
Abstract
Background:
While mid-life hypertension represents a risk factor for the development of Alzheimer’s disease (AD), the risk after the age of 65 is less certain. Establishing relationships between late life hypertension and the pathological changes of AD could be crucial in understanding the relevance of blood pressure as a risk factor for this disorder.
Objective:
We investigated associations between self-reported late-life hypertension, cognitive status and AD pathology at death. The impact of antihypertensive medication was also examined.
Methods:
Using the Cornell Medical Index questionnaire, we ascertained whether participants had ever reported hypertension. We also noted use of antihypertensive medication. The donated brains of 108 individuals were assessed for AD pathology using consensus guidelines. Statistical analysis aimed to elucidate relationships between hypertension and AD pathology.
Results:
We found no associations between self-reported hypertension and cognitive impairment at death. However, those with hypertension were significantly more likely to exhibit lower levels of AD pathology as measured by Thal phase, Braak stage, CERAD score, and NIA-AA criteria—even after controlling for sex, level of education and presence of APOE ɛ4 allele(s). No significant associations could be found when examining use of antihypertensive medications.
Conclusions:
Our findings suggest that late-life hypertension is associated with less severe AD pathology. We postulate that AD pathology may be promoted by reduced cerebral blood flow.
INTRODUCTION
The term “dementia” describes a spectrum of conditions characterized by cognitive and behavioral impairment including memory loss, visuospatial difficulties, and language impairments [1]. As people live longer lives, it is anticipated that the prevalence of dementia worldwide will reach an estimated 150 million cases by the year 2050 [2].
The development of dementia is influenced by a range of risk factors encompassing demographical and lifestyle such as age, sex, educational attainment, smoking habits, and alcohol consumption, as well as morbidities such as hypertension.
Mid-life hypertension, defined as occurring between 40 and 65 years of age, represents a risk factor for the development of vascular dementia and Alzheimer’s disease (AD) [3–6]. After the age of 65 years, the relationship between hypertension and dementia is less certain. Establishing a direct relationship between hypertension and the pathological changes of AD could be crucial in understanding the relevance of blood pressure as a risk factor for dementia. However, it remains uncertain whether such a direct link exists [7]. Some studies showed that both low and high blood pressure are associated with an increased risk of dementia [8] while other studies concluded that late-life hypertension may protect from cognitive decline [9]. Animal models have sought to help elucidate the issue. For example, inducing hypertension in an amyloid precursor protein Tg2576 mouse model led to an increase in amyloid-β (Aβ) [10].
Several studies in humans [11] have explored the relationship between hypertension or blood pressure and AD neuropathological changes in late life, with a proportion showing an association between high blood pressure and increased severity of AD pathology [12, 13]. Likewise, midlife hypertension [14] and late-life hypertension [15] have also been associated with more severe AD pathology. By contrast, other studies have noted that high blood pressure was associated with less severe AD pathology through a mechanism attributed to the use of antihypertensive medications [16–19], while other reports have found no clear association between hypertension and severity of AD pathology [20–23].
Nonetheless, the populations investigated in previous studies and methods employed varied considerably leading to conflicting results. Further work is needed to elucidate the relationships between hypertension and the pathology associated with AD.
Self-reported hypertension is widely regarded as a robust measure of hypertensive status [13, 25]. Thus, in the present study, we exploited the data from The University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age (UMLCHA) [26] to investigate associations between self-reported hypertension, cognitive status, and AD pathology at death. The impact of antihypertensive medication has also been examined.
MATERIALS AND METHODS
Participants and study design
In 2003, individuals who were part of UMLCHA were approached to seek their consent for brain donation. Out of the initial 6,542 healthy participants recruited, ranging in age from 42 to 92 years, 312 agreed to donate their brain. To date, 134 brain donations have been collected. Information regarding the clinical and pathological features of this cohort has been previously documented [27, 28].
The study was approved by Manchester Brain Bank Management Committee (REC reference 19/NE/0242). Under conditions agreed with the Research Ethics Committee, The Manchester Brain Bank can supply tissue or data to researchers, without requirement for researchers to apply individually to the REC for approval.
The Cornell Medical Index (CMI) was employed to gather information about the medical history and lifestyle of each participant. This questionnaire covers both physical and mental health conditions. The CMI questionnaire was given to all participants at regular intervals between 1994 to 2007. Whether the participants had ever experienced hypertension was recorded in the CMI questionnaire as an answer to the question: “Has a doctor ever said your blood pressure was too high?” A positive indication on any of the CMI tests was recorded as ‘hypertensive’ whereas a negative response was noted as ‘normotensive’. The CMI questionnaire has been validated against clinical examinations in a number of previous studies [29]. Alongside this, we collected self-reported use of antihypertensive medications.
Furthermore, participants underwent five further rounds of cognitive assessment between 2004 and 2017 using the modified Telephone Instrument for Cognitive Status (TICSm), which encompasses 13 questions assessing cognitive domains such as orientation, concentration, immediate and delayed memory, naming, calculation, comprehension, and reasoning. The TICSm test [30] is scored with a maximum of 39 points, and for this study, a score of 21 was used as the threshold below which indicated the presence of cognitive impairment. Cognitive status at the time of death was determined by a combination of the last TICSm score, medical notes obtained from the participants’ general practitioners, and the cause of death as documented on the death certificate.
The APOE status was available for all cases.
Pathological examination
Postmortem brains were extensively sampled including the superior and middle frontal gyrus, anterior cingulate, superior and middle temporal gyrus, parietal, occipital cortex, hippocampus, amygdala, corpus striatum, thalamus, midbrain, pons and medulla, and cerebellum. The samples were routinely processed to paraffin embedding. 5μm-thick sections were cut from each block. One section was stained with hematoxylin-eosin and the other were used for immunohistochemical stains with antibodies directed against Aβ (Cambridge Bioscience, clone 4G8, 1 : 3000), tau protein phosphorylated at Ser202 and Thr205 (P-tau) (Innogenetics, clone AT8, 1 : 750), α-synuclein (BD Bioscience, clone 42/alpha synuclein, 1 : 500), and TAR DNA-binding protein 43 (TDP-43) (Proteintech, 1 : 1000). After dewaxing in xylene and rehydration in decreasing alcohols, the sections were either immersed in 70% formic acid for 20 min (Aβ and α-synuclein) or microwaved in 0.1 M citrate buffer with a pH of 6.0 (for all other antibodies) for antigen retrieval. The primary antibodies were incubated overnight at room temperature and the binding to the target protein was visualized using the VECTASTAIN Elite ABC kit (Vector Laboratories). Horse anti-mouse biotinylated secondary antibody was used for Aβ, phosphorylated-tau, and α-synuclein, while goat anti-rabbit biotinylated secondary antibody was utilized for TDP-43.
Two experienced neuropathologists (DM and FR) conducted the neuropathological evaluation using the consensus criteria and staging of neurodegenerative diseases [31–43]. Vascular pathology was assessed following the Vascular Cognitive Impairment Neuropathology Guidelines (VCING) [44].
For the purposes of this study, cases were excluded if the primary neuropathological diagnosis was not AD. Furthermore, AD cases were excluded if they exhibited any secondary or concurrent pathology, except for cerebral amyloid angiopathy (CAA) or small vessel disease. Cases of age-related tau astrogliopathy, primary ageing-related tauopathy, and limbic-predominant age-related TDP-43 encephalopathy were included as these pathologies are common age-related conditions.
Out of the 134 participants from the UMLCHA who had consented to brain donation, 108 met the eligibility criteria. An overview of the pathology of these eligible participants can be found in Supplementary Table 1.
Statistical analysis
After stratification based on hypertensive status, the cohort was divided into pathology groups according to severity of AD pathology: CERAD score: 0–A (low severity) versus B–C (high severity); Thal phase: 0–3 (low severity) versus 4–5 (high severity); Braak stage: 0–II (low severity) versus III–VI (high severity); National Institute on Aging and Alzheimer’s Association (NIA-AA) criteria: None to low (low severity) versus Intermediate to high (high severity).
Differences between hypertensive groups in sex, cognitive impairment, and presence of APOE ɛ4 allele(s) were analyzed with the Chi-squared test while those for age at death, age at baseline CMI, years between baseline CMI and death, age at final CMI, years between final CMI and death, and years of education were analyzed with the Mann-Whitney U test.
Differences between hypertensive groups regarding cognitive and pathology groups were analyzed with the Chi-squared test. Further binary logistic regression analyses were used to determine whether the influence of sex, years of education and presence of APOE ɛ4 allele(s) affected the outcome.
Use of antihypertensive medication and its effect on AD pathology was analyzed with the Chi-squared test.
In all cases, a p value of < 0.05 was considered significant.
RESULTS
Demographics
Information pertaining to the demographics of the 108 eligible participants is shown in Table 1. There were no significant differences in sex, age at death, age at baseline CMI, years between baseline CMI and death, age at final CMI, years between final CMI and death, education, or presence of APOE ɛ4 allele(s) between the normotensive and hypertensive groups.
Demographics of the UMLCHA cohort stratified by self-reported hypertensive status
ISCED, International Standard Classification of Education).
Associations between self-reported hypertension and cognitive impairment at death
Initial analysis showed that cognitive impairment at death was more likely in the normotensive group than in the hypertensive group (Fig. 1: χ2 = 4.2; p = 0.042). However, regression analysis demonstrated that after accounting for sex, level of education, and presence of APOE ɛ4 allele(s), the association between cognitive impairment and death and hypertensive status was no longer significant (Table 2: p = 0.056).
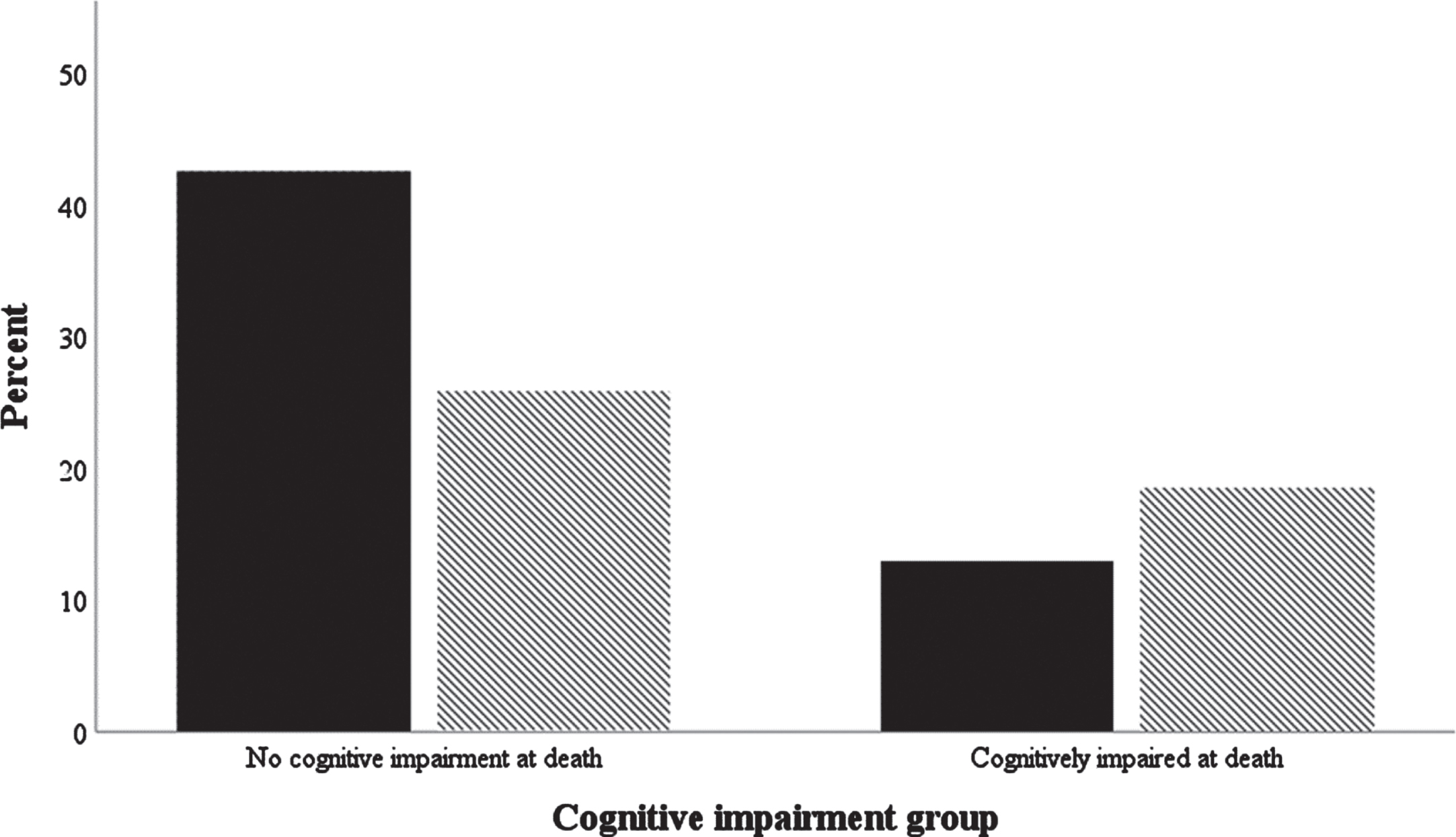
Associations between self-reported hypertension and cognitive impairment at death. Black = Hypertensive; Diagonal pattern = Normotensive.
Logistic regression analysis assessing the impact of sex, level of education, and presence of APOE ɛ4 allele(s) on the significant outcomes in presence of hypertension between cognitive impairment, Thal phase, CERAD score and Braak stage groups
Bold indicates significant difference. OR, Odds ratio; C.I., Confidence Interval.
Associations between self-reported hypertension and AD pathology at death
Relationships between self-reported hypertension and AD pathology as measured by Thal phase, CERAD score, Braak stage and NIA-AA criteria are shown in Fig. 2.
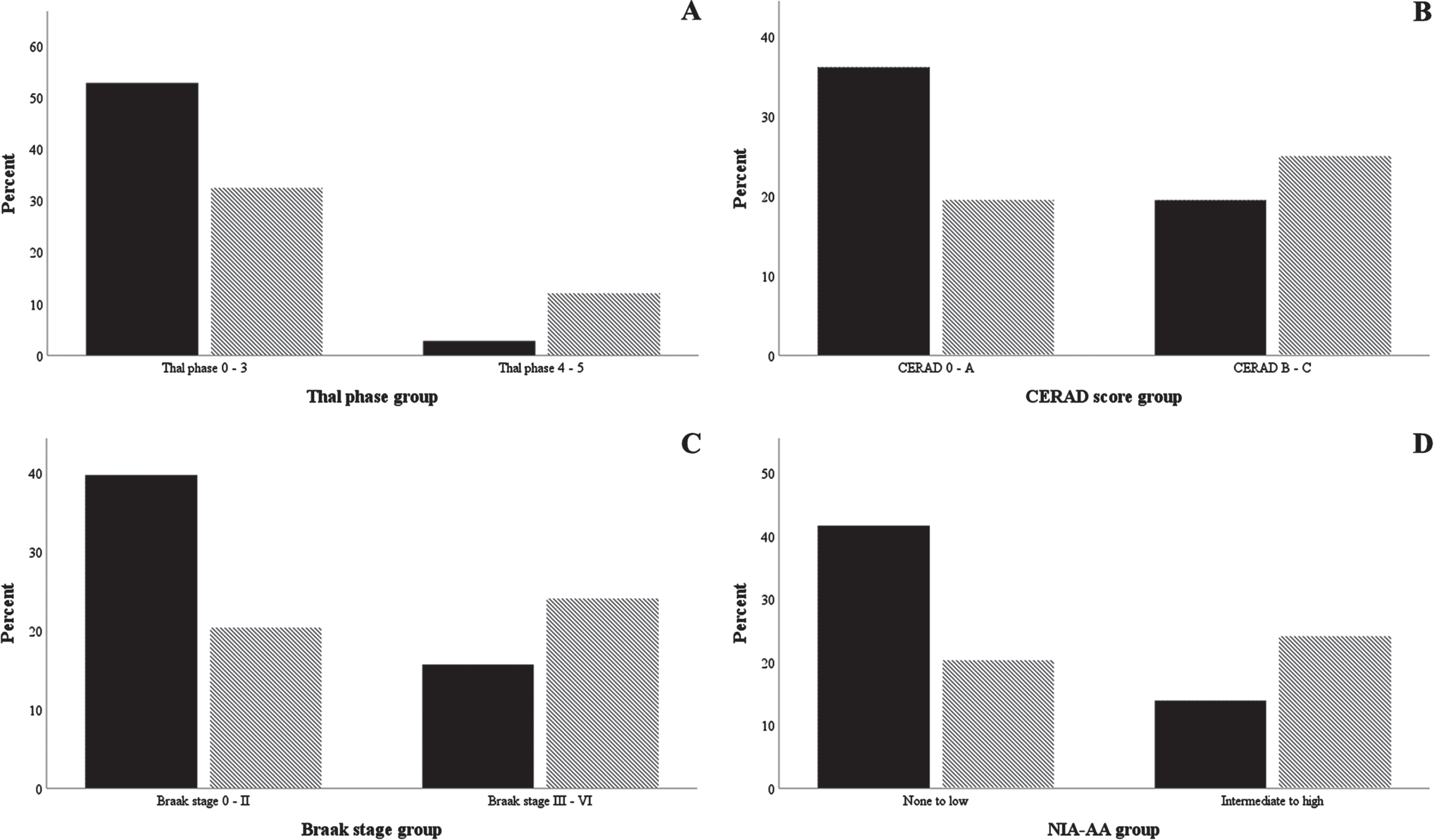
Associations between self-reported hypertension and AD pathology at death. A) Thal phase; B) CERAD score; C) Braak stage; D) NIA-AA grouping. Black = Hypertensive; Diagonal pattern = Normotensive.
Individuals with self-reported hypertension were more likely to be Thal phase 0–3 (χ2 = 10.3; p = 0.001), CERAD score 0-A (χ2 = 4.9; p = 0.027), and Braak stage 0-I (χ2 = 7.4; p = 0.006) than normotensive individuals. When considering NIA-AA criteria, those with self-reported hypertension were more likely to be in the none to low group when compared with normotensive individuals (χ2 = 9.6; p = 0.002)
Regression analyses (Table 2) showed that these significant differences remained after accounting for sex, level of education, and presence of APOE ɛ4 allele(s).
Use of anti-hypertensive medications
Of the 108 eligible participants, 60 (55.6%) reported that they had hypertension. Of these 60 individuals, 40 were known to be on hypertensive medications. A full breakdown of medications taken are shown in Table 3.
Breakdown of antihypertensive medications stated by those with self-reported hypertension
ACE, Angiotensin-converting enzyme.
When comparing individuals with high blood pressure taking antihypertensive medication against those taking no medication there were no differences of cognitive impairment at death (χ2 = 1.4; p = 0.239), nor were there any differences in AD pathology as measured by Thal phase (χ2 = 0.2; p = 0.664), CERAD score (χ2 = 0.6; p = 0.425), Braak stage (χ2 = 0.6; p = 0.447), or NIA-AA criteria (χ2 = 0.2; p = 0.664).
As documented in Table 3, individuals taking antihypertensive medications could be further stratified by those taking a single treatment and those taking combination treatment. However, there were no significant differences between no hypertensive treatment, single treatment or combination treatment when examining cognitive impairment at death (χ2 =3.8; p = 0.151), Thal phase (χ2 =0.2; p = 0.891), CERAD score (χ2 =0.8; p = 0.666), Braak stage (χ2 =0.9; p = 0.622), or NIA-AA criteria (χ2 =0.6; p = 0.739).
Associations between self-reported hypertension and vascular pathology at death
There was no significant difference in vascular pathology, as measured by VCING consensus criteria, between the normotensive and hypertensive groups (χ2 =3.4; p = 0.179). Similarly, when examining each of the features included in the VCING criteria, there were no significant differences between normotensive and hypertensive groups for presence of large (>10 mm) subcortical cerebral infarcts (χ2 =1.5; p = 0.227), presence of moderate or severe occipital leptomeningeal CAA (χ2 =0.24; p = 0.627) or moderate/severe occipital white matter arteriosclerosis (χ2 =1.1; p = 0.290).
DISCUSSION
The role of hypertension as a risk factor for AD and its effects on AD pathology is yet to be fully understood. The consensus view suggests that mid-life hypertension is more likely to lead to dementia [3–6, 45] and the pathological features associated with AD [11, 14] whereas the impact of late-life hypertension on dementia and AD pathology is less clear [15, 46]. The present study used a well-characterized cohort of elderly people for whom we held self-reported hypertension status and also had access to brain donation to ascertain associations between late-life hypertension, cognitive impairment and AD pathology. We also used the history of medications to determine whether antihypertensive medication might play any role in reducing cognitive impairment and AD pathology load.
When considering cognitive impairment, we found that there were no significant differences between the hypertensive and normotensive groups, nor were there any differences in cognitive impairment when comparing hypertensive individuals who were taking antihypertensive medications and those who were not. Although some studies have found an increase in incidence of cognitive impairment and dementia in those with late-life hypertension [15] others have reported contrasting results. For example, a recent study [8] observed that dementia risk was lower for older individuals with higher systolic pressure and that associations between diastolic pressure and the risk of dementia was similar, although the association was less clearly defined. The advanced age of the hypertensive individuals at time of baseline and final CMI data collection is likely to explain the similarity of our findings.
We found no significant differences in VCING scores [44] between the normotensive and hypertensive groups. A recent study showed an association between elevated late-life diastolic blood pressure and severe vascular damage, including arteriolosclerosis and CAA [47]. Replication of this result was not possible in the present study due to the method of data collection; self-reporting of hypertension does not provide systolic and diastolic readings. Similarly, imaging studies have shown that white matter hyperintensities and coinciding systolic blood pressure are most strongly associated in early- and mid-life [48–50]. As our study examined late-life hypertension, it is possible that the associations between self-reported hypertension and VCING scores were not seen due to the advanced age of the subjects. Controlling blood pressure with antihypertensive medication reduces the risk of cerebrovascular events [51]. The majority of the hypertensive participants in our study (67%) were on antihypertensive drugs, which possibly accounts for the lack of association between hypertensive status and VCING scores.
The present study demonstrated that late-life hypertension associated with less severe AD pathology, as measured by Thal phase, CERAD score, Braak stage, and NIA-AA criteria; findings which remained significant after controlling for sex, level of education and presence of APOE ɛ4 allele(s). These results concur with previous studies [16–19] but they contradict other studies [5, 20–23]. Such discrepant results may depend on the differences in methodology. Prior studies have varied widely in populations, assumptions regarding hypertensive status, statistical analyses, and neuropathological assessment. Here, we used ‘gold standard’ neuropathological criteria to assess AD pathology rather than an arbitrary measure of Aβ and tau (e.g., counts of neurofibrillary tangles or neuritic plaques in selected brain regions), which may lead to an inaccurate assessment.
Self-reported hypertension has been used in many previous studies as a way of determining hypertensive status [13, 25]. However, not all previous studies followed participants over time, suggesting that individuals with late-life hypertension could have been missed. Our study relied on self-reported hypertension over a number of years rather than just on one occasion. Unlike other studies, this approach allowed us to track individuals who only developed hypertension at a later time point. In contrast, using self-report as a way of determining hypertensive status also has limitations. Such limitations can be based around the participant, such as memory lapses or misunderstanding the comments of medical staff, or may reflect data collection methods, such as the inability to differentiate between diastolic and systolic blood pressure; a distinction shown to be important in dementia risk [8], cerebrovascular disease [20] and AD pathology [15].
The use of antihypertensive medication has been suggested as a possible reason for less AD pathology in those with hypertension [16–19]. A recent study [19] of 149 subjects found that in individuals with moderate or severe white matter small vessel disease, antihypertensive medication use was associated with lower Aβ accumulation. We were unable to replicate these findings and found no association with cognitive impairment at death or any of the measures of AD pathology and antihypertensive treatment. Sample size of those with hypertension (n = 60) and the proportion of these with uncontrolled hypertension (n = 20) is a limitation that may have impacted on our results.
It is also possible that the interaction between late-life hypertension and less severe AD pathology may work by a mechanism independent from antihypertensive medication. Some authors suggested that high blood pressure might be protective for the brain by increasing cerebral blood flow [46]. Aβ can be transported out of the brain and into the bloodstream through various pathways, including the blood-brain barrier, arachnoid villi, and the blood-cerebrospinal fluid barrier [52]. Thus, adequate blood flow is essential for effective clearance of Aβ. In addition, it has been suggested [47] that hypertension may contribute to the reduction of cerebral ischemia (potentially slowing down the accumulation of Aβ) in the presence of rising cerebral vascular resistance. However, this would be at the expense of exacerbating vascular pathology which could lead to later infarction or stroke. In contrast, tau cannot be transported across the blood-brain barrier, and it is thought its clearance mainly relies on degradation, interstitial fluid bulk flow, and cerebrospinal fluid absorption [53]. The lower tau load in those with late-life hypertension may be a secondary event. If Aβ is cleared from the brain quickly and efficiently, there may be less aggregate stress from decreased Aβ deposition and, therefore, a reduction in paired helical filament tau production as per the amyloid cascade hypothesis [54].
In conclusion, we postulate that late-life hypertension is associated with less severe AD pathology and suggest that AD pathology may be promoted by reduced cerebral blood flow. A clear correlation between antihypertensive medications and lower AD pathology could not be proven.
AUTHOR CONTRIBUTIONS
Andrew C. Robinson (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing); Tawfique Bin Rizwan (Data curation; Formal analysis; Investigation; Writing – original draft; Writing – review & editing); Yvonne S. Davidson (Data curation; Investigation; Writing – original draft; Writing – review & editing); James Minshull (Data curation; Investigation; Writing – original draft; Writing – review & editing); Phillip Tinkler (Data curation; Writing – original draft; Writing – review & editing); Antony Payton (Data curation; Writing – original draft; Writing – review & editing); David M.A. Mann (Data curation; Writing – original draft; Writing – review & editing); Federico Roncaroli (Data curation; Supervision; Writing – original draft; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The work of Manchester Brain Bank is supported by Alzheimer’s Research UK and Alzheimer’s Society through the Brains For Dementia Research (BDR) Programme. We would also like to thank Professor Neil Pendleton for his work on the UMLCHA cohort.
FUNDING
Longitudinal Cognitive studies were funded by Medical Research Council, Economic and Social Research Council, The Wellcome Trust [Grant reference number 003889] and Unilever PLC.
No funding was received for the specific work undertaken in this study.
CONFLICT OF INTEREST
Andrew Robinson is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.