
Abstract
Background
The growing burden of dementia and Alzheimer's disease may be mitigated by a combination of primary and secondary preventive strategies, including lifestyle interventions and targeted disease-modifying therapy at the individual-level.
Objective
Our aim is to estimate the effects of primary and secondary prevention on a population level in terms of life years lived with and without dementia.
Methods
We used the previously developed and validated microsimulation model MISCAN-Dementia, modified to evaluate the impact of individual-level primary and secondary preventative interventions in the Dutch population aged 55 years and older, between 2025 and 2050. We expanded this model with prevention-specific effectiveness and eligibility, based on observed trial effects (primary analysis) and assuming a range of combinations of eligibility and effects (secondary analyses).
Results
Extrapolating results from available randomized controlled trials, combined primary and secondary preventative interventions result in a 6.1% decrease of life years lived with moderate to severe dementia until 2050, compared to no additional prevention. Dementia-free life years increased by 3.1%. The magnitude of risk reduction was the primary driver of impact, with the most optimistic assumptions resulting in a stabilization of dementia prevalence by 2050.
Conclusions
A combination of primary and secondary preventative strategies likely is needed to achieve optimal effects on the future burden of dementia. These approaches differ in the time needed to achieve maximal population-level impact, with the overall magnitude of effect primarily determined by the size of the intervention's impact.
Introduction
The WHO recognizes dementia as a rapidly growing public health challenge and has made it a public health priority.1,2 In 2023, over 55 million people were living with dementia worldwide, 3 which is forecasted to increase to 152 million people in 2050 due to aging. 4 In the Netherlands it is expected that dementia prevalence will increase by 43% from 2020 to 2050 without new interventions, provided favorable trends in age-specific dementia incidence prevail. 5 This expected increase shows the need for intervention strategies to reduce the number of people living with (advanced stages of) dementia. There are currently no curative treatments available for dementia of any type.
With respect to dementia, prevention can occur at different points throughout the disease process. Interventions that delay the onset of cognitive impairment are part of primary prevention, whereas interventions that slow the progression of disease after onset of early symptoms are part of secondary prevention. In the last decade, several trials on primary dementia prevention have been concluded. Of the 17 trials investigating multidomain lifestyle interventions, 6 13 focused on improving physical activity, nutrition, and cognition, and are sometimes supplemented with other lifestyle factors. Results show statistically significant slowing of cognitive decline on a cognitive composite score in some, but not all trials. Often, these trials focus on intermediate cardiovascular outcomes and cognition, and not on dementia diagnosis. Follow-up in these trials ranged from 2 weeks to 6 years, which in general is too short to show an effect on dementia. Regarding secondary prevention among patients with mild cognitive impairment, two amyloid-targeting therapies are available in the United States and several other countries: lecanemab and donanemab.7–9 These therapies target amyloid-β plaques in order to slow Alzheimer's disease progression. The effects of these drugs were expressed as changes in cognitive and functional abilities. 10 Despite statistically significant differences in cognitive decline between active treatment and placebo groups, absolute risk reductions were modest at best during the 18-month follow-up. 11
Empirical data on the long-term impact of these individual-level primary and secondary prevention interventions on the population dementia burden is lacking. Such knowledge is urgently needed to support policy choices on dementia prevention. Because optimal prevention strategies may well require a combination of primary and secondary prevention, it is important to evaluate their combined effect, but no published studies have evaluated combined intervention strategies before. The aim of this study is to estimate the effects of primary and secondary prevention on a population level in terms of life years lived with and without dementia. We do this by using the previously developed and validated MISCAN-Dementia microsimulation model. 5 Furthermore, we explore under which circumstances combined primary and secondary prevention interventions can stabilize the prevalence of dementia over time, which would represent a considerable reduction in the dementia burden compared to current projection.
Methods
This analysis was conducted using the MISCAN-Dementia microsimulation model, which is based on the validated Microsimulation Screening Analysis (MISCAN) model. First, we describe the previously developed MISCAN-Dementia model for which details have been published elsewhere.5,12 Second, the addition of new model features to allow the reflection of primary and secondary prevention interventions are described.
MISCAN-Dementia model description
We simulated the life courses of 15 million people born between 1910–1989 according to Dutch life tables. We reflected the situation with current usual dementia care (i.e., without dementia-specific prevention) and compared three alternative prevention strategies: a strategy reflecting primary dementia prevention, a strategy reflecting secondary dementia prevention, and a strategy applying both primary and secondary prevention. From this, we model an elderly population (≥65 years of age) from 2025 until 2050.
The model simulates the unidirectional transitions between disease stages: normal (normal cognition without neurodegenerative pathology or cognitive symptoms), presymptomatic neurodegenerative disease (pathological changes in the brain that may develop into any form of dementia, but did not yet result in cognitive symptoms), mild cognitive impairment, mild dementia, moderate dementia, and severe dementia, followed by death due to dementia (Figure 1). MISCAN-Dementia is a time-to-event model, so transition timing is determined by stage duration. 5 Individuals at any stage may die from other causes, based on death rate by sex and age in years from birth cohort specific life tables. The increased mortality of individuals with dementia is implicitly accounted for by the duration from severe dementia to death before reaching death from other causes. The model was calibrated using age- and sex-specific dementia incidence data from the Rotterdam Study, an ongoing population-based cohort study of 17,931 individuals over the age of 40 who live in the Ommoord suburb of Rotterdam, the Netherlands. 13 Based on a recent meta-analysis of North American and European cohorts, we assumed a linear decline in the age-specific dementia incidence of 13% per decade for the birth cohorts for which trend data is available (1910 to 1940) and stable age-specific incidence for subsequent birth cohorts (1950 to 1980).
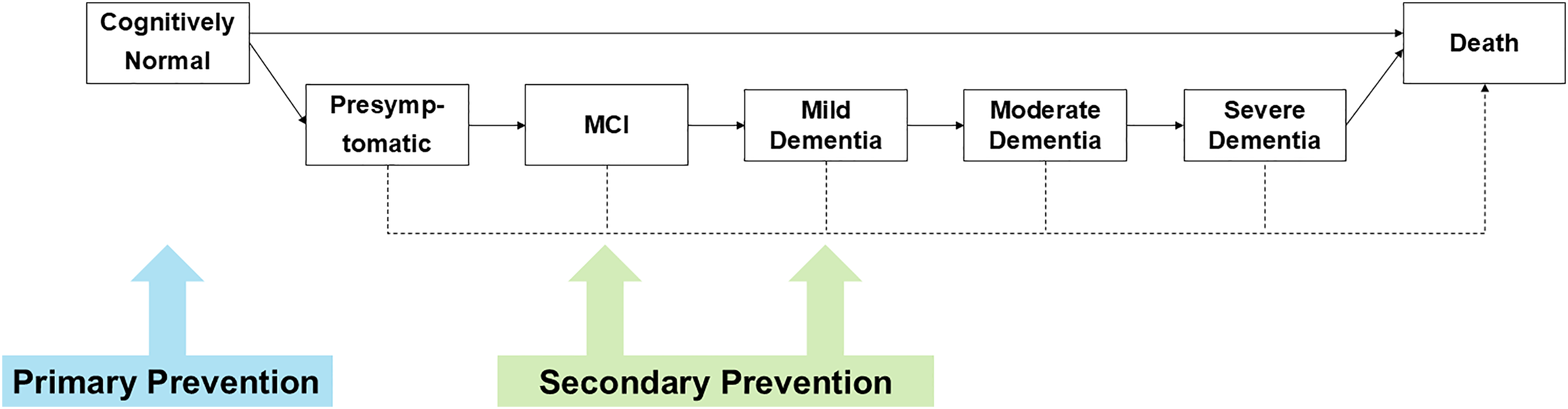
MISCAN-dementia structure with severity stages and prevention interventions.
Addition of new model features
We implemented primary and secondary prevention by first introducing a presymptomatic stage as part of the existing MCI and dementia disease progression in MISCAN-Dementia and then adding features of primary prevention (e.g., responsive to dementia lifestyle or blood pressure lowering intervention) and secondary prevention (e.g., eligible and responsive to amyloid-targeting treatment in early Alzheimer's disease). As the clinical trials of amyloid-targeting medication included patients with MCI and early stage (mild) dementia due to Alzheimer's disease, we considered individuals with current mild dementia due to Alzheimer's disease eligible for the “secondary preventative” intervention at baseline, with subsequent secondary prevention over time applying only to individuals newly developing MCI due to Alzheimer's disease, at time of entering the MCI stage. Responsiveness to risk factor modification and amyloid altering medication eligibility are assumed to be independent of one another.
A presymptomatic stage was added to this version of MISCAN-Dementia and represents the time when a person exhibits brain pathology, such as amyloid-β or cerebral small vessel disease, but no cognitive impairment. This presymptomatic stage duration was obtained from an estimate of this stage by Vermunt et al. based on persons with at least one abnormal marker of amyloid accumulation or a clinical Alzheimer's disease dementia diagnosis. 14 The duration was pragmatically implemented as a triangular distribution, with a lower limit of 7 years, a mode of 10 years, and an upper limit of 11.5 years.
Implementation of primary prevention
We define primary prevention as any individual-level prevention measure aimed at reducing dementia risk before MCI onset. We implemented this as a delay in the onset of the presymptomatic dementia stage and, consequentially, the MCI stage. As a notable example of primary dementia prevention, we calibrated the change in dementia progression to the odds ratio of cognitive decline from the FINGER trial, 15 which resulted in a 1.6 year delay of the presymptomatic stage. We assumed primary prevention is effective if people have not entered the presymptomatic dementia stage and the dementia is responsive to lifestyle or cardiovascular risk factor interventions. However, we relaxed this assumption and extended the effectiveness of primary prevention into the presymptomatic stage to be able to calibrate to the odds ratio from the FINGER trial, and because these interventions likely still modify disease risk in the presence of some subclinical pathology. Risk factor intervention responsiveness is assigned at random based on the fraction of risk factor attributable dementias of 0.40 based on the Lancet Commission report. 16 In addition to dementia risk, lifestyle and cardiovascular risk factors also influence life expectancy through other pathways. The average life expectancy increase if a person eliminates one of their risk factors was calculated based on obesity, hypertension, smoking and alcohol consumption and the model parameter was set to a 1 year shift in other cause death.17,18 This life expectancy increase was applied to every individual that received primary prevention, regardless of the result on dementia delay.
Implementation of secondary prevention
Secondary prevention was defined as pharmacological intervention aimed at slowing disease progression, starting in the MCI stage. Examples of such intervention are anti-amyloid therapies lecanemab and donanemab against early Alzheimer's disease. As the clinical trials of amyloid-targeting medication included patients with MCI and early stage (mild) dementia due to Alzheimer's disease. We considered individuals with current mild dementia eligible for the “secondary preventative” intervention at baseline, with subsequent secondary prevention over time applying only to individuals newly developing MCI, at time of entering the MCI stage. The effect size of secondary prevention is expressed in the model as a multiplication factor for the duration of MCI and mild dementia stages. The average time spent in dementia in our model is approximately 8 years. Analysis from the TRAILBLAZER-ALZ 2 clinical trial for Donanemab estimates the delay of moderate dementia as 7.53 months. 7 Another modelling study, assuming increasing long-term effects, estimates that adding anti-amyloid therapies to the standard of care adds 1.95 years to the time to reach moderate dementia. 19 Our model produced these estimations when a multiplication factor of 1.08 to 1.24 was applied. Considering the uncertainty around the effect size estimation, we decided to set the base case multiplication factor to 1.10, giving more weight to the clinical trial.
According to current diagnostic classification guidelines, targeted therapies for the prevention of Alzheimer's disease in those with MCI and mild dementia require confirmed amyloid accumulation in the brain. 20 Consequently, the fraction of persons with MCI or dementia eligible for anti-amyloid therapies was calculated by multiplying the proportion of cases with the diagnosis of clinical Alzheimer's disease in the Netherlands (65%) and the fraction of patients with Alzheimer's disease indeed displaying amyloid-positive biomarkers (79–87%) resulting in a final model parameter of 0.60.21,22
Base case analysis
Effect sizes taken from trial results (both primary and secondary preventative interventions) were obtained from intention to treat analysis and reflect the adherence levels in the trial, which were assumed to hold up throughout the lifetime.
We have summarized the above-described base case characteristics of the primary and secondary prevention in Table 1. A more complete summary of model inputs and assumptions can be found in Supplemental Table 1. Both primary and secondary prevention interventions are initiated in 2025. We compared the life years lived with and without dementia for primary and/or secondary prevention. For a subset of analyses, we chose to focus on moderate and severe dementia, as these stages represent the largest burden.
Summary of new model parameters.
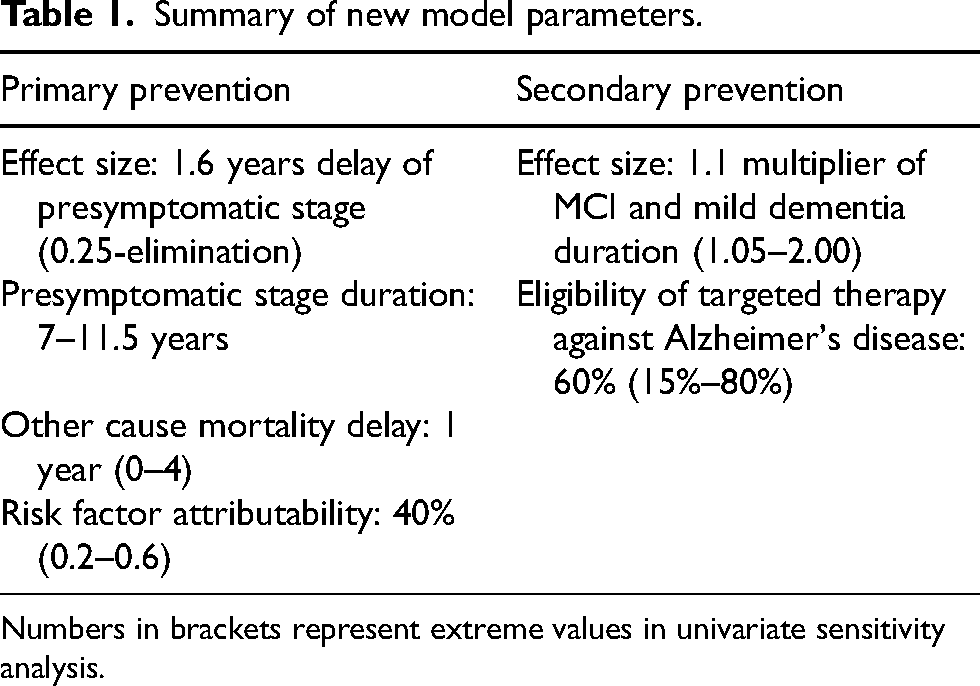
Numbers in brackets represent extreme values in univariate sensitivity analysis.
Life years in 2050 in thousands for different prevention scenarios.
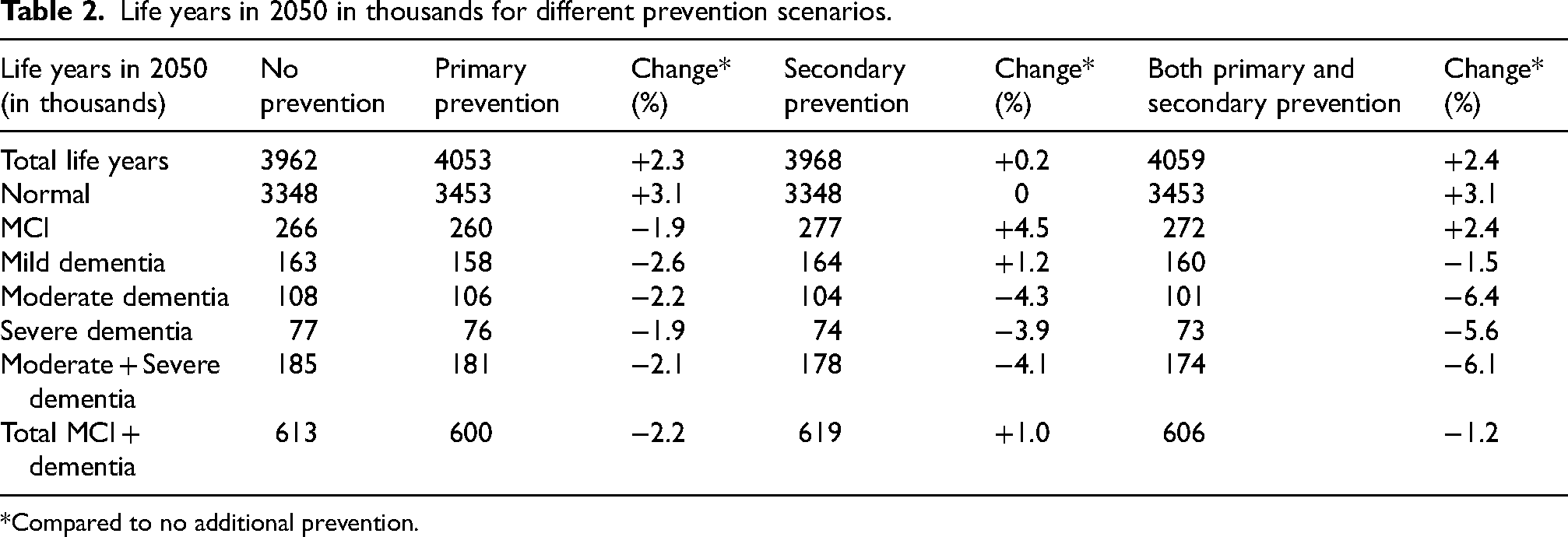
*Compared to no additional prevention.
Sensitivity analysis
The uncertainty of both the primary prevention effect size and secondary prevention effect size potentially have a substantial impact on dementia life years as they have a large confidence interval. In univariate sensitivity analyses, we therefore varied several uncertain parameters to investigate their influence on the results. We performed an additional analysis to investigate the interaction between primary and secondary effect size on the prevalence of moderate and severe dementia.
We varied the following parameters between hypothetical bounds: Primary prevention effect size (0.25-elimination), delay in other cause mortality (0–4), age of intervention (55–75, annual steps), risk factor attributability (0.2–0.6), secondary prevention effect size (1.05–2.00), and amyloid altering medication eligibility (0.15–0.80). These bounds were chosen due to lack of expert opinion or literature.
We also performed a multivariate sensitivity analysis on the primary and secondary effect size. Primary prevention delay time was varied between 0 and 10 years in steps of 0.4, and secondary prevention multiplication factor was varied between 1 and 2.25 in steps of 0.05. The stepsizes were chosen such that they represent the same mean time delay in moderate dementia onset. The total life years in moderate and severe dementia for each combination were presented in a heatmap.
Results
Results are provided per base case and univariate and multivariate sensitivity analysis.
Base case
Compared to no dementia-specific prevention, primary prevention increased total life years in 2050 by approximately 2.3% in 2050. Secondary prevention increased life years lived by about 0.2%. Both interventions in combination achieved an increase in life years lived of 2.4% (Table 2). The development of total and dementia life years over time can be found in Supplemental Figure 1.
With primary prevention, life years in all disease stages decreased, with the largest decrease in mild dementia (−2.6%). Life years without any neurodegenerative pathology increased by 3.1%. For secondary prevention, the life years spent with MCI and mild dementia increased (+4.5% and +1.2%), whereas the number of life years with moderate and severe dementia decreased (−3.9% to −4.1%). By design, there was no change in the number of life years without neurodegenerative pathology for secondary prevention, as it targets individuals in the early clinical stage of the disease course.
For both types of interventions together, the life years spent with MCI increased (2.4%) whereas life years spent with dementia decreased across dementia stages (mild: −1.5%, moderate: −6.4%, severe: −5.6%). Life years without neurodegenerative pathology increased by 3.1%, similar to primary prevention only.
Univariate sensitivity analysis
The sensitivity analysis (Figure 2) shows that the results are least influenced by risk factor prevalence (−4.2% to 2.5% compared to base case) and most influenced by the effect size of risk factor treatment for primary prevention (−4.2% to +12.2% compared to base case) and secondary prevention (−2.0% to +24.1% compared to base case). Age at intervention (−8.1% to +0.5% compared to base case, Supplemental Figure 2), delay in death due to other causes (−7.0% to +2.8% compared to base case) and eligibility for secondary preventative targeted therapies (−3.0% to +1.3% compared to base case) moderately influence the results.
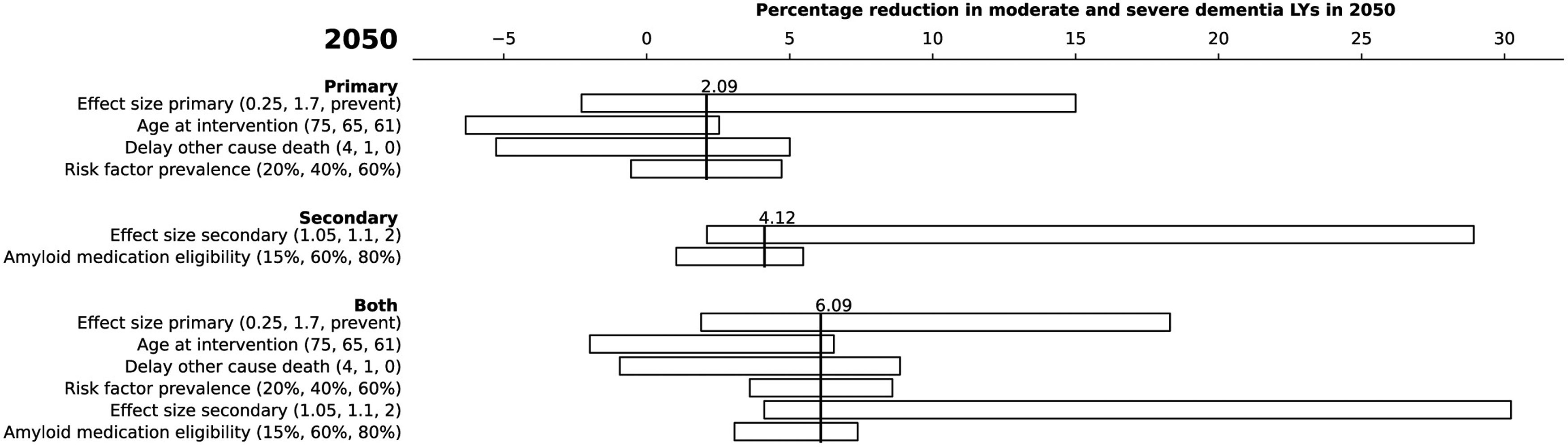
Tornado diagram of sensitivity analysis for different model parameter assumptions. Numbers in brackets after parameter description indicate left bound, base case and right bound parameter assumptions.
Multivariate sensitivity analysis
The cumulative moderate and severe dementia prevalence per 100,000 life years until 2050 in the base case scenario is 96,000. This cumulative dementia prevalence ranges from 67,000 under maximally effective interventions to 102,000 with no intervention (Figure 3A, Supplemental Figure 3).
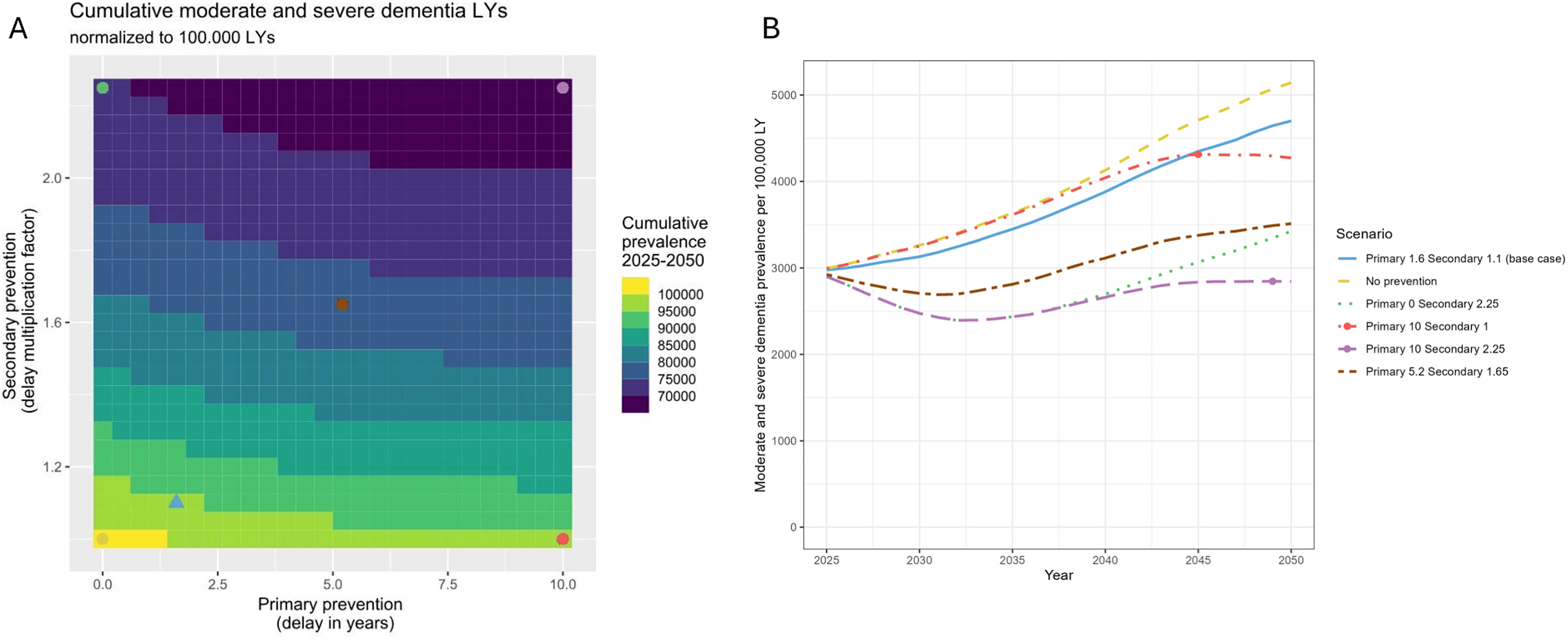
(A) Heatmap of the cumulative moderate and severe dementia rate in the period 2025–2050. The blue triangle indicates the base case. The combined moderate and severe dementia prevalences of base case and scenarios annotated by circles are shown in panel B. The colors of the circles correspond to the line colors in panel B. (B) Combined prevalences of moderate and severe dementia in different prevention scenarios. Circles indicate the maximum prevalence in each scenario in years other than 2050. In the legend, primary x secondary y denotes a primary prevention delay of neurodegenerative pathology onset by x years, and a secondary prevention multiplication factor y applied to the durations of MCI and mild dementia (Color figure available online).
We focused on six scenarios in more detail to examine the prevalence over time, varying both primary and secondary effect sizes (Figure 3B). The scenario with the largest values for the effect sizes (primary 10 secondary 2.25) shows an initial decrease in dementia prevalence, after which it returns to roughly the same prevalence as in 2025. None of the scenarios produced a sustained reduction in prevalence. Scenarios with a high secondary prevention effect (secondary 2.25) diverge from their non-effective counterparts (secondary 1) starting in 2025. Scenarios of primary prevention take more time to take effect, with effect size of 10 diverging from their counterparts (primary 0) from 2037. These scenarios with a large effect size for primary prevention are the only ones of these six that achieve a stable prevalence already some years prior to 2050.
Discussion
This study explored the potential future effects of individual-level primary and secondary prevention on life years spent in moderate and severe dementia, overall life years, and life years lived without dementia.
We found that individual-level dementia prevention interventions have moderate effectiveness of up to a 6.1% decrease in life years spent with moderate and severe dementia compared to no prevention in 2050. Individual-level primary prevention interventions mostly target cardiovascular risk factors, with beneficial effects on life expectancy due to the prevention of other diseases than dementia. This postpones death due to other causes, limiting the effect on life years with moderate and severe dementia. This effect becomes apparent when we vary the delay in other cause death as shown in the sensitivity analysis. We observe a 5.0% decrease in moderate and severe dementia prevalence for 0 years of delay, 2.1% decrease for 1 year of delay, and 5.3% increase in dementia prevalence for a 4-year delay in other cause death. Although precise effects on competing mortality are uncertain, there is some evidence from prospective cohort studies for compression of morbidity, i.e., the delay in onset of dementia outweighing the extension of life expectancy by at least a little. It should be noted too that primary prevention has the benefit of a 3.1% increase in dementia-free life years, whereas secondary prevention has none due to the design of the intervention.
The parameters with the largest influence on dementia life years were the effect sizes for both primary and secondary prevention. It must be stressed that these parameters also had the widest confidence intervals in the univariate sensitivity analysis.
Against the backdrop of the ageing population, none of the currently realistic scenarios showed a full stabilization of prevalence. Only if we assume 5 to 20 times larger effect sizes than there is evidence for (the most extreme case considered in the multivariate sensitivity analysis), the moderate and severe dementia life years stabilized in the future. Secondary prevention becomes effective immediately upon introduction and contributes more than primary prevention to the decrease in life years with moderate and severe dementia until 2050 due to compression of moderate and severe disease, although primary prevention also has the benefit of more normal life years. These effects may differ depending on the age at which treatment is initiated.
Using a dementia microsimulation model for France, Jacqmin-Gadda et al. estimated that dementia prevalence could decrease by 26% for women and 33% for men in a hypothetical situation when hypertension, diabetes, and physical inactivity are completely eliminated. 23 Applying more realistic risk factor reduction effects from the FINGER trial in our study, effects were substantially smaller. The FINGER trial demonstrated no significant change in the prevalences of most risk factors 15 Only physical activity prevalence showed a 9.1% point increase. This smaller effect on risk factor prevalence is most likely the major driver for the observed difference. Taken together, our findings underline that modelling of realistic effects is a prerequisite to provide sensible estimates of real-world intervention effects on the population burden of dementia. Moreover, joint modelling and presentation of the effect of combined primary and secondary prevention is insightful to this aim.
As the common aphorism has it, “all models are wrong, but some are useful”. We consider the MISCAN-dementia model valuable for estimating the impact of dementia interventions on the population-level disease burden. Yet, like any model, MISCAN-dementia is a simplification of reality and appropriate care should be taken when interpreting the results. Three considerations are of particular relevance. First, the effect of primary and secondary prevention on dementia onset has not been widely studied, except for blood-pressure lowering interventions. Instead, research has mostly relied on cognition outcomes or surrogate measures such as risk scores. This limitation is driven by the short duration of primary and secondary prevention trials relative to the slow disease progression, which also forced this study to assume sustained effects after the follow-up period, which we set to lifetime. This approach may overestimate the benefits in both approaches. We emphasize the need for longer clinical trials that have dementia incidence and stage progression as primary outcomes for reliable prediction of the benefit of prevention interventions and their projected future impact on society. Second, we assumed that all patients with MCI due to Alzheimer's disease were eligible for secondary preventative intervention, which is not realistic for currently available treatment options.24,25 Third, our understanding of the presymptomatic (Alzheimer's disease) stage and its relation to primary prevention remains limited. Vermunt et al., 14 which was used to inform presymptomatic disease stage durations in our model, only included participants with abnormal amyloid, so their conclusions are only applicable to Alzheimer's disease. Other dementia types, such as vascular dementia, are better characterized by different biomarkers, 26 although there is an overlap in the pathophysiological pathways. There is limited understanding of the interaction between pathophysiological pathways and various preventative interventions. Nevertheless, the primary prevention effect was implemented such that the overall result matched the results of the FINGER primary prevention trial. It is difficult to judge whether this over- or underestimated the benefits of primary prevention, which further calls for longer-term evidence.
The impact of secondary preventative therapies depends predominantly on effect size and percentage of the population with MCI eligible for the intervention. The strict inclusion and exclusion criteria in current trials for anti-amyloid therapies result in 8–15% of the population being eligible,24,25,27 and the appropriate use recommendations are restrictive accordingly. 20 We assumed 60% eligibility for anti-amyloid treatment and therefore likely overestimated its benefits.
It is important to emphasize that the model used in this study projects dementia trends specifically for the Dutch population. 5 Although population demographics and dementia incidence trends are similar in other high-income country in Europe and North America, results are not directly applicable to low- and middle-income setting. Beyond demographics, the external validity for primary prevention depends largely on lifestyle factors, while secondary prevention is mostly influenced by dementia type. Western countries share similar risk factor prevalences, but Latin American, Asian and African countries have a different distribution of risk factors and population attributable fractions, meaning that primary effect size may not be directly translatable.28–30 Moreover, the base case scenario in the current study included relatively high standards of cardiovascular risk management, and effects of similar interventions may be higher in healthcare settings where risk factor treatment is less widespread.
Conclusions
Individual-level primary or secondary prevention have different effects on the population-wide dementia burden, depending mostly on the anticipated effect size of the intervention. Primary prevention postpones disease and increases life expectancy, but effects take many years to manifest and accrue over time. In contrast, secondary prevention yields more immediate effects. However, per definition, reductions in years lived with moderate/severe dementia are offset by prolonged time in MCI and mild dementia. Whilst a combination of both primary and secondary preventative interventions will be needed to fulfill the potential of prevention, none of the modelled scenarios completely offset the aging-related increasing population dementia prevalence before 2050. The estimates from this study can be used by policymakers to anticipate on the increasing prevalence of dementia in our aging society and the potential of current individual-level primary and secondary intervention to reduce it.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457937 - Supplemental material for Primary and secondary prevention strategies for reducing population-level dementia burden: A microsimulation modeling study
Supplemental material, sj-docx-1-alz-10.1177_13872877261457937 for Primary and secondary prevention strategies for reducing population-level dementia burden: A microsimulation modeling study by Lynn Van Rosmalen, Chiara C. Brück, Frank J. Wolters, Ron Handels and Inge M. C. M. De Kok in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
During the preparation of this work the lead author used ChatGPT in order to improve the articulation of the discussion section, and Microsoft Copilot to refine the abstract. After using this tool/service, all authors reviewed and edited the content as needed and the lead author takes full responsibility for the content of the publication.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the BIRD-NL consortium funded by the Dutch Medical Research Council, ZonMw (Dementia research program) project number: 10,510,032,120,005.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Code and raw model output will be available upon request.
Supplemental material
Supplemental material for this article is available online.