
Abstract
Background
Although previous studies have shown that cognitive decline in Alzheimer's disease (AD) is associated with various risk factors, they primarily focused on late-onset AD (LOAD).
Objective
We aim to evaluate the differential impact of risk factors on the cognitive decline between early-onset AD (EOAD, onset < 65 years) and LOAD (onset
Methods
Using data from 212 EOAD and 1101 LOAD participants in the Alzheimer's Disease Neuroimaging Initiative (ADNI), we conducted multivariable mixed-effect models to evaluate the impact of APOE ε4, education, hypertension, diabetes, dyslipidemia, and body mass index on cognitive performance. Preprocessed MRI data were utilized for longitudinal parametric mapping.
Results
APOE ε4 carriers in both groups showed significantly accelerated declines in language, verbal memory, executive function, and general cognition. By controlling other significant risk factors, APOE ε4 carriers showed faster declines in language and verbal memory in both groups. Females exhibited accelerated declines in Language and verbal memory in the EOAD and LOAD cohorts respectively. LOAD individuals with hypertension showed faster declines while overweight and obese participants displayed slower declines in both cohorts across all domains except visuospatial. Notably, APOE ε4 status was associated with longitudinal cortical atrophy in the LOAD cohort but not in the EOAD cohort.
Conclusions
Known risk factors for AD were associated with cognitive decline in both EOAD and LOAD cohorts.
Introduction
Alzheimer's disease (AD), ranked among the top ten causes of death in the United States, is a progressive and irreversible neurodegenerative disorder with no known cure. Its hallmark features include early memory decline followed by impairments in language, executive function, and visuospatial skills. AD is often divided into two groups based on the age of onset: early-onset (EOAD, onset <65 years of age) and late-onset AD (LOAD, onset
Risk factors for AD have been extensively studied in LOAD. However, their association with the rate of cognitive decline in EOAD has not been extensively investigated previously. The apolipoprotein E (APOE ε4) allele has been identified as the primary genetic risk factor for AD. As an important mediator of AD susceptibility, its presence is strongly associated with greater brain atrophy in the medial temporal lobe, leading to greater memory impairment and accelerated cognitive decline. 7 Low education levels have also been identified as a risk factor for dementia. According to the cognitive reserve theory, individuals with limited education may struggle to manage pathological burdens effectively, resulting in a lower threshold for experiencing dementia symptoms. 8 Several other well-studied risk factors for AD include vascular risk factors such as obesity or being overweight, diabetes, hypertension, and dyslipidemia.9–14 Obesity, for instance, is reported to be associated with cognitive decline through its promotion of systemic inflammation. 15 Diabetes can cause hyperglycemia, which can deteriorate cognitive function, potentially leading to AD development.16,17 Hypertension has been linked to increased amyloid-β (Aβ) plaque buildup, higher parahippocampal neurofibrillary tangle density, and in vivo brain imaging markers of Aβ deposition. 18 While the precise mechanisms of how cholesterol influences AD remain unclear, evidence from genetic, cellular, epidemiological, and animal studies supports the association between dyslipidemia and dementia and AD development. 19 APOE ε4 and the aforementioned metabolic risk factors continue to gain importance for risk assessment in a broad AD population.
To date, the majority of investigations have focused on LOAD, with limited published research examining the association of these risk factors with cognitive decline in EOAD. In this paper, we aimed to investigate the influence of APOE ε4 and vascular risk factors on cognitive decline in both EOAD and LOAD, using data from the Alzheimer's Disease Neuroimaging Initiative (ADNI) study. Additionally, we further investigate the longitudinal effects of APOE on cortical atrophy in both variants of the disease.
Methods
Participants
Data from the Alzheimer's Disease Neuroimaging Initiative (ADNI) study were utilized in this analysis and were obtained from the ADNI database (http://adni.loni.usc.edu). All diagnostic criteria can be found on ADNI's website under the clinical protocol documents and the list of inclusion/exclusion criteria can be accessed in the ADNI procedures documents (http://adni.loni.usc.edu/methods/documents/). Written and informed consent was obtained from all participants. Our analyses included subjects diagnosed with AD or mild cognitive impairment (MCI) at baseline with at least one follow-up visit. In total, 1313 subjects (9408 visits) were analyzed. Age of onset was defined as the earliest time of cognitive symptoms in confirmed AD/ MCI subjects. Using the age of onset of 65 as a cut-off point, 333 subjects were categorized as EOAD, while 980 were classified as LOAD patients. Among all patients, 355 of them (22.82% EOAD versus 28.47% LOAD) were diagnosed with AD at baseline. In 258 participants where the age of onset was unavailable, age at baseline was used as onset times.
Cognitive outcomes
In addition to assessing general cognition using the Mini-Mental Status Examination (MMSE), 20 our study focused on evaluating specific cognitive domains. Language function was assessed using the Boston Naming Test (BNT), 21 visuospatial function was evaluated using Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog) constructional praxis score,22,23 verbal memory function was measured by summing the scores of Word recall (ADAS-WRT), Naming (ADAS-Naming), and Word recognition (ADAS-Word), and executive function assessed by using the category fluency (CFanimals) test. To maintain consistency with other cognitive endpoints, we have inverted the ADAS-Cog scores for each test question to reflect the correctness of the items. In this way, a higher score indicates better performance. To address the age difference between EOAD and LOAD, each test variable was standardized by the mean and standard deviation of the corresponding test scores obtained from normal participants younger than 65 for the EOAD group and those older than 65 for the LOAD group without cognitive impairment at baseline, respectively.
Risk factors
In the current study, we evaluated potential risk factors including the APOE ε4 carrier status, gender, education level, comorbidities (hypertension, diabetes, dyslipidemia), and body mass index (BMI).
APOE genotyping procedures are detailed at https://adni.loni.usc.edu/. APOE ε4 carrier status was categorized as “non-carrier” for individuals lacking APOE ε4 alleles and as “carrier” for those with either one or two APOE ε4 alleles.
Statistical analyses
To compare baseline characteristics between EOAD and LOAD participants, we employed two-sample t-tests for continuous variables and Fisher's exact tests (or Chi-square tests) for categorical variables. For each cognitive domain, the scores of EOAD and LOAD participants were standardized using the means and standard deviations from cognitively normal participants in the corresponding age groups in ADNI. We reported both original cognitive scores and standardized scores, although only standardized scores were utilized for subsequent analyses.
First, to evaluate the impact of each risk factor on cognitive decline in both EOAD and LOAD patients, mixed effect models with two-way interaction (risk factor*time) were conducted. Each model included baseline age, time, a single risk factor, and risk factor*time as fixed effects. Additionally, random intercepts and random slopes were included in each model. The significance of the risk factor by time interaction term indicates an association between the risk factor and cognitive decline over time.
Second, to evaluate the influence of each risk factor on the rate of cognitive decline in both EOAD and LOAD patients while controlling for other risk factors, multivariable analyses with two-way interaction (risk factors*time) were conducted. Risk factors that demonstrated interaction significance in the single risk factor models (p < 0.05) were included in the multivariable models. These models included baseline age, time, risk factors, and the interaction between risk factors and time (risk factors*time) as fixed effects. The same random effects as those used in the univariable analyses were used.
Finally, we examined whether each risk factor had differential effects on cognitive decline between EOAD and LOAD patients while controlling for other risk factors. To achieve this, multivariable mixed effects models with three-way interactions (risk factor*time*group) were performed. These models included baseline age, time, group, risk factors, two-way interactions (risk factor*time, risk factor*group, group*time), and a three-way interaction (risk factor*time*group) as fixed effects. The same random effects as those used in the previous models were retained. Risk factors that demonstrated interaction significance in univariable analyses (p < 0.05) were assessed in this evaluation.
All hypothesis tests were two-sided, and statistically significant was defined by a p-value < 0.05. SAS 9.4 was used for all analyses.
MRI acquisition and analyses
ADNI MRI acquisition and preprocessing protocols can be found at www.adni-info.org. T1 structural MRI scans were downloaded from LONI IDA (https://ida.loni.usc.edu) in NifTI format and analyzed using voxel-based morphometry (VBM) in SPM12.24,25 Briefly, baseline scans were co-registered to the Montreal Neurological Institute (MNI) space, while follow-up or longitudinal scans were co-registered to their corresponding baseline scan. MRIs were then segmented into gray matter (GM), white matter (WM), and cerebrospinal fluid (CSF) components, bias-corrected and spatially normalized. 26 Following this step, we used a nonlinear registration procedure, DARTEL, on each subject's GM and WM tissue maps, which iteratively matches a subject-specific mean template. 27 The resulting GM maps were then normalized to Montreal Neurological Institute (MNI) space as 1 × 1 × 1 mm voxels and smoothed using 10 mm full-width half maximum (FWHM) Gaussian kernel which yielded gray matter density images to be used in imaging analysis. Volumetric measures for MRI, such as intracranial volume (ICV), were obtained from the ADNI standardized MRI data sets on LONI IDA.28–30
Longitudinal parametric mapping
To visualize the longitudinal neurodegenerative effects of APOE ε4 in 3D, we relied on the Sandwich Estimator (SwE) SPM toolbox. 31 SwE not only has the flexibility to handle an unbalanced dataset but also the ability to estimate a covariance matrix, overcoming traditional pitfalls seen by spatially homogenous correlation assumptions. 31 Scans up to 48 months were selected to analyze the effect of the APOE ε4 carrier status (ε4 carrier or ε4 non-carrier) in EOAD and LOAD cohorts separately, controlling for age, sex, intracranial volume (ICV), and field strength. All longitudinal results are displayed at a false discovery rate (FDR) of p < 0.05.
Sensitivity analyses
We conducted sensitivity analyses to assess the potential impact of inadvertently including EOAD participants in the LOAD group due to limited data on the onset of cognitive decline in some LOAD patients. We excluded LOAD patients aged between 65 and 70 (inclusive). All statistical models and MRI analysis methods used in the subsample were identical to those applied in the main analyses.
Results
Demographics and baseline characteristics of participants
Table 1 provides an overview of the baseline characteristics and demographics of the participants. LOAD patients exhibited a significantly lower level of education compared to EOAD patients (LOAD versus EOAD: 20.10% versus 12.31% with ≤12 years of education, p < 0.001). Additionally, LOAD patients had a higher percentage of hypertension compared to EOAD patients (LOAD versus EOAD: 33.33% versus 18.06%, p < 0.001). Original scale scores for language, verbal memory, executive function, and MMSE were lower in LOAD participants than in EOAD patients (LOAD versus EOAD: BNT 24.79 ± 4.78 versus 26.44 ± 4.18, p < 0.001; summing scores of ADAS-WRT, ADAS-Naming, and ADAS-Word 25.18 ± 8.9 versus 28.67 ± 10.14, p < 0.001; CFanimals 15.4 ± 5.39 versus 17.46 ± 5.67, p < 0.001 and MMSE 26.25 ± 2.68 versus 26.97 ± 2.81, p < 0.001). However, no significant differences were observed between the two groups in standardized cognitive scores, except for language and executive function scores, where LOAD participants had higher language scores and lower executive function scores than EOAD participants (LOAD versus EOAD: BNT −1.55 ± 2.21 versus −1.94 ± 3.73, p = 0.032; CFanimals −1.06 ± 0.98 versus −0.93 ± 0.96, p = 0.033). Notably, LOAD participants have significantly shorter years from the age of onset (i.e., disease duration) than EOAD participants (LOAD versus EOAD: 6.14 ± 3.83 versus 9.15 ± 5.54, p < 0.001).
Baseline demographics and cognitive scores of individuals with Alzheimer's disease by onset age.

Bold values denote statistical significance.
The effects of risk factors on cognitive decline in EOAD and LOAD
Single risk factor models
We conducted univariable analyses for both EOAD and LOAD patients to identify significant risk factors for further multivariable analyses. The effects of each risk factor on cognitive decline in both cohorts are presented in Supplemental Table 1.
Multivariable analyses in EOAD
Multivariable models for both EOAD and LOAD are presented in Table 2. In EOAD, APOE ε4 carriers showed a faster decline in language (p < 0.001), visuospatial (p = 0.007), verbal memory (p < 0.001), executive function (p < 0.001), and MMSE (p < 0.001) than non-carriers after adjusting for other risk factors. Overweight and obese patients displayed a slower cognitive decline in language (p = 0.003 and p = 0.011), verbal memory (p = 0.012 and p = 0.017), and MMSE (p = 0.003 and p < 0.001) than underweight or normal-weight patients. In addition, overweight patients also experienced a significantly slower decline in visuospatial (p = 0.022), and obese patients experienced a significantly slower decline in executive function (p = 0.029) than underweight or normal-weight patients. EOAD patients with hypertension significantly escalated cognitive decline in language (p < 0.001), executive function (p = 0.023), and MMSE (p < 0.001). EOAD patients with dyslipidemia showed a faster decline in visuospatial (p = 0.006).
Comparisons of risk factors for cognitive decline between EOAD and LOAD.
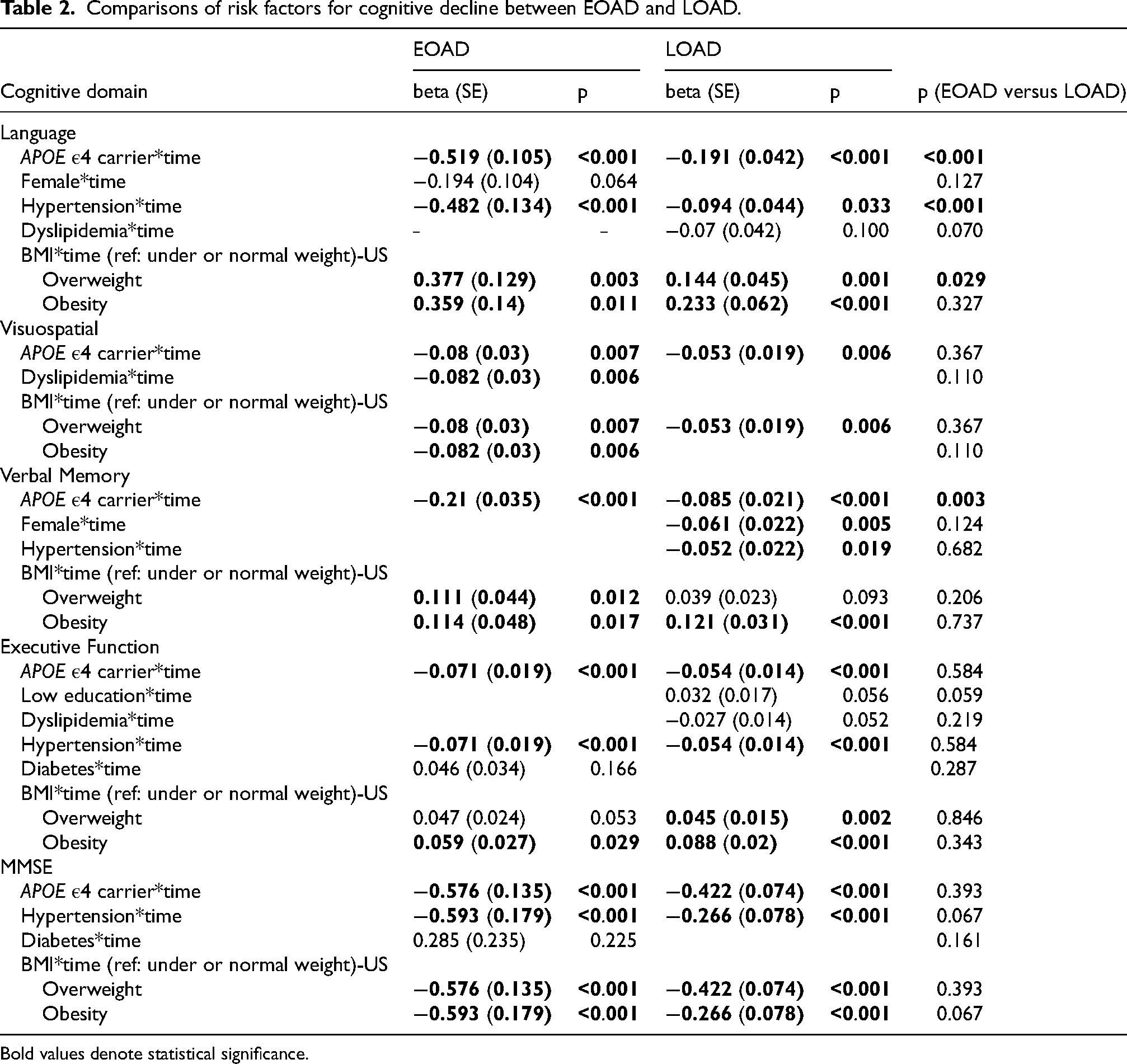
Bold values denote statistical significance.
Multivariable analyses in LOAD
In LOAD, multivariable analyses presented that APOE ε4 carriers showed a faster cognitive decline across all domains than non-carriers (language: p < 0.001; visuospatial: p = 0.006; verbal memory: p < 0.001, executive function: p < 0.001; MMSE: p < 0.001). Except for visuospatial and executive function, patients with hypertension showed a faster cognitive decline than patients without hypertension across all domains (language: p = 0.033; verbal memory: p = 0.019; MMSE: p < 0.001). While overweight and obese patients showed a slower cognitive decline than underweight or normal-weight patients in language, executive function, and MMSE (language: p = 0.001, p < 0.001; executive function: p = 0.002, p < 0.001; MMSE: p = 0.003, p < 0.001). Also, obese patients experienced a significantly slower decline in verbal memory (p < 0.001). Besides, female LOAD patients showed a faster decline in verbal memory than their male counterparts (p = 0.005).
Differential effects of risk factors on cognitive decline between EOAD and LOAD patients
Results of multivariable analyses in Table 2 showed that EOAD patients who are APOE ε4 carriers showed a significantly faster language and verbal memory decline compared to LOAD (p < 0.001 and p = 0.003) after controlling for other risk factors (Figure 1(a)–(e)). Moreover, patients with hypertension showed a significantly faster language decline compared to LOAD (p < 0.001). While overweight EOAD patients showed a significantly slower language decline than LOAD (p = 0.029). The effect of other risk factors on cognition was not significantly different between EOAD versus LOAD patients.

Changes in standardized cognitive scores of language (A), visuospatial (B), executive function (C), MMSE (D), and verbal memory (E), over time by APOE ε4 carrier status in EOAD and LOAD.
Longitudinal neurodegenerative effects of APOE in EOAD and LOAD
Based on the sandwich estimator results, APOE ε4 carrier status had no significant effect on longitudinal gray matter density in the EOAD cohort (Figure 2(b)). In contrast, in the LOAD cohort, APOE ε4 carriers showed greater longitudinal atrophy than ε4 non-carriers in the entorhinal cortex, anterior temporal lobe, anterior parahippocampal gyrus, and amygdala (Figure 2(a)).
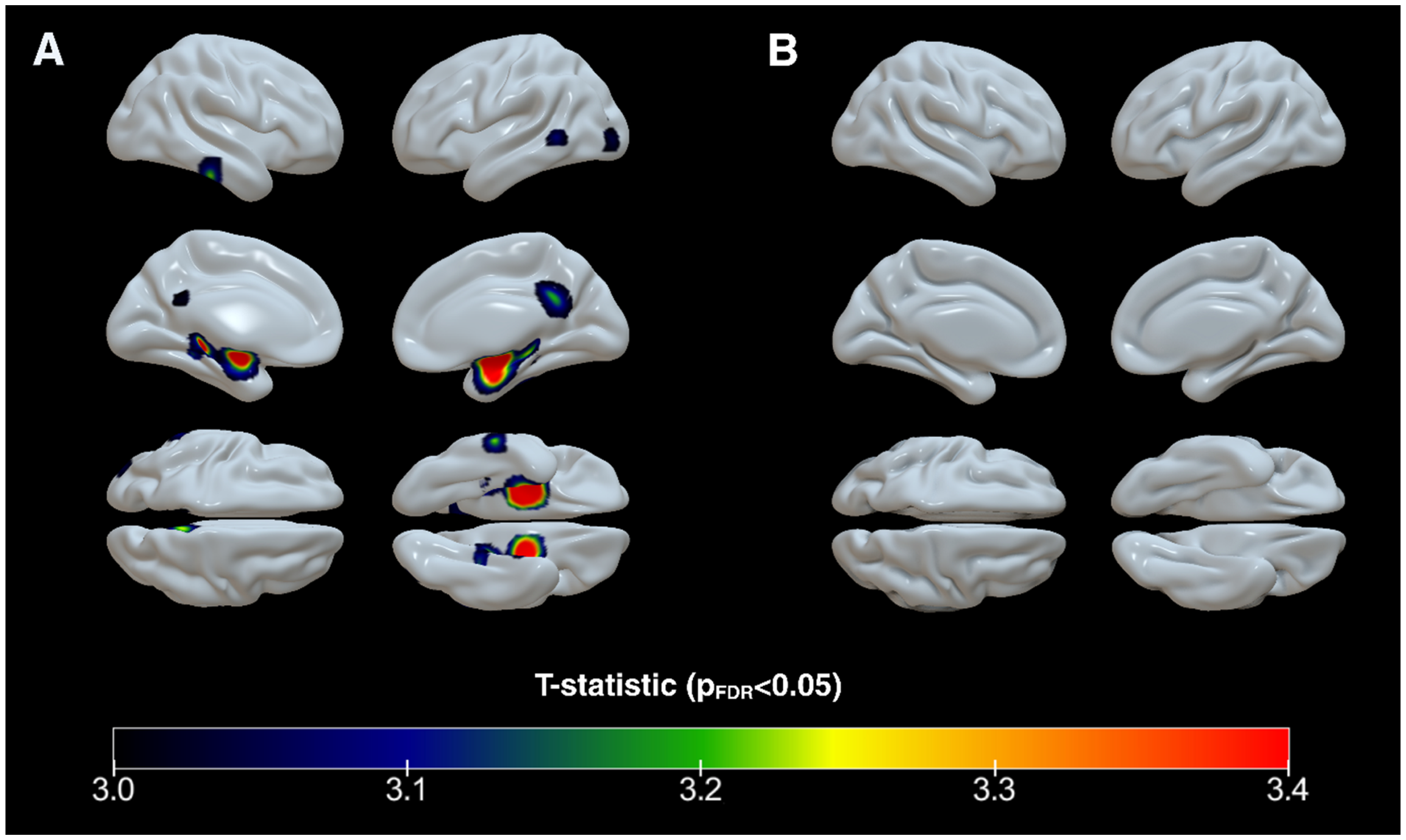
Statistical T-maps comparing the effect of APOE ε4 carrier status (carriers versus non-carriers) on longitudinal cortical atrophy in LOAD (A) and EOAD (B). All results are displayed at a false discovery rate (FDR) of p-value < 0.05.
Sensitivity analysis results
To reduce the likelihood of including potential EOAD participants in the LOAD group, we excluded LOAD patients aged 65 and 70 in our sensitivity analyses. The results were similar to those from the full sample, with differential APOE ε4 effects between EOAD and LOAD observed in both language and verbal memory domains. However, LOAD females showed a significantly faster decline in verbal memory than EOAD females, and the previously significant effect of being overweight on language between EOAD and LOAD was no longer significant when LOAD patients aged 65 to 70 were excluded. In the sensitivity analysis of longitudinal neuroimaging, unlike the main analysis, APOE ε4 carrier status did not significantly affect longitudinal gray matter density at an FDR correction threshold of p < 0.05. Detailed results are presented in Supplemental Tables 2–4 and Supplemental Figure 1.
Discussion
In our longitudinal analyses, we investigated the cognitive trajectories of two AD variants, EOAD and LOAD, for well-established risk factors for AD. Overall, the results show that APOE ε4 carriers exhibited significantly accelerated cognitive decline across multiple domains compared to non-carriers in both EOAD and LOAD. These results align with some but not all previously published studies. In 2009, Caselli et al. analyzed 815 subjects of the Arizona APOE cohort with a mean baseline age of 60.1 years and a mean follow-up of 5 years. They found that APOE ε4 homozygous experienced steeper cognitive decline, with no such effect observed in heterozygotes compared to APOE e4 non-carriers. 32 Similarly, another study involving 621 participants (mean age 58 years, follow-up 6 years) reported greater cognitive decline was observed only for APOE ε4 homozygotes. 33 A third study, assessing individuals from midlife to older age (43–69) from the National Survey for Health and Development, reported a dose-dependent cumulative negative effect of APOE ε4 on episodic memory. This effect was more evident in older ages. 34 Furthermore, as a multifactorial disease, other genetic and environmental exposures due to race, ethnicity, and cultural differences can affect the relationship between APOE ε4 exposure and disease. 35 Also, previous research found that frequencies of APOE ε4 alleles varied among ethnic groups. 36 In contrast to these findings, a study by Kim et al. among a Korean research cohort reported a slower cognitive decline in APOE ε4 carriers in EOAD but not in LOAD. 37 Our multivariable analyses detected significantly faster language and verbal memory declines in EOAD patients compared to LOAD concerning the APOE ε4 genotype in the ADNI cohort. We note that ADNI recruits only individuals with amnestic phenotypes, limiting the generalizability of our results to the broader EOAD and LOAD populations, which may include non-amnestic phenotypes and even younger EOAD participants (those younger than 55 years were excluded from ADNI). To address these limitations, ongoing studies like the Longitudinal Early-onset AD study (LEADS) will be able to address this research question 38
In our longitudinal imaging analyses, we found that compared to ε4 non-carriers, APOE ε4 carriers had a strong association with atrophy in the LOAD cohort only in the entorhinal, anterior temporal, anterior parahippocampal, and amygdala regions. Atrophy in these regions is consistent with previous findings in LOAD APOE ε4 carriers.7,39 Given the relatively late disease onset in our EOAD cohort (61.17 ± 2.73) we cannot be fully confident that the APOE ε4 effect on cognitive decline throughout the EOAD age spectrum is constant and whether these results are generalizable to the EOAD spectrum. Additionally, there may be other undiscovered genetic risk factors that drive longitudinal atrophy in EOAD. 40 These are questions that could be addressed by LEADS. 38
For the obesity risk factors, we found that BMI had a significant positive relationship with cognitive slopes for major domains in our analyses, suggesting a protective effect of higher BMI on cognitive decline in both cohorts. This is a somewhat counterintuitive observation since midlife obesity and being overweight are recognized risk factors for AD.41–43 A long preclinical phase precedes the clinical diagnosis of dementia (10–20 years) during which, cardiometabolic changes including weight loss are common.44,45 Thus, a plausible explanation might be the confounding effect of weight loss during the preclinical dementia phase, which can cause the higher BMI to appear protective via reverse causation. Moreover, we observed that the protective effect of being overweight or obese was stronger in EOAD.
Hypertension showed a significant association with cognitive decline in major domains in both EOAD and LOAD cohorts. The effects of hypertension on the brain are likely mediated by cerebral blood flow, endothelial damage, formation of atherosclerotic plaques, and sustained microvascular pressure changes all of which are pronounced in both cohorts. Further, a bidirectional link between AD pathology and hypertension (leading to cerebrovascular disease) might be a prominent driver for both EOAD and LOAD. 46
Women appeared significantly faster decline in verbal memory in LOAD only. These results are consistent with prior research that suggested that the verbal memory advantage of healthy older women was reserved in patients with AD, where men with AD displayed better verbal recall ability than women with AD. 47 It is also consistent with a more recent research report that women display a faster trajectory of memory decline in the setting of pathology. 48
Low education, dyslipidemia, and diabetes were not significant risk factors for cognitive decline in our analyses. It is worth noting that many of these risk factors were shown to be risk factors for cognitive decline in the general population, while our analyses focus on cognitive change after disease onset that may reflect different mechanisms involved for these risk factors. Our findings warrant further investigations in larger sample sizes with longer follow-up periods to better understand the differences as well as ascertain the relationship between these risk factors and age of onset.
In our study, we addressed prior limitations of the potential age difference between EOAD and LOAD cohorts by normalizing each cognitive outcome by using test scores from cognitively normal individuals. To the best of our knowledge, this is the first comprehensive investigation to systematically characterize the influence of APOE ε4, education, and vascular risk factors along with the onset period on cognitive decline in EOAD and LOAD patients in a North American population.
However, our analysis is not without limitations. The EOAD cohort within ADNI is smaller than the LOAD group, which limits the power to detect risk factors specific to the EOAD group. Furthermore, since only people older than 55 years with amnestic phenotype presentations are included in ADNI, a sizeable portion of both EOAD and LOAD populations are excluded from our analyses. To better generalize our findings to other populations, further investigations based on data with diverse inclusion and exclusion criteria are needed. Another limitation of our analyses is that some LOAD individuals lacked data on the onset of cognitive declines. For these individuals, age at baseline was substituted for age at cognitive decline thus some EOAD might have been inadvertently classified as LOAD. Sensitivity analyses excluding potential EOAD participants from the LOAD group showed that, while most major results remained consistent, some findings changed after excluding LOAD participants aged 65 to 70. It is important to note that this exclusion also reduces the power of the analysis, making it unclear whether the differences in results are due to removal of potential EOAD participants or to the reduction in power. Further research with more accurate data on the age of onset for both EOAD and LOAD is needed to confirm these findings. Lastly, although our analyses considered several risk factors, we may have not included all potential risk factors for cognitive decline in these two age groups. 34 Also, more studies are needed to explore how changes in vascular risk conditions (e.g., treated versus untreated) and other risk factors over time will influence longitudinal cognitive outcomes.
In summary, our longitudinal analyses of cognitive decline in EOAD and LOAD cohorts with respect to well-established risk factors in the ADNI study showed that APOE ε4 carriers had a faster decline in multiple cognitive domains than non-carriers in both EOAD and LOAD. Our results need to be confirmed in other longitudinal studies of EOAD and LOAD.
Supplemental Material
sj-pdf-1-alz-10.1177_13872877241307321 - Supplemental material for Effect of genetic and vascular risk factors on rates of cognitive decline in early-onset and late-onset Alzheimer's disease
Supplemental material, sj-pdf-1-alz-10.1177_13872877241307321 for Effect of genetic and vascular risk factors on rates of cognitive decline in early-onset and late-onset Alzheimer's disease by Yunyi Li, Apoorva Bharthur Sanjay, Mohit Manchella, Aryan Mishra and Paige E Logan, Hee Jin Kim, Shannon L Risacher, Sujuan Gao, Liana G Apostolova, in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
Data collection and sharing for the Alzheimer's Disease Neuroimaging Initiative (ADNI) is funded by the National Institute on Aging (National Institutes of Health Grant U19AG024904). The grantee organization is the Northern California Institute for Research and Education. In the past, ADNI has also received funding from the National Institute of Biomedical Imaging and Bioengineering, the Canadian Institutes of Health Research, and private sector contributions through the Foundation for the National Institutes of Health (FNIH) including generous contributions from the following: AbbVie, Alzheimer's Association; Alzheimer's Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics.
Authors contributions
Yunyi Li (Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Apoorva Bharthur Sanjay (Project administration; Software; Visualization; Writing – original draft; Writing – review & editing); Mohit Manchella (Visualization); Aryan Mishra (Visualization); Paige E Logan (Software; Visualization; Writing – review & editing); Hee Jin Kim (Conceptualization; Writing – review & editing); Shannon L Risacher (Validation); Sujuan Gao (Conceptualization; Funding acquisition; Methodology; Supervision; Writing – review & editing); Liana G Apostolova (Conceptualization; Funding acquisition; Supervision; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is supported by the following grants: U01AG057195, P30AG072976, and K07AG076659.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.G.A. has provided consultation to Eli Lilly, Biogen, Genentech, GE Healthcare, Eisai, Roche Diagnostics, Siemens, Alnylam, Corium, Otsuka, Two Labs, FL Dept Health, and the NIH Biobank. LGA receives the following research support: NIA U01 AG057195, NIA R01 AG057739, NIA P30 AG010133, Alzheimer Association LEADS GENETICS 19-639372, Alzheimer Association SG-23-1061716, Roche Diagnostics RD005665, AVID Pharmaceuticals and Life Molecular Imaging. LGA has received honoraria for participating in independent data safety monitoring boards and providing educational CME lectures and programs.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.