
Abstract
Background:
Previous cross-sectional studies have identified a possible link between Helicobacter pylori (H. pylori) infection and dementia. However, the association of H. pylori infection with longitudinal cognitive decline has rarely been investigated.
Objective:
This cohort study aims to demonstrate the effects of H. pylori infection on longitudinal cognitive decline.
Methods:
This cohort study recruited 268 subjects with memory complaints. Among these subjects, 72 had a history of H. pylori infection, and the rest 196 subjects had no H. pylori infection. These subjects were followed up for 24 months and received cognitive assessment in fixed intervals of 12 months.
Results:
At baseline, H. pylori infected, and uninfected participants had no difference in MMSE scores. At 2 years of follow-up, H. pylori infected participants had lower MMSE scores than uninfected participants. H. pylori infection was associated with an increased risk of longitudinal cognitive decline, as defined by a decrease of MMSE of 3 points or more during follow-up, adjusting for age, sex, education, APOE ɛ4 genotype, hypertension, diabetes, hyperlipidemia, and smoking history (HR: 2.701; 95% CI: 1.392 to 5.242). H. pylori infection was associated with larger cognitive decline during follow-up, adjusting for the above covariates (standardized coefficient: 0.282, p < 0.001). Furthermore, H. pylori infected subjects had significantly higher speed of cognitive decline than uninfected subjects during follow-up, adjusting for the above covariates.
Conclusion:
H. pylori infection increases the risk of longitudinal cognitive decline in older subjects with memory complaints. This study is helpful for further understanding the association between infection and dementia.
INTRODUCTION
Dementia affects approximately 55 million people globally and has emerged as one of the leading causes of disability and mortality among older adults [1]. The most prevalent type of dementia is Alzheimer’s disease (AD), which is a devastating neurodegenerative disease with no disease-modifying treatment currently [2, 3]. In the past decades, a panel of risk factors for dementia have been figured out, such as hypertension, diabetes mellitus, unhealthy lifestyles, and changes in body mass index [4–6]. More comprehensive understanding of the risk factors for dementia is of significance for developing interventions to halt cognitive decline.
Infection is a well-established risk factor for dementia, including AD, vascular dementia, and other types of dementia [7]. Recent studies have shown that viruses, such as Herpes simplex, human cytomegalovirus, Epstein-Barr virus, and SARS-CoV-2, bacteria, such as Treponema pallidum, Borrelia burgdorferi, and chlamydia may factor into cognitive decline [8–15]. Chronic Helicobacter pylori (H. pylori) infection is prevalent in human, especially in Asian populations [16]. Previous reports about the association between H. pylori infection and dementia obtained inconsistent findings [17], and most investigations were conducted in cross-sectional study design. Therefore, it is necessary to determine the association of H. pylori infection and longitudinal cognitive decline. Based on this consideration, we performed this 2-year follow-up study in a cohort of patients with memory complaints to determine the effects of H. pylori infection on long-term cognitive decline.
METHODS
Participants
We screened patients with subjective memory complaints within the past one year who visited the Department of Neurology, Sichuan Provincial People’s Hospital, during February 11, 2018, and July 16, 2019. H. pylori infectious status was confirmed by the 14 C urea breath test. Participants were categorized into the infected and uninfected group according to their 14 C test. All infected participants received H. pylori eradication upon diagnosis. The inclusion criteria were: 1) had subjective memory complaints; 2) aged 60 years or above; 3) could complete the cognitive assessment; 4) willing to participate in this study. Subjects were excluded if they have one or more of the following conditions: 1) diagnosed with any other types of chronic infection, such as herpes simplex, human immunodeficient virus (HIV), and hepatitis; 2) had hepatic, renal, or heart failure; 3) had co-existing diseases that may affect cognition (such as hepatic encephalopathy, central nervous system infection, autoimmune encephalitis, etc.); 4) unable to complete the cognitive assessment due to hearing, visual, or language problems; 5) not willing to participate. All participants were tested for H. pylori infection at one year and two years of follow-up. No patient had previously diagnosed H. pylori infection in this cohort. It also is notable that uninfected subjects were excluded if they were infected with H. pylori during follow-up. Written informed consent for participation was obtained from all participants or their legal relatives prior to the study. The research protocols of this study were approved by the ethics committee of Sichuan Provincial People’s Hospital.
Brain imaging and cognitive assessment
All participants, including both H. pylori-infected and uninfected subjects, received a magnetic resonance imaging (MRI) scan of the brain. The cognitive functions of participants were first assessed using the Mini-Mental State Examination (MMSE). Participants with a MMSE score below 27 further received a clinic dementia rating (CDR) test to determine the severity of cognitive impairment. All participants received cognitive assessment at 12 and 24 months since their first visit.
Statistical analysis
For the sociodemographic information and clinical characteristics, continuous variables were described as median and IQR or means and standard deviation (SD), and categorical data were summarized as absolute frequencies and percentages. Intergroup p-values were determined via independent samples t-test, Mann-Whitney Test, or χ2 test where appropriate.
The association between H. pylori infection and the severity of cognitive decline during follow-up, as reflected by the decrease of MMSE, was determined by a linear mixed effects model, with adjustment of age, sex, education, APOE ɛ4 genotype, hypertension, diabetes mellitus, hyperlipidemia, and smoking history. A multivariate logistical regression model was also hired to investigate the association between H. pylori infection and longitudinal cognitive decline, which is defined by a decrease of 3 points or more in MMSE [18, 19]. Furthermore, a mixed linear effects model was used to compare the slope of cognitive decline between H. pylori infected and uninfected participants, adjusting for the above covariates. Statistical analyses were conducted using SPSS statistical package version 25 and R version 3.6.2. Tests were 2-tailed, and significance was set at p < 0.05.
RESULTS
Clinical characteristics of participants
This cohort study screened 336 subjects with memory complaints during the past one year before hospital visit. Among these subjects, 37 subjects were not willing to participate, 11 subjects had hearing or visual problems that may confounder the outcomes of cognitive assessment, 3 subjects had renal failure, and 1 subject was infected with hepatitis B. During follow-up, 13 participants were lost, and 3 participants deceased. Finally, 268 subjects completed the 2-year follow-up (Fig. 1). Among these participants, 72 participants were infected with H. pylori and all infected participants received eradication therapy. The rest 196 participants had no history of H. pylori infection and tested negative for H. pylori at baseline. The H. pylori-infected and uninfected group had no difference in age, sex, education level, proportion of APOE ɛ4 carriers, frequencies in hypertension, diabetes mellitus, hyperlipidemia, stroke, and proportion of smokers (Table 1). These findings suggest that the two groups had comparable clinical parameters at baseline.
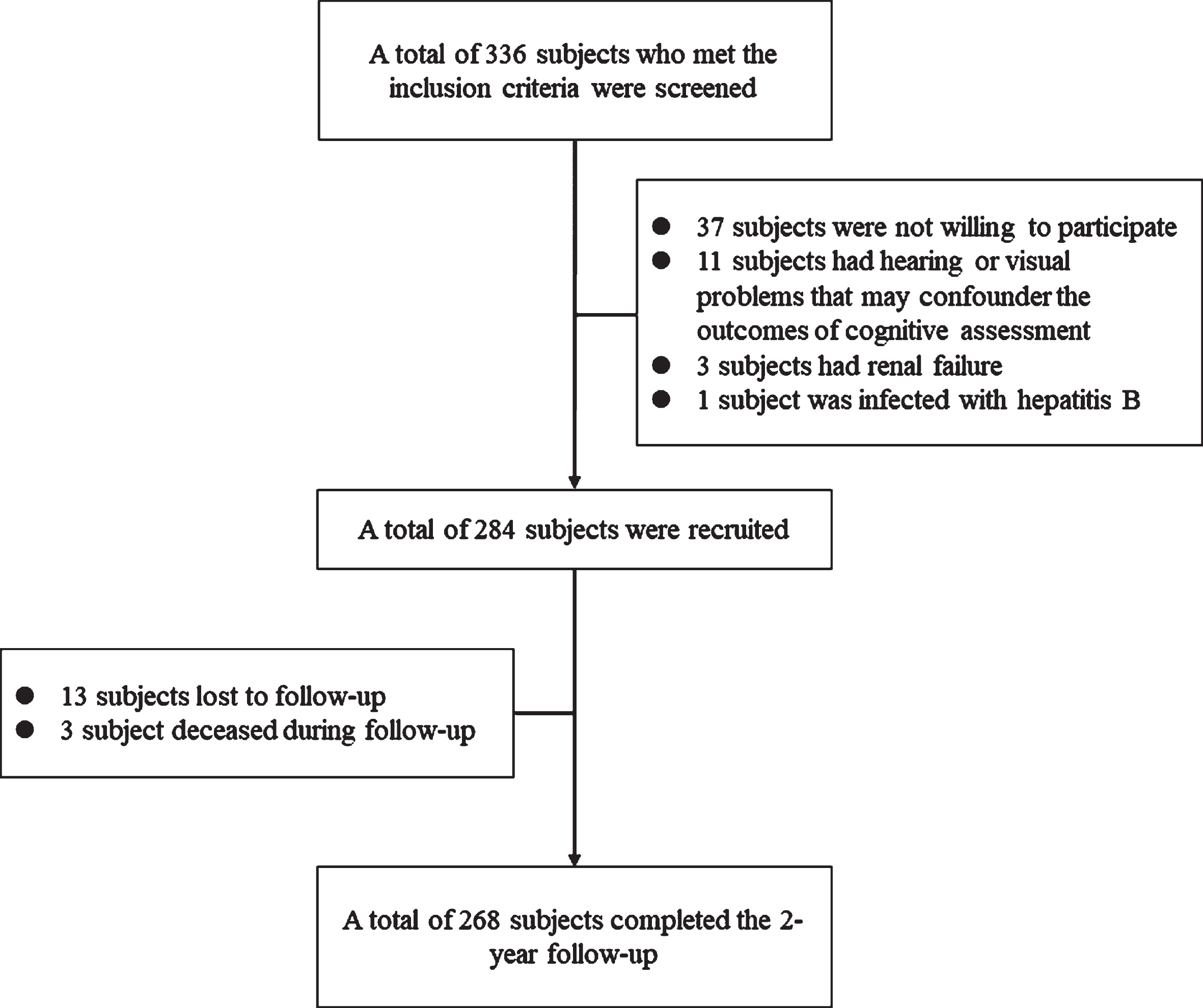
Study flowchart.
Demographic information of participants
HP, Helicobacter pylori; MMSE, Mini-Mental State Examination. a Mann-Whitney Test. b Fisher’s exact Test.
Associations of H. pylori infection with longitudinal cognitive decline
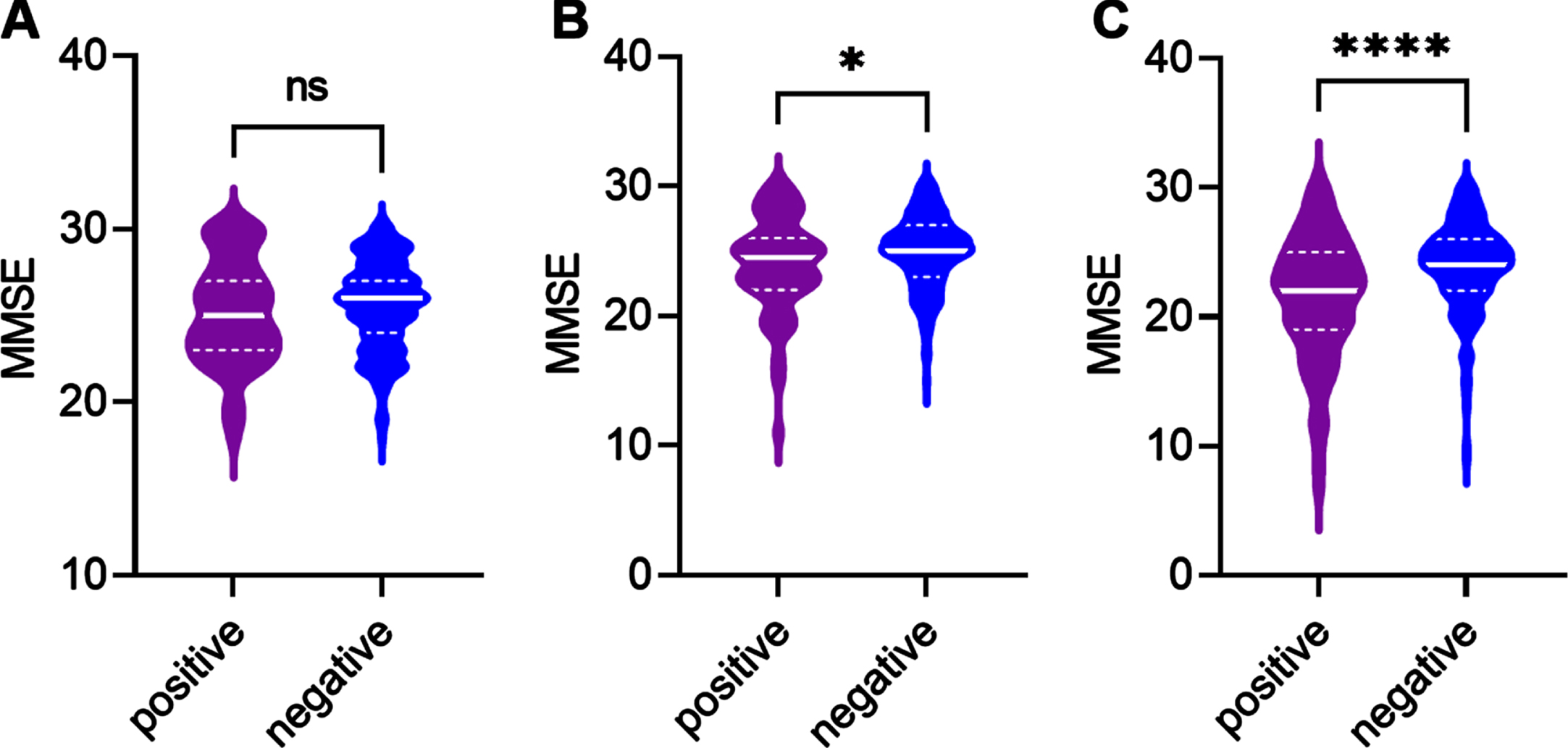
At baseline, H. pylori infected and uninfected participants had no difference in median MMSE scores (Fig. 2A). At one year of follow-up, H. pylori infected participants had significantly lower MMSE scores than uninfected participants (Fig. 2B). Similarly, H. pylori infected participants also had lower MMSE scores than uninfected participants at two years of follow-up (Fig. 2C). We next investigated the association between H. pylori infection and longitudinal cognitive decline during follow-up.
Cognitive functions and brain amyloid-β deposition at endpoint of follow-up. A) Comparison of cognitive functions, as reflected by MMSE scores, between H. pylori infected and uninfected participants. B) Comparison of brain amyloid-β deposition, as reflected by PET-PiB SUVR, between H. pylori infected and uninfected participants. Mann-Whitney Test.
In the multivariate logistical regression model, we found that H. pylori infection was associated with an increased risk of longitudinal cognitive decline, as reflected by a decrease of MMSE of 3 points or more during follow-up according to previous reports [18, 19], adjusting for age, sex, education, APOE ɛ4 genotype, hypertension, diabetes mellitus, hyperlipidemia, and smoking history (HR: 2.701; 95% CI: 1.392 to 5.242) (Table 2). In the linear regression model, H. pylori infection was associated with larger cognitive decline during follow-up (standardized coefficient: 0.282, p < 0.001), adjusting for the above covariates (Table 3). Furthermore, vascular risk factors, such as hypertension, diabetes mellitus, hyperlipidemia, and stroke history were also found to increase the risk of cognitive decline in the model. In the mixed effects models, H. pylori infected subjects had significantly higher speed of cognitive decline than uninfected subjects during follow-up, adjusting for the above covariates (slope difference: –2.050, 95% CIL: –2.586 to –1.515) (Fig. 3). These findings imply that H. pylori infection may increase the risk of longitudinal cognitive decline.
Risk factors for longitudinal cognitive decline
Logistical regression model. The dependent varaible is cognitive decline, as defined by a decrease in MMSE score of 3 or more during follow-up.
Association between H. pylori infection and the severity of cogntive decline during follow-up
Linear regression model. The severity of cognitive decline is defined by the decrease in MMSE scores during follow-up.
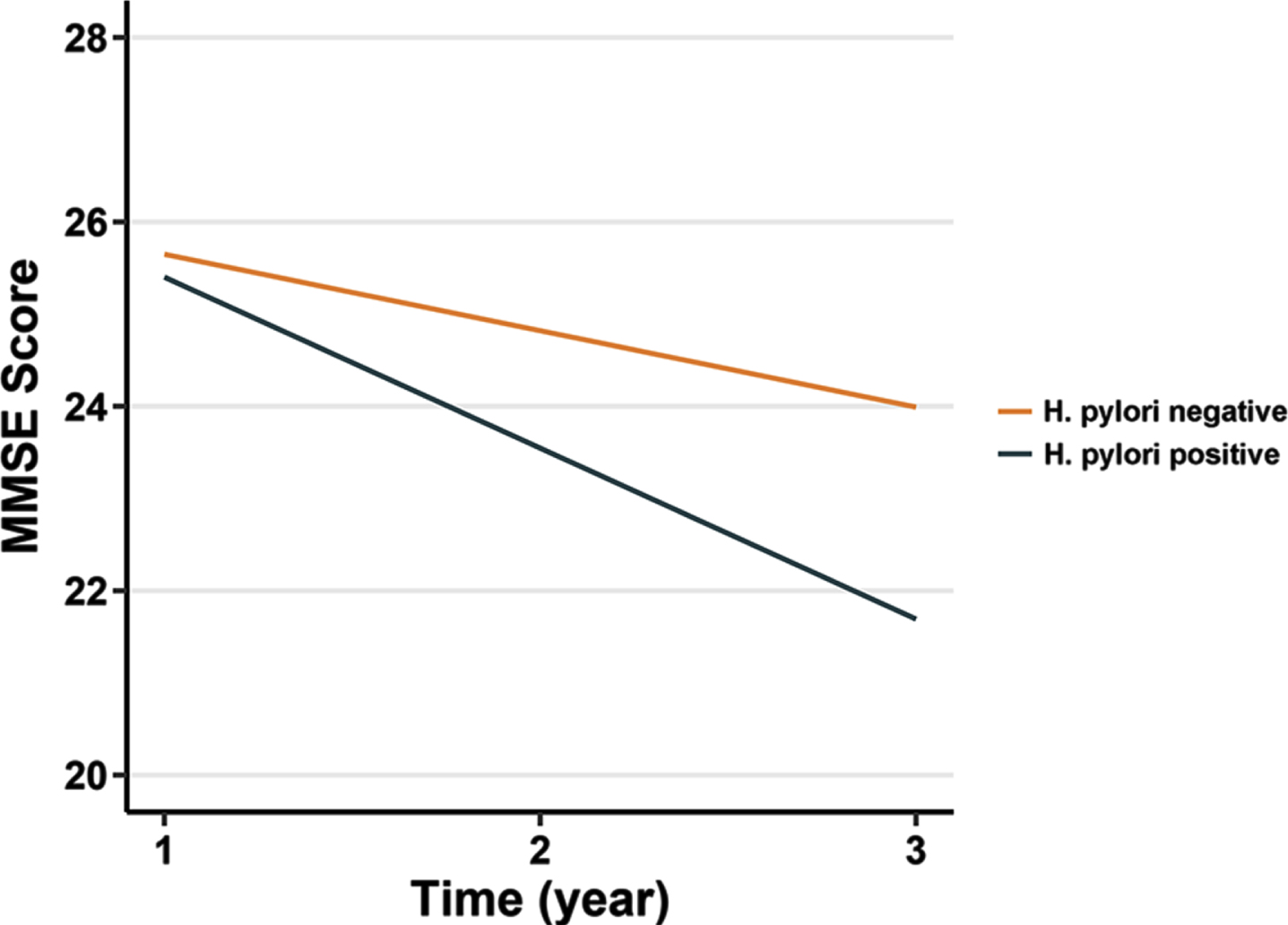
Longitudinal cognitive trajectories among H. pylori infected and uninfected participants. Longitudinal change of cognitive functions as reflected by MMSE among H. pylori positive and negative subjects. Mixed linear effects model, adjusting for age, sex, education, APOE ɛ4 genotype, hypertension, diabetes mellitus, hyperlipidemia, and smoking history.
DISCUSSION
The risk factors for cognitive impairment are largely unrevealed, which impedes the development of disease-modifying treatment. The role of microorganisms in triggering neuronal damage has been reported by a panel of studies [20–22]. Demented patients had a higher prevalence of H. pylori infection [23, 24], partly due to unhealthy diet. However, limited evidence is currently available upon the association between H. pylori infection and cognitive decline. Therefore, revealing the impact of H. pylori on the development and progression of cognitive impairment has important clinical and therapeutic implications.
In this study, we selected participants with self-reported memory impairment (subjective cognitive impairment), in which cognitive decline is more frequently seen than in cognitively intact populations [25, 26]. In the past decades, the associations between H. pylori infection and dementia, such as AD, have been investigated by numerous studies, which generated inconsistent findings. A study from the Third National Health and Nutrition Examination Survey (NHANES-III) suggested that the H. pylori-infected population had impaired cognitive performances [27]. Similarly, a positive association between H. pylori infection and cognitive impairment is reported in an Asian population from Taiwan [28]. In a recent report from the Framingham Heart Study, a negative association of infection serologies with incidences of dementia, total brain volume, and white matter hyperintensities was found [29]. However, the levels of H. pylori antibodies are associated with worse global cognition in this cohort [29]. In a previous study from Japan, where the prevalence of H. pylori infection is high, a negative association between H. pylori infection and dementia was reported [30]. Except for the heterogeneity in the study population, the possible reason for the inconsistency might be due to the cross-sectional setting which could not reveal the causative relationship between H. pylori infection and dementia. To further address this issue, this longitudinal study followed up the participants for 2 years to investigate the dynamic change of brain cognitive decline and generated a positive association between H. pylori infection and the development of dementia.
The mechanisms of H. pylori-associated cognitive impairment might be multifactorial. In animals, H. pylori infection is suggested to impair spatial learning and memory and increase amyloid-β deposition (a major pathological hallmark of AD) by enhancing the expression of presenilin-2 [31], and promote tau (a major pathological hallmark of AD) hyperphosphorylation through activating the glycogen synthase kinase-3β signaling pathway [32]. However, the impact of H. pylori infection on AD-type pathologies has rarely been investigated in humans. A study reported that H. pylori infection is associated with higher CSF pTau-181and total tau levels [33]. A previous study suggests that H. pylori eradication rescued cognitive decline in AD patients during a 2-year follow-up [34], and another study demonstrates that H. pylori eradication increases the survival rate of AD [35]. Based on the above studies, we suppose that patients may benefit from H. pylori eradication in cognition and brain amyloid deposition. Except for AD, H. pylori infection is also suggested to contribute to the development of vascular dementia. For example, a previous study found that H. pylori infection might exacerbate atherosclerosis, thus promoting the development of cognitive decline in patients with vascular dementia [36]. Further investigations demonstrate that infection-associated chronic inflammation is the major cause of cognitive impairment in these subjects [37].
The microbiota-gut-brain axis, which is a bidirectional communication system, plays a pivotal role in neurodegeneration [38, 39]. Gastrointestinal populating bacteria secrete large amounts of amyloid peptides and lipopolysaccharides and produce proinflammatory cytokines associated with neuronal damage [40]. Therefore, post-infection inflammation may have an important role in the pathogenesis of AD and vascular dementia [41]. Besides, an association between H. pylori infection and tau hyperphosphorylation is suggested to be mediated by its urease [42]. Increased plasma homocysteine, which is a risk factor for cognitive impairment [43], is a common feature after H. pylori infection [44]. Furthermore, increased autoantibodies against H. pylori are found in the CSF of demented patients, suggesting a possible autoimmune element of H. pylori-induced cognitive decline [34].
Limitations
This study has several limitations. First, the etiology of cognitive impairment in our cohort cannot be determined in such a study design, which lacks information of disease-specific biomarkers. Besides, the present data cannot generate a causative association between H. pylori infection and cognitive decline. Furthermore, the follow-up time is not long enough for long-course diseases including AD. During follow-up, no brain imaging information was obtained, thus the effects of H. pylori infection on the brain structural change are not clear. Based on this consideration, studies in community populations with longer follow-up periods are needed to confirm the present findings. Meanwhile, information about the H. pylori infection status prior to enrollment was obtained from the medical records or reported by the patient. In our cohort, no patient had previously diagnosed H. pylori infection. As H. pylori infection is insidious and not routinely screened, it is possible that the patient was not aware of the infection. In this regard, another limitation of this study is that the duration of H. pylori could not be obtained, which may cause bias to the present findings. However, our study reported the longitudinal change in cognitive functions in patients with H. pylori infection. The research findings are valuable for understanding the complex pathogenesis of dementia, such as AD, and reinforcing an infectious etiology ofdementia.
Footnotes
ACKNOWLEDGMENTS
We thank all participants for their contribution to this work.
FUNDING
This study was supported by the Sichuan Provincial Science and Technology Department (No. 2019ZYZF0063 and No.2020YJ0497) and Sichuan Medical Association (Grant No. Q21049).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.