound, Multimodal ultrasound: two-dimensional ultrasound, contrast-enhanced ultrasound, contrast-enhanced ultrasound-microflow imaging; HCC: Hepatocellular carcinoma; CI: confidence interval.
Discuss
In recent years, many scholars are doing extensive research on the role of GPC-3 in the diagnosis, invasion, metastasis and treatment of HCC. GPC-3 is a molecule connected to the surface of cell membrane and has strong immunostaining. GPC-3 is a regulated carcinoembryonic protein and one of the earliest transcripts in the process of malignant transformation of hepatocytes. it is not expressed in normal liver tissues, cirrhosis and benign nodules, but is overexpressed in HCC, which can distinguish AFP-negative HCC from cirrhotic benign nodules.26,27 Intrahepatic and extrahepatic metastasis is an important node in the progression of HCC. GPC-3 participates in the metastasis and invasion of HCC by activating Wnt signal pathway, interacting with growth factors, stimulating the aggregation of macrophages and promoting epithelial-simple transformation, thus promoting the progress of HCC, 28 and GPC-3 is considered to be the cause of death in patients with HCC. 29 With the deepening of research, GPC-3 has become a target for the treatment of HCC, such as GPC3 targeted antibody therapy, peptide/DNA vaccine therapy, immunotoxin use and gene therapy.30–32 Therefore, if the non-invasive detection method can accurately predict the expression of GPC-3 in HCC, it can greatly help clinicians to make personalized treatment plans. In our study, we explored the correlation between multimodal ultrasound features and GPC-3 of HCC, and explored the predictive efficiency of joint diagnosis.
In the 2D-US features, the number of nodules was closely related to the metastasis and recurrence of HCC.33,34 Some scholars believe that multiple nodules are independent predictors of recurrence after HCC, and multiple nodules in the liver may be caused by monoclonal mode. 35 We believe that multiple nodules in the liver may be caused by monocentric or multicentric metastasis in the liver; compared with single focus, the cancer cells in multiple nodules are more malignant, more invasive and easier to carry out intrahepatic metastasis by invading blood vessels and bile ducts. However, this study did not find that the number of nodules was an independent predictor of GPC-3, which was consistent with other imaging results.36,37 Further large sample, multicenter studies are needed. This study also found that diameter larger than 3 cm is an independent predictor of GPC-3 positivity. some studies have found that lesion diameter can independently predict recurrence after HCC liver transplantation, 38 which is consistent with the results of ChenY and other scholars in the field of enhanced magnetic resonance imaging. 39 In addition, some scholars believe that different imaging methods and observation angles of nuclear magnetic resonance and ultrasound will lead to inconsistent results, 40 so it is necessary to further verify the correlation between diameter and GPC-3.
CEUS can real-time and dynamically display the whole process of local liver nodules and hepatic parenchyma microcirculation perfusion changes, and is not affected by liver and kidney function. In local liver nodules, ultrasound doctors can diagnose and differentiate the nodules according to the CEUS mode, and indirectly reflect the invasive biological characteristics, such as vascular density, vascular invasion, tissue differentiation and so on. 41 The CEUS features of HCC are usually highly enhanced in the arterial phase, followed by gradual clearance of the portal vein and delayed phase.42,43 Among them, enhancement and clearance are important features in CEUS. Among them, the clearance time was significantly correlated with the degree of differentiation and vascular invasion of HCC. 44 Jia-YanHuang et al. confirmed that the clearance of nodules within<60 s may indicate poorly differentiated HCC or non-hepatocellular malignant tumors. 45 This study found that time of start washing out is an independent predictor of GPC-3 in HCC, which may be due to the fact that positive GPC-3 mediates the development of cancer cells in the nodules, resulting in low differentiation and high invasiveness of cancer cells in the foci. In biological behavior, tumor thrombus is formed by invasion of blood vessels, and then more neovascularization and abnormal blood supply are formed in the tumor, such as arteriovenous fistula formation. As a result, CEUS showed that the time of high enhancement in arterial phase was shortened and washing out began earlier. Arterial phase enhancement is one of the important features of HCC, which can indicate the prognosis of patients. The results of Ran Q et al. showed that there was a significant correlation between postoperative recurrence and arterial phase enhancement pattern (P < 0.05), in the early recurrence group, most of the nodules (40 beat 59) showed uneven enhancement in arterial phase. 46 In addition, some scholars have confirmed that the arterial phase enhancement pattern is closely related to GPC-3. 40 However, although our study found enhancement patterns and GPC-3 in the results of univariate analysis, there were no independent predictors. Therefore, a large sample, multicenter prospective study is also needed.
MFI is a new ultrasonic imaging technology, which can detect blood vessels with diameter 0.1 mm and velocity 1 cm/s. It is more effective than color Doppler flow imaging in microvascular visualization. 47 CEUS-MFI is an imaging technique formed by the superposition of microflow imaging and CEUS. This technique can not only display the angiographic characteristics of the nodules in real time, but also show the morphological characteristics such as the number, distribution and shape of microvessels in the nodules according to the formation and flow of microbubbles in blood vessels. Kuang Xiufeng and others confirmed this in the study of kidney disease. 48 In this study, there was a significant correlation between GPC-3 and CEUS-MFI, and multivariate analysis showed that it was an independent risk factor. Among them, GPC-3 positive nodules accounted for 80% of CEUS- MFI3 type. The results showed that CEUS-MFI showed more blood flow signals in the nodules, and the appearance of messy, twisted and thick blood vessels could indicate the occurrence of GPC-3 positive. This may be due to aggressive cancer cells invading blood vessels, resulting in hemodynamic changes, vascular distortion, irregular shape, when intravascular cancer thrombus formation, will cause some small vascular occlusion, resulting in the formation of large supply vessels. Therefore, this study suggests that the characteristics of CEUS-MFI in the nodules can reflect the biological behavior of the tumor.
In this study, after making the ROC curve, the combination of independent predictive factors in multimodal ultrasound(2D-US, CEUS, CEUS-MFI) is feasible to predict GPC-3 of HCC(AUC = 0.761, P < 0.001), which is higher than that of 2D-US(AUC = 0.733, P < 0.001) and MFI combined with CEUS(AUC = 0.657, P = 0.007), and is more accurate and more effective than single mode.
However, this study has some limitations: 1.This study did not exclude nodules with a diameter less than 10 mm, which may not accurately reflect the CEUS-MFI characteristics of nodules. In subsequent research, multicenter collaborative studies will be carried out to further expand the sample size, especially for CEUS characterization of lesions smaller than 15 mm for research and analysis.2.Ultrasound observation mainly depends on the technique of the operating doctor and the matching degree of the patient. 3.This study is a single-center, retrospective analysis, and there will be selective segregation.
Conclusion
To sum up, multimodal ultrasound features (diameter, start washout time, CEUS-MFI) are helpful for the prediction of GPC-3 positive in HCC, thus helping clinicians to identify high-risk patients with high invasiveness and easy recurrence, and provide a reference basis for patients to make accurate treatment plans.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.