
Abstract
Background
Clinical diagnosis in primary progressive aphasia (PPA) is challenging. Recently, emphasis has been placed on the importance of screening evaluation. Three different screening tests that use different strategies based on the assessment of language (Mini-Linguistic State Examination, MLSE) or different cognitive domains (Addenbrooke's Cognitive Examination, ACE-III and Dépistage Cognitif de Québec, DCQ) have been proposed and independently validated. These tests aim to detect PPA and classify into the three main variants (non-fluent (nfvPPA), semantic (svPPA) and logopenic (lvPPA)).
Objective
This study aims to evaluate and compare the diagnostic capacity of these three instruments in PPA.
Methods
A cross-sectional study including 43 patients with PPA (nfvPPA (n = 19), svPPA (n = 8), and lvPPA (n = 16)) and 21 cognitively unimpaired controls was conducted. Clinical diagnoses were established based on an extensive multidisciplinary assessment including neuropsychological assessment, fluorodeoxyglucose-positron emission tomography, MRI, and cerebrospinal fluid biomarkers. Both PPA patients and controls completed the three tests (MLSE, ACE-III, and DCQ).
Results
Internal consistency was excellent for the three tests. The area under the curve for the diagnosis of PPA was 0.950 for MLSE, 0.953 for ACE-III, and 0.933 for DCQ. Correlations between the three tests were high. The MLSE, ACE-III, and DCQ tests obtained adequate levels of discrimination between the variants of PPA, with accuracies between 76–79%.
Conclusions
This study confirms the validity of ACE-III, MLSE, and DCQ for the diagnosis of PPA and its variants. This suggests that detailed assessment of linguistic characteristics (MLSE) and non-linguistic features (DCQ, ACE-III) are relevant for the diagnosis and classification of PPA.
Keywords
Introduction
Primary progressive aphasia (PPA) is a clinical syndrome with insidious onset characterized by prominent language impairment secondary to a neurodegenerative disorder. 1 PPA may be the onset of Alzheimer's disease (AD) or several forms of frontotemporal degeneration (FTD). 2 The diagnosis of PPA is made following the international consensus criteria by Gorno-Tempini et al. (2011). 3 Accordingly, three main subtypes are recognized: non-fluent variant (nfvPPA), semantic variant (svPPA), and logopenic variant (lvPPA). Each variant presents relatively specific clinical, anatomical, and neuropathological characteristics. These diagnostic criteria provide a standardized framework for the identification and classification of PPA. Nonetheless, diagnosis remains challenging. Patients often experience significant delays in receiving a proper diagnosis compared to other neurodegenerative disorders and they may be initially assigned alternative diagnostic labels.4,5 Additionally, it is acknowledged that not all patients meet the proposed criteria due to either presenting a mixed clinical profile or exhibiting isolated language deficits.3,6,7 Some authors suggest that challenges in classifying PPA variants also arise from the lack of consensus regarding specific tests for assessing the different symptoms and deficits, highlighting the need for standardized batteries in this patient population.7,8
Over the past few years, there has been a growing interest in developing and validating tests specifically for atypical causes of cognitive impairment, such as PPA. 9 However, there are still issues with the reliability, examiner consistency, and administration time of these tests. Some tests have been developed or applied to address this issue, 10 but tests with greater discriminative validity are still needed. At the same time, some authors have evaluated the sensitivity and specificity of neuroimaging tools11,12 or fluid biomarkers.13,14 However, the controversy regarding the applicability of the consensus criteria7,15,16 and the best clinical tools to diagnose and categorize PPA variants is still open.17–19 For these reasons, there is a need for standardized tests that are accessible and easy to administer. Screening tests are used in populations at risk of having a disease and represent the initial approach to the patient. They therefore require a high level of sensitivity, and a simple and brief application format. 20 Moreover, given the rising number of people who require an evaluation for cognitive complaints, along with the long waiting lists and limited resources, conducting comprehensive assessments often becomes challenging, highlighting the importance of this initial screening. 21
Two screening tools that were specifically developed for assessing patients with language impairments are the Mini-Linguistic State Examination (MLSE) 22 and the Dépistage Cognitif de Québec (DCQ). 23 The MLSE consists of various subtests that assess different language abilities, including reading, writing, oral production, oral comprehension and naming. The DCQ is a comprehensive screening test that evaluates language and other cognitive functions such as executive functions, memory, visuospatial abilities, and behavior. Furthermore, there are widely used tools in neuropsychology that have proven useful in PPA, such as the Addenbrooke's Cognitive Examination III (ACE-III). 24 This test includes five subdomains: attention, memory, fluency, language and visuospatial. In this regard, ACE-III may be useful in detecting patients with PPA and in delineating its variants. 25
The three mentioned tools offer a standardized approach that is easily accessible and simple to implement, making them practical for routine clinical use. They are efficient and less time-consuming compared to more complex language and neuropsychological assessments. Furthermore, both the MLSE and ACE III have been adapted and validated in several languages, including Spanish,21,26,27 which broadens their applicability. In contrast, the DCQ has versions available only in French and English.23,28,29 To our knowledge, there are no studies comparing the diagnostic capacity of these tools. This kind of study comparing the diagnostic performance of different neuropsychological instruments in the same population is relevant to contextualize the usefulness of each cognitive test and provide efficient alternatives without compromising diagnostic accuracy. Therefore, this study aimed to compare the diagnostic capacity of these three instruments, MLSE, ACE-III, and DCQ, in detecting PPA and distinguishing between PPA variants. We also aimed to present the adaptation of the DCQ into Spanish.
Methods
Study design and participants
A comparative, observational, cross-sectional study was conducted with 64 participants recruited between September and December 2022 at the Department of Neurology of the Hospital Clínico San Carlos, Madrid, Spain. The clinical group consisted of 43 patients diagnosed with PPA who were consecutively recruited from patients attending the department. The healthy control (HC) group comprised 21 voluntary participants. Participants from both groups met the inclusion and exclusion criteria defined below.
The HC group was recruited among the relatives of patients attending the Neurology Department, considering the age range, education level, and sex of the patients diagnosed with PPA evaluated to ensure there were no sociodemographic differences between the groups. The main clinical and demographic characteristics of patients and controls are depicted in Table 1.
Main demographic characteristics of HC, PPA, and PPA variants.

U-Mann Whitney; bChi-squared.
The inclusion criteria for the clinical group were as follows: (1) PPA diagnosed and classified according to Gorno-Tempini et al. (2011), 3 (2) Spanish-speaking individuals, (3) aged between 50 and 90 years. The diagnostic gold standard was determined by applying the diagnostic criteria of Gorno-Tempini et al. (2011) 3 based on the results of a comprehensive language assessment battery, as well as the findings from MRI and fluorodeoxyglucose (FDG)-positron emission tomography (PET) imaging. The exclusion criteria included: (1) severe language impairment that hinders the ability to follow instructions, (2) uncompensated auditory or visual impairments, (3) previous neurological history involving acquired lesions or neurodevelopmental disorders.
The inclusion criteria for HC were: (1) Spanish-speaking individuals, (2) aged 50 to 90 years, (3) absence of cognitive impairments, confirmed through a Mini-Mental State Examination score greater than 27, (4) absence of psychiatric, neurological, or neurodevelopmental disorders, (5) preserved or compensated visual and auditory abilities.
Assessments
To confirm the clinical diagnosis, the patients underwent a standard neurological and neuropsychological evaluation, and an in-depth language assessment, which has been described in a previous study. 30 Patients were also examined in all cases with MRI and FDG-PET imaging. Cerebrospinal fluid (CSF) biomarkers were also available in selected cases when clinically needed.
Both PPA and HC were evaluated with the Spanish version of the three screening tests: MLSE, 26 ACE III21,27 and DCQ.
MLSE
MLSE is a brief screening test designed to evaluate language impairments in various neurodegenerative disorders, specifically PPA. 22 It consists of the following tasks that assess different language processes: naming, syllable repetition, repeat and point, non-word repetition, semantic association, sentence comprehension, reading, sentence repetition, writing, and picture description. These tasks are grouped to generate scores in five language domains: motor, phonology, semantics, syntax, and working memory, and scoring is done by classifying the errors made by the subject. The time of administration is approximately 20 min.
ACE-III
ACE-III is a general cognitive screening tool that assesses attention, memory, verbal fluency, language, and visuospatial skills. 24 It consists of the following tasks: temporal-spatial orientation, 3-item registration, serial subtractions, recall of 3 words, formal fluency, categorical fluency, anterograde memory (name and address registration), retrograde memory, command comprehension, sentence writing, word repetition, proverb repetition, naming, semantic knowledge, reading irregular words, infinite constructive praxis, cube constructive praxis, clock drawing, dot counting, incomplete letters, free recall of name and address, and name and address recognition. The scores are grouped into five cognitive subdomains: attention, memory, verbal fluency, language, and visuospatial. A higher total score indicates better cognitive functioning of the individual. The time of administration is approximately 15 min.
DCQ
DCQ is a general cognitive screening tool designed to identify atypical dementias which assesses memory, visuospatial skills, executive functions, language, and behavior.23,31 It consists of the following tasks: forward digit span, immediate registration and recall of a word list, delayed recall of the list, list recognition, overlapping figures, visuospatial rotation, visuospatial construction, letter detection, backward digit span, months backward, alternate sequence, abstraction, verbal fluency, modified Stroop, storytelling, naming and writing, sentence writing, comprehension, semantics, repetition, social cognition. Additionally, it includes a caregiver questionnaire that is considered within the behavior index score. The time of administration is approximately 25 min.
The DCQ has been developed in both English and French,28,29 and it was specifically adapted to Spanish for this study.
DCQ adaptation
The adaptation of the DCQ to Spanish was carried out following the methodology proposed by the International Test Commission. 32 Initially, blinded translation and back-translation of the protocol and verbal items of the stimulus booklet were performed. The documents from the English version 23 were used as a reference as they were the latest produced by the authors and presented slight modifications compared to those of the previous French version.
A cultural and linguistic verification of the stimuli was conducted, considering the existing differences between both populations. Changes were made in the following tasks: (1) Immediate registration and recall of a word list. Three stimuli were changed: “pineapple” to “PERA” (pear), “jacket” to “PANTALÓN” (pants), and “volleyball” to “NATACIÓN” (swimming). The modification was made considering the discrepancy between the frequency of each word's usage in its original language and Spanish. This modification also impacted the tasks of delayed recall and word list recognition; (2) Modified Stroop task. In the original versions, the selected colors were yellow, green, red, and blue. On one hand, the tone of the blue was changed to a classic blue without any additional color. On the other hand, yellow was changed to black (“negro”), as the Spanish word for yellow (“amarillo”) has a significantly higher number of letters compared to the other colors. Thus, in the Spanish version, the colors were black, red, green, and blue. Accordingly, all colors had a length of 4 to 5 letters; 3) Visuospatial rotation. A slight modification was made to the task instructions. The English version states, “Picture yourself on the bicycle. Which of these images best corresponds to what you would see in front of you?”. In the modified Spanish version, it mentions, “Observe the man on the bicycle. Which of these images best corresponds to what the man is seeing in front of him?”. The task is intended to assess processes related to visuospatial abilities, and requesting the participants to position themselves as if they were the person in the image creates an additional difficulty that goes beyond the main objective of the task.
Procedure of administration
The three tests were administered in the same session, and the order of administration was changed every 10 cases. The diagnosis of PPA variant was made independently of the results, and before the tests were administered according to the collected clinical information, neuropsychological assessment, and neuroimaging.
Statistical analysis
Statistical analysis was performed using IBM® SPSS Statistics 24.0 and R. Descriptive data are presented as mean (M) ± standard deviation (SD), and a p-value <0.05 was considered statistically significant.
Pearson's correlations between the different tests were calculated to assess convergent validity, that is, how well the different tests that measure similar constructs are related. Comparisons between PPA and control means were calculated using the Mann-Whitney U test, while Kruskal-Wallis with a post-hoc analysis was used for comparisons between the three types of PPA. Bonferroni correction was applied to correct for multiple comparisons. Effect sizes were calculated (Cohen's d, eta-squared), considering small (d = 0.2; η2 = 0.01), medium (d = 0.5; η2 = 0.06), and large (d = 0.8; η2 = 0.14) effects.
Additionally, receiver-operating characteristic (ROC) curves with a 95% confidence interval were estimated for the discrimination between PPA patients and control participants. The ROC curves help determine the test's ability to correctly classify individuals into PPA group or control group. To compare the ROC curves and evaluate the observed differences in diagnostic capacity, the DeLong et al. (1988) 33 method was used, a statistical technique employed to determine if there are significant differences in the area under the curve between the tests.
Multinomial logistic regression analysis was performed to create a model of the relationship between the predictor variables (test subdomain scores) and the diagnosis of each PPA variant for each test.
Results
Diagnosis of PPA
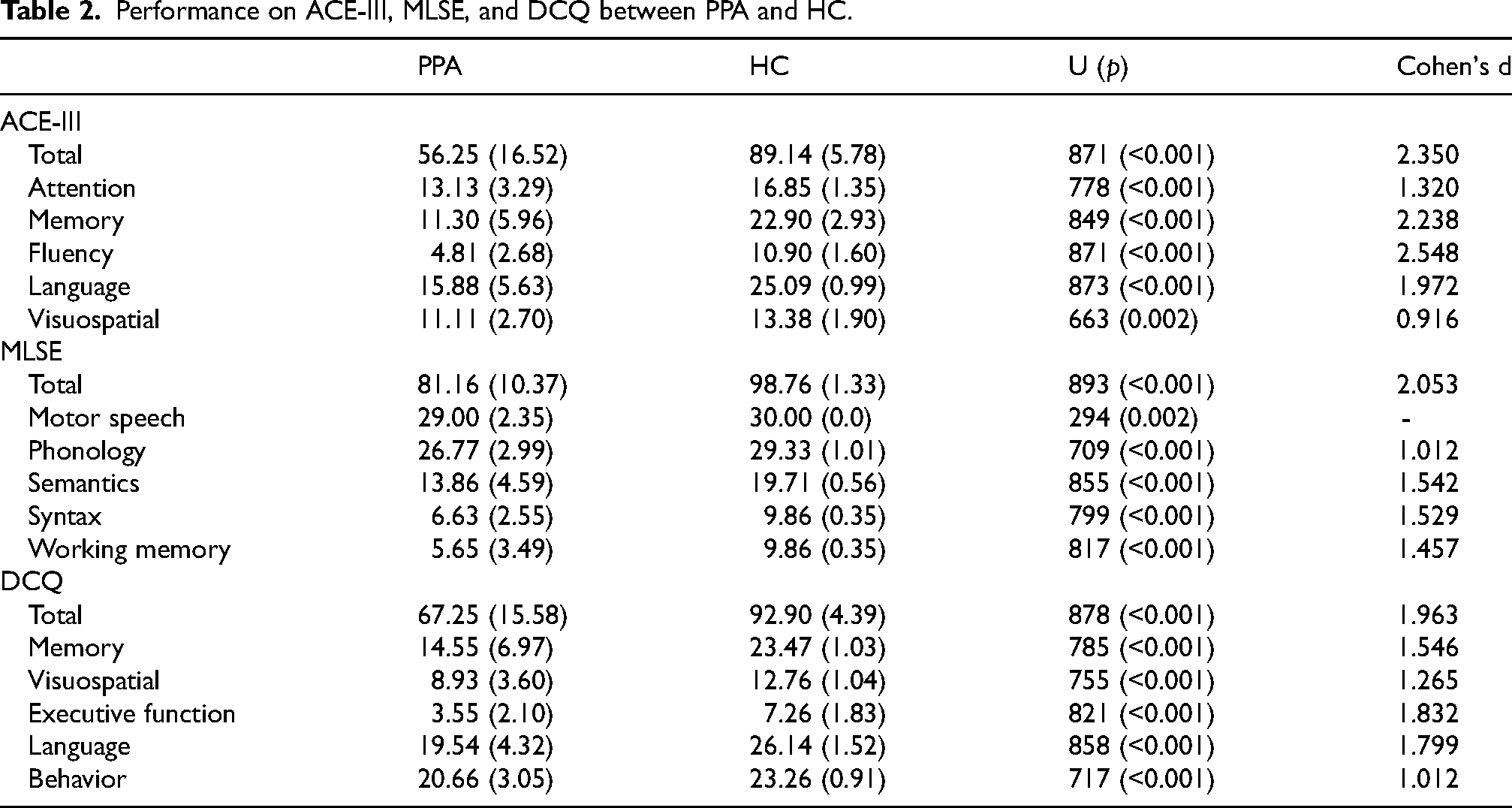
The clinical group showed significantly lower performance in all ACE-III, MLSE, and DCQ scores (Table 2). Effect sizes were large for all the scores. The area under the curve was 0.965, 0.989, and 0.973 (in all cases p < 0.001), respectively (Figure 1). According to Youden's index, the best cutoff for the ACE-III was 76 (Youden's index = 0.90, sensitivity 100%, specificity 90.7%); for the MLSE it was 96 (Youden's index = 0.93, sensitivity 100%, specificity 93.02%); and for the DCQ was 85.5 (Youden's index = 0.81, sensitivity 95.24%, specificity 86.05%). There were no statistically significant differences in the comparison between the three areas under the curve according to the DeLong test (p = 0.418).

ROC curve analysis for the discrimination between PPA and HC using ACE-III total (blue), DCQ total (red), and MLSE (orange).
Performance on ACE-III, MLSE, and DCQ between PPA and HC.
Differential diagnosis between PPA variants
There was a statistically significant effect group for all the scores of ACE-III, MLSE, and DCQ (p < 0.001 in all cases). Post-hoc analyses showed statistically significant differences between nfvPPA and svPPA in MLSE-semantics (M = 17.21 ± 2.15 and M = 7.86 ± 2.41, respectively) and DCQ-memory (M = 19.26 ± 6.05 and 8.14 ± 4.56). There were differences between nfvPPA and lvPPA in ACE-III-total (M = 65.74 ± 14.7 and 46.88 ± 14.94), ACE-III-memory (M = 14.90 ± 5.86 and M = 7.71 ± 4.50), MLSE-semantics (17.21 ± 2.15 and M = 12.59 ± 4.15), and DCQ-memory. In the comparison between lvPPA and svPPA, there were significant differences in MLSE-phonology (M = 25.24 ± 2.77 and M = 29.14 ± 0.9, respectively).
In addition, there were significant differences when comparing each PPA variant and HC. Specifically, nfvPPA and HC showed differences in ACE-III-total (M = 65.74 ± 14.7 and M = 89.14 ± 5.78), ACE-III-attention (M = 13.90 ± 3.07 and M = 16.86 ± 1.35), ACE-III-fluency (M = 5.37 ± 3.22 and M = 10.91 ± 1.61), ACE-III language (M = 19.42 ± 4.11 and M = 25.10 ± 1.0), ACE-III visuospatial (M = 12.16 ± 2.5 and M = 13.38 ± 1.91), MLSE-total (M = 85.58 ± 11.11 and M = 98.76 ± 1.34), MLSE-motor speech (M = 28.26 ± 3.33 and M = 30.0 ± 0.0), MLSE-phonology (M = 27.26 ± 3.03 and M = 29.33 ± 1.02), MLSE-semantics (M = 17.21 ± 2.15 and M = 19.71 ± 0.56), MLSE-syntax (M = 7.32 ± 2.43 and M = 9.86 ± 0.36), MLSE-working memory (M = 6.79 ± 2.97 and M = 9.86 ± 0.36), DCQ-total (M = 75.95 ± 13.92 and M = 92.91 ± 4.39), DCQ-visuospatial (M = 10.16 ± 2.67 and M = 12.76), DCQ-executive (M = 4.0 ± 2.07 and M = 7.26 ± 1.84), DCQ-language (M = 21.21 ± 4.57 and M = 26.14 ± 0.92), and DCQ-behavior (M = 21.29 ± 2.86 and M = 23.26 ± 0.92).
When comparing lvPPA and HC, there were significant differences in ACE-III-total (M = 46.88 ± 14.94 and M = 89.14 ± 5.78), ACE-III-attention (M = 11.59 ± 3.34 and M = 16.86 ± 1.35), ACE-III-memory (M = 7.71 ± 4.5 and M = 22.91 ± 2.93), ACE-III-fluency (M = 4.29 ± 2.17 and M = 10.91 ± 1.61), ACE-III language (M = 13.53 ± 5.52 and M = 25.10 ± 1.0), ACE-III visuospatial (M = 9.77 ± 2.46 and M = 13.38 ± 1.91), MLSE-total (M = 75.47 ± 8.75 and M = 98.76 ± 1.34), MLSE-phonology (M = 25.24 ± 2.77 and M = 29.33 ± 1.02), MLSE-semantics (M = 12.59 ± 4.15 and M = 19.71 ± 0.56), MLSE-syntax (M = 5.18 ± 2.33 and M = 9.86 ± 0.36), MLSE-working memory (M = 3.47 ± 3.56 and M = 9.86 ± 0.36), DCQ-total (M = 60.38 ± 13.9 and M = 92.91 ± 4.39), DCQ-memory (M = 11.94 ± 5.20 and M = 23.48 ± 1.03), DCQ-visuospatial (M = 7.88 ± 4.15 and M = 12.76 ± 1.04), DCQ-executive (M = 2.47 ± 1.92 and M = 7.26 ± 1.84), DCQ-language (M = 17.47 ± 3.85 and M = 26.14 ± 1.53), and DCQ-behavior (M = 19.07 ± 2.51 and M = 23.26 ± 0.92).
Finally, there were differences in ACE-III-total (M = 5.29 ± 11.18 and M = 89.14 ± 5.78), ACE-III-memory (M = 10.29 ± 3.68 and M = 22.91 ± 2.93), ACE-III-fluency (M = 4.57 ± 2.23 and M = 10.91 ± 1.61), ACE-III language (12.0 ± 4.12 and M = 25.10 ± 1.0), MLSE-total (M = 83.0 ± 4.66 and M = 98.76 ± 1.34), MLSE-semantics (7.86 ± 2.41 and M = 19.71 ± 0.56), DCQ-total (M = 60.36 ± 13.24 and M = 92.91 ± 4.39), DCQ-memory (8.14 ± 4.56 and M = 23.48 ± 1.03), DCQ-visuospatial (M = 8.14 ± 3.89 and M = 12.76 ± 1.04), DCQ-language (M = 20.07 ± 2.78 and M = 26.14 ± 1.53), and DCQ-behavior (M = 19.07 ± 2.51 and M = 23.26 ± 0.92) in the comparison between svPPA and HC. The comparisons between the different subdomains of each test are also depicted in Table 3.
Performance of ACE-III, MLSE, and DCQ across groups.
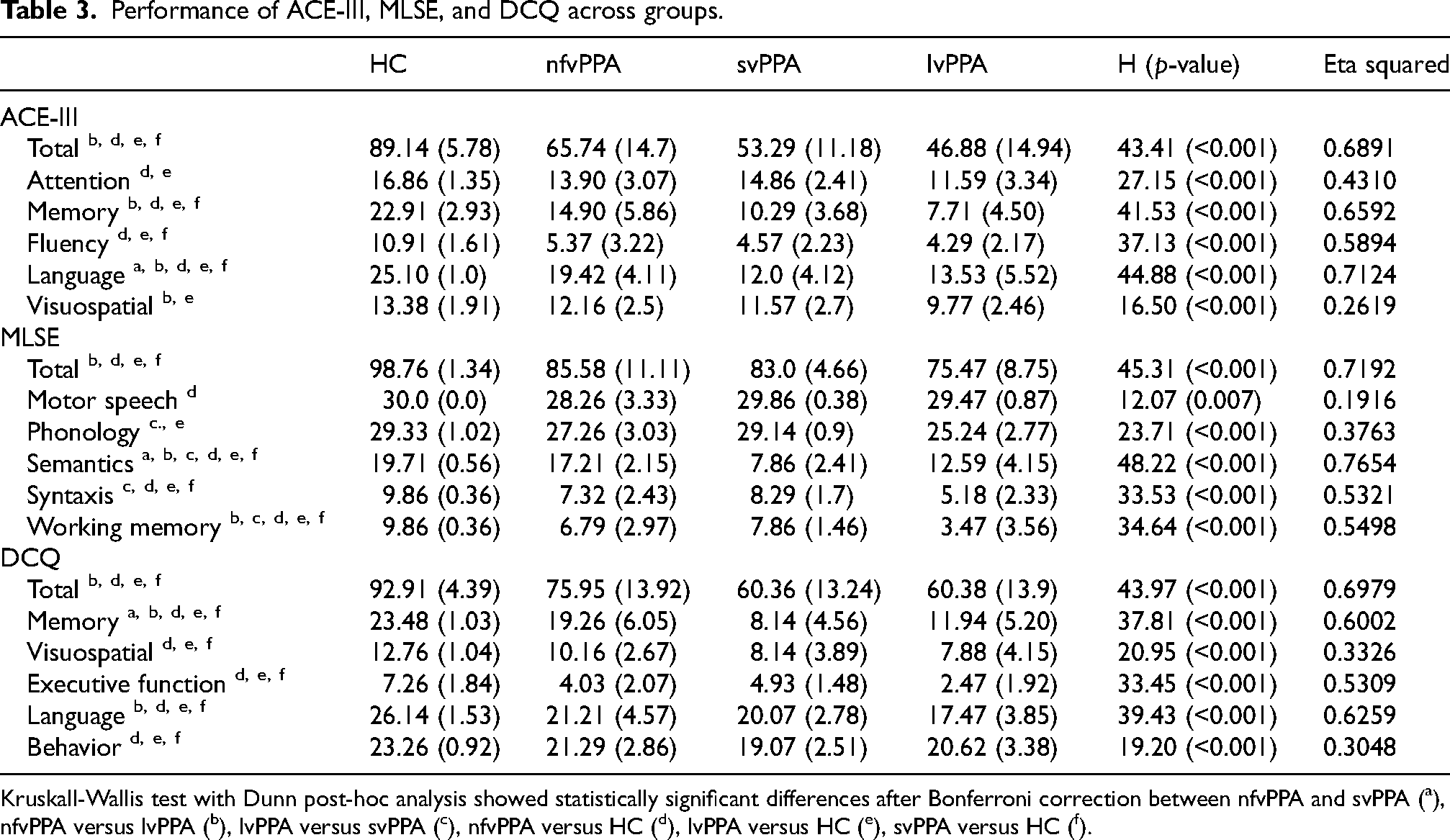
Kruskall-Wallis test with Dunn post-hoc analysis showed statistically significant differences after Bonferroni correction between nfvPPA and svPPA (a), nfvPPA versus lvPPA (b), lvPPA versus svPPA (c), nfvPPA versus HC (d), lvPPA versus HC (e), svPPA versus HC (f).
Internal consistency correlations between tests
Internal consistency was excellent for the three tests. Cronbach's alpha was 0.911 for ACE-III, 0.857 for MLSE, and 0.902 for DCQ.
ACE-III-total showed high correlations with MLSE-total (r = 0.881, p < 0.001) and DCQ-total (r = 0.943, p < 0.001). MLSE-total was also highly correlated with DCQ-total (r = 0.867, p < 0.001).
Multinomial logistic regression analysis
The model for MLSE (χ 2 = 58.97, p < 0.001, Nagelkerke's R2 0.741) correctly classified 79.1% of cases (83.3% of nfvPPA, 100% of svPPA, and 66.7% of lvPPA). lvPPA was distinguished from nfvPPA by MLSE-semantics. SvPPA was distinguished from nfvPPA with MLSE-motor speech, MLSE-phonology, MLSE-semantics, and MLSE-syntax.
The model for ACE-III (χ 2 = 40.40, p < 0.001, Nagelkerke's R2 0.543) correctly classified 76,7% of cases (77.8% of nfvPPA, 71.4% of svPPA, and 77.8% of lvPPA). ACE-III-language distinguished between nfvPPA versus svPPA, ACE-III-memory between nfvPPA versus lvPPA, and ACE-III-language and ACE-III-visuospatial distinguished between svPPA versus lvPPA.
The model for DCQ (χ 2 = 39.16, p < 0.001, Nagelkerke's R2 0.529) correctly classified 76.7% of cases (72.2% of nfvPPA, 85.7% of svPPA, and lvPPA 77.8%). DCQ-memory distinguished between nfvPPA versus svPPA, and nfvPPA versus lvPPA.
Discussion
Our study found a high diagnostic capacity and excellent reliability of the three tests ACE-III, MLSE, and DCQ for the diagnosis of PPA as a group. These results confirm the usefulness of these brief assessments for the detection of PPA and are consistent with previous studies validating individually these tools in the diagnosis of PPA (MLSE, 22 DCQ, 23 ACE III 24 ). Interestingly, the diagnostic capacity for detecting PPA compared with controls was very high in the three cases, and there were non-statistically significant differences between the three tests. This finding suggests that the three tools have similar validity in the screening of PPA. This is clinically meaningful, especially in non-specialized settings where PPA diagnosis might not be suspected, because it suggests that a specific language test designed for PPA, like the MLSE, is not strictly necessary to detect potential cases of PPA. MLSE could be more appropriate for assessment in specialized contexts where professionals have knowledge regards language processes and aphasic errors. General screening tests, such as the ACE-III and DCQ, could be enough in non-specialized settings, as they could also be sensitive to other causes of cognitive dysfunction. 34
Another important finding of our study is regarding the discrimination between PPA variants. The three tests reached good levels of classification (76–79%) of patients with PPA into the three clinical variants. This finding is noteworthy, considering the difficulties in the differential diagnosis of PPA variants. In this regard, previous studies applying consensus criteria with comprehensive language batteries obtained a significant proportion of unclassifiable or misclassified patients.6,7,35 Even specific batteries such as SYDBAT obtained an 80% of correct classification. 36 As the three tests used different approaches (assessment of several cognitive domains in ACE-III and DCQ, and specific assessment of language in MLSE), our study suggests that both language and other cognitive functions are relevant in the differential diagnosis of PPA variants. The usefulness of non-language tasks, in addition to the assessment of language deficits, has also previously been suggested for the differential diagnosis of PPA. 37 In the comparison of means, lvPPA showed a lower performance in ACE-III total and memory. This may suggest a more general cognitive impairment, as has been suggested in the literature. 38 However, the degree of word finding difficulties may also explain this finding in the ACE-III and the DCQ-memory, because these tests assess verbal episodic memory and anomia is generally more prominent in svPPA and lvPPA than nfvPPA. 2 It is worth mentioning that all variants may display involvement of the different language and cognitive functions. The analysis of the probability of each variant according to the different scores on each test domain confirms, on the one hand, the usefulness of the tests, because the probability changes along the score range of each item; but, on the other hand, it confirms that there are no specific cognitive or language functions of each PPA variant. The search for dissociations and the individual comparison between functions may be more informative than the group comparisons. In this regard, multinomial regression analysis found that many of the test domains were useful in discriminating between PPA variants.
Our study also provides a Spanish version of the DCQ. The DCQ was specifically designed to detect cognitive patterns associated with atypical dementias such as PPA. It is more accurate in detecting atypical dementias than the Montreal Cognitive Assessment, 18 and it is able to distinguish between amnestic AD and lvPPA. 39 Our findings also suggest a potential utility in the discrimination between PPA variants and the applicability to other languages and cultures outside Canada, with some minimal changes in a few items. The availability of DCQ in Spanish may be relevant because the screening tools specifically designed for the detection of typical and atypical dementias are scarce. 40 Furthermore, these types of tests do not usually evaluate behavior. However, further studies are necessary before implementing the Spanish DCQ in clinical practice, including normative data collection and validation in other causes of dementia and mild cognitive impairment.
We acknowledge some potential limitations. First, the sample size is relatively low. For this reason, our analysis primarily focused on the evaluation of the main scores of each test. Future studies with larger samples should examine the potential improvement of diagnostic capacity between PPA variants including the individual items, as has been recently shown using the ACE-III. 25 Secondly, even if the diagnosis of each PPA patient was clinically supported by a comprehensive language, cognitive, neuroimaging, and biomarkers assessment, and at least one year of follow-up, pathological confirmation was lacking.
It is essential to consider the clinical purpose of assessment tools and their role in providing timely and accurate diagnoses. Efficient and reliable diagnostic tools are key to minimize participant burden and facilitate effective clinical decision-making. Our study highlights the need for sensitive assessments that could be used as a first orientation for the diagnosis of PPA. Studies have pointed out that while highly sensitive assessments are valuable, they must also be feasible to use in routine practice to be effective.7,41,42 The three tools examined in this study balance between sensitivity and practicality, making them valuable additions to clinical practice.
In conclusion, our study confirms the validity of the MLSE, ACE-III, and DCQ for detecting PPA and classifying its variants, and highlights the absence of significant differences in their diagnostic abilities. These findings have important implications for clinical practice and can serve as a guide when deciding which tool to use. Furthermore, they support the consideration of language characteristics and other cognitive domains in the characterization and diagnosis of PPA variants. Future studies using longitudinal designs are warranted to evaluate the best tool for monitoring and follow-up of patients with PPA.
Additionally, our study adapted the DCQ to Spanish, a test developed specifically to assess atypical dementias. This novel tool is, like the ACE-III and MLSE, easily accessible and rapid to administer. Overall, our research contributes to the search of efficient and standardized neuropsychological tools that may be implemented in research and clinical practice.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241284199 - Supplemental material for Comparative accuracy of Mini-Linguistic State Examination, Addenbrooke's Cognitive Examination, and Depistage Cognitif de Quebec for the diagnosis of primary progressive aphasia
Supplemental material, sj-docx-1-alz-10.1177_13872877241284199 for Comparative accuracy of Mini-Linguistic State Examination, Addenbrooke's Cognitive Examination, and Depistage Cognitif de Quebec for the diagnosis of primary progressive aphasia by Lucía Fernández-Romero, Florentina Morello-García, Robert Laforce, Cristina Delgado-Alonso, Alfonso Delgado-Álvarez, María José Gil-Moreno, Monica Lavoie, Jorge Matias-Guiu, Fernando Cuetos and Jordi A. Matias-Guiu in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Lucia Fernandez-Romero (Data curation; Formal analysis; Investigation; Writing – original draft); Florentina Morello-Garcia (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Writing – original draft; Writing – review & editing); Robert Laforce Jr (Methodology; Writing – review & editing); Cristina Delgado-Alonso (Data curation; Investigation; Writing – review & editing); Alfonso Delgado-Alvarez (Formal analysis; Investigation; Methodology; Writing – review & editing); Maria José Gil-Moreno (Data curation; Investigation; Writing – review & editing); Monica Lavoie (Investigation; Methodology; Writing – review & editing); Jorge Matias-Guiu (Resources; Supervision; Writing – review & editing); Fernando Cuetos (Conceptualization; Methodology; Supervision; Writing – review & editing); Jordi A. Matias-Guiu (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Instituto de Salud Carlos III (PI22/00677). Florentina Morello García has received funding from the ‘Fundación Carolina’ (Spain) and the Education Ministry of Argentina through the Mobility Program for Argentine Faculty, as well as from the University of Buenos Aires (Argentina) through the UBAINT Teachers’ Scholarship to enable her stay at the Hospital Clínico San Carlos (Madrid, Spain) under the guidance of Dr Matias-Guiu. Jordi A. Matias-Guiu is supported by Instituto de Salud Carlos III through the project INT20/00079 and INT23/00017 (co-funded by European Regional Development Fund “A way to make Europe”).
Declaration of conflicting interests
Jordi A Matias-Guiu is an Associate Editor of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. The other authors have no conflict of interest to report.
Data availability
The dataset is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.