
Abstract
Background
Physical activity and fitness are major targets in Alzheimer's disease (AD) preventive research. However, current research is heterogeneous and often disregards the relationship between these parameters and disease outcomes.
Objective
To assess the effects of physical activity and fitness on AD within the context of a multicomponent sports intervention.
Methods
46 participants with early-stage AD (mean age 70 ± 7 years, 18 women, mean Montreal Cognitive Assessment (MoCA) score 19±5) were included in a six-month randomized controlled trial (Dementia-MOVE), participating in either a multicomponent sports intervention or a control condition with a psychoeducational program. The modulating effect of fitness and physical activity changes on AD outcome parameters such as cognition, function and cerebral brain structure from 3T-MRI were examined using multiple linear regression analyses.
Results
An increase in VO2max was associated with assignment to the intervention group (p = 0.016), lower baseline fitness (p = 0.001), and an increased rate of physical activity (p = 0.046). Only in the intervention group, ΔVO2max had a beneficial modulating effect on the MoCA score (p = 0.039), the executive functions (p = 0.017) and regional brain volumes of the temporal lobe, e.g., the hippocampus (p = 0.044). High daily step count was associated with preserved executive functions (p = 0.001), and caregivers’ quality of life (p ≤ 0.001) in the overall sample.
Conclusions
Our results confirm that multicomponent exercise improves cardiorespiratory fitness in AD, which is associated with advantageous developments in cognitive performance and preservation of brain structure. These findings suggest that especially patients with comparably worse cognition and fitness benefit and should be encouraged for activity engagement.
Keywords
Introduction
Aging society and rising life expectancy are associated with an increased prevalence of chronic diseases like dementia, accompanied by higher rates of care dependency and mortality, as well as elevated treatment costs. 1 Looking at Alzheimer's disease (AD) as the most common type of dementia, the disease often progresses over years, from mild cognitive impairment (MCI) or early manifest AD, characterized by clinically assessed minor cognitive limitations, to increasing symptom burden and disability as the neurodegeneration advances.2,3 Aside from pharmacological therapies, exercise that increases cardiorespiratory fitness (CRF) has previously been shown to be an effective, low-cost, and easily accessible treatment option for both elder individuals at risk, as well as patients diagnosed with amnestic MCI (aMCI) or AD.4,5
While there is increasing evidence that general physical activity, defined in contrast to sedentary behavior, can protect against cognitive decline,6,7 the underlying effects at the cerebral level with regard to neurodegeneration are still subject to intensive research. Current findings suggest that physical activity influences neuronal molecular pathways, optimizes brain metabolism, and increases regional cerebral blood flow.8,9 Neuroimaging studies based on these considerations show that high physical activity levels and short-term interventions for up to six months could influence brain structure in AD-affected regions such as the hippocampus and further regions of the temporal lobe. Yet their findings are inconsistent due to the general heterogeneity of study designs and often not clearly characterized study populations.10–13 Thus, the question of how exactly fitness and physical activity affect brain integrity during neurodegeneration still remains unanswered.
Furthermore, previous exercise trials often fail to consider the complex mutual relation of physical activity and fitness improvement in the context of a sports intervention; hence, their interacting effect on the different aspects of AD pathology is unclear. 14 Establishing a suitable intervention and finding the optimal exercise dose for the elderly and cognitively impaired population is therefore challenging but at the same time highly clinically relevant. So far, multicomponent exercise interventions comprising moderate-to-vigorous physical activity (MVPA) at least twice a week for a minimum duration of three to six months appear to be the most promising for increasing CRF.15,16 In line with these findings, the World Health Organization (WHO) has also published recommendations on the rate of physical activity in elder subjects, constituting at least 150–300 min of moderate-intensity or at least 75–150 min of vigorous-intensity aerobic physical activity per week, with the recommendation to perform multicomponent activity to prevent falls and increase muscle strength. 17 Additional psychoeducational and lifestyle-modifying programs, for instance based on the FINGER study design, can also increase adherence to and acceptance of such recommendations and interventions,18,19 pointing again to the relevance of multicomponent lifestyle interventions.
The Dementia-MOVE trial (
We expect that people with AD participating in the exercise intervention program will improve their fitness compared to a control group attending a psychoeducational program only. We hypothesize that increased fitness and a higher level of physical activity due to participation in the intervention program leads to a positive impact on cognitive performance, neuropsychiatric health and brain integrity in AD. As an underlying goal, we examine the feasibility and acceptance of this intensified program as a treatment option in a cohort of elderly people affected by AD.
Methods
Study design and participants
The study Dementia-MOVE is a randomized controlled clinical trial with two arms, including an intervention group receiving a six-month multicomponent exercise training and a control group undergoing a psychoeducational program. 20 In summary, a total of 46 people aged between 50 to 80 years with early AD, who were cognitively and physically eligible for a physical exercise program, were recruited at the memory clinic of the Department of Neurology of the RWTH Aachen University Hospital (UKA), and via advertising and search in newspapers (see Figure 1). All participants were characterized as having mild cognitive impairment (MCI) or mild AD with a cerebrospinal fluid (CSF) constellation of amyloid-β 1-42 or amyloid-β 42/40 ratio (A), phospho-tau (T), and tau (N) based on Jack et al. (2018), resulting in their characteristic ATN-status alongside the AD-continuum. 21 According to this, all participants included showed a pathological amyloid CSF concentration (A+), with phospho-Tau CSF concentrations in either elevated (A+T+; n = 32) or normal range (A+T−, n = 9). In cases where CSF biomarkers were not available (n = 5), the diagnosis of AD was based on neuroimaging and clinical evaluation (i.e., neurological examination, and neuropsychological assessment) as part of an expert consensus at the memory clinic at UKA. All participants presented an early-stage disease with a Clinical Dementia Rating scale (CDR) ≤1. Exclusion criteria mainly included severe systemic, cardiopulmonary, orthopedic and/or psychiatric diseases (for a complete overview of the inclusion and exclusion criteria, see also Supplemental Table 1). Sample size calculations were based on power analyses which were derived from our primary outcome parameter presented by metabolic MR imaging and our previous results in this context.20,22,23 After performing baseline assessments at time point T1, participants were randomized into either the exercise intervention group (n = 26) or the control group (n = 20) by a blinded member of the study team using the WINPEPI software. 24 Stratification followed age and fitness level, as determined via VO2max, or in case of non-availability, the result of the 6-min walk test (6MWT). The site of residency was further considered when allocating between Aachen and Simmerath. In case of unequal numbers of participants, allocation was performed in favor of the intervention group.
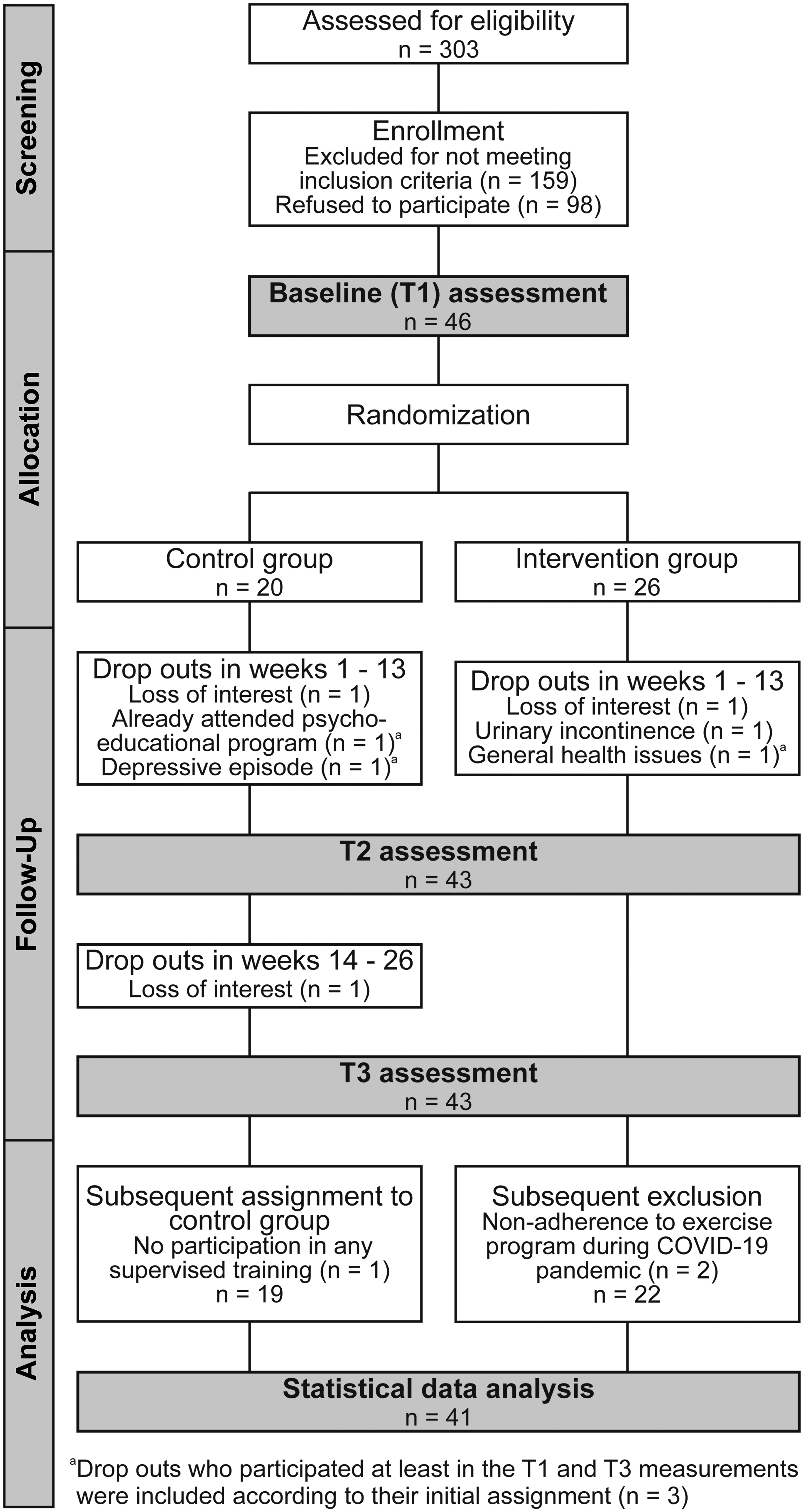
Participant flow chart of the screening and intervention period and the subsequent analysis. A total of 41 patients (22 in the intervention group and 19 in the control group) were finally included for statistical data analysis. Note that even when nine participants dropped out of the program, four participants still agreed to participate in the outcome assessments.
The study and all protocol changes were approved by the Ethics Committee at the Medical Faculty of the Rheinisch-Westfälische Technische Hochschule Aachen (RWTH Aachen) (EK 306/18) and were performed according to the latest Declaration of Helsinki. All participants gave written informed consent for study participation and protocol changes. The trial was registered at ClinicalTrials.gov (NCT03939286). Further details on the study design of the Dementia-MOVE protocol have been previously published. 20
The multicomponent intervention program
A detailed overview of all intervention components is presented in Figure 2. The intervention program started after randomization and took place for a total duration of 26 weeks (six months plus two weeks for optional compensation on missed appointments). Participants assigned to the intervention group attended a supervised exercise session for 60 min per week, taking place at two study sites, the UKA or the hospital Eifelklinik St Brigida in Simmerath, located approximately 20 km south-east of Aachen, with its affiliated professional physiotherapy practice. The program was homogenized between both sites and included aerobic, resistance, and coordination exercises. It was supervised by physiotherapists and members of the study team. Sports groups usually consisted of about five participants per group, therefore assuring an optimized supervision and individualized guidance of the sports program. During the first supervised training session, the optimal exercise load for the program was determined for each individual: (1) ergometer wattage was estimated from 6-MWT distance according to Luxton et al., 25 and (2) load for a moderate resistance training intensity was calculated according to the Epley formula for 40% of one-repetition-maximum. 26 Over the course of the intervention period, the exercise load was then gradually increased according to moderate-to-vigorous physical exertion regularly surveyed using the Borg RPE-scale during the training sessions. 27 An exemplary training plan including mean initial exercise loads is provided in the Supplemental Table 2.
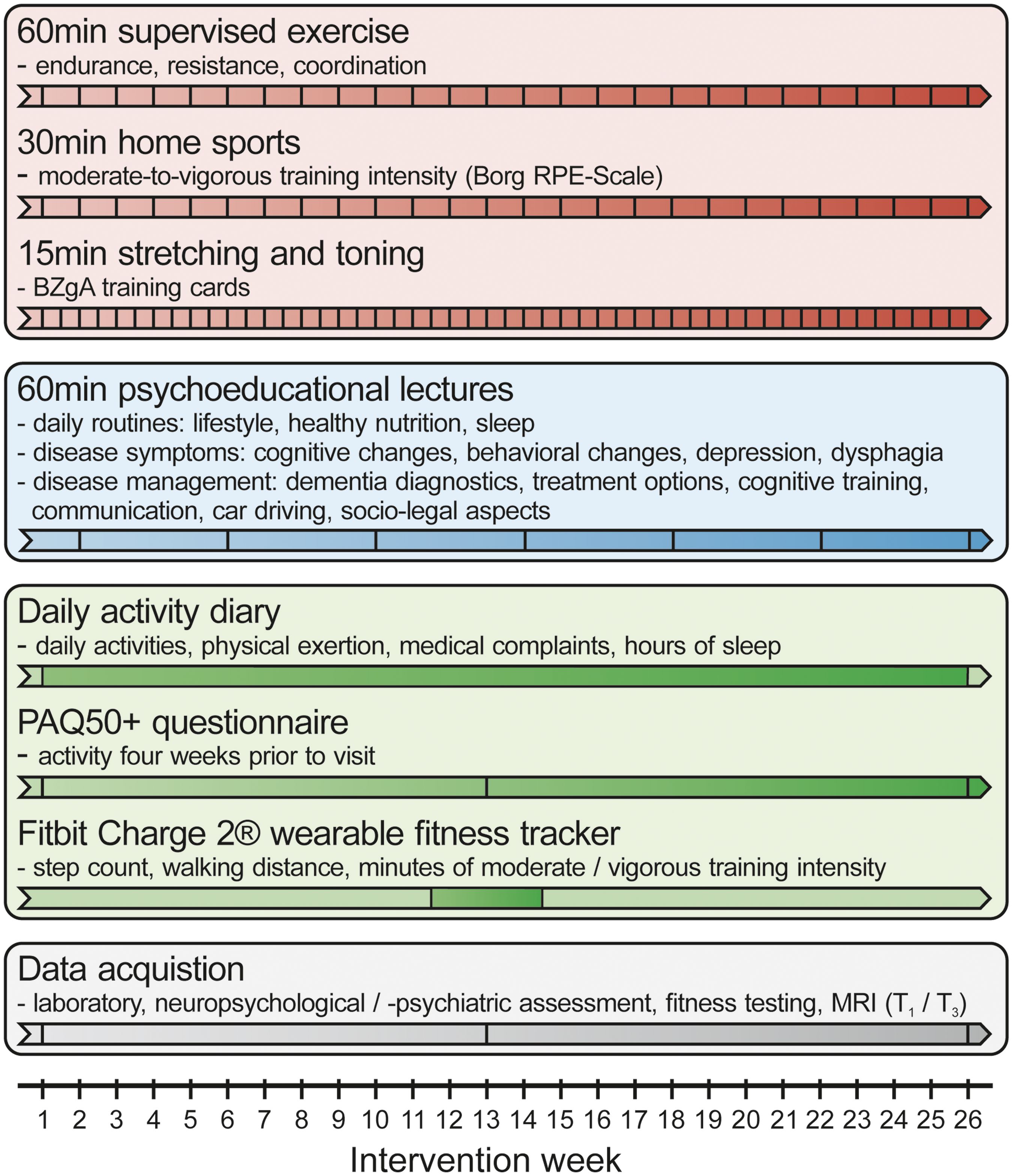
Outline and timeline of the multicomponent intervention design with its three main components: the supervised exercise, the psychoeducation program and the different methods for activity monitoring as well as the three acquisition time points. Borg RPE-Scale: Borg Rating of Perceived Exertion Scale; BZgA: German Federal Centre for Health Education.
In addition to the participation in the supervised training program, participants of the intervention group were further instructed to perform a moderate-to-vigorous intensity home-based training for at least 30 min per week, as well as stretching and toning exercises for at least 15 min twice per week, following current recommendations on repetitive physical exercise. 28 Supporting training cards from the German Federal Centre for Health Education (BZgA) for the stretching and toning exercises were distributed to the intervention participants. 29
Furthermore, both groups participated in monthly psychoeducational lectures at both study sites, respectively, with a focus on lifestyle modifying factors, disease management, and help offers, as well as therapy options based on the content of the FINGER study (see Figure 2), 30 thus, also controlling for the social aspect of the intervention as control condition.
During the first COVID-19 lockdown in Germany, the supervised exercise program was substituted by a home-based training for nine weeks from March to May 2020, for 18 participants. Exercises in the home-based training were chosen to optimally resemble the supervised training and to address the same muscle groups without resorting to training machines, yet participants were allowed to implement available home gym equipment at any time. To optimize coordination training at home, the participants received an MFT Fun Disc® balance plate, which was also used during the training sessions at both study sites. Instructions for a homogenized home-based training were sent in written form and orally explained to all participants of the sports groups and their relatives (see also Supplemental Table 2). The psychoeducational topics were summarized in paper form and sent to all participants during the lockdown period. The discussion of these lectures and a check for training adherence was carried out by weekly telephone calls through the study team. Since the T3 assessment of five participants was not feasible at that time, the intervention was extended for a further nine weeks for these individuals to maintain the intervention effect, until the lockdown was terminated, and assessments could be safely performed.
Measuring fitness and physical activity
Aerobic fitness was assessed via estimation of VO2max, a well-established and validated parameter in exercise testing, which defines a person's maximum capacity to absorb and metabolize oxygen. 31 We therefore performed a submaximal ergometer test on a Lode Corival CPET® device following a modified Astrand protocol. 32 Additionally, the 6-MWT was performed for an alternative estimation of VO2max when the participants failed to increase heart frequency during the Astrand protocol, for instance, due to β-blocker intake or orthopedic impairment impeding ergometer cycling, which can be common in an elder population. 33
Furthermore, handgrip strength was measured using a Saehan® hand dynamometer, 34 as well as postural stability via the MFT-S3-Check® system, which records stability, sensomotorics, and symmetry data of two passes, with a balance plate tilting front/back and left/right, respectively. 35 Previous studies have associated weak performance in both parameters with cognitive decline.36,37 All fitness assessments were performed at time point T1 at baseline, after three months at time point T2, and after six months at time point T3.
A written diary was used to monitor physical activity and compliance throughout the entire duration of the intervention. It was completed by the participants with the help of their caregivers if needed and included space for the participants to record types and duration of daily activities as well as additional information such as subjective exertion during exercise, hours of sleep, medication taken if necessary, and medical issues occurring during study participation. Filled pages were regularly collected by the study team and checked for missing or incomplete data. In case of such occurrences, the participants and caregivers were re-advised to avoid missing data on previous activities. 38
Furthermore, the PAQ50+ questionnaire, which is adapted to physical activity assessment in elder people, was used at each assessment time point four weeks prior to the visits T1, T2, and T3. 39 To demonstrate the reliability of these two subjective assessing methods, the Fitbit Charge 2® (Fitbit), a wearable fitness tracker, was distributed to the study participants for an average duration of 14 days around the middle of the intervention period to objectively record activity during that time. The Fitbit registered step count, walking distance, activity minutes of varying intensity, calorie consumption, as well as sleep.
Processing of physical activity and fitness assessment data
A detailed methodological description and comparison of the three assessment methods of physical activity and fitness, i.e., the wearable fitness tracker, the written diary, and the PAQ50+, is presented in our recent publication.
38
In short, daily metabolic equivalent of task (MET) scores were calculated based on the different output data as follows:

A further MVPA score was calculated by summarizing daily moderate and vigorous activity minutes for all three assessing methods. For the diary and the PAQ50+, activity minutes were computed based on the activities’ individual MET scores, classifying moderate activity as MET 3–5.9 and vigorous activity as MET >6 according to previous literature.41,42
VO2max as a measure of CRF was estimated from ergometer testing data according to von Dôbeln et al.,
43
taking the advanced age and differing body compositions as well as maximum heart rates of an elder study population into account compared to the classic nomogram introduced by Astrand and Rhyming (1954)
32
:

For handgrip strength, we focused on the participants’ dominant hand (right = 38, left = 2, ambidextrous = 1 of the included subjects). Furthermore, a mean composite score of all postural stability measuring components was calculated, including Z-standardized stability, sensomotoric and symmetry values of the two different passes performed.
Assessment of AD outcome parameters
Neuropsychiatric and cognitive screening
Neuropsychiatric and behavioral symptoms were assessed via questionnaires sent to the participants and their relatives in advance of each assessment appointment T1, T2, and T3. This assessment included the Quality of Life in AD (QoL-AD), 45 the German version of the Hospital Anxiety and Depression Scale (HADS-D), 46 the Neuropsychiatric Inventory Questionnaire (NPI-Q), 47 as well as the Pittsburgh Sleep Quality Index (PSQ-I). 48 Absolute questionnaire scores were used for the subsequent analyses. For HADS-D and PSQ-I, higher scores indicate more severe depressive symptoms and worse sleep quality, respectively.
Global cognitive screening was evaluated via the Mini-Mental State Examination (MMSE, at baseline T1 only), 49 and the Montreal Cognitive Assessment (MoCA). 50 Furthermore, a neuropsychological test battery focusing on attention, verbal memory, and executive functions was performed. Alternate versions of the tests were used at the three assessment time points T1, T2, and T3, if available. The attention score comprised cued and non-cued reaction time of the Test of Attentional Performance (TAP), 51 and digit span forward. 52 Verbal memory was assessed via the California Verbal Learning Test (CVLT). 53 Executive functions domain included the Trail Making Test's (TMT) B/A-ratio, 54 phonemic and semantic word fluency, 55 digit span backwards, 52 and the Stroop interference task. 56 Results of the individual tests were Z-standardized with baseline means and standard deviations as references and then summarized as mean composite scores for each domain. 57
Structural MRI analysis
All MRI images were acquired on the same 3-Tesla Siemens PRISMA whole-body MR scanner at baseline (T1) and after the intervention (T3). Isotropic high-resolution T1-weighted images of the brain were obtained with an MP-RAGE sequence (TR = 2400 ms, TI = 1000 ms, TE = 2.4 ms, FA = 8°, 0.8 mm isotropic resolution). Images were segmented into gray matter, white matter, CSF, brainstem and cerebellum via the antsLongitudinalCorticalThickness.sh pipeline implemented in Advanced Normalization Tools (ANTs). 58 Parcellation for a region of interest (ROI) approach was performed via the Hammersmith Brain Atlas, containing 68 brain regions, 59 as well as VolBrain for the segmentation of subcortical regions. 60 For the current analysis, eight ROIs in the temporal lobe were preselected, of particularly high interest in AD: hippocampus (HPC), amygdala (AMG), medial anterior temporal lobe (M-ATL), lateral anterior temporal lobe (L-ATL), parahippocampal and ambient gyri (PHC), superior temporal gyrus (STG), middle and inferior temporal gyri (MTG/ITG) and fusiform gyrus (FFG). All brain volumetric data were normalized for the total intracranial volume (TIV) and averaged between both hemispheres.
Furthermore, T1-weighted and fluid-attenuated inversion recovery (FLAIR) MR images (TR = 9000 ms, TI = 2500 ms, TE = 79 ms, FA = 150°, 0.4 mm × 0.4 mm × 3 mm resolution) were used for the segmentation of white matter lesions in VolBrain, resulting in the total lesion volume of all intracerebral lesions at baseline and after intervention.61,62
For whole-brain group comparison, a tensor-based-morphometry analysis was performed. The logarithm of the determinant of the Jacobians (Log(
Statistical data analysis
Statistical analyses were performed using IBM SPSS Statistics 26 software and MATLAB R2019b. First, all data were visually inspected for normal distribution and possible outliers in boxplots and scatter plots. MR data were checked for segmentation failure, movement artifacts, and structural brain lesions as well. Pairwise deletion was applied for missing data. The participants’ characteristics and measurement data were compared for group differences using mean (M), standard deviation (SD), median (Mdn), median absolute deviation (MAD) as well as independent samples t-test, Mann-Whitney-U-test and Chi-square analysis, as indicated. Correlation analyses of fitness and activity data were performed using Pearson's correlation and Spearman's rank correlation, reporting the correlation coefficients r and ρ, respectively. Differences between follow-up minus baseline values (T3-T1) for the different assessment parameters were calculated and indicated with delta (Δ). Changes in fitness parameters were analyzed via multiple linear regression analysis, including group, fitness baseline levels, age, and sex as predictors, considering collinearity tests. To investigate the influence of the COVID-19 study protocol changes, a categorical variable (encoding 0 = not affected, 1 = affected), further referred to as Cov-19adj, was entered into the model as well.
Prediction of neuropsychiatric, cognitive, and brain structural changes was then carried out via multiple linear regression analysis. Changes in VO2max, i.e., ΔVO2max, and activity via Fitbit step count were entered as predictors in separate models. At first instance, we tested for potential confounding factors, including age, sex, baseline cognition, CSF status and study site as covariables in the model. Based on the results of this analysis, the design was simplified by excluding non-significant covariables for the final analysis, which was performed in each group separately regarding ΔVO2max as the dependent variable, and in the overall cohort regarding the Fitbit step count. The influence of ATN and APOE4 carrier status was further investigated by additionally entering those parameters as categorial variables into the regression models (encoding 0 = A+T−, 1 = A+T+, as well as 0 = heterozygous APOE4 allele carrier/non-APOE4 allele carrier, 1 = homozygous APOE4 allele carrier) on a probatory basis.64–66 For neuropsychiatric and cognitive parameters, the respective baseline level was included in all models to adjust for the individual clinical disease manifestation. If the model included more than one possible predictor, the best fit was determined via changes in RMSE and R2 as well as overall significance in all models. Significance is determined by an uncorrected p < 0.05 to meet the exploratory concept of the analysis. Effect size estimates were calculated using Cohen's d and Pearson's r as indicated. The 95% confidence intervals (95% CI) are reported. Furthermore, for the whole brain analysis, a voxel-wise permutation analysis (n = 2000 permutations) for comparison of the intervention and the control group was performed in BROCCOLI, 67 on voxels inside the brain tissue mask with a statistical threshold of p < 0.05, including MoCA at baseline, VO2max at baseline, and education in years as covariates into the model.
Results
Participant flow
A total of 46 participants were initially included at baseline and randomized into either the intervention group (n = 26) or the control group (n = 20). At the UKA site, 19 people participated in the sports program, and seven in Simmerath. 43 participants completed the three-month and 43 completed the six-month follow-up (see Figure 1). Participants who missed all exercise sessions or psychoeducational lectures, yet still participated at least at the T1 and T3 assessments (n = 3) remained in the final analysis. Apart from that, one participant originally randomized to the intervention group, but unable to participate in any training session due to urinary incontinence and therefore sedentary, yet regularly attending the psychoeducational lectures, was allocated to the control group for final analysis. Furthermore, two participants of the intervention group were excluded from the final analysis for non-adherence to the home-based exercise program during the COVID-19 lockdown (German lockdown 03/19/2020 to 05/12/2020). Brain MRI was omitted in four out of the 41 remaining participants (n = 1 intervention group, n = 3 from control group) from at least one assessment time point. Reasons for not performing the MRI on these subjects were claustrophobia (n = 3), and the presence of a cardiac pacemaker unit (n = 1). For a detailed illustration of the participant flow, see also Figure 1.
Adherence to protocol
Mean adherence to the supervised exercise intervention was 72% (SD = 16%) and could be increased to 76% (SD = 16%) including two additional appointments that were offered if attendance was below the targeted 80% after 26 weeks of intervention. Eleven participants of the intervention group (50%) had an attendance of more than 80%. Reasons for reducing training participation for longer than a week were chronic musculosceletal pain (n = 5), rehabilitation after minor surgery (n = 3), respiratory infection (n = 2) and a toe abscess (n = 1).
Participants of the intervention group attended an average of four out of the seven psychoeducation lectures offered during the intervention period, while those in the control group attended an average of five events.
Regarding the activity diary, an average of 85% (SD = 22%) versus 77% (SD = 36%) of diary entries were completed, based on 182 days (26 weeks), in the intervention and the control group, respectively.
Occurrence of adverse events
There were no severe adverse events to report in both groups. Non-serious adverse events possibly associated with the intervention during the supervised exercise mainly included musculoskeletal pain (n = 4), vertigo (n = 2), nausea (n = 1), arterial hypertension (n = 1), and headache (n = 1). In case of discomfort, the exercise load was reduced, or the training session was terminated prematurely, which occurred once for three subjects and twice for one subject over the course of the intervention.
Baseline results and patient characteristics
An overview of the baseline characteristics and measurements of the analyzed study sample is given in Table 1A and 1B. At baseline, there was a group difference between the intervention group compared to the control group in terms of mean years in education (12.5 ±. 3.8 years versus 14.8 ±. 2.4; U = 107, z = -2.71, 95% CI (1.00, 4.00), p = 0.01, r = 0.42) and mean MoCA score (17.1 ± 4 versus 21.3 ± 4.8; t (39) = -3.02, 95% CI (−6.89, −1.36), p = < 0.01, |d| = 0.95). Performance in the executive functions domain also differed between the intervention and the control group (−0.21 ± 0.61 versus 0.24 ± 0.6; t (39) = -2.41, 95% CI (−0.84, −0.07), p = 0.02, |d| = 0.75). There were no group differences at baseline in other cognitive domains. Furthermore, the amyloid-β 42/40-ratio as well as tau and phospho-tau levels from CSF differed between both groups. However, it is important to note that CSF markers were acquired during the diagnostic process and not at the time point of study inclusion, with a maximum time distance of 1954 days before the intervention start. Therefore, interpretation of these differences in CSF pathology must be made with caution.
Basic characteristics of the included study sample (n = 41/46) at baseline.
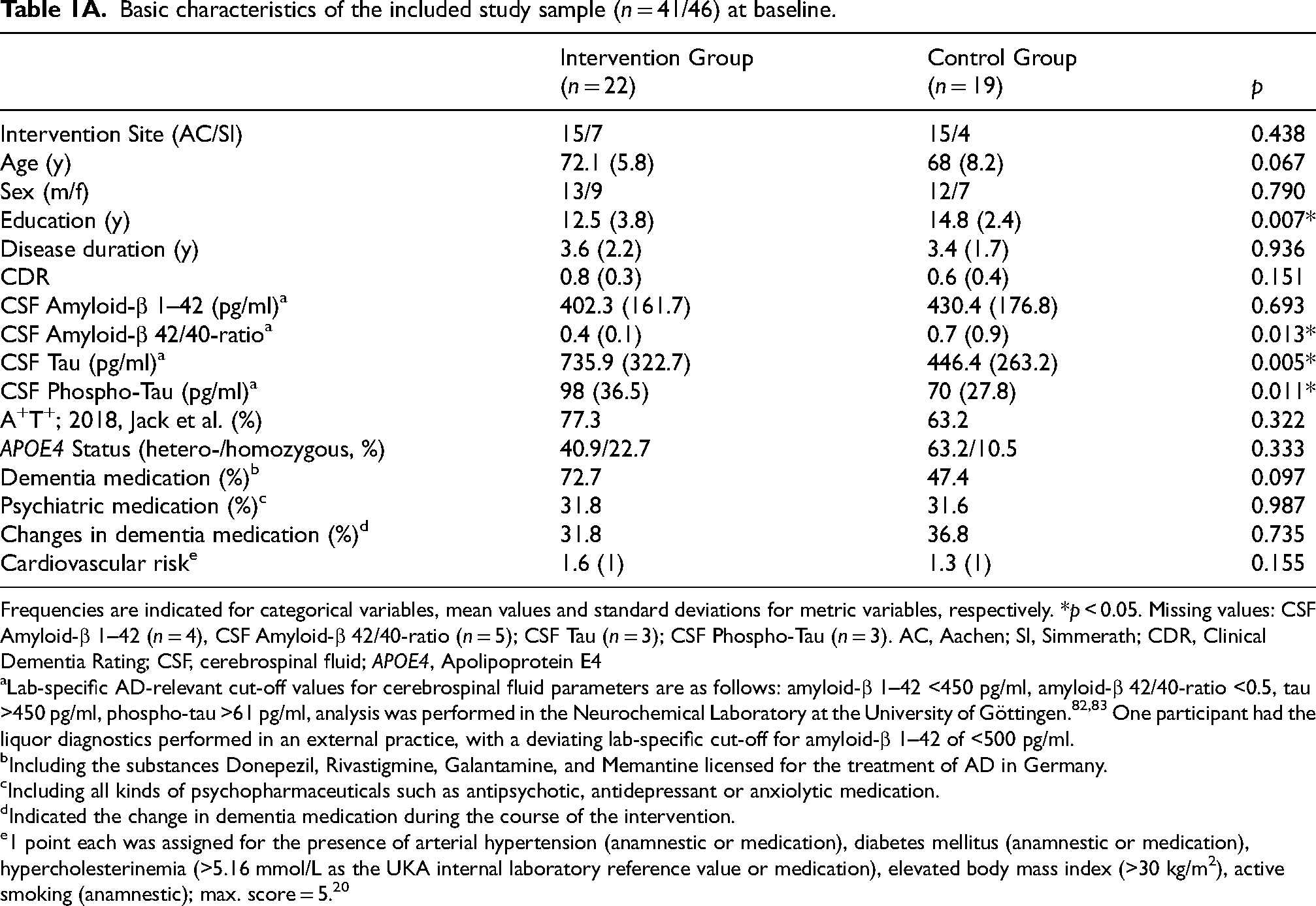
Frequencies are indicated for categorical variables, mean values and standard deviations for metric variables, respectively. *p < 0.05. Missing values: CSF Amyloid-β 1–42 (n = 4), CSF Amyloid-β 42/40-ratio (n = 5); CSF Tau (n = 3); CSF Phospho-Tau (n = 3). AC, Aachen; SI, Simmerath; CDR, Clinical Dementia Rating; CSF, cerebrospinal fluid; APOE4, Apolipoprotein E4
Lab-specific AD-relevant cut-off values for cerebrospinal fluid parameters are as follows: amyloid-β 1–42 <450 pg/ml, amyloid-β 42/40-ratio <0.5, tau >450 pg/ml, phospho-tau >61 pg/ml, analysis was performed in the Neurochemical Laboratory at the University of Göttingen.82,83 One participant had the liquor diagnostics performed in an external practice, with a deviating lab-specific cut-off for amyloid-β 1–42 of <500 pg/ml.
Including the substances Donepezil, Rivastigmine, Galantamine, and Memantine licensed for the treatment of AD in Germany.
Including all kinds of psychopharmaceuticals such as antipsychotic, antidepressant or anxiolytic medication.
Indicated the change in dementia medication during the course of the intervention.
1 point each was assigned for the presence of arterial hypertension (anamnestic or medication), diabetes mellitus (anamnestic or medication), hypercholesterinemia (>5.16 mmol/L as the UKA internal laboratory reference value or medication), elevated body mass index (>30 kg/m2), active smoking (anamnestic); max. score = 5. 20
Measurement results at time points T1 and T3. Mean values and standard deviations, as well as group tests in direct time-point comparison, are indicated.
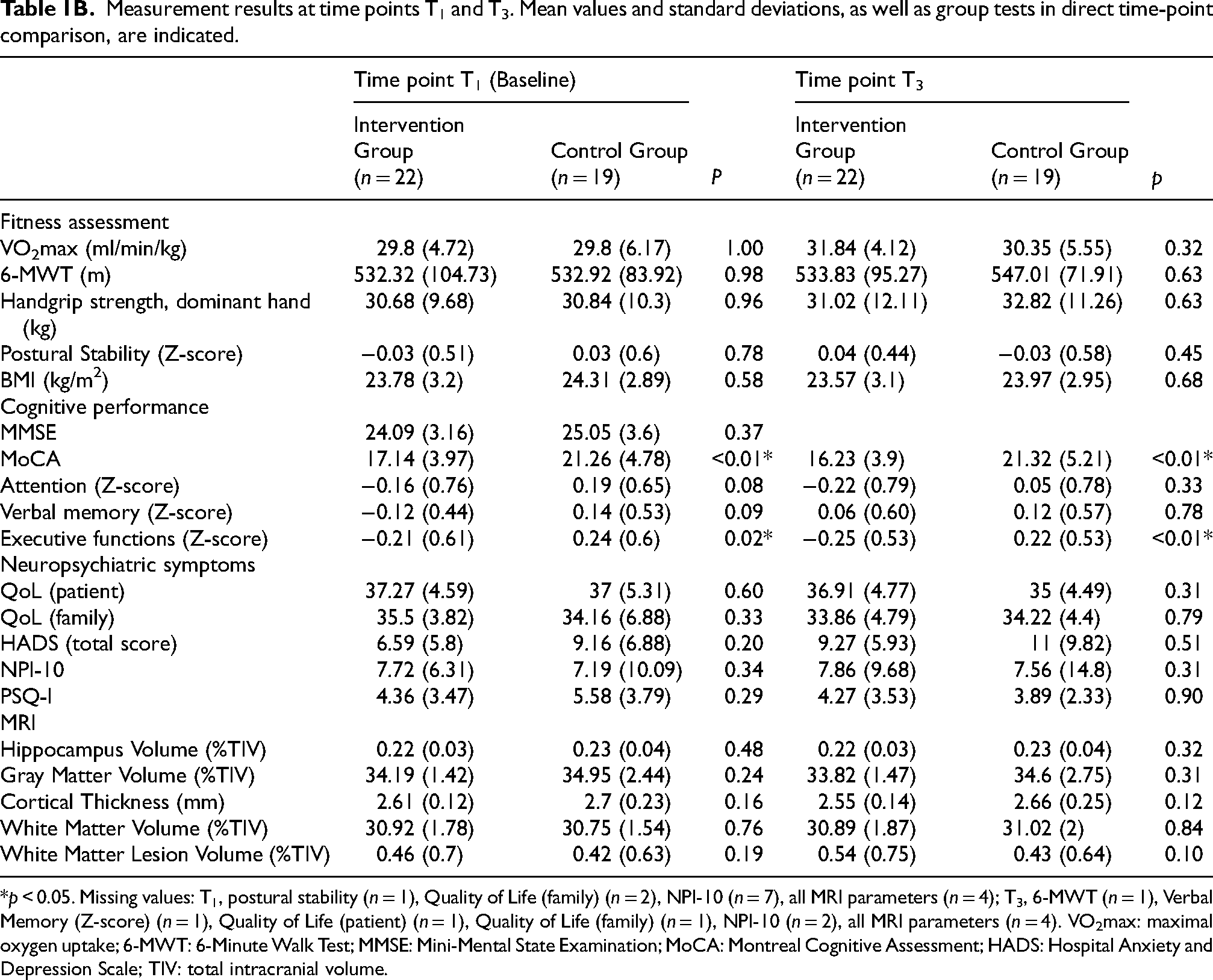
p < 0.05. Missing values: T1, postural stability (n = 1), Quality of Life (family) (n = 2), NPI-10 (n = 7), all MRI parameters (n = 4); T3, 6-MWT (n = 1), Verbal Memory (Z-score) (n = 1), Quality of Life (patient) (n = 1), Quality of Life (family) (n = 1), NPI-10 (n = 2), all MRI parameters (n = 4). VO2max: maximal oxygen uptake; 6-MWT: 6-Minute Walk Test; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; HADS: Hospital Anxiety and Depression Scale; TIV: total intracranial volume.
Monitoring of physical activity and fitness during the intervention
Assessment and monitoring of physical activity served mainly two purposes: (1) to check for protocol adherence, and (2) to assess general physical activity and fitness during the study. In a recent publication, we demonstrated the good validity of the diary and fitness trackers for the assessment of physical activity and fitness in the same patient group, 38 with comparable values in MET-scores and MVPA between the assessment via the fitness tracker and the diary (see Supplemental Table 3 and Supplemental Figure 1). Therefore, fitness tracker activity levels were considered as representative for general activity level for the whole intervention period, while physical activity reported by the PAQ50+ questionnaire was used as an assessment prior to intervention start.
Based on the physical activity reported in the diaries, both the intervention and the control group fulfilled, on average, the current WHO recommendations for general physical activity for the elderly during the study period, with a median weekly activity time of 171 min of moderate-intensity and 91 min of vigorous activity in the intervention group, and 281 min of moderate-intensity and 72 min of vigorous activity in the control group per week. 17 At the subject level, the WHO recommendation was achieved by 19 participants in the intervention group and 16 participants in the control group.
Over the six-month intervention period, the global level of daily MET derived from the diary remained constant over time in both groups. The rate of vigorous activity reported was higher in the intervention group compared to the control group (intervention, Mdn = 15.18, MAD = 3.50; control, Mdn = 10.39, MAD = 6.87; U = 112, z = -2.13, 95% CI (−11.93, −0.57), p = 0.03, r = 0.34). However, the rate of moderate activity appeared to be higher in the control group compared to the intervention group (see also Figure 3), where we observed that a few outlying individuals in the control group with an exceptionally high activity level led to a generally higher level of reported moderately intense activity on average (intervention, Mdn = 27.39, MAD = 12.94; control, Mdn = 48.19, MAD = 20.25; U = 86, z = -2.86, 95% CI (6.99, 41.60), p = < 0.01, r = 0.46).

Physical activity development during the intervention period derived from the paper-based physical activity diary. Daily median moderate (A) and vigorous (B) activity minutes for every intervention month in both groups are indicated, including the 95% confidence intervals. For the intervention group, the supervised exercise program and all home sports activities are included. *significant results in the Mann-Whitney U test with p < 0.05. Missing values: n = 2.
The development of fitness parameters over the intervention is illustrated in Figure 4: all fitness parameters increased in the intervention group. Compared to the control group, however, only VO2max (intervention, MT3–1 = 2.04, SD = 2.34; control, MT3–1 = 0.55, SD = 2.57) and the postural stability score (intervention, MT3–1 = 0.1, SD = 0.41; control, MT3–1 = -0.06, SD = 0.45) improved in the intervention group.
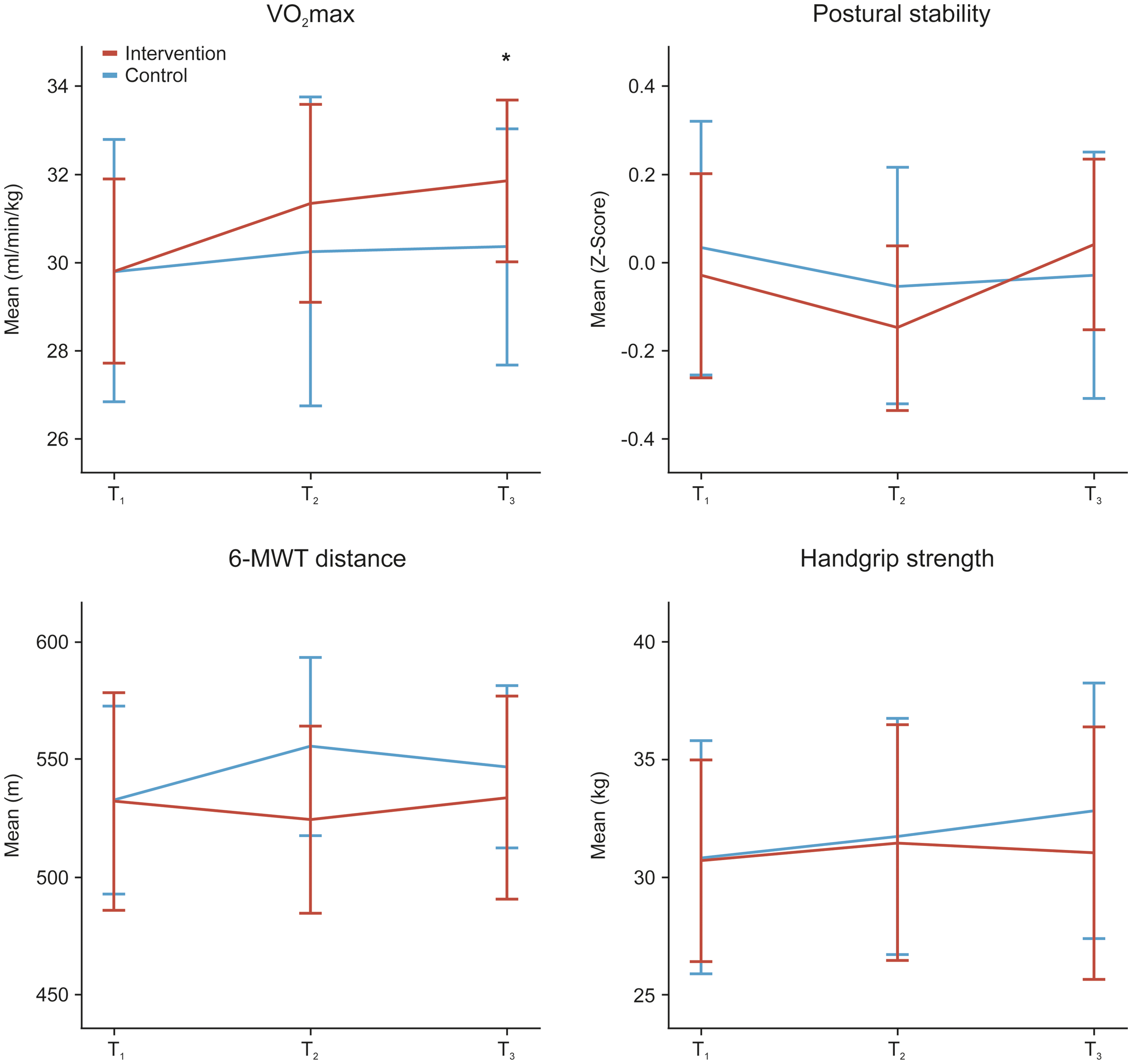
Development of fitness parameters assessed at all three visits (at baseline T1, T2, and T3) in both groups. Mean values are indicated, including the 95% confidence intervals, significant group difference in ΔVO2max in multiple linear regression analysis with p = 0.02, considering baseline VO2max and ΔPAQ50+ as covariables (see also Figure 5). There were no significant group differences concerning the other fitness parameters.
We then analyzed which factors positively predicted ΔVO2max in multiple linear regression analyses. As expected, ΔVO2max was significantly associated with an affiliation to the intervention group (t = 2.52, p = 0.02), furthermore with an increase of activity compared to before the intervention start as reflected by ΔPAQ50+T2/3–1 (t = 2.07, p = 0.05), and a lower baseline VO2max (t = -3.59, p = < 0.01) (see Figure 5). Regarding the additional fitness parameters, there were no group differences revealed in the regression analyses. A summary of all statistical models is available in Supplemental Table 4.

Multiple linear regression model of ΔVO2max. The unstandardized predicted values of the model, including group, baseline VO2max, and ΔPAQ50+ as significant predictors are plotted on the x-axis against ΔVO2max on the y-axis. Colors indicate data points of the intervention group in red and data points of the control group in blue, respectively. The model summary is included below, indicating the regression coefficient B, its 95% confidence interval (95% CI), the standardized regression coefficient β, the respective t value, and the significance level p for each predictor, as well as the overall model accuracy, including the effect size
No significant change was detected in the general activity levels, measured by diary MET, of participants affected by changes to the study protocol during the COVID-19 pandemic (z = -1.34, 95% CI (−3.08, 0.57), p = 0.26, r = 0.28), compared to those who were not affected. Furthermore, multiple regression analysis revealed no influence of the COVID-19 adjustment variable (Cov-19adj) on development of VO2max, 6-MWT distance, and postural stability, leading to its subsequent exclusion from the models. However, a certifiable beneficial effect on the development of handgrip strength could be reported for people being affected by the COVID-19 protocol changes (t = 2.35, p = 0.03). None of the participants in the exercise group presented clinical symptoms or were tested positive for COVID-19 during their six-month intervention period.
Influence of physical activity and fitness development on changes in neuropsychiatric symptoms, cognitive performance, and brain integrity
As mentioned before, baseline VO2max showed a negative association with ΔVO2max (r = -0.44, 95% CI [-0.66, −0.15], p = < 0.01) and was therefore initially regressed out from further analyses, applying the unstandardized residuals of ΔVO2max ∼ VO2maxT1 in subsequent regression analyses. Since both groups revealed differences in cognitive and educational status and potentially in the neurodegenerative markers from CSF at baseline, and to circumvent that baseline imbalances potentially hampered direct group comparisons (see Table 1B), we performed multiple linear regression analyses for disease outcome parameters separately in both groups. After screening the covariables, only the respective baseline levels of neuropsychiatric and cognitive parameters, showing a significant modifying effect, remained in the model; all other covariables were subsequently excluded to simplify the analysis. Interestingly, only in the intervention group CRF improvement did positively predict changes in MoCA (RMSE = 2.48, p = 0.03,
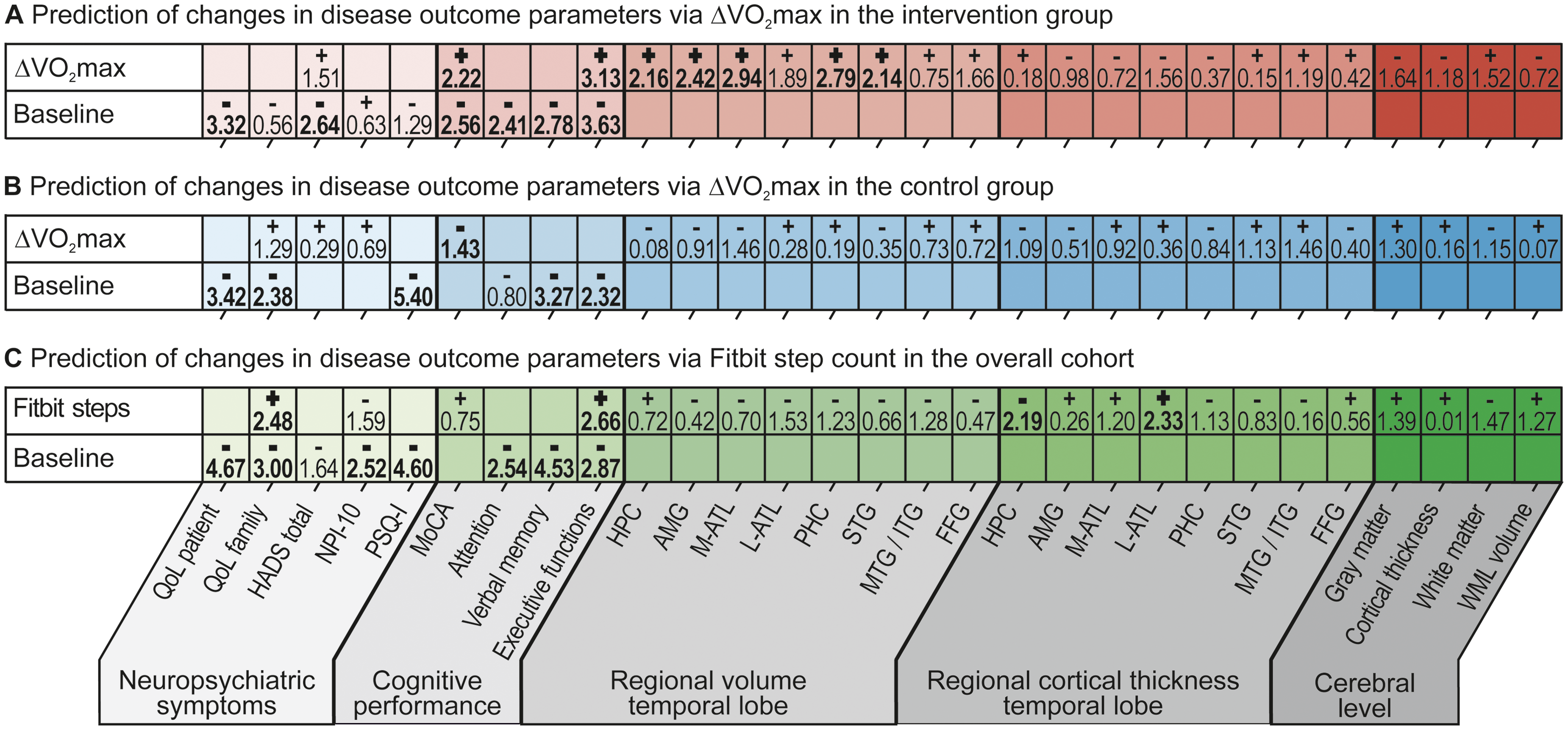
T-values of the regression analyses for predicting disease outcome parameters from changes in VO2max (i.e., ΔVO2max), separately in the intervention group (A) and the control group (B), and physical activity via Fitbit step count in the overall cohort (C). ΔVO2max was preliminary corrected for baseline VO2max in both groups by determining the residuals of the regression ΔVO2max ∼ VO2maxT1. For neuropsychiatric symptom and cognitive performance variables, baseline variables were additionally added to the model. The best models were chosen via comparison of R2, RMSE, and significance level. QoL: quality of life; HADS: Hospital Anxiety and Depression Scale; NPI-10: Neuropsychiatric Inventory; PSQ-I: Pittsburgh Sleep Quality Index; MoCA: Montreal Cognitive Assessment; HPC: hippocampus; AMG: amygdala; M-ATL: medial anterior temporal lobe; L-ATL: lateral anterior temporal lobe; PHC: parahippocampal and ambient gyri; STG: superior temporal gyrus; MTG/ITG: middle and inferior temporal gyri; FFG: fusiform gyrus; WML: white matter lesions.
As a second step, the influence of the physical activity level derived from Fitbit step count was analyzed on the outcome parameters, as this was shown to be the generally most reliable measurement of the Fitbit tracker in previous studies.68,69 Since mean activity levels via Fitbit recordings were similar between groups, we hypothesized that the influence of physical activity itself might differ from the immediate intervention effect reflected by the CRF improvement. Supporting this assumption, a small to moderate positive association was found between the Fitbit step count as the absolute physical activity level and baseline VO2max (ρ = -0.37, 95% CI (0.05, 0.62), p = 0.02), but not ΔVO2max (ρ = -0.15, 95% CI (−0.45, 0.18), p = 0.36). Again, multiple linear regression analyses were performed to analyze the influence of physical activity via Fitbit step count on disease outcome parameters in the overall cohort (n = 39) (Figure 6C). Higher physical activity levels were associated with an increased Quality of Life for caregivers (RMSE = 3.53, p = 0.01,
Whole-brain analysis revealed higher brain volume in the intervention group in the upper frontal brain lobe compared to the psychoeducation control group when taking MoCA and VO2max baseline levels, as well as education, as covariates into account at a liberal cluster threshold of p < 0.1 with n = 2000 permutations. There were no significant group clusters at a cluster threshold of p < 0.05 (see Figure 7).

Illustration of the TBM results from the voxel-wise permutation analysis at the whole- brain level, revealing higher brain volume in the upper frontal lobe in the contrast intervention group > control group with MoCA and VO2max at baseline and education as covariates, correction at the cluster-level at p < 0.1, n = 2000 permutations.
Discussion
This study presents the results of activity and fitness development from the Dementia-MOVE trial, a six-month multicomponent exercise intervention in AD. We examined the influence of CRF and physical activity on different clinical aspects of AD pathology, such as neuropsychiatric symptoms, sleep, quality of life, cognitive performance, as well as structural cerebral changes assessed by 3T MRI.
The physical activity and fitness assessment methods used in our study demonstrated high compliance with our protocol instructions, adhering to the current WHO recommendations on weekly activity rates for the elderly. 17 The physical activity assessment via wearable fitness trackers showed comparable physical activity levels between the intervention and the control group. However, the written diary revealed differences, particularly in the reporting of moderate activity levels. It, therefore, cannot be entirely ruled out that participants in the control group were more diligent and detailed in keeping the diary, especially when referring to moderate activities, compared to the intervention group, which might have focused more on the intensive training and its reporting. One might further argue that a difference in the cognitive state of the control group at baseline might lead to better activity reporting in the diaries in the control group. However, our findings did not show an association between cognitive state, as represented by the MoCA score, and compliance in keeping the diary in our sample.
We further analyzed the association between physical activity and CRF, represented by VO2max. As expected, high activity levels derived from the Fitbit were positively associated with VO2max from baseline, but not with ΔVO2max. Interestingly, participants with lower baseline CRF levels who successfully increased their physical activity levels, as indicated by the ΔPAQ50+T2/3−1 score, benefited the most from our multicomponent intervention program. They increased their VO2max, which had a positive effect on various AD progress parameters, including a positive mediating effect on regional brain structure and cognitive performance. Therefore, it can be assumed that, although there is a detectable positive influence of increased physical activity on CRF development, the individual baseline activity level must be considered separately concerning its influence on AD progression.14,70 CRF improvement itself, reflected by an increase in VO2max, was positively associated with an affiliation to the intervention group validating the effectiveness of our structured training concept for improving fitness in a sample of elderly and cognitively impaired participants. This aligns with previous findings emphasizing that increased physical activity is a crucial element to improve CRF, yet conveying its greatest effect through organized and regular training sessions of especially vigorous intensity,71,72 which, regardless of the average activity level, was only ensured in our intervention group. It could therefore be inferred that a specific level of activity at a specific intensity level is regularly required to produce benefits. This is underlined by the results of the intervention group, which showed a higher rate of activity on a vigorous level, while the control group engaged at a more moderate activity level, not revealing a significant impact. A positive trend was also reported regarding the development of postural stability, a domain that was actively trained in our program, which should be recommended even apart from its sheer effect on AD progression as an important preventive measure to reduce the risk of falls. 73 On the other hand, there was no remarkable response in other fitness parameters that were not specifically addressed in our intervention program, such as handgrip strength and the 6-MWT distance. A beneficial effect of the COVID-19 protocol changes on development of handgrip strength can probably be explained by training adjustments to home-based and space-restricted training forms with a focus on single muscle groups during the lockdown.
We further analyzed how VO2max improvement and average activity levels influenced AD outcome parameters. A modifying beneficial effect of CRF improvement was only observed in the intervention group that successfully increased VO2max over the course of the intervention period, supporting previous findings that demonstrated an effect of exercise-induced CRF increase on cognitive performance and AD-affected brain regions of the temporal lobe. This effect could be related to a combination of reduced brain inflammation, higher brain reserve, and reduced brain damage in terms of reduced vascular, neurotoxic, or oxidative stress, 74 leading to a reduced cellular loss and, therefore, maintained brain volumes and cortical thickness. Additionally, we were able to validate the previously described beneficial effects of VO2max improvement on cognitive performance, 75 as represented in the MoCA and executive functions composite score in the intervention group. Further negative associations with included baseline levels as non-specific progress markers for neuropsychiatric and cognitive parameters suggest that clinically more severely affected individuals of our sample were able to benefit more from the intervention in combination with their thereby achieved fitness improvement.64,76 However, there was no clear beneficial effect of CRF improvement on neuropsychiatric symptoms which has been reported in previous studies.77,78 In contrast, we found higher activity levels associated with increased quality of life for caregivers, highlighting another quality sign of multicomponent intervention concepts, by effectively relieving caregivers and offering space for discourse of likewise affected people and their relatives, even if this effect was not significantly reflected by the participants themselves. 79 Not only CRF, but also high physical activity led to a beneficial effect on the executive functions in the overall sample, pointing out that not only CRF increase but also physical activity on a regular base itself contributes to a positive development of cognitive performance in AD. This beneficial effect on executive functions is also reflected on the brain level, where our brain voxel-wise permutation analysis points at positive volume effects in frontal brain regions in trend. Recent research has pointed to an assumed predominant effect of multicomponent exercise on executive functions which is also in line with our cerebral findings of effects in the frontal lobe. 80 There was no beneficial effect of physical activity and CRF on vascular lesions, which one would assume given the positive mediating influence of these factors on the cardiovascular risk profile. 62 However, it might be the case that the intervention period of six months is too short to observe large effects in vascular changes on the cerebral level but would rather be observed on long-term outcomes.
In conclusion, we demonstrated that our multicomponent exercise intervention design can be an effective method to improve CRF in a sample of people affected with AD, especially for those with previously low fitness levels after six months of intervention. VO2max improvement was associated with advantageous developments in cognitive performance and a positive mediating effect on brain structure in AD-relevant regions of the temporal lobe in the intervention group, while negative associations with cognitive baseline levels suggest a higher benefit for people with more cognitive impairment. Furthermore, we found high levels of physical activity to be associated with increased cognitive performance, sustained cortical thickness in the temporal lobe area, and higher quality of life in caregivers of AD-affected individuals, marking another crucial domain to reduce the disease burden through physical interventions.
Even though there was a randomization process before group allocation, group differences occurring at baseline in single assessment parameters are inevitable, and our intervention group may have been more strongly affected by AD pathology based on their initial CSF status at the time of diagnosis and cognitively more impaired and with a lower cognitive reserve compared to the control group, pointing to differences in the MoCA score, the executive function, and the education level at baseline. This was taken into account in our statistical analyses, and we excluded a significant influence of these potential confounding factors on the outcome parameters. Still, this aspect has to be considered when looking at absolute outcome parameters beyond the change from pre- to post-intervention state alone. As suggested by previous publications, it is presumably challenging to account for all potential confounding factors during a temporary intervention, which may influence the outcomes and hinder direct comparisons between groups. In addition, we encountered minor fluctuations in protocol adherence due to medical issues related not only to the underlying disease but also expected in interventions involving an older population. Furthermore, necessary adjustments to the protocol were required during the COVID-19 lockdown. Nevertheless, a strong point of the present sample is the very detailed clinical characterization, which is often lacking in previously reported studies. 11 Considering the current body of research and the mentioned limitations, which are common in interventional research, our study demonstrates the positive influence of both physical activity and fitness improvement on AD pathology. The underlying effects on the cerebral level should be considered multifactorial and will need to be the subject of preclinical and clinical intensive research in the future. 81 Our study provides an important gain in knowledge on the rarely considered relationship between fitness and physical activity, both of which should be taken into account according to our study results. The present study has a limited sample size, which was based on initial power analyses related to our primary outcome parameter (see also 62 ). However, it can support the design of future intervention studies, which should also include well-characterized samples, as in the present study, and additionally incorporate larger sample sizes, longer intervention periods, and long-term follow-ups to enable subgroup analyses and compensate for group differences that might influence the outcomes, particularly concerning baseline cognition, fitness, activity levels, and differences in AD pathology, which might influence the distinct response to intervention effects.
According to our findings, which show a positively mediating influence of cardiovascular fitness and physical activity on several disease outcome parameters in AD, regular, structured exercise and activity increase in people affected by AD should be aimed at, both for primary and secondary prevention. Additionally, the intensity of physical activity must always be considered. Connection to professional, multicomponent training programs should be established early in the disease, but it is also highly effective for people with advanced disease manifestations, as shown in our study, and is therefore never too late.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241303764 - Supplemental material for Modulating effects of fitness and physical activity on Alzheimer's disease: Implications from a six-month randomized controlled sports intervention
Supplemental material, sj-docx-1-alz-10.1177_13872877241303764 for Modulating effects of fitness and physical activity on Alzheimer's disease: Implications from a six-month randomized controlled sports intervention by Shari David, Ana S Costa, Christian Hohenfeld, Sandro Romanzetti, Shahram Mirzazade, Jennifer Pahl, Luisa Haberl, Kai M Schneider, Axel Kilders, Thomas Eggermann, Christian Trautwein, Frank Hildebrand, Jörg B Schulz, Kathrin Reetz and Alexa Haeger in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors thank the team from the physiotherapy department at RWTH Aachen University Hospital, especially Rudolph Schifflers and David Uebis, as well as Gökhan Giray and Rebecca Schulze from the MedAix physiotherapy practice in Simmerath for their assistance during the intervention, and Michael Beulertz for his assistance in data acquisition. The authors also thank Prof. Ingo Kurth from the Department of Human Genetics at RWTH Aachen University for his support in ApoE-analysis. This work was supported by the Brain Imaging Facility of the Interdisciplinary Center for Clinical Research (IZKF) Aachen within the Faculty of Medicine at RWTH Aachen University.
Author contributions
Shari David (Data curation; Formal analysis; Investigation; Supervision; Visualization; Writing – original draft; Writing – review & editing); Ana S Costa (Conceptualization; Investigation; Methodology; Writing – review & editing); Christian Hohenfeld (Formal analysis; Software; Writing – review & editing); Sandro Romanzetti (Data curation; Writing – review & editing); Shahram Mirzazade (Investigation; Writing – review & editing); Jennifer Pahl (Investigation; Writing – review & editing); Luisa Haberl (Investigation; Writing – review & editing); Kai M Schneider (Resources; Writing – review & editing); Axel Kilders (Investigation; Writing – review & editing); Thomas Eggermann (Resources; Writing – review & editing); Christian Trautwein (Resources; Writing – review & editing); Frank Hildebrand (Resources; Writing – review & editing); Jörg B Schulz (Conceptualization; Resources; Writing – review & editing); Kathrin Reetz (Conceptualization; Investigation; Project administration; Supervision; Writing – review & editing); Alexa Haeger (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Validation; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project was funded by RWTH-Startup granted to AH (StUpPD_329-18) and further supported by the Stiftung Universitätsmedizin Aachen. SD and LH were funded by the IRTG Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – 269953372/GRK2150. This research project was supported by the Rotation Program and Short Term Program of the Faculty of Medicine RWTH Aachen University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.