
Abstract
Background
The continuously increasing aging population and life expectancy have led to an inconsistent and underestimated dementia prevalence in China. An updated epidemiologic study is urgently needed.
Objective
To update the prevalence rate and risk factors of dementia in China.
Methods
For this national cross-sectional study, 20,438 participants aged ≥65 from 28 communities and 56 villages from 14 centers were recruited using a multistage cluster sampling design between May 2019 and December 2019. Participants were assessed with a series of clinical and neuropsychological measurements. The prevalence rates of dementia, Alzheimer's disease (AD), and vascular dementia (VaD), as well as the risk factors, were calculated using multivariate-adjusted models.
Results
The crude prevalence rates were 9.1% (95% CI, 8.7%–9.5%) for dementia, 6.0% (95% CI, 5.7%–6.3%) for AD, 1.4% (95% CI, 1.2%–1.5%) for VaD, and 1.8% (95% CI, 1.6%–2.0%) for other dementias in a population aged ≥65 years. The overall sex- and age-standardized prevalence was 8.8%. Apart from VaD, the prevalence rates of dementia and AD were higher in females than males (10.3% versus 7.7%, respectively). Moreover, the prevalence rates of dementia and AD increased significantly with age. Being unmarried and having fewer social activities increased the risks of dementia and main subtypes. Risk factors were not exactly the same for participants with AD and VaD.
Conclusions
The prevalence of dementia is increased and almost comparable with that of developed countries for individuals aged ≥65 years. These findings may serve as new evidence for government interventions in aging.
Introduction
Dementia is a global health challenge.1,2 China is facing a great challenge owing to its aging population and increased risk of dementia. Compared with the 2010 population census, the percentage of people aged ≥65 years old increased by 4.6 points. 3 It is estimated that more than 50 million people are living with dementia, and this figure will probably increase to 152 million by 2050, 4 with about 15.07 million patients with dementia in China. 5 In the coming decades, the global burden and annual global public issues will be priority events for health services, with disease prevention highlighted as a key strategy to reduce societal burden levels.6,7
Including the most representative research by Jia et al.8,9 and Zhang et al.,10,11 numerous epidemiological studies have been conducted in China in the last decade.8,12–16 The prevalence rates of dementia range from 2% to 13% for older individuals (i.e., ≥60 years or ≥65 years of age),17,18 with Alzheimer's disease (AD) and vascular dementia (VaD) being the most prevalent subtypes in the elderly population. 19 The burden of dementia seems to be increasing more quickly than is generally assumed by the international health community. 19 Chinese economic development and a rapidly aging population have meant dementia has become a major cause of disability, and a significant public health challenge. In the recent five years, few surveys were conducted to report the prevalence of dementia in China. The prevalence rates of 7.24% (95% confidential interval [CI]: 6.68%–7.80%) in the Hubei Memory & Aging Cohort Study, 20 and 7.62% in Xiamen City 21 in older adults were not much different from those of the previous results, possibly due to the limitations of sample size and being a single-center study. Moreover, these studies generally agree that factors such as older age, being female, having cerebrovascular disease, and obesity significantly increase the risk of dementia.8,9,20–22
Over 176 million (12.6% of the population) citizens aged ≥65 years in 2019 3 is closer to the population (190 million, 13.5% of the population) reported by the National Bureau of Statistics of China in 2021. 23 Given the continuously increasing proportion of the elderly population, as well as the life expectancy, the prevalence rate of dementia in China has been obviously underestimated, and the current health policy was based on the past prevalence rate of dementia that is likely to be inadequate. Due to the COVID-19 pandemic during the past three years, there has been no new epidemiological investigation of dementia. Most of the published data were conducted before 2019. Therefore, an updated epidemiologic study with a large multicenter sample representing the latest dementia status in China is needed urgently.
To update the prevalence rate and risk factors of dementia and provide new evidence for new health policy, we conducted a multicenter cross-sectional survey involving community-dwelling older adults, with a nationally representative sample of 20,438 adults aged 65 years or older.
Methods
Study design and samples
Our study was a population-based, cross-sectional survey conducted from May 2019 to December 2019. We used a multistage, stratified, and random sampling procedure, which considered geographical regions, economic development status, sex distribution and population sizes based on 2010 China census data.
In stage one, 31 representative regions were divided the into three regions according to economic level: east, middle, and west (the National Bureau of Statistics). The east section included Liaoning, Beijing, Tianjin, Hebei, Shandong, Jiangsu, Shanghai, Zhejiang, Fujian, Guangdong, and Hainan. The middle section included Heilongjiang, Jilin, Shanxi, Henan, Anhui, Hubei, Hunan, and Jiangxi. The west section included Xinjiang Uyghur Autonomous Region, Inner Mongolia Autonomous Region, Gansu, Qinghai, Ningxia Autonomous Region, Shanxi, Xizang Autonomous Region, Sichuan, Chongqing, Guizhou, Yunnan, and Guangxi.
In stage two, we randomly chose 14 provinces, metropolises, and autonomous areas that were representative of the socioeconomic status and lifestyles of the three regions, including six centers from the east (Beijing, Tianjin, Hebei, Shanghai, Fujian, and Hainan), four from the middle (Heilongjiang, Shanxi, Hubei, and Hunan), and four from the west (Xinjiang Uyghur Autonomous Region, Gansu, Chongqing, and Guizhou).
In stage three, we randomly selected 1 city (classified as urban) and 2 counties (classified as rural) from each of the 14 provinces, metropolises, and autonomous areas. In stage four, we randomly selected 2 districts from each city and 2 townships from each county.
In stage five, we randomly selected 1 community from each district and 1 village from each township. Finally, we randomly selected 28 communities and 56 villages from the 14 centers. All eligible individuals ≥65 years were chosen from each community or village.
To be eligible for the study, individuals had to be (1) living in target areas for at least one year before the survey commencement date; and (2) aged ≥65 years and listed in census documents. The following were excluded: individuals who refused to participate, were untraceable, had a life-threatening illness, were deceased, or had medical conditions such as inadequate hearing or vision. After a face-to-face questionnaire-based survey, a total of 20,438 participants completed this study.
The ethics committee of Tianjin Huanhu Hospital approved the study protocol (2019-40). Written informed consent was obtained from participants or their guardians.
Measures
Based on the experience of previous studies,5,16 we designed this face-to-face questionnaire-based survey that was conducted by study investigators/interviewers who were junior neurologists and senior neurology graduate students. The expert panel consisted of senior neurologists and neuropsychologists with expertise in cognitive impairment. All interviewers and experts received the same one-week training on collecting information (including basic social-demographic characteristics: sex, age, education, marriage, occupation, social activity, etc.; comorbidities: stroke, diabetes mellitus (DM), heart disease, and hypertension; lifestyles: smoking and alcohol consumption), neuropsychological assessments, and diagnosis and participated in a retraining course every two months. The inter-rater reliability for cognitive tests and diagnostic procedures was set at >0.90 that was maintained throughout the study.
Age was classified as 65–69, 70–74, 75–79, 80–84, and ≥85 years. Educational attainment was divided into three levels: <1, 1–6, and >6 years of education. The single, widowed, or divorced participants are described as “unmarried.” A smoker was defined as an individual with a history of smoking ≥5 cigarettes per day for >2 years. An alcohol drinker was defined as an individual with a history of drinking an alcoholic beverage ≥1 time per week for >2 years. Social activity was measured using a self-rated questionnaire referencing a cohort study that assessed the number and frequency of contact with relatives and friends. 24
Cross-sectional dementia survey
We conducted a two-stage prevalence dementia survey. In the first screening, each interviewer conducted individual, semi-structured interviews with participants and their guardians (carer/family member) at their residence. Interviews lasted approximately 1.5–2 h. Detailed information on sociodemographic characteristics, lifestyle, and medical history was collected. Lifestyle information was gathered, including smoking history; alcohol consumption; social activities; marital status; and medical history including hypertension, DM, heart disease, and stroke.
Standardized general and neurological examinations were also performed. Participants then completed a battery of neuropsychological tests administered by the interviewer. Cognition was assessed using the Mini-Mental State Examination (MMSE), 25 and social functioning was assessed using the Activities of Daily Living (ADL) test. 26 When MMSE test scores were less than or equal to the cutoff point (≤17 for illiterate individuals, ≤20 for those with 1–6 years of education, and ≤24 for individuals with ≥7 years of education), we performed a second screening survey including physical and neurological examinations, medical record review, and questionnaires on daily living activities. Trained staff collected all data according to standard protocols.
Dementia assessment and diagnosis
The diagnostic criteria for dementia were based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition. 27 The National Institute of Neurological and Communicative Disorders-AD and Related Disorders Association criteria were used for the clinical diagnosis of AD. 28 We also used the National Institute of Neurological Disorders and Stroke–Association Internationale pour la Recherche et l’Enseignementen Neurosciences for VaD. 29 Other dementias (ODs) defined by globally accepted criteria include mixed dementia, frontotemporal dementia, dementia with Lewy bodies, 30 Parkinson's disease dementia, alcoholic dementia, hydrocephalus dementia and posttraumatic dementia according to various globally accepted criteria.
The expert panel and interviewers reviewed all information; diagnoses were made at the end of each working day. If consensus was not reached, an expert returned to the residence to re-examine and re-evaluate the participant for a final diagnosis.
Statistical analysis
Participant demographic characteristics were described as the mean ± standard deviation (SD) for continuous variables, and prevalence rates of dementia and main subtypes were estimated for the entire study population, as well as according to sex, age, education, location, marital status, social activity, and comorbidity subgroups. Age- and sex-standardized prevalence (odd ratios [ORs] with 95% CI) rates were calculated based on the population distribution of China in 2010.
We calculated descriptive statistics for continuous variables; Student's t test was used for continuous variables consistent with a normal distribution, with a nonparametric test for non-normal applications. The chi-square and Mann-Whitney U tests were used to assess the clinical factors associated with the presence of dementia. A multivariate logistic regression analysis examined the demographic factors and comorbidities associated with dementia. A p-value <0.05 was considered significant. All statistical analyses were conducted using IBM SPSS Statistics for Windows (Version 25.0; IBM Corp., Armonk, NY, US).
Results
Sample population characteristics
We sampled 20,438 individuals from 14 centers: 8969 males and 11,469 females. Of the 20,438 individuals, 8472 were from the east, 6347 were from the middle, and 5619 were from the west of China. The response rate was 82%. Sample population characteristics are presented in Table 1. Women accounted for 56.1% of the sample, consistent with the sex distribution of the entire population. The mean age was 73.8 ± 6.3 years, and approximately 60.2% of the sample were 65–74 years old. Among participants, 44.1% were from urban areas and 55.9% from rural areas. Women accounted for 63.2% of the dementia group and 55.4% of the non-dementia group. Dementia was more common among participants aged ≥80 years (p < 0.001); with poorer education (p < 0.001); in rural areas (p < 0.001); being single, divorced or widowed (p < 0.001); and with less social activity (p < 0.001) than that of the participants without dementia. Apart from stroke (16.3% versus 11.2%, respectively; p < 0.001), we found no significant differences between the dementia group and non-dementia group with respect to hypertension, DM, and heart disease.
General characteristics of our sample.

The p-value was calculated by comparing the proportions between the participants with dementia and without.
Prevalence rates of dementia and main subtypes
Overall, the crude prevalence rates of dementia, AD, VaD, and ODs among people aged 65 years and older were 9.1% (95% CI, 8.7%–9.5%), 6.0% (95% CI, 5.7%–6.3%), 1.4% (95% CI, 1.2%–1.5%), and 1.8% (95% CI, 1.6%–2.0%), respectively. The overall sex- and age-standardized dementia prevalence was 8.8%. The crude prevalence rates for subgroups stratified by sex, age, education, location, marital status, and social activity are also presented in Table 2. The prevalence rates were 6.6% (95% CI, 6.2%–7.1%) for AD, 1.4% (95% CI, 1.2%–1.6%) for VaD, and 2.3% (95% CI, 2.0%–2.5%) for ODs in females. The corresponding figures for males were 5.1% (95% CI, 4.7%–5.6%), 1.4% (95% CI, 1.1%–1.6%), and 1.1% (95% CI, 0.9%–1.4%), respectively.
Prevalence (with 95% CI) of dementia and main subtypes by socio-demographic characteristics.
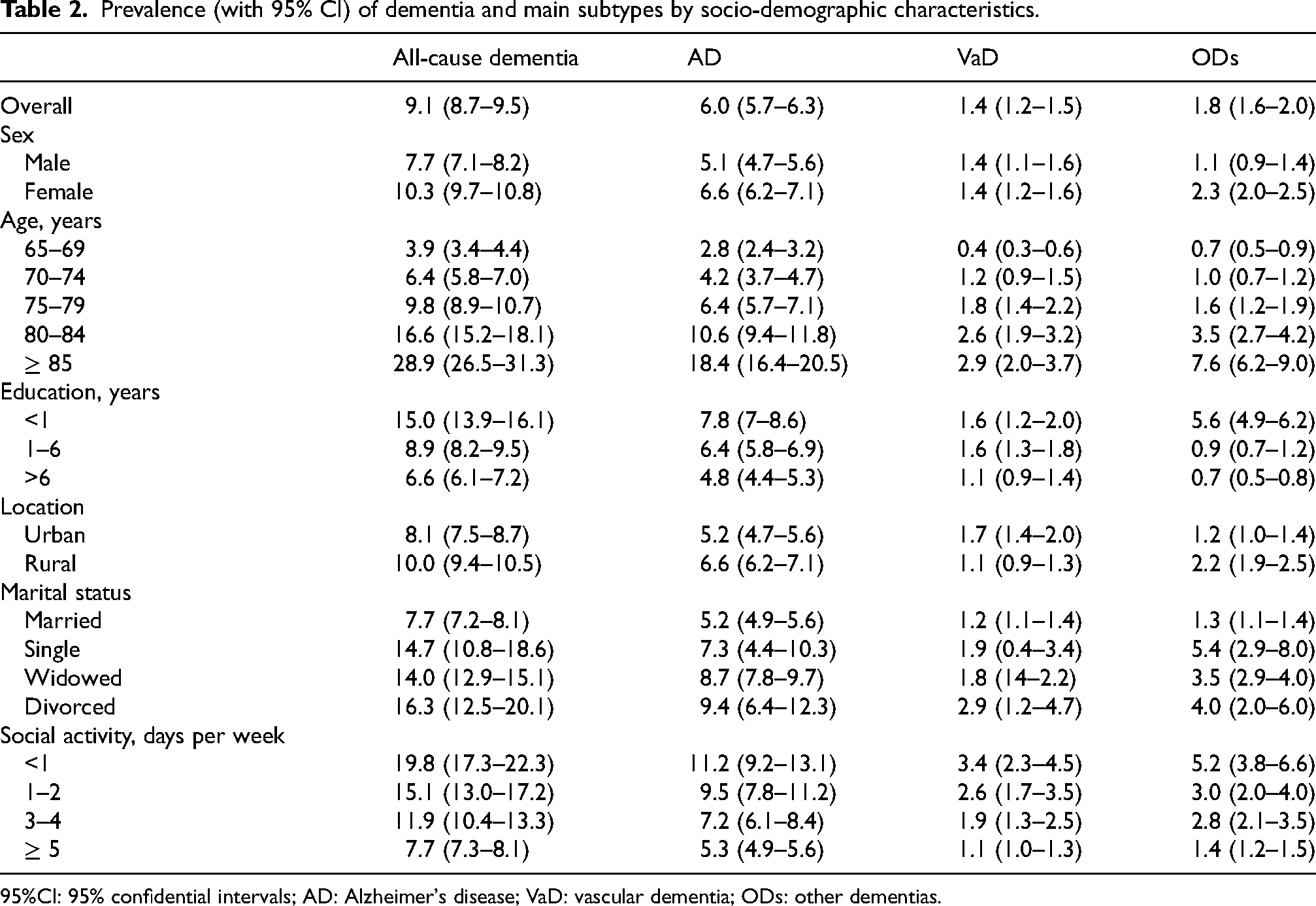
95%CI: 95% confidential intervals; AD: Alzheimer's disease; VaD: vascular dementia; ODs: other dementias.
Among individuals with dementia, the proportion of AD was 65.5%; AD was the most common type of dementia. The changing patterns as stratified by sex and other sociodemographic variables are shown in Figures 1 and 2. The prevalence rates of dementia increased significantly with age in both sexes, but the rate increased more rapidly in females than males from 4.4% (95% CI, 3.7%–5.1%) to 36.9% (95% CI, 33.3%–40.4%), respectively. This trend was also seen for AD, VaD, and ODs, but no significant difference in the prevalence of VaD was demonstrated by sex (Figure 1(c)). The prevalence of ODs demonstrated a significant but weak age trend for those younger than 80 years of age and a significantly sharp trend after 80 years of age (Figure 1(d)). Dementia prevalence increased with age in both sexes, while it decreased with higher education levels in both. Educational effects on dementia were observed more in females with >6 years of education (Figure 2).

Prevalence rates (with 95% CI) of dementia and main subtypes by sex and age categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and age categories, respectively. 95%CI: 95% confidential intervals.
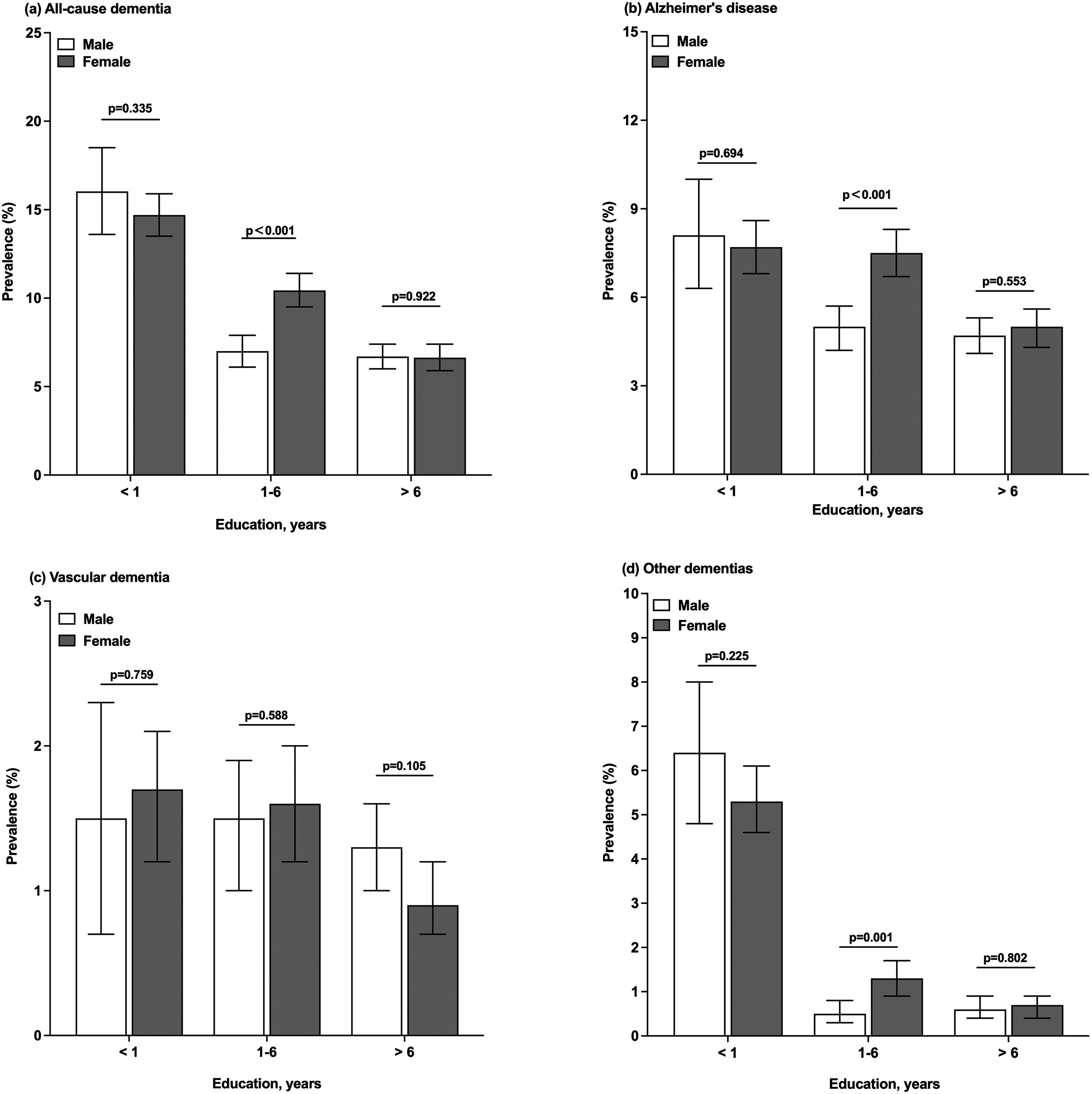
Prevalence rates (with 95% CI) of dementia and main subtypes by sex and education categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and education categories, respectively. 95%CI: 95% confidential intervals.
As shown in Figures 3–6, the prevalence rates of dementia stratified by sex and other sociodemographic variables were higher in females than males and demonstrated a decrease, along with the increasing frequency of social activity (Figure 3). Dementia prevalence was 7.7% (95% CI, 7.2%–8.1%) in the married group but was significantly higher in unmarried groups, including single, divorced, or widowed males and females (Figure 4). Females in rural areas had a substantially higher prevalence of dementia than males or females in urban areas, whereas levels were comparable for females living in both areas (Figure 5). The prevalence of dementia and AD was higher in divorced males, and VaD was more prevalent in urban or west-region males (Figure 6).
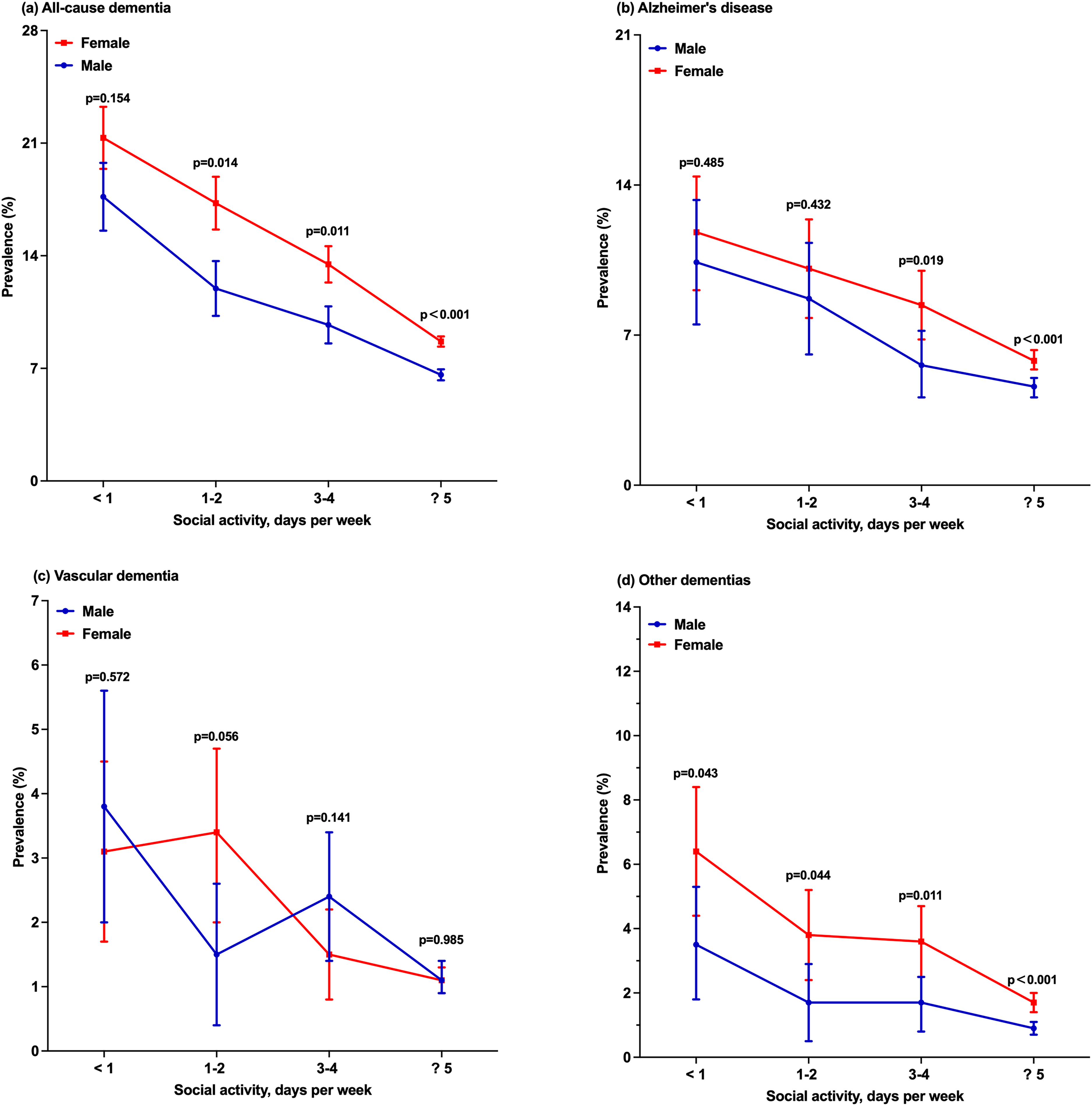
Prevalence rates (with 95% CI) of dementia and main subtypes by sex and social activity categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and social activity categories, respectively. 95%CI: 95% confidential intervals.
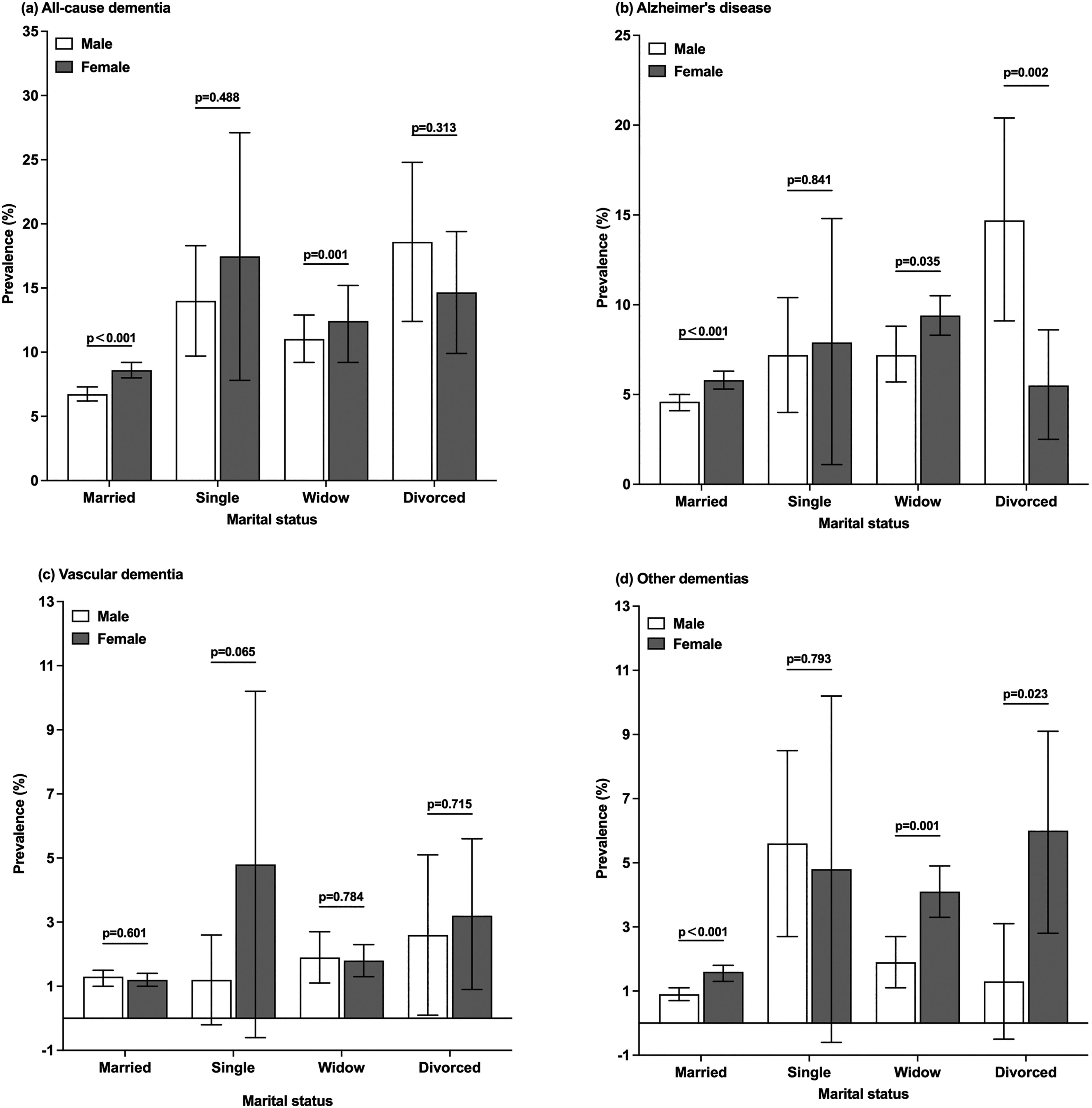
Prevalence rates (with 95% CI) of dementia and main subtypes by sex and marital status categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and marital status categories, respectively. 95%CI: 95% confidential intervals.
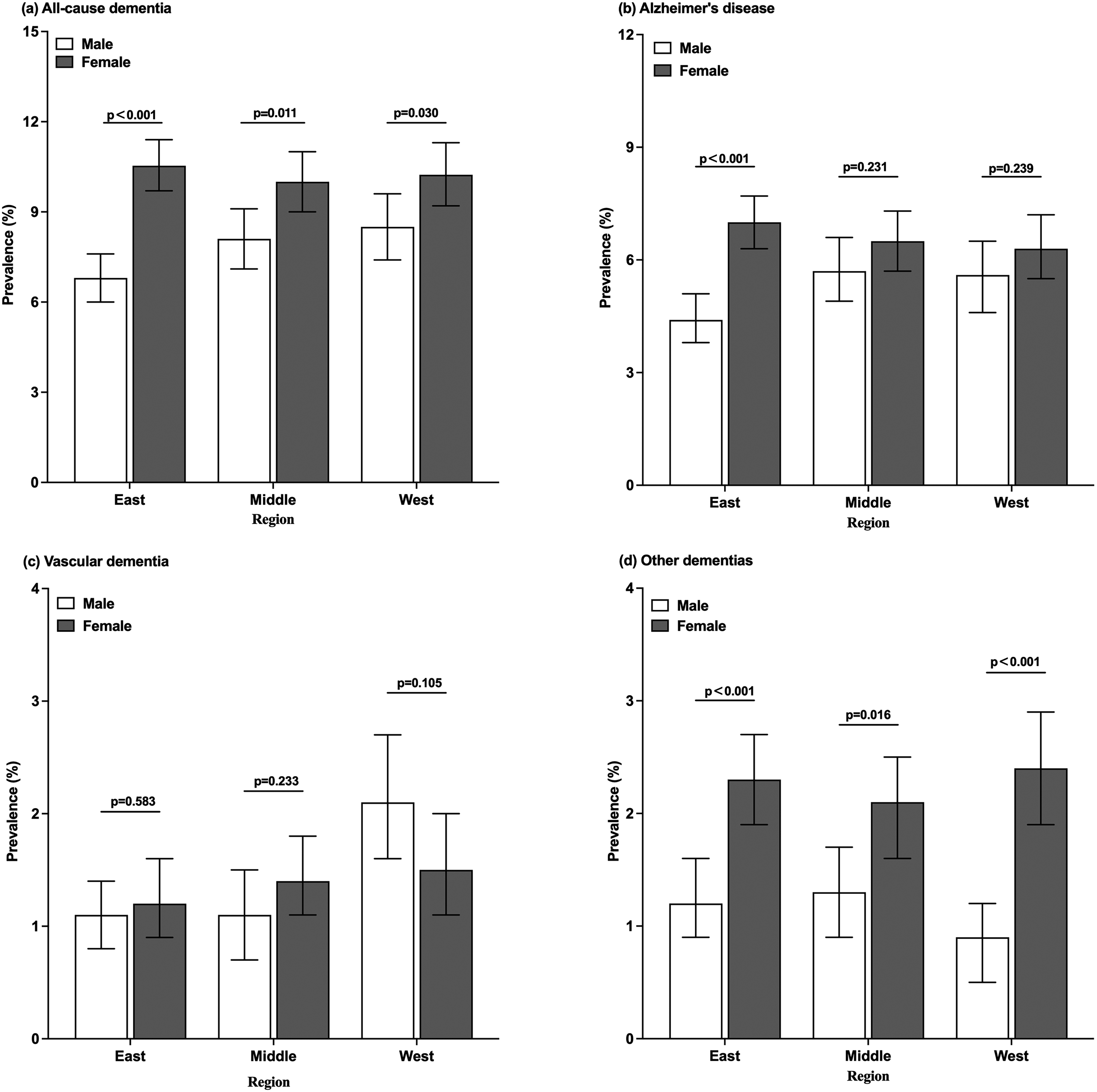
Prevalence rates (with 95% CI) of dementia and main subtypes by sex and region categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and region categories. 95%CI: 95% confidential intervals.
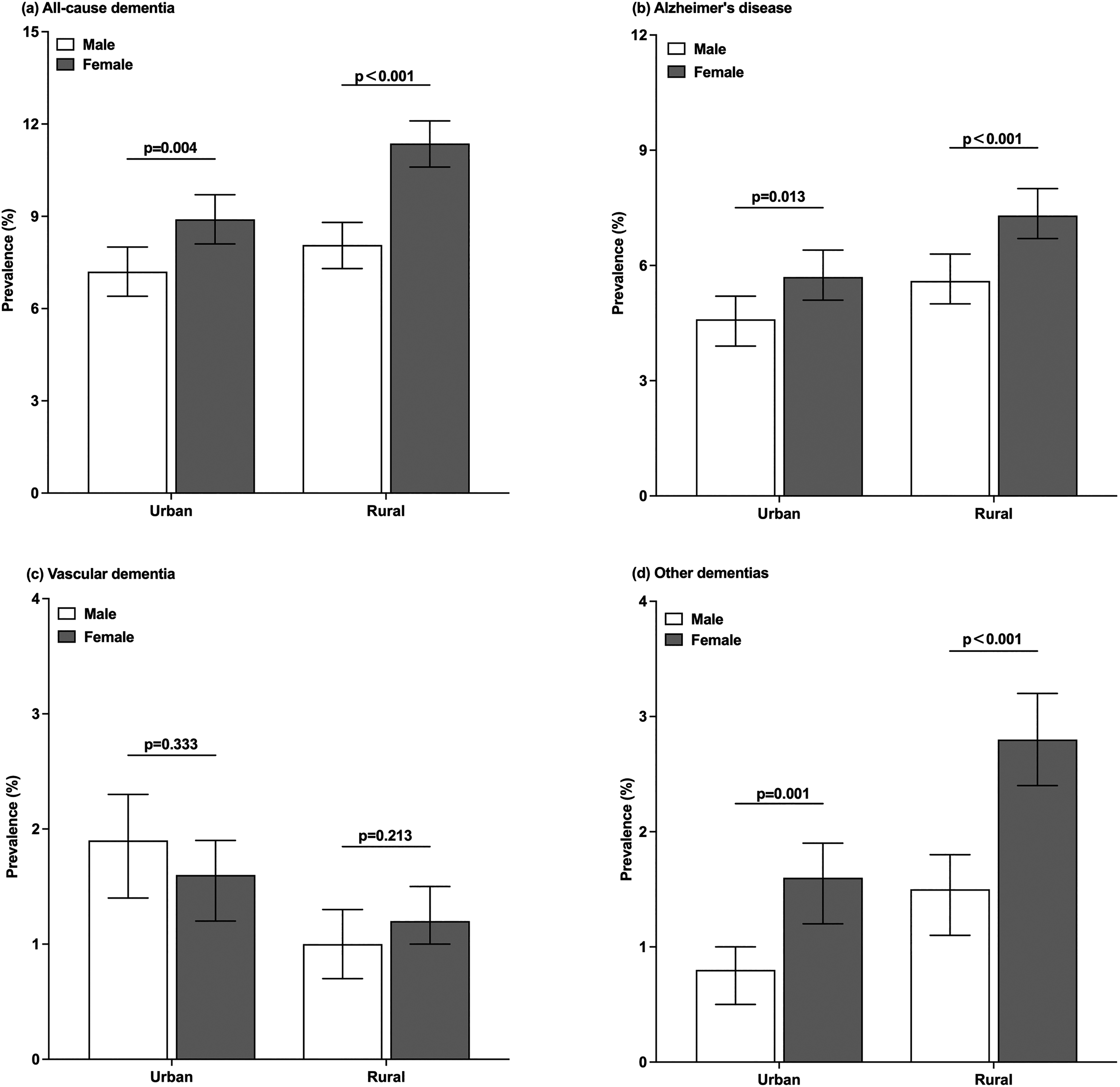
Prevalence rates (with 95% CI) of dementia and main subtypes by sex and location categories. Prevalence rates for dementia (a), Alzheimer's disease (b), Vascular dementia (c), and other dementias (d) by sex and location categories, respectively. 95%CI: 95% confidential intervals.
Multivariate risk factors assessment
Using multivariate logistic regression analysis, models based on the whole sample, including participants with dementia (AD, VaD, and ODs) and individuals without dementia, were arranged to identify possible risk factors for dementia (Table 3). We found that being female, an older age, and having less education were common risk factors for dementia. Meanwhile, rural living (p < 0.001), being unmarried (p < 0.001), lower frequency of social activities (p < 0.001), and stroke (p < 0.001) were all significantly associated with higher risks of dementia. Compared with participants having social activity ≥5 days per week, a lower frequency of social activities significantly increased the risks for AD (<1 day per week: OR, 2.44; 95% CI, 1.98–3.01, p < 0.001; 1–2 days per week: OR, 1.97; 95% CI, 1.60–2.43, p < 0.001; and 3–4 days per week: OR, 1.44; 95% CI, 1.20–1.73, P < 0.001), VaD (<1 day per week: OR, 3.50; 95% CI, 2.41–5.09, p < 0.001; 1–2 days per week: OR, 2.56; 95% CI, 1.73–3.78, p < 0.001; and 3–4 days per week: OR, 1.75; 95% CI, 1.23–2.51, p = 0.002), and ODs (<1 days per week: OR, 4.41; 95% CI, 3.23–6.02, p < 0.001; 1–2 days per week: OR, 2.39; 95% CI, 1.65–3.44, p < 0.001; and 3–4 days per week: OR, 2.15; 95% CI, 1.59–2.90, p < 0.001). Apart from the abovementioned, the risks for VaD were greater among participants with hypertension (OR, 4.38; 95% CI, 3.26–5.89, p < 0.001), DM (OR, 10.69; 95% CI, 8.35–13.68, p < 0.001), heart disease (OR, 2.97; 95% CI, 2.31–3.83, P < 0.001), stroke (OR, 10.16; 95% CI, 8.00–12.91, p = 0.017), habitual alcohol consumption (OR, 1.70; 95% CI, 1.32–2.19, p = 0.001), and smoking (OR, 1.51; 95% CI, 1.18–1.93, p = 0.001).
Logistic regression models for all-cause dementia and main subtypes.
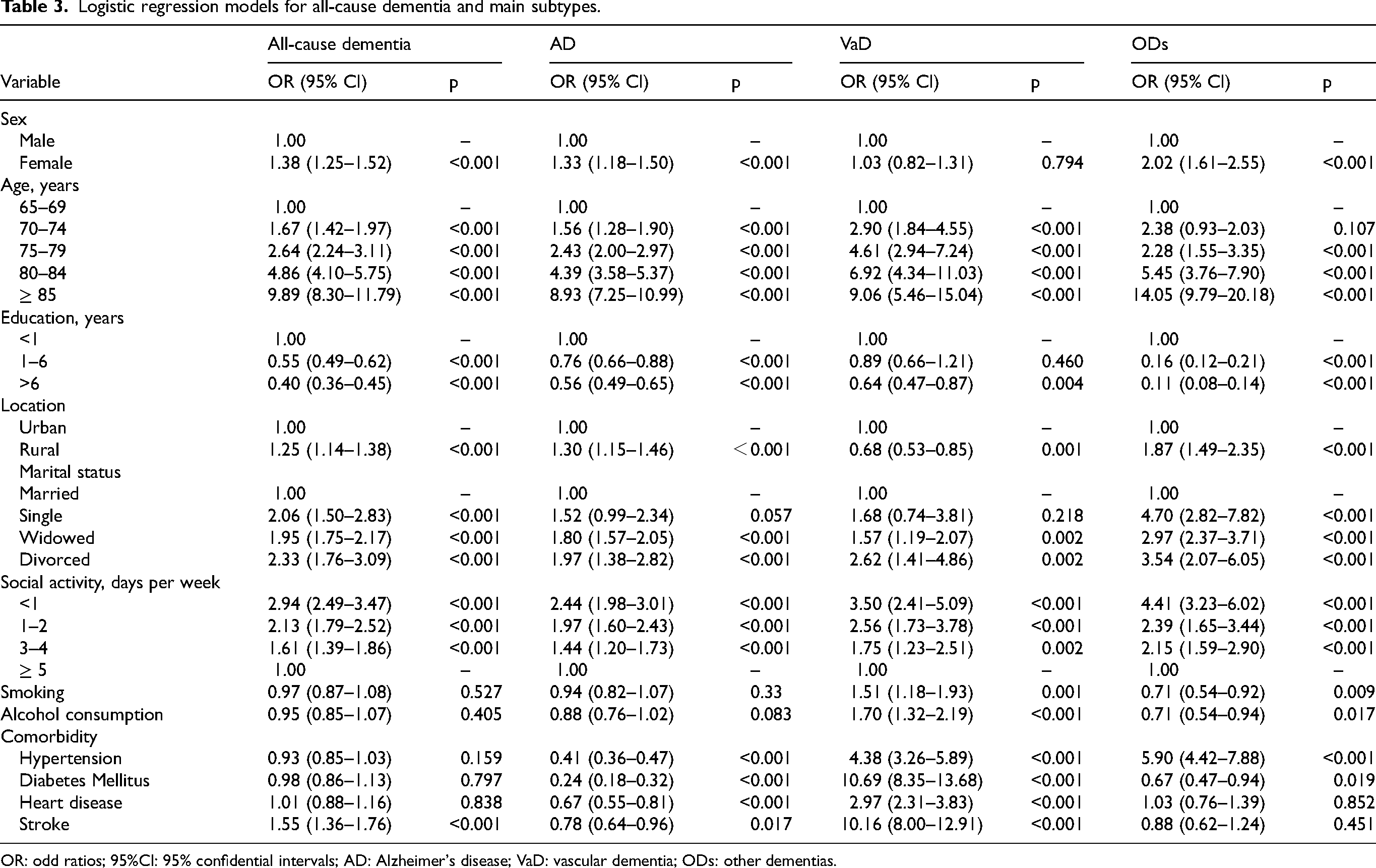
OR: odd ratios; 95%CI: 95% confidential intervals; AD: Alzheimer's disease; VaD: vascular dementia; ODs: other dementias.
Discussion
This national, multicenter, and population-based study in an elderly Chinese sample suggested dementia has become a major public health issue in China. Our study showed that the overall crude dementia prevalence in our sample was 9.1%. The overall sex- and age-standardized dementia prevalence was 8.8%. After stratification by sex, age, education, location, marital status, and social activity, the prevalence was higher in females in rural areas, increasing significantly with increasing age but decreasing with increased education levels. Unmarried and less socially active individuals had a higher dementia prevalence. In addition to being female, having an older age, living rurally, having lower education levels, and having a history of stroke as risk factors for dementia in a Chinese population, marital status and social activity were probably risk factors. These data suggest that dementia prevalence was higher than in previous years and emphasized the condition as a public health issue in China.
Our study was the first nationwide revaluation specific for the prevalence of dementia in individuals aged ≥65 years in China in the past decade. We investigated three major geographical areas (east, middle, and west China), including nine provinces, four municipalities, and one autonomous region. Thus, our study was more geographically and epidemiologically representative than that of previous studies, e.g., which covered one city or area.31–34 The 1997 study by Zhang et al. included four cities, 10 and a study by Jia et al. included five cities, with 10276 residents. 8 However, a more recent study between 2013 and 2015 was the first nationwide survey of mental disorders in China that explored dementia prevalence. 12
The global dementia prevalence is estimated at 5%–7% in those aged ≥60 years and varies between countries and changes with time.7,35 Our data indicated that the dementia prevalence in Chinese individuals aged ≥65 years was 9.1%, comparable with global statistics and higher than that of previous figures. Zhang et al. observed that the dementia prevalence was 5% in elderly individuals aged ≥65 years. 36 Another study by Jia et al. focused on a relatively bigger population and reported that the dementia prevalence was 5.14% in elderly individuals aged ≥65 years. 8 Another study conducted between 2013 and 2015 reported that the dementia prevalence was 5.6% in people aged ≥65 years. 12 A recently published study reported that the age- and sex-adjusted prevalence was approximately 6.0% in adults aged ≥60 years. 9 Our data indicated a higher prevalence that was probably actually increased. 9 The most probable reason is that China's population is rapidly aging and accelerating and will do so in the decades to come. Other reasons include an increased life expectancy and dramatic lifestyle changes. Trends in the dementia prevalence are also equivocal depending on global geography. 7 Relatively stable or decreasing trends have been reported in several countries including the US, UK, Sweden, Spain, and the Netherlands,37–39 whereas an increasing prevalence has been recorded in Canada and Japan.7, 40
The factors affecting dementia occurrence have also been reported in previous studies.8,9 Ours and others have shown that age is the strongest risk factor for the disease, and similarly, being female is also an independent risk factor.41–43 In addition, having a limited education is also a risk factor, consistent with previous studies. 7 Studies have also shown that higher education levels may maintain cognitive function and even delay dementia onset. 44 A history of stroke was also an independent risk factor as it was related to vascular dementia.45,46 Living in rural areas probably increases dementia risk that is consistent with a previous study. 8 Smoking was also a risk factor as it is a risk factor for cerebral vascular disease, whereas the OR was close to 1. Apart from these observations, we also observed that being unmarried and fewer social activities were risk factors in elderly individuals. Previous studies demonstrated the beneficial effects of social contacts for dementia risk reduction.47,48 A recent study indicated that all unmarried groups including cohabiting, divorced/separated, widowed, and being single had significantly higher odds of developing dementia than their married counterparts. For divorced/separated and widowed participants, the differences in the odds of dementia relative to married respondents were greater in men than women. 49 Evidence has also suggested that being married may prevent progression from mild cognitive impairment to dementia. 50
Although there have been many epidemiological studies on dementia in the past, the current study comprises the most recent data and a relatively large sample size in an elderly Chinese population in the past five years. While a limitation of this study is that it was designed and conducted with only classical risk factors based on previous research experience, the potential effects of sarcopenia, 51 the environmental factors52–54 (including exposure to air pollution, heavy metals, metalloids and residential green space), and other novel factors 55 on dementia proposed in recent studies were not included. Future studies focused on more potential risk factors to evaluate their association more specifically and objectively with dementia are warranted. We will investigate the prevalence of dementia subtypes and explore the reasons and mechanisms for the increasing prevalence of dementia. Further research into the effect of social activities and marital status on dementia will be conducted.
In conclusion, we observed that the prevalence rate of dementia in China has significantly increased and is now similar to that of other developed countries, such as the USA and Italy.56–59 Moreover, the prevalence rates of dementia, AD, and VaD were significantly higher in females. In addition to the probable risk factors of being older, being female, rural living, having a lower education, and having a history of stroke, being unmarried and having fewer social activities could increase the risk for dementia. These findings will help health policymakers and practitioners identify vulnerable subpopulations and design effective intervention strategies to reduce dementia risk. We call on the government to intervene early in aging, increase publicity on dementia-related knowledge, and cultivate a healthy lifestyle. In addition, it is necessary to increase investment in early dementia screening, further promote community-based early screening and management, and form a direct referral model with tertiary hospitals to facilitate the diagnosis and treatment of patients in the early stage of dementia to reduce the incidence of dementia.
Footnotes
Acknowledgments
The authors thank the neurologists and neuropsychological scale evaluators who coordinated data collection from all centers, as well as the Tianjin Key Medical Discipline (Specialty) Construction Project for their help. All these authors accept responsibility for all aspects of the manuscript and approved the final version of the manuscript.
Author contributions
Jinghuan Gan (Formal analysis; Investigation; Writing – original draft; Writing – review & editing); Yan Zeng (Conceptualization; Investigation; Methodology; Resources; Writing – review & editing); Guowei Huang (Conceptualization; Formal analysis; Investigation; Methodology; Resources; Writing – review & editing); Xiao-Dan Wang (Investigation; Software; Supervision; Validation); Yang Lü (Investigation; Resources; Visualization); Jianping Niu (Investigation; Resources; Visualization); Xinling Meng (Investigation; Resources; Validation); Pan Cai, MD (Investigation; Resources); Xia Li (Investigation; Resources); Yang Li (Investigation; Resources); Lu Shen (Investigation; Resources); Yong You (Investigation; Resources); Baozhi Gang (Investigation; Resources); Yanqing Tang (Investigation; Resources); Yan Lv (Investigation); Zhihong Ren (Investigation); Shuai Liu (Data curation; Investigation; Software; Writing – original draft); Yong Ji (Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Writing – review & editing)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [grant number 82171182], Beijing Friendship Hospital, Capital Medical University (No. YYZZ202309), Tianjin Science and Technology Plan Project [grant number 22ZYCGSY00840], Tianjin Health Research Project [grant numbers ZC20121, TJWJ2023QN060 and TJWJ2022MS032], Tianjin Municipal Education Commission Research projects [grant number 2023KJ060], and Tianjin Key Medical Discipline (Specialty) Construction Project [grant number TJYXZDXK-052B]. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of conflicting interests
Dr Yong Ji is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.