
Abstract
Background:
Women comprise approximately two-thirds of Alzheimer's disease cases.
Objective:
This is the first known study to investigate the role of intersectionality between gender and other social determinants of health (SDOH) in the presentation of cognitive symptoms (i.e., being asymptomatic or symptomatic) among those with pathologically confirmed Alzheimer's disease.
Methods:
We studied 3107 individuals with Alzheimer's disease neuropathology (ADNP) confirmed at autopsy. Asymptomatic ADNP was defined as the absence of a clinical diagnosis of mild cognitive impairment (MCI) or dementia before death (versus symptomatic: diagnosis of MCI/dementia). SDOH included gender, education, ethnoracial group, living alone, and primary language. Multivariable logistic regression tested associations between SDOH and asymptomatic ADNP (versus symptomatic); models were also stratified by gender.
Results:
Women, Hispanics, those living alone, and more educated individuals were found to have higher odds of asymptomatic ADNP. Non-English speakers had lower odds of asymptomatic ADNP. Both women and men had higher odds of asymptomatic ADNP if Hispanic or living alone. In only women, non-English speakers had lower odds while in only men, more education was associated with higher odds of asymptomatic ADNP.
Conclusions:
Gender, education, ethnicity, primary language, and living alone, and intersectionality of gender with primary language, may differentially influence MCI and dementia diagnosis prior to death among those with underlying ADNP. These findings emphasize the need for future Alzheimer's disease research to prioritize social determinants of brain health including their intersectionality with gender and how to inform targeted interventions.
Keywords
Introduction
Alzheimer's disease (AD) is the most common type of dementia and the fifth leading cause of death among ≥65-year-olds in the US. 1 Typically, AD initially presents with memory loss that progresses to more significant cognitive impairment. Neuropathologically, AD is characterized by extracellular deposits of amyloid-β (Aβ) plaque and intracellular tau neurofibrillary tangles. 2
Sex differences, as a biological distinction, in AD prevalence are often attributed to hormonal and genetic factors, or women's longer lifespans that increase risk of developing AD in older ages.3,4 However, recently, research has been shifting to consider how gender as a social determinant of health (SDOH) may also contribute to disparities. SDOH are the “conditions in the environments where people are born, live, learn, work, play, worship, and age.” 5 Gender is socially patterned and affects a wide range of life course factors that ultimately impact AD risk, including socioeconomic status, access to and quality of education and healthcare, and health behaviors. 6
Although gender is now recognized as a determinant of AD disparities separate from sex assigned at birth, 7 most cohort studies and available data to date have not distinguished between sex and gender. 8 However, it has been estimated that ∼97% of individuals identify as cisgender (sex and gender match), 9 and thus prior studies of sex differences in AD prevalence and risk factors can be used to estimate differences between cisgender men and women (but not for non-cisgender, transgender, or nonbinary/third gender individuals). We will use the term gender hereafter to emphasize its importance as a social determinant of AD and not as a biological risk factor.
Women are disproportionately affected by AD—comprising approximately two-thirds of cases. 10 Comorbidities and other risk factors for AD also differ by gender, such as the higher risk of depression in women and for sleep apnea in men. 11 Although more prevalent among women, incidence rates of AD appear to be similar by gender. 12 Therefore, understanding the influence of gender on AD risk, onset, and progression is crucial for crafting effective prevention and treatment strategies.
Ethnoracial group, immigrant status, education, and living situation are additional SDOH that have been linked to AD disparities. AD risk is higher in Black/African American and Hispanic individuals (versus non-Hispanic White) and among US immigrants and individuals whose primary language is not English.13–16 These racial/ethnic disparities are not explained by underlying biological differences due to genetics in these minoritized populations, but instead to their experiences of lifelong discrimination, stress, and reduced access to health promoting resources and opportunities that increase their AD risk. 17 Individuals with fewer years of education also have higher risk of AD and earlier onset, which has been explained in terms of low educational attainment as a proxy for lower socioeconomic status that is in turn is associated with lower health literacy, greater stress associated with financial instability, and limited access to preventative health care.17–20 Additionally, AD risk factors such as diabetes, obesity, hypertension, smoking, and physical inactivity, are often more prevalent among racial/ethnic minoritized and socioeconomically disadvantaged populations. 15 Other studies have shown that individuals who are single (i.e., not in a relationship), living alone, or experiencing social isolation display faster cognitive decline, while conversely, greater social connections are associated with slower cognitive decline and reduced risk for dementia. 4
The concept of intersectionality refers to interlocking and multifaceted identities of an individual that are intertwined (e.g., “Black, middle-aged women” or “Hispanic immigrants without a college degree”), that are defined by social systems of stratification that advantage some and disadvantage others, and that are posited to relate to risk for disease including ADRD.21,22 A very limited number of preliminary studies have considered intersectional identities such as between gender and ethnoracial group with respect to ADRD outcomes,21,23 with no conclusive findings to date. However, known differences by gender and ethnoracial group in ADRD risk factors and prevalence detected via biomarkers and neuropathology, when considered separately,1,24–27 calls attention to the need to study intersectionality of these social determinants, which could further increase risk depending on group (e.g., Black women versus White men).
Although disparities in AD related to SDOH such as ethnoracial group and socioeconomic status are well-documented, research on how the combination of these factors with gender specifically impacts AD's presentation is lacking. Thus, in this study, we aimed to examine the associations between gender in combination with key SDOH (i.e., ethnoracial group, education, primary language, living alone) and asymptomatic neuropathologically-confirmed AD. We hypothesized that the intersectionality of these factors is associated with differential odds of presenting with no cognitive impairment in the presence of AD neuropathology (ADNP).
Methods
Study sample
Our analytic sample included individuals with neuropathology data in the National Alzheimer's Coordinating Center's (NACC) Uniform Data Set (UDS) as of June 2023. Research using the NACC data is approved by the University of Washington Institutional Review Board and informed consent was obtained from all participants at each National Institute on Aging-funded Alzheimer's Disease Research Center (ADRC). The NACC data used in this study were de-identified.
Since September 2005, UDS participants have been followed approximately annually (rolling enrollment over time) at over 30 ADRCs located across the US. At each visit, comprehensive data are collected on demographics, comorbidities, and medical history, and functional, clinical, and cognitive assessments are performed. Clinical Dementia Rating (CDR) global scores (range = 0–3) and sum of box scores (range = 0–18) are calculated at each visit indicating the participant's level of impairment (higher = more impaired). Clinician-based diagnoses of cognitive status (normal cognition, mild cognitive impairment (MCI), or dementia) are made at every visit. Participants consenting to autopsy have detailed neuropathology data collected using the Neuropathology (NP) Form. Additional details on the UDS and NP protocols are found elsewhere.28–31 We restricted to UDS participants with (i) moderate to frequent neuritic plaques (i.e., amyloid plaque burden) and Braak neurofibrillary tangle stages III-VI, and (ii) their last UDS visit within 24 months of autopsy. Our analyses include data from 38 ADRCs.
Asymptomatic Alzheimer's disease neuropathology outcome
All participants in our sample had ADNP present at autopsy (i.e., moderate/frequent neuritic plaques and Braak stage III-VI). Neuropathological evaluations are conducted in a standardized manner across the ADRCs and AD neuropathology is determined using established guidelines delineated by Montine et al. 32 Our dichotomous outcome of interest was asymptomatic (versus symptomatic) ADNP, where individuals with asymptomatic ADNP lacked an MCI or dementia diagnosis before death while individuals with symptomatic ADNP had a MCI or dementia before death.
Social determinants of health variables
At the initial UDS visit, participants self-report their sex assigned at birth (male, female), which we used as a proxy for gender. UDS participants also report their racialized group (i.e., White, Black or African American, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, Asian, or Other) and whether they identify as being Hispanic (i.e., “having origins from a mainly Spanish-speaking Latin American country”). From the questions on primary and additional self-reported racialized groups, NACC created a derived variable to indicate whether participants only report one racialized category or whether they identified as multi-racial (selected more than one racialized group), and this derived variable was used in our analyses. Also at their initial visit, participants report number of years of education completed and their primary language (English, Spanish, Mandarin, Cantonese, Russian, Japanese, Other). Due to small numbers of individuals reporting languages other than Spanish or English, we created a dichotomous variable indicating non-English primary language (yes, no). At each UDS visit, participants report their living situation (i.e., lives alone; lives with spouse or partner; lives with relative, friend, or roommate; lives with non-family/friend caregiver; lives with a group in private residence; lives in group home). From that variable, we created a dichotomous measure of lives alone (yes, no).
Statistical analyses
Descriptive statistics (mean and standard deviation, frequency and percentage) describe the demographics, clinical, and neuropathological characteristics of the sample stratified by asymptomatic ADNP status (yes versus no). Multivariable logistic regression using generalized estimating equations accounting for clustering by ADRC tested associations between SDOH and odds of asymptomatic ADNP. We ran a single model that included all SDOH as predictors and controlled for covariates including age at death (years), co-participant reporting that the participant's memory had declined, months between last UDS visit and autopsy, presence of ≥1 apolipoprotein E ε4 allele, self-reported comorbidities (hypertension, diabetes, or depression), and presence of Lewy body disease (brainstem predominant, limbic predominant, or neocortical) and/or vascular neuropathology (i.e., arteriolosclerosis, hemorrhage, microbleed, microinfarct, or infarct/lacune) at autopsy. Differences in associations by gender were examined by stratifying the model described above by gender, as well as by entering interaction terms separately in the multivariable models (e.g., primary language × gender and education × gender). We present models stratified by gender because while there may be significant associations found for women or men or both, we may lack sufficient statistical power to detect differences for smaller samples including Black or other racialized groups. In combination with this, gender stratified results are important to report irrespective of statistically significant interactions. Researchers on health disparities have called attention 33 to the importance of within group findings (e.g., Black women or men with lower education) as critical to report irrespective of statistically significant interactions focused on comparing groups. Analyses were conducted in SAS v9.4 and statistical significance was defined as p < 0.05.
Results
After exclusions, our analytic sample included 3107 individuals (Figure 1). Age at death was 80 ± 11 years and was greater for those with asymptomatic ADNP (88 ± 7 years) than symptomatic ADNP (80 ± 11 years) (Table 1). Forty-six percent were women, and a larger proportion of those with asymptomatic ADNP were women compared to those with symptomatic ADNP (59% versus 46%). Participants had 16 ± 8 years of education, with no differences by asymptomatic versus symptomatic ADNP. Ninety-three percent were White, 4% Black/African American, 0.1% American Indian/Alaska Native, 0.9% Asian, and 1.9% multiracial, and 4% were Hispanic, and no differences were observed in presence of asymptomatic versus symptomatic ADNP by racialized or ethnic group. Depression, apolipoprotein ε4 carriers, CDR-SB score, co-participant reported memory decline, severe ADNP (i.e., frequent neuritic plaques and Braak V-VI), and Lewy body disease neuropathology were more frequent/higher in the symptomatic than asymptomatic ADNP group.

Sample size flow diagram.
Sample characteristics for those with neuropathologically-confirmed Alzheimer's disease.

SD, standard deviation; APOE, apolipoprotein E, CDR-SB, Clinical Dementia Rating Sum of boxes; LBD, Lewy body disease; ADNP, Alzheimer's disease neuropathology.
aMissing data: racial group, n = 18; Hispanic, n = 12; marital status; LBD, n = 18; APOE, n = 354; vascular neuropathology, n = 238.
bArteriolosclerosis, hemorrhage, microbleed, microinfarct, or infarct/lacune found at autopsy.
cBrainstem predominant, limbic predominant, or neocortical
In adjusted analyses, women (OR = 1.02, 95% CI = 1.00–1.03), those with more years of education (OR = 1.004, 95% CI = 1.002–1.006), Hispanic individuals (OR = 1.07, 95% CI = 1.03–1.11), and those living alone (OR = 1.11, 95% CI = 1.06–1.17) were more likely to be asymptomatic with ADNP (versus symptomatic) (Table 2). Conversely, those whose primary language was not English were less likely to be asymptomatic with ADNP (OR = 0.88, 95% CI = 0.85–0.92). These adjusted models controlled for all of these characteristics simultaneously.
Association between social determinants of health and asymptomatic Alzheimer's disease neuropathology.
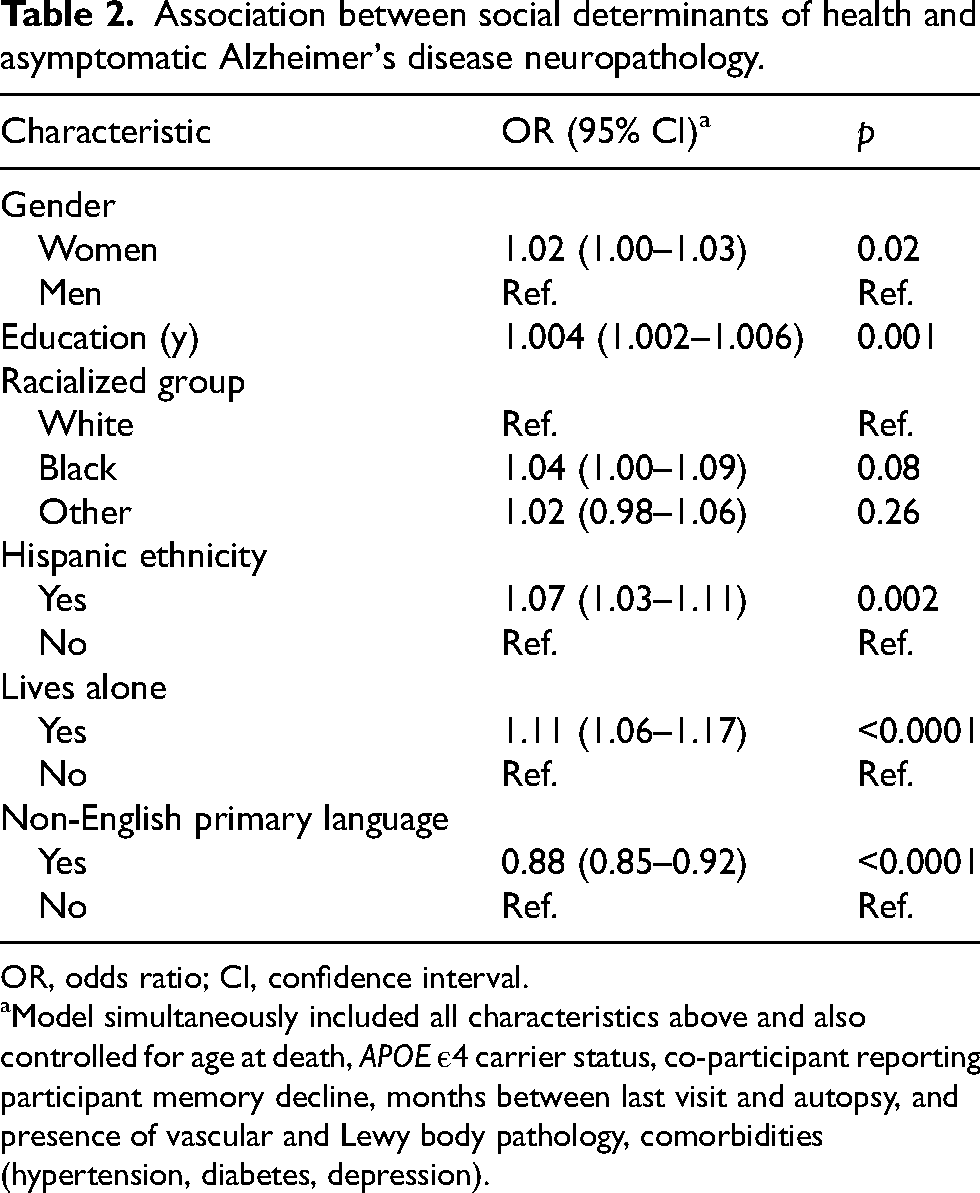
OR, odds ratio; CI, confidence interval.
Model simultaneously included all characteristics above and also controlled for age at death, APOE ε4 carrier status, co-participant reporting participant memory decline, months between last visit and autopsy, and presence of vascular and Lewy body pathology, comorbidities (hypertension, diabetes, depression).
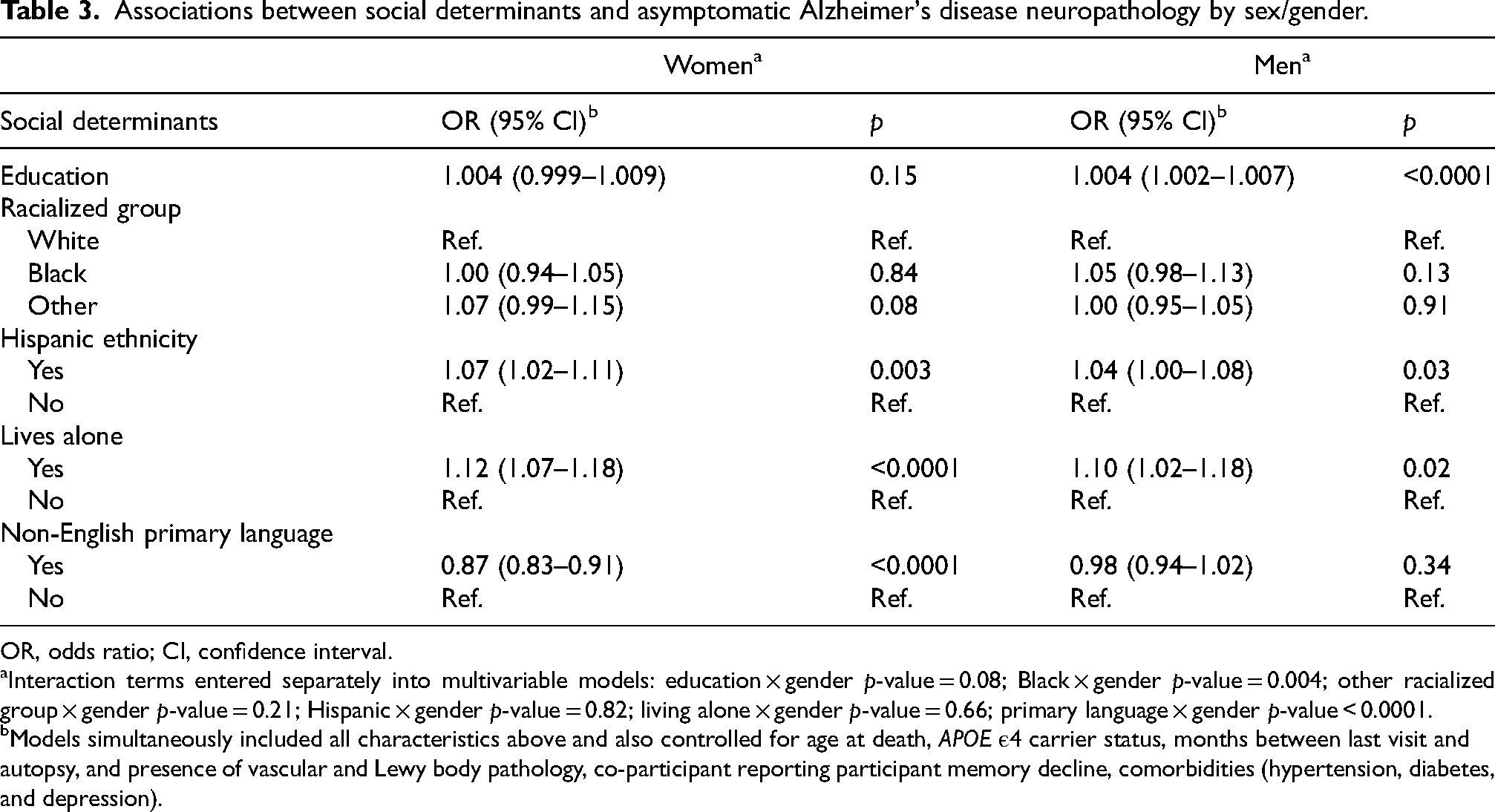
In adjusted analyses stratifying by gender, both men and women were more likely to be asymptomatic with ADNP if they were Hispanic (women: OR = 1.07, 95% CI = 1.02–1.11; men: OR = 1.04, 95% CI = 1.00–1.08) or living alone (women: OR = 1.12, 95% CI = 1.07–1.18; men: OR = 1.10, 95% CI = 1.02–1.18) (Table 3). Men with higher education were more likely to be asymptomatic with ADNP (OR = 1.004, 95% CI = 1.002–1.007), but the association between education and asymptomatic ADNP was not statistically significant for women (OR = 1.004, 95% CI = 0.999–1.009). Although the association between education and asymptomatic ADNP was significant for men but not women in the gender-stratified analyses, the difference in associations by gender were not statistically significant (i.e., education × gender interaction term p = 0.08). Women whose primary language was not English were less likely to be asymptomatic with ADNP (OR = 0.87, 95% CI = 0.83–0.91), with no such association observed for men (OR = 0.98, 95% CI = 0.94–1.02), and the difference by gender was significant (language × gender interaction term: p < 0.0001). On the other hand, while the interaction term between Black racial group (versus White) and gender was statistically significant (p = 0.004), the associations between Black racial group and asymptomatic ADNP was not significant for women (OR = 1.00, 95% CI = 0.94–1.05) or men (OR = 1.05, 95% CI = 0.98–1.13) in the gender-stratified models. Interaction terms between the other SDOH (i.e., other racial group, living alone, and Hispanic ethnicity) and gender were not statistically significant (p > 0.05) (reported in Table 3 footnote).
Associations between social determinants and asymptomatic Alzheimer's disease neuropathology by sex/gender.
OR, odds ratio; CI, confidence interval.
Interaction terms entered separately into multivariable models: education × gender p-value = 0.08; Black × gender p-value = 0.004; other racialized group × gender p-value = 0.21; Hispanic × gender p-value = 0.82; living alone × gender p-value = 0.66; primary language × gender p-value < 0.0001.
Models simultaneously included all characteristics above and also controlled for age at death, APOE ε4 carrier status, months between last visit and autopsy, and presence of vascular and Lewy body pathology, co-participant reporting participant memory decline, comorbidities (hypertension, diabetes, and depression).
Discussion
We found that women (versus men) were more likely to have asymptomatic ADNP, along with more educated and Hispanic individuals and those living alone. Non-English speakers were less likely to have asymptomatic ADNP. Stratified analyses showed that both women and men were more likely to have asymptomatic ADNP if they were Hispanic or living alone. Lastly, women speaking a non-English primary language were less likely to have asymptomatic ADNP, while men with more education were more likely to have asymptomatic ADNP. Although the difference in the odds of asymptomatic ADNP between women and men may not be clinically significant (OR = 1.02), effect sizes were larger when the association between primary language and asymptomatic ADNP was stratified by gender (OR = 0.87 for women and OR = 0.98 for men). This demonstrates the importance of considering the intersectionality of gender with other SDOH, which can uncover associations only present for one gender.
While women have a greater lifetime AD risk, at least one study suggested that women are less likely to be symptomatic with neuropathologically-confirmed AD, 34 and multiple studies demonstrated that older women perform better on cognitive tests than men. A prior study using the NACC Neuropathology Dataset found that 56% of women versus 44% of men had asymptomatic ADNP. 34 In addition, among ≥55-year-olds in the Longitudinal Aging Study Amsterdam and Doetinchem Cohorts, women demonstrated better processing speed, memory, and global cognitive function than men, and similar gender differences have been observed in other cohorts. 35 Reasons for gender-based disparities in cognitive status may relate to biological factors (e.g., genetics, hormones), but also social factors such as life course differences in social support/engagement that can impart cognitive reserve (brain employs alternative/compensatory approaches to complete a task that imparts resilience against brain injury/neurodegeneration) that delays cognitive decline onset.36,37 We demonstrated that among those with neuropathologically confirmed AD, women are less likely to be diagnosed with cognitive impairment than men after controlling for the other SDOH and important sociodemographic, clinical, genetic, and neuropathologic covariates. Thus, our study corroborates published studies in suggesting greater cognitive reserve for women.38,39
Although no known studies have investigated intersectional SDOH in relation to asymptomatic ADNP, our findings are informed by studies examining differences in cognitive function by gender, socioeconomic status, and ethnoracial group.40,41 A study of cognitively normal ≥60-year-olds in NACC's UDS found that fluid and crystallized memory scores were higher in women (versus men), those with more education (versus lower), and White (versus Black) individuals. 41 The study also found that women but not men had significantly higher ability discrepancy scores (crystallized ability minus average fluid ability) when they possessed a college versus high school degree. Another study combined English Longitudinal Study of Ageing (ELSA) and the Whitehall II study data to investigate the interplay of gender and education on cognitive functioning among ≥50-year-olds. 40 In that study, women in all birth cohorts (1930–1955) scored better on memory than men, men with lower education had higher semantic fluency, and women with greater education performed better on semantic fluency. Our findings are consistent with the two prior studies in that women were less likely to receive a diagnosis of cognitive impairment (e.g., greater cognitive reserve); in our case, despite having neuropathologically-confirmed AD. Unlike the prior studies that found statistically significant interactions between gender and education, we found that greater educational achievement was associated with asymptomatic ADNP in men but not women, but the education × gender interaction was not statistically significant. In our study, regression estimates were similar between men and women, suggesting no substantive differences in associations between education and asymptomatic ADNP by gender, but this will need to be further evaluated in other cohorts.
We found no difference in the presence of asymptomatic ADNP by racialized group, likely due to the limited diversity in the dataset. A significant limitation is that we could not focus on other racialized groups (i.e., American Indian/Alaska Native, Native Hawaiian/Pacific Islander, Asian, or multi-racial) due to limited sample size. Numerous studies have established racialized group disparities in cognitive testing and AD prevalence.1,20,42 These disparities are not inherent biological differences by racialized group, as a social construct, but instead are due to the uneven distribution of SDOH (e.g., education, occupation, health care). 43 Differences in SDOH and AD outcomes by racialized group are the result of systemic racism and associated structural determinants of health (e.g., policies and laws) that impact health throughout the life course, ultimately influencing brain health measured via cognitive testing and clinical and neuropathological evaluations. 43 While our study provides an initial look at potential intersectionality in associations with asymptomatic ADNP by gender and racialized group, diverse samples are crucial to test the hypothesis that asymptomatic ADNP varies by these factors.
For both men and women, we found that Hispanic ethnicity and living alone were associated with greater odds of asymptomatic ADNP. This might be explained by social factors that are protective against cognitive decline that are more prevalent or more beneficial in Hispanic populations, such as elements of social engagement, cohesion, and support.44,45 Although not currently collected in the UDS, these social factors might impact clinical diagnosis differentially by ethnicity and could be studied further in other cohorts. Our observed association between living alone and greater odds of asymptomatic ADNP may reflect the lack of a cohabitating study partner who can provide a more accurate assessment of potential cognitive decline 46 (e.g., during CDR assessment), which is considered during a clinical diagnosis. Similarly, individuals whose primarily language is not English may be more likely to receive a diagnosis of cognitive impairment due to language and cultural barriers affecting cognitive testing and clinical interviews/evaluations, 47 which ultimately impacts clinical diagnosis. Relatedly, we found that for women but not men, primary language other than English was associated with lower odds of asymptomatic ADNP (i.e., greater odds of MCI/dementia diagnosis). This may be explained by lower quality education in other countries for women compared to men, which may result in lower cognitive reserve or poorer neuropsychological test performance that affects the clinical diagnosis.
While cognitive reserve is often suggested as a mechanism to explain why older women perform better on cognitive testing than men,38,39 we did not demonstrate statistically significant intersectionality between gender and education in relation to asymptomatic ADNP (i.e., interaction p-value = 0.08). However, our single measure of cognitive reserve (education) may not have fully captured gender differences in cognitive reserve, such as elements of occupational and leisure time activities. Future studies of asymptomatic ADNP could incorporate other measures (e.g., Cognitive Reserve Index Questionnaire) to further examine intersectionality between gender and cognitive reserve. 48
Our study has several strengths. Unlike prior studies focused on cognitive outcomes, we examined intersectionality of gender and other SDOH in the context of symptomatology of neuropathologically-confirmed AD. Our study is unique in considering living alone status and primary language as SDOH that, by shaping life experiences in positive and negative ways, can differentially impact cognitive reserve and late-life symptoms. We used the large NACC dataset, which incorporates standardized data across >30 ADRCs, uses established ADNP criteria, and that allows for control of important sociodemographic, clinical, genetic, and neuropathologic covariates.
The study also has limitations. Autopsy study recruitment was not population-based and had inadequate racialized/ethnic diversity, limiting power to detect differences by racialized/ethnic group. Thus, findings may not be generalizable and need to be replicated in diverse samples. In this study, we estimated the number of individuals identifying as cisgender women or men from sex assigned at birth because NACC previously only collected data on sex. While sex and gender are the same for ∼97% of people, 9 the distinction is critical to consider and is significantly understudied in health research. We acknowledge the limitations of estimating gender based on sex, as well as our lack of data on non-cisgender, transgender, and non-binary/third gender individuals. Until recently, most aging cohort studies have not collected data on gender (collected sex assigned at birth exclusively) since gender only recently became recognized as an important SDOH for aging related outcomes including AD.7,8,49 In 2024, NACC is finalizing UDS version 4, which will collect data on both sex assigned at birth and gender. Thus, future studies can examine whether the results remain the same using the self-reported gender variable and can also examine associations for non-cisgender individuals. Additional SDOH (e.g., social support, engagement, cohesion) were not available to further explicate intersectional differences in asymptomatic ADNP. We could not tease apart whether asymptomatic ADNP disparities were more pronounced for some primary languages versus others due to few individuals (1%) speaking languages other than English and Spanish. Therefore, we view this paper as a catalyst for future studies using diverse cohorts that have both AD pathology/biomarker data and additional SDOH measures that will allow the elucidation of mechanisms linking our studied SDOH to asymptomatic ADNP. To maximize sample size, we defined ADNP as moderate to frequent neuritic plaques and Braak Stage III-VI, a definition used in many published neuropathology studies.50,51 Nonetheless, current criteria for ADNP incorporates Thal phase indicating location of amyloid plaques, which temporally progresses from midfrontal to cerebellum with increasing ADNP severity. 52 As neuropathology datasets that include Thal phase grow to provide a sufficiently diverse sample, our analyses can be redone using current ADNP criteria.
Overall, our study suggests that gender, education, Hispanic ethnicity, primary language, and living alone, as well as the intersectionality of primary language with gender, differentially influence the odds of asymptomatic ADNP. These findings emphasize the need for AD research to prioritize intersectional SDOH. Future research needs to replicate and expand upon our findings to understand the underlying biological mechanisms relating gender and other SDOH to cognitive reserve, as well as the social/structural mechanisms that influence whether some individuals (e.g., those living alone/lacking a close informant) are less likely to receive clinical diagnoses of cognitive impairment with underlying ADNP.
Footnotes
Acknowledgments
Dr Besser is supported by NIH/NIA R21 AG075291 and Alzheimer's Association Research Grant AARG-21-850963. The NACC database is funded by NIA/NIH Grant U24 AG072122. NACC data are contributed by the NIA-funded ADRCs: P30 AG062429 (PI James Brewer, MD, PhD), P30 AG066468 (PI Oscar Lopez, MD), P30 AG062421 (PI Bradley Hyman, MD, PhD), P30 AG066509 (PI Thomas Grabowski, MD), P30 AG066514 (PI Mary Sano, PhD), P30 AG066530 (PI Helena Chui, MD), P30 AG066507 (PI Marilyn Albert, PhD), P30 AG066444 (PI John Morris, MD), P30 AG066518 (PI Jeffrey Kaye, MD), P30 AG066512 (PI Thomas Wisniewski, MD), P30 AG066462 (PI Scott Small, MD), P30 AG072979 (PI David Wolk, MD), P30 AG072972 (PI Charles DeCarli, MD), P30 AG072976 (PI Andrew Saykin, PsyD), P30 AG072975 (PI David Bennett, MD), P30 AG072978 (PI Neil Kowall, MD), P30 AG072977 (PI Robert Vassar, PhD), P30 AG066519 (PI Frank LaFerla, PhD), P30 AG062677 (PI Ronald Petersen, MD, PhD), P30 AG079280 (PI Eric Reiman, MD), P30 AG062422 (PI Gil Rabinovici, MD), P30 AG066511 (PI Allan Levey, MD, PhD), P30 AG072946 (PI Linda Van Eldik, PhD), P30 AG062715 (PI Sanjay Asthana, MD, FRCP), P30 AG072973 (PI Russell Swerdlow, MD), P30 AG066506 (PI Todd Golde, MD, PhD), P30 AG066508 (PI Stephen Strittmatter, MD, PhD), P30 AG066515 (PI Victor Henderson, MD, MS), P30 AG072947 (PI Suzanne Craft, PhD), P30 AG072931 (PI Henry Paulson, MD, PhD), P30 AG066546 (PI Sudha Seshadri, MD), P20 AG068024 (PI Erik Roberson, MD, PhD), P20 AG068053 (PI Justin Miller, PhD), P20 AG068077 (PI Gary Rosenberg, MD), P20 AG068082 (PI Angela Jefferson, PhD), P30 AG072958 (PI Heather Whitson, MD), P30 AG072959 (PI James Leverenz, MD).
Author contributions
Lilah Besser (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing—original draft; Writing—review & editing); Anthony J Fuentes (Writing—original draft; Writing—review & editing); Jessica N Zhang (Writing—original draft; Writing—review & editing); Deirdre M O'Shea (Writing—original draft; Writing—review & editing); James E Galvin (Writing—original draft; Writing—review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Besser is supported by NIH/NIA K01 AG063895.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Besser, Dr O’Shea, and Dr Galvin are Editorial Board Member of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The remaining authors have no conflict of interest to report.